Compliance of Atrial Fibrillation Treatment with the Atrial Fibrillation Better Care (ABC) Pathway Improves the Clinical Outcomes in the Middle East Population: A Report from the Gulf Survey of Atrial Fibrillation Events (SAFE) Registry

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
- ‘A’—‘Avoid stroke’—we identified patients at low risk of ischemic stroke (those with a CHA2DS2-VASc score of 0 in men or 1 in women) and assess whether everyone else is treated with OAC. (‘A compliant’). Patients at high risk of stroke, who did not receive OAC and those with low risk of stroke, but unnecessarily anticoagulated were considered as ‘A non-compliant’. The vast majority of patients receiving OAC in the current study were administered with vitamin K antagonists (VKA, e.g., warfarin).
- ‘B—better symptoms control’—we evaluated the occurrence of symptoms and classified them according to the European Heart Rhythm Association (EHRA) symptom scale. We assumed that patients with EHRA I or II had good control of AF symptoms (‘B complaint’) in comparison to those with EHRA III or IV, who were treated insufficiently (‘B non-complaint’).
- ‘C—Cardiovascular risk and other comorbidity optimisation’—To reduce cardiovascular risk, we evaluated appropriate treatment of the following comorbidities based on available data: hypertension (HT), coronary artery disease (CAD), peripheral artery disease (PAD) and ischemic stroke/TIA. HT assessment was based on an average of the blood pressure values at hospital admission that should be < 140/90 mmHg in order to be considered as well controlled. For other comorbidities, optimal pharmacologic management was evaluated in accordance with the current European guidelines and recommendations. (Figure S2). ‘C compliant’ means that all comorbidities were either well-controlled or treated with appropriate prevention drugs or both.
2.1. Outcomes
2.2. Statistical Analysis
3. Results
3.1. “ABC” Pathway Compliance
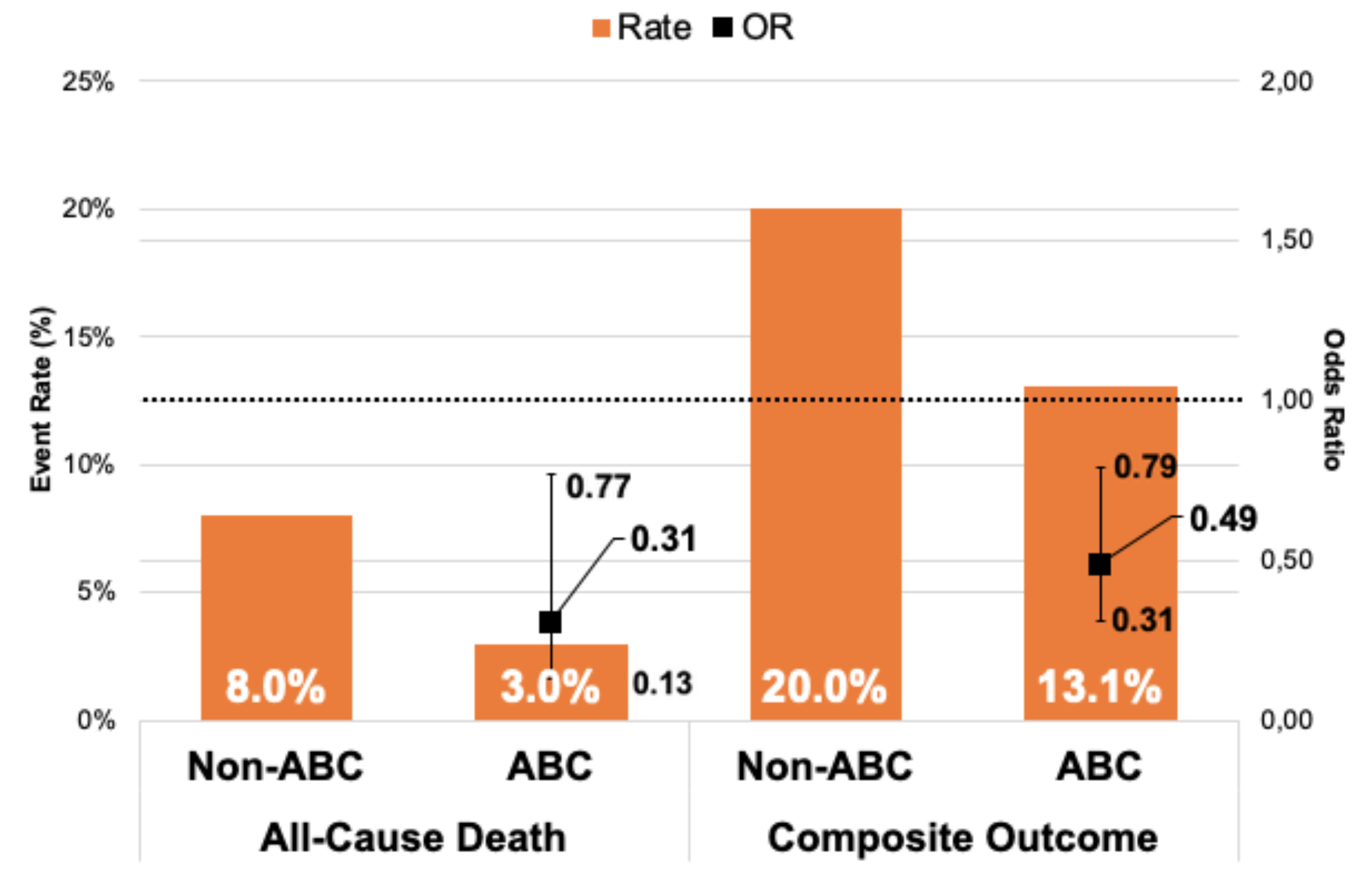
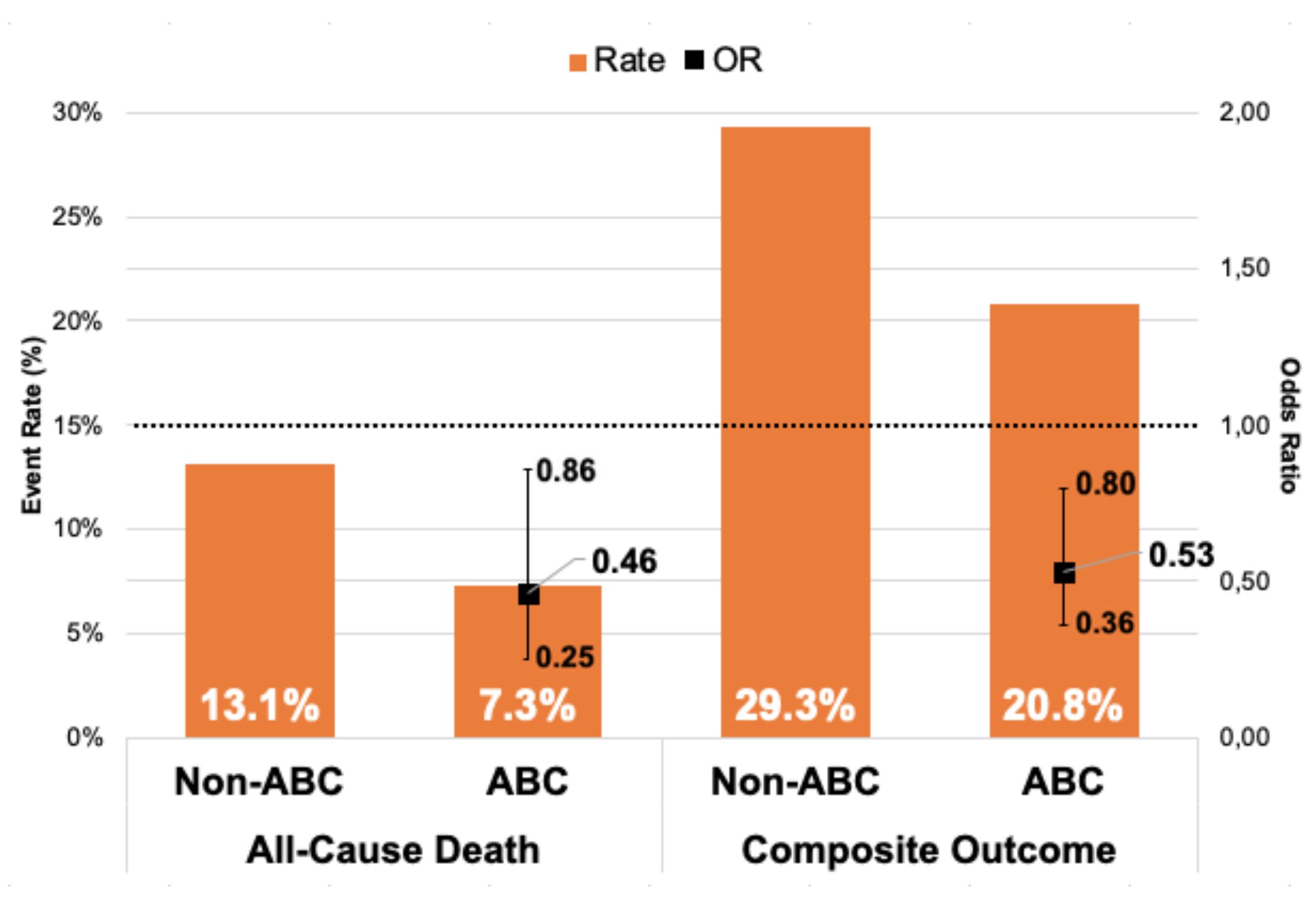
3.2. Clinical Outcomes
3.3. Number of Fulfilled ABC Criteria and Clinical Outcomes
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Amin, A.; Houmsse, A.; Ishola, A.; Tyler, J.; Houmsse, M. The current approach of atrial fibrillation management. Avicenna J. Med. 2016, 6, 8. [Google Scholar] [PubMed]
