Validation of Hyponatremia as a Prognostic Predictor in Multiregional Upper Tract Urothelial Carcinoma

 , , , , , , , , , ,
, , , , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Collection
2.2. Postoperative Follow-Up
2.3. Statistical Analysis
3. Results
3.1. Clinicopathologic Characteristics
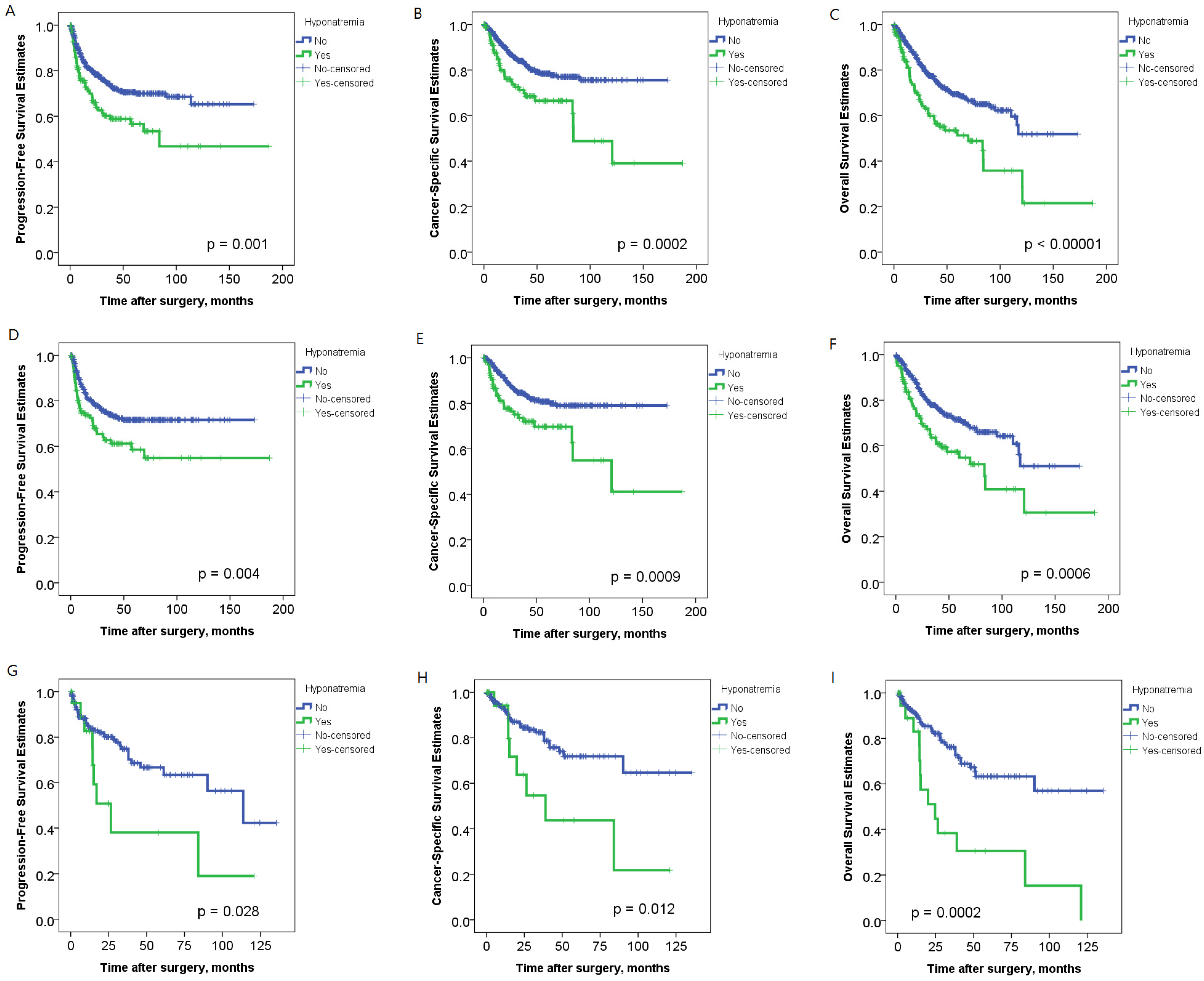
3.2. Correlation of Hyponatremia with Outcomes of UTUC Patients
3.3. Effect of Hyponatremia on Outcomes in Different Ethnicities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Singla, N.; Fang, D.; Su, X.; Bao, Z.; Cao, Z.; Jafri, S.M.; Xiong, G.; Zhang, L.; Hutchinson, R.; Sagalowsky, A.; et al. A multi-institutional comparison of clinicopathological characteristics and oncologic outcomes of upper tract urothelial carcinoma in china and the United States. J. Urol. 2017, 197, 1208–1213. [Google Scholar] [CrossRef] [PubMed]
- Singla, N.; Fang, D.; Su, X.; Bao, Z.; Cao, Z.; Robyak, H.; Xiong, G.; Zhang, L.; Woldu, S.; Hutchinson, R.; et al. Preoperative predictors of nonorgan-confined disease in upper-tract urothelial carcinoma differ between China and the United States. Urol. Oncol. 2018, 36, 88-e11. [Google Scholar] [CrossRef] [PubMed]
- Favaretto, R.L.; Shariat, S.F.; Savage, C.; Godoy, G.; Chade, D.C.; Kaag, M.; Bochner, B.H.; Coleman, J.; Dalbagni, G. Combining imaging and ureteroscopy variables in a preoperative multivariable model for prediction of muscle-invasive and non-organ confined disease in patients with upper tract urothelial carcinoma. BJU Int. 2012, 109, 77–82. [Google Scholar] [CrossRef]
- Remzi, M.; Haitel, A.; Margulis, V.; Karakiewicz, P.; Montorsi, F.; Kikuchi, E.; Zigeuner, R.; Weizer, A.; Bolenz, C.; Bensalah, K.; et al. Tumour architecture is an independent predictor of outcomes after nephroureterectomy: A multi-institutional analysis of 1363 patients. BJU Int. 2009, 103, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Doshi, S.M.; Shah, P.; Lei, X.; Lahoti, A.; Salahudeen, A.K. Hyponatremia in hospitalized cancer patients and its impact on clinical outcomes. Am. J. Kidney Dis. 2012, 59, 222–228. [Google Scholar] [CrossRef]
- Vasudev, N.S.; Brown, J.E.; Brown, S.R.; Rafiq, R.; Morgan, R.; Patel, P.M.; O’Donnell, D.; Harnden, P.; Rogers, M.; Cocks, K.; et al. Prognostic factors in renal cell carcinoma: Association of preoperative sodium concentration with survival. Clin. Cancer Res. 2008, 14, 1775–1781. [Google Scholar] [CrossRef] [Green Version]
