miR−21 and NT-proBNP Correlate with Echocardiographic Parameters of Atrial Dysfunction and Predict Atrial Fibrillation

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
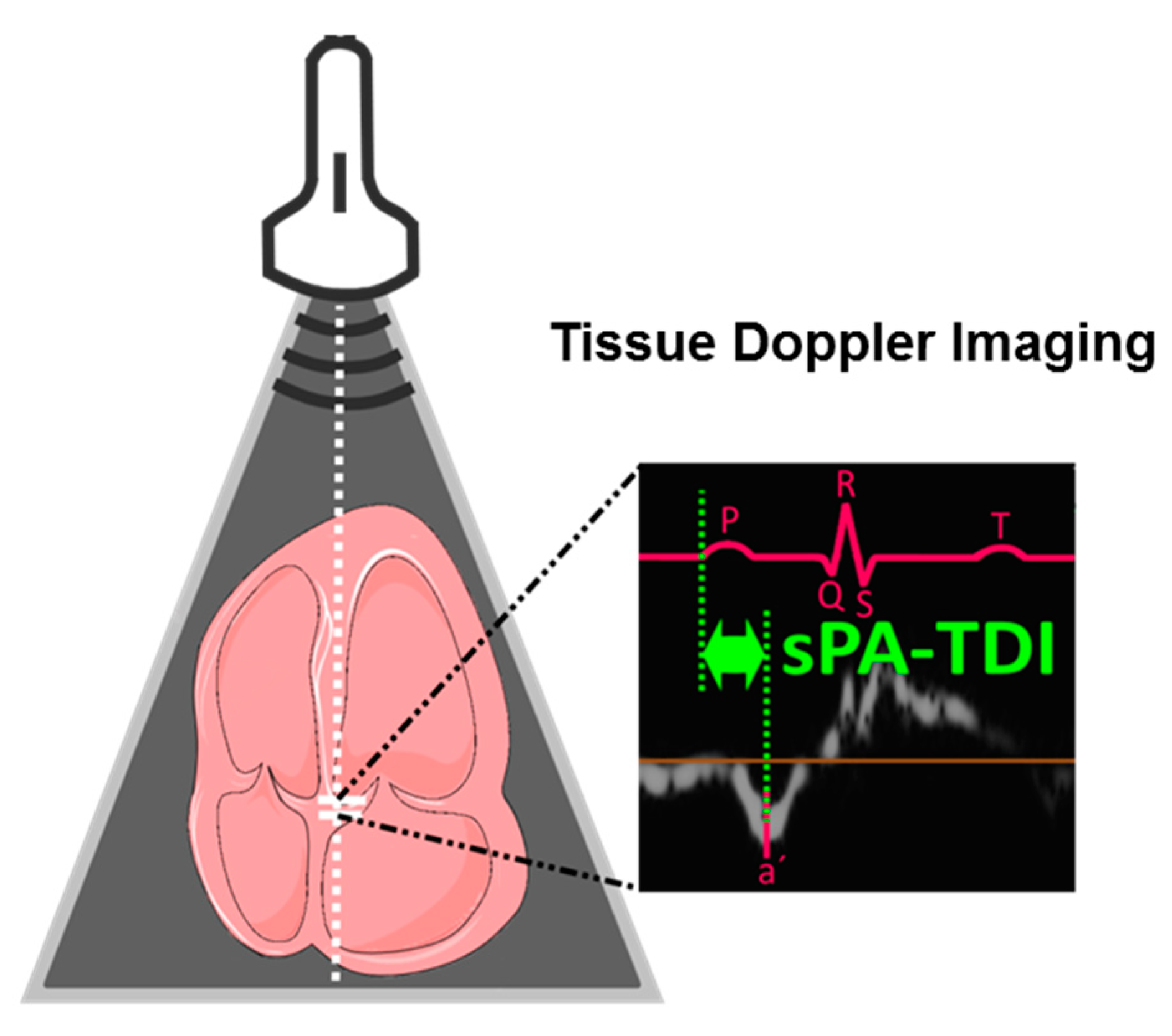
2.2. Echocardiography
2.3. Holter Electrocardiogram (ECG) Monitoring
2.4. Biomarker Assays
2.5. RNA Isolation from EDTA Plasma
2.6. Real-Time Polymerase Chain Reaction (PCR)-Based Amplification of MicroRNAs
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Soluble ST−2, Gal3 and NT-proBNP
3.3. MicroRNA-Panel Results
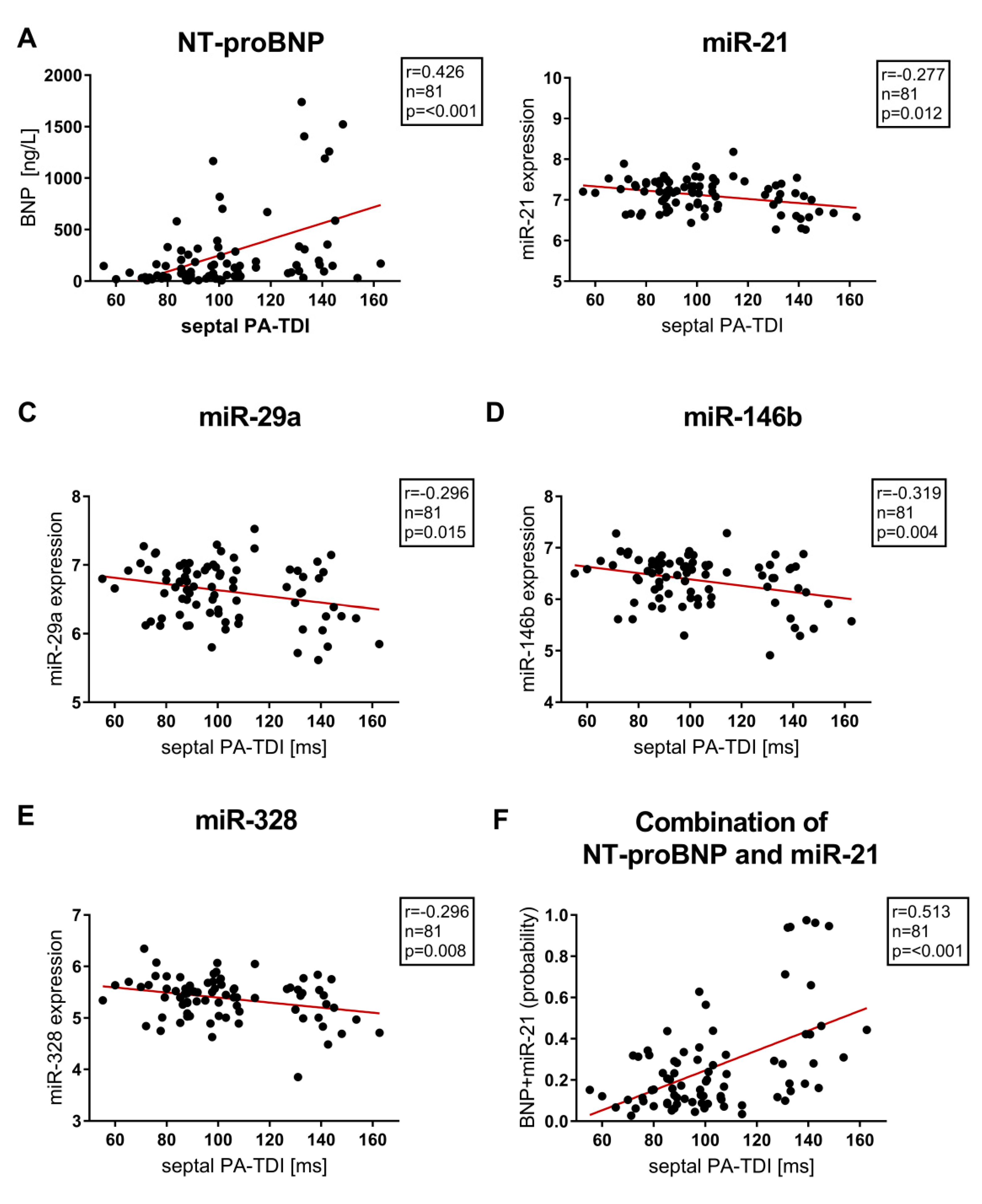
3.4. Correlation of Biomarkers and Echocardiographic Parameters of Left Atrial (LA) Function and Remodeling
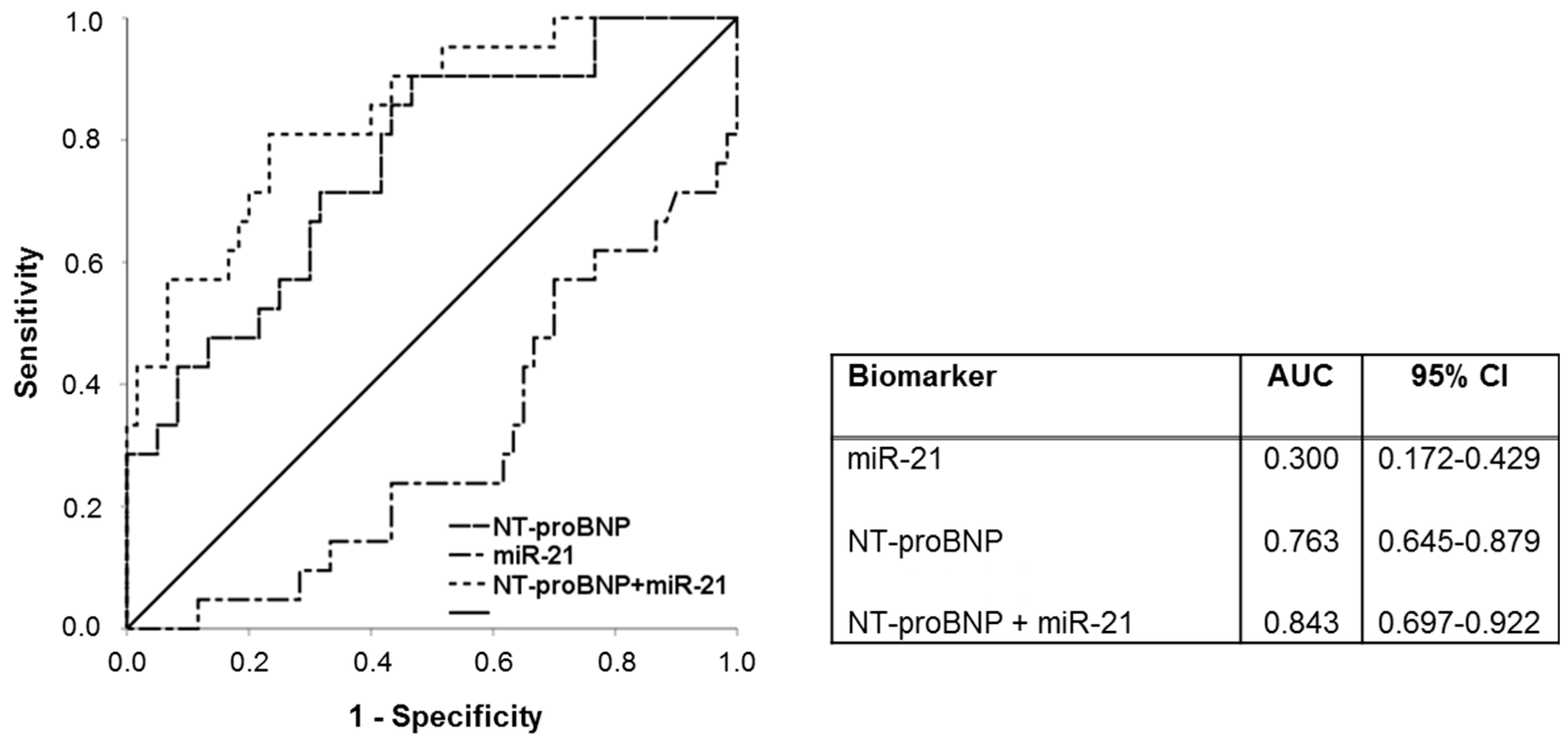
3.5. Biomarkers and Prediction of Atrial Fibrillation (AF)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AF | Atrial fibrillation |
| Cis | Confidence intervals |
| Gal3 | Galectin−3 |
| HR | Hazard ratio |
| LA | Left atrial |
| LAVI/á | Ration of LA volume index to tissue Doppler á |
| miR | MicroRNA |
| NT-proBNP | N-terminal fragment of pro-B-type natriuretic peptide |
| PA-TDI | Total atrial conduction time |
| ROC | Receiver operating characteristic |
| SRa | Second negative peak strain rate during LA contraction |
| sST2 | Soluble suppression of tumorigenicity 2 |
References
- Chinitz, J.S.; Castellano, J.M.; Kovacic, J.C.; Fuster, V. Atrial fibrillation, stroke, and quality of life. Ann. N. Y. Acad. Sci. 2012, 1254, 140–150. [Google Scholar] [CrossRef]
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Global Burden of Stroke. Circ. Res. 2017, 120, 439–448. [Google Scholar] [CrossRef]
- Haeusler, K.G.; Groschel, K.; Kohrmann, M.; Anker, S.D.; Brachmann, J.; Bohm, M.; Diener, H.C.; Doehner, W.; Endres, M.; Gerloff, C.; et al. Expert opinion paper on atrial fibrillation detection after ischemic stroke. Clin. Res. Cardiol. 2018, 107, 871–880. [Google Scholar] [CrossRef]