- Domek, M.; Gumprecht, J.; Mazurek, M.; Chao, T.-F.; Lip, G.Y.H. Should we judge stroke risk by static or dynamic risk scores? A focus on the dynamic nature of stroke and bleeding risks in patients with atrial fibrillation. J. Cardiovasc. Pharmacol. 2019, 74, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Odutayo, A.; Wong, C.X.; Hsiao, A.J.; Hopewell, S.; Altman, D.G.; Emdin, C.A. Atrial fibrillation and risks of cardiovascular disease, renal disease, and death: Systematic review and meta-analysis. BMJ 2016, 354, i4482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lip, G.Y.H. The ABC pathway: An integrated approach to improve AF management. Nat. Rev. Cardiol. 2017, 14, 627–628. [Google Scholar] [CrossRef] [PubMed]
- Gumprecht, J.; Domek, M.; Lip, G.Y.H.; Shantsila, A. Invited review: Hypertension and atrial fibrillation: Epidemiology, pathophysiology, and implications for management. J. Hum. Hypertens. 2019. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.H.; Freedman, B.; de Caterina, R.; Potpara, T.S. Stroke prevention in atrial fibrillation: Past, present and future comparing the guidelines and practical decision-making. Thromb. Haemost. 2017, 117, 1230–1239. [Google Scholar] [CrossRef] [PubMed]
- Alkhouli, M.; Friedman, P.A. Ischemic Stroke Risk in Patients With Nonvalvular Atrial Fibrillation. J. Am. Coll. Cardiol. 2019, 74, 3050–3065. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castellà, M.; Diener, H.-C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Hear. J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gumprecht, J.; Domek, M.; Lip, G.Y.H. A drug safety evaluation of apixaban for the treatment of atrial fibrillation, acute coronary syndrome, and percutaneous coronary intervention. Expert Opin. Drug Saf. 2019, 18, 1119–1125. [Google Scholar] [CrossRef]
- Pastori, D.; Farcomeni, A.; Pignatelli, P.; Violi, F.; Lip, G.Y. ABC (Atrial fibrillation Better Care) Pathway and Healthcare Costs in Atrial Fibrillation: The ATHERO-AF Study. Am. J. Med. 2019, 132, 856–861. [Google Scholar] [CrossRef]