- Hansen, O.; Sorensen, P.; Hansen, K.H. The occurrence of hyponatremia in SCLC and the influence on prognosis: A retrospective study of 453 patients treated in a single institution in a 10-year period. Lung Cancer 2010, 68, 111–114. [Google Scholar] [CrossRef]
- Rinaldi, S.; Santoni, M.; Leoni, G.; Fiordoliva, I.; Marcantognini, G.; Meletani, T.; Armento, G.; Santini, D.; Newsom-Davis, T.; Tiberi, M.; et al. The prognostic and predictive role of hyponatremia in patients with advanced non-small cell lung cancer (NSCLC) with bone metastases. Support. Care Cancer 2019, 27, 1255–1261. [Google Scholar] [CrossRef]
- Castillo, J.J.; Glezerman, I.G.; Boklage, S.H.; Chiodo, J., 3rd; Tidwell, B.A.; Lamerato, L.E.; Schulman, K.L. The occurrence of hyponatremia and its importance as a prognostic factor in a cross-section of cancer patients. Bmc Cancer 2016, 16, 564. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S.; Yi, S.Y.; Jun, H.J.; Lee, J.; Park, J.O.; Park, Y.S.; Jang, J.; Kim, H.J.; Ko, Y.; Lim, H.Y.; et al. Clinical outcome of gastric cancer patients with bone marrow metastases. Oncology 2007, 73, 192–197. [Google Scholar] [CrossRef] [Green Version]
- Huo, T.I.; Lin, H.C.; Hsia, C.Y.; Huang, Y.H.; Wu, J.C.; Chiang, J.H.; Chiou, Y.Y.; Lui, W.Y.; Lee, P.C.; Lee, S.D. The MELD-Na is an independent short- and long-term prognostic predictor for hepatocellular carcinoma: A prospective survey. Dig. Liver Dis. 2008, 40, 882–889. [Google Scholar] [CrossRef]
- Choi, J.S.; Bae, E.H.; Ma, S.K.; Kweon, S.S.; Kim, S.W. Prognostic impact of hyponatraemia in patients with colorectal cancer. Colorectal Dis. 2015, 17, 409–416. [Google Scholar] [CrossRef]
- Dhaliwal, H.S.; Rohatiner, A.Z.; Gregory, W.; Richards, M.A.; Johnson, P.W.; Whelan, J.S.; Gallagher, C.J.; Matthews, J.; Ganesan, T.S.; Barnett, M.J.; et al. Combination chemotherapy for intermediate and high grade non-Hodgkin’s lymphoma. Br. J. Cancer 1993, 68, 767–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berardi, R.; Caramanti, M.; Fiordoliva, I.; Morgese, F.; Savini, A.; Rinaldi, S.; Torniai, M.; Tiberi, M.; Ferrini, C.; Castagnani, M.; et al. Hyponatraemia is a predictor of clinical outcome for malignant pleural mesothelioma. Support. Care Cancer 2015, 23, 621–626. [Google Scholar] [CrossRef] [PubMed]
- Fujita, K.; Tanigawa, G.; Imamura, R.; Nakagawa, M.; Hayashi, T.; Kishimoto, N.; Hosomi, M.; Yamaguchi, S. Preoperative serum sodium is associated with cancer-specific survival in patients with upper urinary tract urothelial carcinoma treated by nephroureterectomy. Int. J. Urol. Off. J. Jpn. Urol. Assoc. 2013, 20, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Fujita, K.; Uemura, M.; Yamamoto, Y.; Tanigawa, G.; Nakata, W.; Sato, M.; Nagahara, A.; Kiuchi, H.; Nakai, Y.; Matsumiya, K.; et al. Preoperative risk stratification for cancer-specific survival of patients with upper urinary tract urothelial carcinoma treated by nephroureterectomy. Int. J. Clin. Oncol. 2015, 20, 156–163. [Google Scholar] [CrossRef]