- Flint, A.C.; Banki, N.M.; Ren, X.; Rao, V.A.; Go, A.S. Detection of paroxysmal atrial fibrillation by 30-day event monitoring in cryptogenic ischemic stroke: The Stroke and Monitoring for PAF in Real Time (SMART) Registry. Stroke 2012, 43, 2788–2790. [Google Scholar] [CrossRef] [PubMed]
- Tayal, A.H.; Callans, D.J. Occult atrial fibrillation in ischemic stroke: Seek and you shall find. Neurology 2010, 74, 1662–1663. [Google Scholar] [CrossRef] [PubMed]
- Gladstone, D.J.; Spring, M.; Dorian, P.; Panzov, V.; Thorpe, K.E.; Hall, J.; Vaid, H.; O’Donnell, M.; Laupacis, A.; Cote, R.; et al. Coordinators Atrial fibrillation in patients with cryptogenic stroke. N. Engl. J. Med. 2014, 370, 2467–2477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanna, T.; Diener, H.C.; Passman, R.S.; Di Lazzaro, V.; Bernstein, R.A.; Morillo, C.A.; Rymer, M.M.; Thijs, V.; Rogers, T.; Beckers, F.; et al. Cryptogenic stroke and underlying atrial fibrillation. N. Engl. J. Med. 2014, 370, 2478–2486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wachter, R.; Groschel, K.; Gelbrich, G.; Hamann, G.F.; Kermer, P.; Liman, J.; Seegers, J.; Wasser, K.; Schulte, A.; Jurries, F.; et al. Holter-electrocardiogram-monitoring in patients with acute ischaemic stroke (Find-AFRANDOMISED): An open-label randomised controlled trial. Lancet Neurol. 2017, 16, 282–290. [Google Scholar] [CrossRef]
- Israel, C.; Kitsiou, A.; Kalyani, M.; Deelawar, S.; Ejangue, L.E.; Rogalewski, A.; Hagemeister, C.; Minnerup, J.; Schabitz, W.R. Detection of atrial fibrillation in patients with embolic stroke of undetermined source by prolonged monitoring with implantable loop recorders. Thromb. Haemost. 2017, 117, 1962–1969. [Google Scholar] [CrossRef]
- Donal, E.; Lip, G.Y.; Galderisi, M.; Goette, A.; Shah, D.; Marwan, M.; Lederlin, M.; Mondillo, S.; Edvardsen, T.; Sitges, M.; et al. EACVI/EHRA Expert Consensus Document on the role of multi-modality imaging for the evaluation of patients with atrial fibrillation. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 355–383. [Google Scholar] [CrossRef]