- Yoon, M.; Yang, P.-S.; Jang, E.; Yu, H.T.; Kim, T.-H.; Uhm, J.-S.; Kim, J.-Y.; Sung, J.-H.; Pak, H.-N.; Lee, M.-H.; et al. Improved Population-Based Clinical Outcomes of Patients with Atrial Fibrillation by Compliance with the Simple ABC (Atrial Fibrillation Better Care) Pathway for Integrated Care Management: A Nationwide Cohort Study. Thromb. Haemost. 2019, 19, 1695–1703. [Google Scholar] [CrossRef] [PubMed]
- Proietti, M.; Romiti, G.F.; Olshansky, B.; Lane, D.A.; Lip, G.Y.H. Improved Outcomes by Integrated Care of Anticoagulated Patients with Atrial Fibrillation Using the Simple ABC (Atrial Fibrillation Better Care) Pathway. Am. J. Med. 2018, 131, 1359–1366.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zubaid, M.; Rashed, W.A.; Alsheikh-Ali, A.A.; AlMahmeed, W.; Shehab, A.; Sulaiman, K.; Al-Zakwani, I.; AlQudaimi, A.; Asaad, N.; Amin, H. Gulf survey of atrial fibrillation events (Gulf SAFE) design and baseline characteristics of patients with atrial fibrillation in the arab middle East. Circ. Cardiovasc. Qual. Outcomes 2011, 4, 477–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hendriks, J.M.; De Wit, R.; Crijns, H.J.; Vrijhoef, H.J.M.; Prins, M.H.; Pisters, R.; Pison, L.A.F.G.; Blaauw, Y.; Tieleman, R.G. Nurse-led care vs. usual care for patients with atrial fibrillation: Results of a randomized trial of integrated chronic care vs. routine clinical care in ambulatory patients with atrial fibrillation. Eur. Hear. J. 2012, 33, 2692–2699. [Google Scholar] [CrossRef] [PubMed]
- Nieuwlaat, R.; Olsson, S.B.; Lip, G.Y.; Camm, A.J.; Breithardt, G.; Capucci, A.; Meeder, J.G.; Prins, M.H.; Levy, S.; Crijns, H.J.; et al. Guideline-adherent antithrombotic treatment is associated with improved outcomes compared with undertreatment in high-risk patients with atrial fibrillation. The Euro Heart Survey on Atrial Fibrillation. Am. Heart. J. 2007, 153, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Proietti, M.; Laroche, C.; Nieuwlaat, R.; Crijns, H.J.; Maggioni, A.P.; Lane, D.A.; Boriani, G.; Lip, G.Y.H. Increased burden of comorbidities and risk of cardiovascular death in atrial fibrillation patients in Europe over ten years: A comparison between EORP-AF pilot and EHS-AF registries. Eur. J. Intern. Med. 2018, 55, 28–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, E.