- Hoorn, E.J.; Zietse, R. Diagnosis and Treatment of Hyponatremia: Compilation of the Guidelines. J. Am. Soc. Nephrol. 2017, 28, 1340–1349. [Google Scholar] [CrossRef]
- Kawashima, A.; Tsujimura, A.; Takayama, H.; Arai, Y.; Nin, M.; Tanigawa, G.; Uemura, M.; Nakai, Y.; Nishimura, K.; Nonomura, N.; et al. Impact of hyponatremia on survival of patients with metastatic renal cell carcinoma treated with molecular targeted therapy. Int. J. Urol. Off. J. Jpn. Urol. Assoc. 2012, 19, 1050–1057. [Google Scholar] [CrossRef]
- Wald, R.; Jaber, B.L.; Price, L.L.; Upadhyay, A.; Madias, N.E. Impact of hospital-associated hyponatremia on selected outcomes. Arch. Intern. Med. 2010, 170, 294–302. [Google Scholar] [CrossRef]
- Zilberberg, M.D.; Exuzides, A.; Spalding, J.; Foreman, A.; Jones, A.G.; Colby, C.; Shorr, A.F. Epidemiology, clinical and economic outcomes of admission hyponatremia among hospitalized patients. Curr. Med. Res. Opin. 2008, 24, 1601–1608. [Google Scholar] [CrossRef]
- Waikar, S.S.; Mount, D.B.; Curhan, G.C. Mortality after hospitalization with mild, moderate, and severe hyponatremia. Am. J. Med. 2009, 122, 857–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeppesen, A.N.; Jensen, H.K.; Donskov, F.; Marcussen, N.; von der Maase, H. Hyponatremia as a prognostic and predictive factor in metastatic renal cell carcinoma. Br. J. Cancer 2010, 102, 867–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sengupta, A.; Banerjee, S.N.; Biswas, N.M.; Jash, D.; Saha, K.; Maji, A.; Bandyopadhyaya, A.; Agarwal, S. The incidence of hyponatraemia and its effect on the ECOG performance status among lung cancer patients. J. Clin. Diagn. Res. 2013, 7, 1678–1682. [Google Scholar] [CrossRef]
- Balachandran, K.; Okines, A.; Gunapala, R.; Morganstein, D.; Popat, S. Resolution of severe hyponatraemia is associated with improved survival in patients with cancer. BMC Cancer 2015, 15, 163. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, L.; Johnson, B.E. Paraneoplastic syndromes associated with small cell lung cancer. J. Natl. Compr. Cancer Netw. 2006, 4, 631–638. [Google Scholar] [CrossRef]