- Toh, N.; Kanzaki, H.; Nakatani, S.; Ohara, T.; Kim, J.; Kusano, K.F.; Hashimura, K.; Ohe, T.; Ito, H.; Kitakaze, M. Left atrial volume combined with atrial pump function identifies hypertensive patients with a history of paroxysmal atrial fibrillation. Hypertension 2010, 55, 1150–1156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leong, D.P.; Joyce, E.; Debonnaire, P.; Katsanos, S.; Holman, E.R.; Schalij, M.J.; Bax, J.J.; Delgado, V.; Marsan, N.A. Left Atrial Dysfunction in the Pathogenesis of Cryptogenic Stroke: Novel Insights from Speckle-Tracking Echocardiography. J. Am. Soc. Echocardiogr. 2017, 30, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Kuppahally, S.S.; Akoum, N.; Burgon, N.S.; Badger, T.J.; Kholmovski, E.G.; Vijayakumar, S.; Rao, S.N.; Blauer, J.; Fish, E.N.; Dibella, E.V.; et al. Left atrial strain and strain rate in patients with paroxysmal and persistent atrial fibrillation: Relationship to left atrial structural remodeling detected by delayed-enhancement MRI. Circ. Cardiovasc. Imaging 2010, 3, 231–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stahrenberg, R.; Edelmann, F.; Haase, B.; Lahno, R.; Seegers, J.; Weber-Kruger, M.; Mende, M.; Wohlfahrt, J.; Kermer, P.; Vollmann, D.; et al. Transthoracic echocardiography to rule out paroxysmal atrial fibrillation as a cause of stroke or transient ischemic attack. Stroke 2011, 42, 3643–3645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller, P.; Hars, C.; Schiedat, F.; Bosche, L.I.; Gotzmann, M.; Strauch, J.; Dietrich, J.W.; Vogt, M.; Tannapfel, A.; Deneke, T.; et al. Correlation between total atrial conduction time estimated via tissue Doppler imaging (PA-TDI Interval), structural atrial remodeling and new-onset of atrial fibrillation after cardiac surgery. J. Cardiovasc. Electrophysiol. 2013, 24, 626–631. [Google Scholar] [CrossRef]