-J.; Yin, X.; Fontes, J.D.; Magnani, J.W.; Lubitz, S.A.; McManus, D.D.; Seshadri, S.; Vasan, R.S.; Ellinor, P.T.; Larson, M.G.; et al. Atrial fibrillation without comorbidities: Prevalence, incidence and prognosis (from the Framingham Heart Study). Am. Heart J. 2016, 177, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Perera, K.S.; Pearce, L.A.; Sharma, M.; Benavente, O.; Connolly, S.J.; Hart, R.G. Predictors of Mortality in Patients With Atrial Fibrillation (from the Atrial Fibrillation Clopidogrel Trial with Irbesartan for Prevention of Vascular Events [ACTIVE A]). Am. J. Cardiol. 2018, 121, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Pastori, D.; Pignatelli, P.; Menichelli, D.; Violi, F.; Lip, G.Y.H. Integrated Care Management of Patients With Atrial Fibrillation and Risk of Cardiovascular Events: The ABC (Atrial Fibrillation Better Care) Pathway in the ATHERO-AF Study Cohort. Mayo Clinic Proc. 2019, 94, 1261–1267. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | All Patients (n = 2021) | ABC Group (n = 168) | Non-ABC Group (n = 1853) | p Value |
|---|---|---|---|---|
| Demographics | ||||
| Male gender, n (%) | 1053 (52.1%) | 91 (54.3%) | 962 (51.9%) | 0.58 |
| Age, mean ± SD | 56.74 ± 16.47 | 64.46 ± 11.92 | 56.04 ± 16.65 | <0.001 |
| Weight, mean ± SD | 75.62 ± 18.29 | 78.98 ± 20.03 | 75.32 ± 18.11 | <0.015 |
| Height, mean ± SD | 164.25 ± 9.40 | 163.14 ± 9.87 | 164.35 ± 9.35 | 0.12 |
| BMI, mean ± SD | 28.00 ± 6.38 | 29.63 ± 7.24 | 27.86 ± 6.28 | 0.001 |
| Systolic BP, mmHg, mean ± SD | 130.30 ± 26.46 | 121.6 ± 14.00 | 131.10 ± 27.18 | <0.001 |
| Diastolic BP mmHg, mean ± SD | 79.03 ± 16.17 | 74.06 ± 10.25 | 79.50 ± 16.53 | <0.001 |
| Comorbidities, n (%) | ||||
| Coronary artery disease, n (%) | 573 (28.6%) | 89 (53.3%) | 484 (26.3%) | <0.001 |
| Hypertension, n (%) | 1065 (52.7%) | 117 (69.6%) | 948 (51.2%) | <0.001 |
| Dyslipidemia, n (%) | 677 (33.8%) | 103 (61.2%) | 574 (31.2%) | <0.001 |
| Heart failure, n (%) | 557 (27.6%) | 60 (35.7%) | 497 (26.8%) | 0.014 |
| Ischemic stroke or TIA, n (%) | 239 (11.8%) | 19 (11.3%) | 220 (11.9%) | 0.83 |
| Diabetes mellitus, n (%) | 603 (29.8%) | 86 (51.2%) | 517 (27.9%) | <0.001 |
| Chronic kidney disease n (%) | 122 (6.0%) | 6 (3.6%) | 116 (6.3%) | 0.016 |
| Smoking tobacco | 461 (23.0%) | 32 (19.2%) | 429 (23.3%) | 0.219 |