- Martinez-Salamanca, J.I.; Shariat, S.F.; Rodriguez, J.C.; Chromecki, T.F.; Ficarra, V.; Fritsche, H.M.; Kassouf, W.; Matsumoto, K.; Cabello, L.O.; Seitz, C.; et al. Prognostic role of ECOG performance status in patients with urothelial carcinoma of the upper urinary tract: An international study. BJU Int. 2012, 109, 1155–1161. [Google Scholar] [CrossRef] [Green Version]
- Schutz, F.A.; Xie, W.; Donskov, F.; Sircar, M.; McDermott, D.F.; Rini, B.I.; Agarwal, N.; Pal, S.K.; Srinivas, S.; Kollmannsberger, C.; et al. The impact of low serum sodium on treatment outcome of targeted therapy in metastatic renal cell carcinoma: Results from the International metastatic renal cell cancer database consortium. Eur. Urol. 2014, 65, 723–730. [Google Scholar] [CrossRef] [Green Version]
- Fujita, K.; Taneishi, K.; Inamoto, T.; Ishizuya, Y.; Takada, S.; Tsujihata, M.; Tanigawa, G.; Minato, N.; Nakazawa, S.; Takada, T.; et al. Adjuvant chemotherapy improves survival of patients with high-risk upper urinary tract urothelial carcinoma: A propensity score-matched analysis. BMC Urol. 2017, 17, 110. [Google Scholar] [CrossRef] [Green Version]
- Berghmans, T.; Paesmans, M.; Body, J.J. A prospective study on hyponatraemia in medical cancer patients: Epidemiology, aetiology and differential diagnosis. Supportive Care Cancer 2000, 8, 192–197. [Google Scholar] [CrossRef]
- Rosner, M.H.; Dalkin, A.C. Electrolyte disorders associated with cancer. Adv. Chronic Kidney Dis. 2014, 21, 7–17. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | Category/Value | No. of Patients (%) | Hyponatremia | p Value | |
|---|---|---|---|---|---|
| No | Yes | ||||
| Age, years (mean, SD) | 68.0 (10.5) | 737 (100.0) | 67.5 (10.1) | 70.2 (11.7) | 0.006 |
| Gender | Female | 361 (49.0) | 295 (49.7) | 66 (46.2) | 0.451 |
| Male | 376 (51.0) | 299 (50.3) | 77 (53.8) | ||
| Region | Taiwan | 524 (71.1) | 403 (67.8) | 121 (84.6) | 0.00007 |
| U.S. | 213 (28.9) | 191 (32.2) | 22 (15.4) | ||
| ECOG | ≤1 | 603 (81.8) | 504 (84.8) | 99 (69.2) | 0.00001 |
| ≥2 | 134 (18.2) | 90 (15.2) | 44 (30.8) | ||
| eGFR, mL/min/1.73 m2 (mean, SD) | 51.8 (27.8) | 737 (100.0) | 52.8 (27.9) | 47.6 (26.7) | 0.043 |
| History of bladder cancer | No | 527 (71.5) | 418 (70.4) | 109 (76.2) | 0.164 |
| Yes | 210 (28.5) | 176 (29.6) | 34 (23.8) | ||
| Tumor location | Renal pelvis | 308 (41.8) | 247 (41.6) | 61 (42.7) | 0.528 |
| Ureter | 309 (41.9) | 254 (42.8) | 55 (38.5) | ||
| Both | 120 (16.3) | 93 (15.7) | 27 (18.9) | ||
| Hydronephrosis | No | 307 (41.7) | 243 (40.9) | 64 (44.8) | 0.402 |
| Yes | 430 (58.3) | 351 (59.1) | 79 (55.2) | ||
| Type of surgery | Nephroureterectomy | 630 (85.5) | 498 (83.8) | 132 (92.3) | 0.010 |