- Sieweke, J.T.; Biber, S.; Weissenborn, K.; Heuschmann, P.U.; Akin, M.; Zauner, F.; Gabriel, M.M.; Schuppner, R.; Berliner, D.; Bauersachs, J.; et al. Septal total atrial conduction time for prediction of atrial fibrillation in embolic stroke of unknown source: A pilot study. Clin. Res. Cardiol. 2019. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.Y.; Heckbert, S.R.; Lai, S.; Ambale-Venkatesh, B.; Ostovaneh, M.R.; McClelland, R.L.; Lima, J.A.C.; Bluemke, D.A. Association of Elevated NT-proBNP With Myocardial Fibrosis in the Multi-Ethnic Study of Atherosclerosis (MESA). J. Am. Coll. Cardiol. 2017, 70, 3102–3109. [Google Scholar] [CrossRef]
- Vergaro, G.; Del Franco, A.; Giannoni, A.; Prontera, C.; Ripoli, A.; Barison, A.; Masci, P.G.; Aquaro, G.D.; Cohen Solal, A.; Padeletti, L.; et al. Galectin−3 and myocardial fibrosis in nonischemic dilated cardiomyopathy. Int. J. Cardiol. 2015, 184, 96–100. [Google Scholar] [CrossRef]
- Zile, M.R.; O’Meara, E.; Claggett, B.; Prescott, M.F.; Solomon, S.D.; Swedberg, K.; Packer, M.; McMurray, J.J.V.; Shi, V.; Lefkowitz, M.; et al. Effects of Sacubitril/Valsartan on Biomarkers of Extracellular Matrix Regulation in Patients With HFrEF. J. Am. Coll. Cardiol. 2019, 73, 795–806. [Google Scholar] [CrossRef]
- Felker, G.M.; Fiuzat, M.; Thompson, V.; Shaw, L.K.; Neely, M.L.; Adams, K.F.; Whellan, D.J.; Donahue, M.P.; Ahmad, T.; Kitzman, D.W.; et al. Soluble ST2 in ambulatory patients with heart failure: Association with functional capacity and long-term outcomes. Circ. Heart Fail. 2013, 6, 1172–1179. [Google Scholar] [CrossRef] [Green Version]
- Motiwala, S.R.; Szymonifka, J.; Belcher, A.; Weiner, R.B.; Baggish, A.L.; Sluss, P.; Gaggin, H.K.; Bhardwaj, A.; Januzzi, J.L. Serial measurement of galectin−3 in patients with chronic heart failure: Results from the ProBNP Outpatient Tailored Chronic Heart Failure Therapy (PROTECT) study. Eur. J. Heart Fail. 2013, 15, 1157–1163. [Google Scholar] [CrossRef] [PubMed]