| Stroke or bleeding risk scores | ||||
| CHA2DS2-VASc, mean ± SD | 2.34 ± 1.78 | 3.01 ± 1.53 | 2.28 ± 1.79 | <0.001 |
| HAS-BLED, mean ± SD | 1.13 ± 1.065 | 1.33 ± 0.87 | 1.11 ± 1.08 | 0.008 |
| Echocardiogram | ||||
| Left atrium diameter (mm), n = 1444 | 44.36 ± 9.11 | 44.61 ± 7.03 | 44.34 ± 9.28 | 0.753 |
| LVEF, % n = 1490 | 51.23 ± 13.20 | 48.19 ± 14.44 | 51.51 ± 13.06 | 0.007 |
| Medications, n (%) n = 1945 ABC group n = 168, non-ABC group n = 1777 | ||||
| ACEI | 715 (36.8%) | 113 (67.3%) | 602 (33.9%) | <0.001 |
| ARB | 279 (14.3%) | 55 (32.7%) | 224 (12.6%) | <0.001 |
| Aspirin | 1058 (54.4%) | 97 (57.7%) | 961 (54.1%) | 0.36 |
| Beta-blocker | 1133 (58.3% | 119 (70.8%) | 1114 (57.1%) | 0.001 |
| Verapamil or Diltiazem | 164 (8.4%) | 11 (6.5%) | 153 (8.6%) | 0.36 |
| Other calcium channel blocker | 160 (7.9%) | 13 (7.7%) | 147 (8.3%) | 0.81 |
| Clopidogrel | 213 (11%) | 22 (13.1%) | 191 (10.7%) | 0.35 |
| Diuretics | 949 (48.8%) | 101 (60.01%) | 848 (47.7%) | 0.002 |
| Digoxin | 702 (36.1%) | 55 (32.7%) | 647 (36.4%) | 0.34 |
| Statin | 938 (48.2%) | 169 (97.0%) | 775 (43.6%) | <0.001 |
| Other lipid-lowering drug | 29 (1.5%) | 7 (4.2%) | 22 (1.2%) | 0.003 |
| Warfarin | 1049 (51.9%) | 155 (92.3%) | 894 (50.3%) | <0.001 |
| Other anticoagulant | 88 (4.5%) | 13 (7.7%) | 75 (4.2%) | 0.036 |
| Amiodarone | 178 (9.2%) | 27 (16.1%) | 151(8.5%) | 0.001 |
| Flecainide | 14 (0.7%) | 1 (0, 6%) | 13 (0.7%) | 0.84 |
| Propafenone | 34 (1.7%) | 1 (0, 6%) | 33 (1.9%) | 0.23 |
| Sotalol | 13 (0.7%) | 2 (1.2%) | 11 (0.6%) | 0.38 |
| Study Groups | Compliance | Non-Compliance |
|---|---|---|
| A | 1118 (55.3%) | 903 (44.7%) |
| B | 1518 (75.1%) | 503 (24.9%) |
| C | 388 (19.2%) | 1575 (77.9%) |
| ABC | 168 (8.3%) | 1853 (91.7) |
| Risk Factors | All-Cause Mortality | Composite Outcome | ||||||
|---|---|---|---|---|---|---|---|---|
| 6 Months | 1 Year | 6 Months | 1 Year | |||||
| OR (95% CI) | p Value | OR (95% CI) | p Value | OR (95% CI) | p Value | OR (95% CI) | p Value | |
| AF type (paroxysmal vs. persistent/permanent) | 1.11 (0.92–1.33) | 0.3 | 1.26 (1.07–1.48) | 0.006 | 1.29 (1.13–1.46) | <0.001 | 1.33 (1.19–1.49) | <0.001 |
| Renal dysfunction | 3.04 (1.86–4.97) | <0.001 | 3.05 (1.91–4.89) | <0.001 | 1.94 (1.30–2.92) | 0.001 | 1.8 (1.22–2.65) | 0.003 |