| Distal ureterectomy | 107 (14.5) | 96 (16.2) | 11 (7.7) | ||
| Approach of surgery | Open | 389 (52.8) | 311 (52.4) | 78 (54.5) | 0.638 |
| Laparoscopy | 348 (47.2) | 283 (47.6) | 65 (45.5) | ||
| Focality | Unifocal | 521 (70.7) | 420 (70.7) | 101 (70.6) | 0.985 |
| Multifocal | 216 (29.3) | 174 (29.3) | 42 (29.4) | ||
| Grade | Low | 129 (17.5) | 110 (18.5) | 19 (13.3) | 0.139 |
| High | 608 (82.5) | 484 (81.5) | 124 (86.7) | ||
| pT stage | pTa/Tis | 165 (22.4) | 147 (24.7) | 18 (12.6) | 0.002 |
| pT1 | 150 (20.4) | 123 (20.7) | 27 (18.9) | ||
| pT2 | 154 (20.9) | 111 (18.7) | 43 (30.1) | ||
| pT3 | 225 (30.5) | 182 (30.6) | 43 (30.1) | ||
| pT4 | 43 (5.8) | 31 (5.2) | 12 (8.4) | ||
| Lymphovascular invasion | No | 559 (75.8) | 448 (75.4) | 111 (77.6) | 0.581 |
| Yes | 178 (24.2) | 146 (24.6) | 32 (22.4) | ||
| pN stage | pN0 | 277 (37.6) | 219 (36.9) | 58 (40.6) | 0.488 |
| pNx | 393 (53.3) | 323 (54.4) | 70 (49.0) | ||
| pN+ | 67 (9.1) | 52 (8.8) | 15 (10.5) | ||
| Progression | No | 550 (74.6) | 458 (77.1) | 92 (64.3) | 0.002 |
| Yes | 187 (25.4) | 136 (22.9) | 51 (35.7) | ||
| Death of UTUC | No | 607 (82.4) | 503 (84.7) | 104 (72.7) | 0.001 |
| Yes | 130 (17.6) | 91 (15.3) | 39 (27.3) | ||
| All-cause death | No | 537 (72.9) | 453 (76.3) | 84 (58.7) | 0.00002 |
| Yes | 200 (27.1) | 141 (23.7) | 59 (41.3) | ||
| Variable | Progression-Free Survival | Cancer-Specific Survival | Overall Survival | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||||||||||
| HR | 95% CI | p Value | HR | 95% CI | p Value | HR | 95% CI | p Value | HR | 95% CI | p Value | HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age (continuous) | 1.016 | 1.002–1.031 | 0.026 | 1.008 | 0.993–1.023 | 0.281 | 1.029 | 1.011–1.048 | 0.001 | 1.020 | 1.001–1.039 | 0.036 | 1.030 | 1.016–1.045 | 0.00005 | 1.020 | 1.005–1.034 | 0.008 |
| Gender | ||||||||||||||||||
| Female | 1 | 0.096 | 1 | 0.762 | 1 | 0.086 | 1 | 0.871 | 1 | 0.051 | 1 | 0.619 | ||||||
| Male | 1.277 | 0.957–1.704 | 1.048 | 0.775–1.417 | 1.355 | 0.958–1.916 | 1.031 | 0.715–1.485 | 1.320 | 0.999–1.745 | 1.077 | 0.804–1.441 | ||||||
| Region | ||||||||||||||||||
| Taiwan | 1 | 0.385 | 1 | 0.269 | 1 | 0.080 | 1 | 0.044 | 1 | 0.222 | 1 | 0.169 | ||||||
| U.S. | 1.154 | 0.836–1.593 | 1.265 | 0.834–1.918 | 1.395 | 0.960–2.026 | 1.651 | 1.014–2.687 | 1.214 | 0.889–1.658 | 1.332 | 0.885–2.006 | ||||||
| ECOG | ||||||||||||||||||
| ≤1 | 1 | 0.029 | 1 | 0.082 | 1 | 0.035 | 1 | 0.596 | 1 | <0.00001 | 1 | 0.002 | ||||||