- Szadkowska, I.; Wlazel, R.N.; Migala, M.; Szadkowski, K.; Zielinska, M.; Paradowski, M.; Pawlicki, L. The association between galectin−3 and clinical parameters in patients with first acute myocardial infarction treated with primary percutaneous coronary angioplasty. Cardiol. J. 2013, 20, 577–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yalcin, M.U.; Gurses, K.M.; Kocyigit, D.; Canpinar, H.; Canpolat, U.; Evranos, B.; Yorgun, H.; Sahiner, M.L.; Kaya, E.B.; Hazirolan, T.; et al. The Association of Serum Galectin−3 Levels with Atrial Electrical and Structural Remodeling. J. Cardiovasc. Electrophysiol. 2015, 26, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Sardu, C.; Marfella, R.; Santamaria, M.; Papini, S.; Parisi, Q.; Sacra, C.; Colaprete, D.; Paolisso, G.; Rizzo, M.R.; Barbieri, M. Stretch, Injury and Inflammation Markers Evaluation to Predict Clinical Outcomes After Implantable Cardioverter Defibrillator Therapy in Heart Failure Patients With Metabolic Syndrome. Front. Physiol. 2018, 9, 758. [Google Scholar] [CrossRef] [Green Version]
- Ambros, V. The functions of animal microRNAs. Nature 2004, 431, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Thum, T.; Gross, C.; Fiedler, J.; Fischer, T.; Kissler, S.; Bussen, M.; Galuppo, P.; Just, S.; Rottbauer, W.; Frantz, S.; et al. MicroRNA−21 contributes to myocardial disease by stimulating MAP kinase signalling in fibroblasts. Nature 2008, 456, 980–984. [Google Scholar] [CrossRef]
- Fiedler, J.; Jazbutyte, V.; Kirchmaier, B.C.; Gupta, S.K.; Lorenzen, J.; Hartmann, D.; Galuppo, P.; Kneitz, S.; Pena, J.T.; Sohn-Lee, C.; et al. MicroRNA−24 regulates vascularity after myocardial infarction. Circulation 2011, 124, 720–730. [Google Scholar] [CrossRef] [Green Version]
- Lu, D.; Thum, T. RNA-based diagnostic and therapeutic strategies for cardiovascular disease. Nat. Rev. Cardiol. 2019. [Google Scholar] [CrossRef]