| Dyslipidemia | 1.20 (0.83–1.73) | 0.32 | 0.97 (0.71–1.33) | 0.85 | 1.26 (0.99–1.62) | 0.06 | 1.24 (0.99–1.54) | 0.06 |
| Use of aspirin | 1.33 (0.93–1.90) | 0.12 | 1.45 (1.07–1.97) | 0.018 | 1.41 (1.11–1.79) | 0.006 | 1.42 (1.14–1.76) | 0.001 |
| Major bleeding | 1.84 (0.84–4.04) | 0.13 | 1.74 (0.87–3.51) | 0.12 | 2.13 (1.22–3.72) | 0.008 | 3.09 (1.81–5.28) | <0.001 |
| ABC Compliance | 0.31 (0.13–0.77) | 0.013 | 0.46 (0.25–0.86) | 0.015 | 0.49 (0.31–0.79) | 0.003 | 0.53 (0.36–0.80) | 0.002 |
| Fulfilled Criteria | All-Cause Mortality | Composite Outcome | ||
|---|---|---|---|---|
| 1 Year | 1 Year | |||
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| AB | 0.78 (0.58–1.06) | 0.12 | 0.75 (0.61–0.92) | 0.006 |
| AC | 0.95 (0.62–1.46) | 0.83 | 1.0 (0.74–1.36) | 0.99 |
| BC | 0.73 (0.47–1.13) | 0.16 | 0.68 (0.50–0.92) | 0.013 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gumprecht, J.; Domek, M.; Proietti, M.; Li, Y.-G.; Asaad, N.; Rashed, W.; Alsheikh-Ali, A.; Zubaid, M.; Lip, G.Y.H. Compliance of Atrial Fibrillation Treatment with the Atrial Fibrillation Better Care (ABC) Pathway Improves the Clinical Outcomes in the Middle East Population: A Report from the Gulf Survey of Atrial Fibrillation Events (SAFE) Registry. J. Clin. Med. 2020, 9, 1286. https://doi.org/10.3390/jcm9051286
Gumprecht J, Domek M, Proietti M, Li Y-G, Asaad N, Rashed W, Alsheikh-Ali A, Zubaid M, Lip GYH. Compliance of Atrial Fibrillation Treatment with the Atrial Fibrillation Better Care (ABC) Pathway Improves the Clinical Outcomes in the Middle East Population: A Report from the Gulf Survey of Atrial Fibrillation Events (SAFE) Registry. Journal of Clinical Medicine. 2020; 9(5):1286. https://doi.org/10.3390/jcm9051286
Chicago/Turabian StyleGumprecht, Jakub, Magdalena Domek, Marco Proietti, Yan-Guang Li, Nidal Asaad, Wafa Rashed, Alawi Alsheikh-Ali, Mohammad Zubaid, and Gregory Y. H. Lip. 2020. "Compliance of Atrial Fibrillation Treatment with the Atrial Fibrillation Better Care (ABC) Pathway Improves the Clinical Outcomes in the Middle East Population: A Report from the Gulf Survey of Atrial Fibrillation Events (SAFE) Registry" Journal of Clinical Medicine 9, no. 5: 1286. https://doi.org/10.3390/jcm9051286