| ≥2 | 1.464 | 1.041–2.059 | 1.384 | 0.960–1.996 | 1.545 | 1.031–2.316 | 1.128 | 0.722–1.763 | 2.129 | 1.568–2.890 | 1.702 | 1.221–2.371 | ||||||
| eGFR (continuous) | 0.998 | 0.993–1.004 | 0.534 | 1.000 | 0.994–1.006 | 0.949 | 0.997 | 0.991–1.003 | 0.353 | 1.000 | 0.992–1.008 | 0.980 | 0.997 | 0.992–1.002 | 0.269 | 1.000 | 0.994–1.006 | 0.979 |
| History of bladder cancer | ||||||||||||||||||
| No | 1 | 0.247 | 1 | 0.130 | 1 | 0.195 | 1 | 0.122 | 1 | 0.270 | 1 | 0.216 | ||||||
| Yes | 1.201 | 0.881–1.639 | 1.291 | 0.927–1.799 | 1.276 | 0.882–1.844 | 1.366 | 0.920–2.029 | 1.186 | 0.875–1.607 | 1.227 | 0.887–1.699 | ||||||
| Tumor location | ||||||||||||||||||
| Renal pelvis | 1 | 0.001 | 1 | 0.162 | 1 | 0.00004 | 1 | 0.211 | 1 | <0.00001 | 1 | 0.288 | ||||||
| Ureter | 1.106 | 0.796–1.538 | 1.195 | 0.815–1.753 | 1.069 | 0.710–1.610 | 1.044 | 0.650–1.679 | 1.193 | 0.861–1.653 | 1.141 | 0.783–1.662 | ||||||
| Both | 1.970 | 1.351–2.872 | 1.639 | 0.986–2.724 | 2.469 | 1.600–3.812 | 1.650 | 0.904–3.011 | 2.352 | 1.641–3.371 | 1.487 | 0.908–2.434 | ||||||
| Hydronephrosis | ||||||||||||||||||
| No | 1 | 0.015 | 1 | 0.718 | 1 | 0.035 | 1 | 0.071 | 1 | 0.033 | 1 | 0.129 | ||||||
| Yes | 1.457 | 1.076–1.973 | 1.066 | 0.753–1.509 | 1.463 | 1.027–2.084 | 1.504 | 0.966–2.341 | 1.361 | 1.025–1.806 | 1.307 | 0.925–1.847 | ||||||
| Type of surgery | ||||||||||||||||||
| Nephroureterectomy | 1 | 0.110 | 1 | 0.528 | 1 | 0.248 | 1 | 0.830 | 1 | 0.132 | 1 | 0.609 | ||||||
| Distal ureterectomy | 0.666 | 0.404–1.097 | 0.815 | 0.432–1.539 | 0.705 | 0.389–1.277 | 0.919 | 0.424–1.990 | 0.689 | 0.424–1.118 | 0.851 | 0.458–1.581 | ||||||
| Approach of surgery | ||||||||||||||||||
| Open | 1 | 0.023 | 1 | 0.534 | 1 | 0.004 | 1 | 0.762 | 1 | 0.008 | 1 | 0.460 | ||||||
| Laparoscopy | 0.712 | 0.531–0.955 | 1.119 | 0.785–1.595 | 0.586 | 0.408–0.841 | 1.072 | 0.683–1.685 | 0.679 | 0.510–0.904 | 1.140 | 0.806–1.612 | ||||||
| Focality | ||||||||||||||||||
| Unifocal | 1 | 0.0004 | 1 | 0.843 | 1 | 0.0001 | 1 | 0.981 | 1 | 0.00003 | 1 | 0.645 | ||||||
| Multifocal | 1.712 | 1.273–2.303 | 1.041 | 0.698–1.552 | 1.994 | 1.407–2.827 | 0.994 | 0.607–1.628 | 1.830 | 1.378–2.430 | 1.099 | 0.736–1.640 | ||||||
| Grade | ||||||||||||||||||
| Low | 1 | <0.00001 | 1 | 0.023 | 1 | 0.00003 | 1 | 0.170 | 1 | <0.00001 | 1 | 0.106 | ||||||
| High | 5.517 | 2.822–10.786 | 2.268 | 1.118–4.602 | 5.844 | 2.573–13.274 | 1.847 | 0.770–4.432 | 3.186 | 1.934–5.247 | 1.564 | 0.909–2.692 | ||||||
| pT stage | ||||||||||||||||||
| pTa/Tis | 1 | <0.00001 | 1 | <0.00001 | 1 | <0.00001 | 1 | <0.00001 | 1 | <0.00001 | 1 | <0.00001 | ||||||
| pT1 | 1.730 | 0.823–3.637 | 1.665 | 0.775–3.577 | 0.938 | 0.329–2.675 | 0.895 | 0.306–2.617 | 0.921 | 0.495–1.713 | 0.933 | 0.491–1.774 | ||||||
| pT2 | 3.179 | 1.614–6.260 | 2.442 | 1.189–5.016 | 2.455 | 1.025–5.879 | 1.832 | 0.725–4.629 | 1.705 | 0.987–2.946 | 1.375 | 0.759–2.492 | ||||||
| pT3 | 7.450 | 3.988–13.916 | 4.634 | 2.365–9.080 | 8.600 | 3.959–18.681 | 5.146 | 2.221–11.928 | 3.961 | 2.446–6.413 | 2.786 | 1.621–4.786 | ||||||
| pT4 | 18.286 | 9.086–36.802 | 6.111 | 2.668–13.998 | 26.655 | 11.503–61.764 | 7.482 | 2.735–20.465 | 10.728 | 6.025–19.102 | 3.809 | 1.830–7.928 | ||||||
| Lymphovascular invasion | ||||||||||||||||||
| No | 1 | <0.00001 | 1 | 0.012 | 1 | <0.00001 | 1 | 0.007 | 1 | <0.00001 | 1 | 0.058 | ||||||
| Yes | 3.253 | 2.437–4.343 | 1.544 | 1.101–2.163 | 4.055 | 2.867–5.735 | 1.729 | 1.158–2.581 | 2.646 | 1.987–3.524 | 1.384 | 0.989–1.938 | ||||||
| pN stage | ||||||||||||||||||
| pN0 | 1 | <0.00001 | 1 | 0.003 | 1 | 0.00001 | 1 | 0.048 | 1 | <0.00001 | 1 | 0.028 | ||||||
| pNx | 0.805 | 0.581–1.116 | 0.941 | 0.672–1.317 | 0.804 | 0.539–1.198 | 0.953 | 0.631–1.441 | 0.790 | 0.580–1.076 | 0.944 | 0.685–1.301 | ||||||
| pN+ | 4.287 | 2.892–6.354 | 2.021 | 1.259–3.244 | 4.818 | 3.038–7.641 | 1.822 | 1.036–3.204 | 3.441 | 2.307–5.134 | 1.751 | 1.080–2.839 | ||||||
| Hyponatremia | ||||||||||||||||||
| No | 1 | 0.001 | 1 | 0.010 | 1 | 0.0002 | 1 | 0.0002 | 1 | 0.00001 | 1 | 0.0005 | ||||||
| Yes | 1.735 | 1.257–2.394 | 1.585 | 1.115–2.253 | 2.030 | 1.394–2.955 | 2.225 | 1.457–3.397 | 1.974 | 1.456–2.677 | 1.819 | 1.299–2.545 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeh, H.-C.; Li, C.-C.; Wen, S.-C.; Singla, N.; Woldu, S.L.; Robyak, H.; Huang, C.-N.; Ke, H.-L.; Li, W.-M.; Lee, H.-Y.; et al. Validation of Hyponatremia as a Prognostic Predictor in Multiregional Upper Tract Urothelial Carcinoma. J. Clin. Med. 2020, 9, 1218. https://doi.org/10.3390/jcm9041218
Yeh H-C, Li C-C, Wen S-C, Singla N, Woldu SL, Robyak H, Huang C-N, Ke H-L, Li W-M, Lee H-Y, et al. Validation of Hyponatremia as a Prognostic Predictor in Multiregional Upper Tract Urothelial Carcinoma. Journal of Clinical Medicine. 2020; 9(4):1218. https://doi.org/10.3390/jcm9041218
Chicago/Turabian StyleYeh, Hsin-Chih, Ching-Chia Li, Sheng-Chen Wen, Nirmish Singla, Solomon L. Woldu, Haley Robyak, Chun-Nung Huang, Hung-Lung Ke, Wei-Ming Li, Hsiang-Ying Lee, and et al. 2020. "Validation of Hyponatremia as a Prognostic Predictor in Multiregional Upper Tract Urothelial Carcinoma" Journal of Clinical Medicine 9, no. 4: 1218. https://doi.org/10.3390/jcm9041218