- Adam, O.; Lohfelm, B.; Thum, T.; Gupta, S.K.; Puhl, S.L.; Schafers, H.J.; Bohm, M.; Laufs, U. Role of miR−21 in the pathogenesis of atrial fibrosis. Basic Res. Cardiol. 2012, 107, 278. [Google Scholar] [CrossRef]
- Dawson, K.; Wakili, R.; Ordog, B.; Clauss, S.; Chen, Y.; Iwasaki, Y.; Voigt, N.; Qi, X.Y.; Sinner, M.F.; Dobrev, D.; et al. MicroRNA29: A mechanistic contributor and potential biomarker in atrial fibrillation. Circulation 2013, 127, 1466–1475. [Google Scholar] [CrossRef] [Green Version]
- Santulli, G.; Iaccarino, G.; De Luca, N.; Trimarco, B.; Condorelli, G. Atrial fibrillation and microRNAs. Front. Physiol. 2014, 5, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheitlin, M.D.; Armstrong, W.F.; Aurigemma, G.P.; Beller, G.A.; Bierman, F.Z.; Davis, J.L.; Douglas, P.S.; Faxon, D.P.; Gillam, L.D.; Kimball, T.R.; et al. ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography: Summary article: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASE Committee to Update the 1997 Guidelines for the Clinical Application of Echocardiography). Circulation 2003, 108, 1146–1162. [Google Scholar] [CrossRef] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace 2016, 18, 1609–1678. [Google Scholar] [CrossRef] [PubMed]
- Derda, A.A.; Thum, S.; Lorenzen, J.M.; Bavendiek, U.; Heineke, J.; Keyser, B.; Stuhrmann, M.; Givens, R.C.; Kennel, P.J.; Schulze, P.C.; et al. Blood-based microRNA signatures differentiate various forms of cardiac hypertrophy. Int. J. Cardiol. 2015, 196, 115–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kok, M.G.; Halliani, A.; Moerland, P.D.; Meijers, J.C.; Creemers, E.E.; Pinto-Sietsma, S.J. Normalization panels for the reliable quantification of circulating microRNAs by RT-qPCR. FASEB J. 2015, 29, 3853–3862. [Google Scholar] [CrossRef]
- Bayes-Genis, A.; Lanfear, D.E.; de Ronde, M.W.J.; Lupon, J.; Leenders, J.J.; Liu, Z.; Zuithoff, N.P.A.; Eijkemans, M.J.C.; Zamora, E.; De Antonio, M.; et al. Prognostic value of circulating microRNAs on heart failure-related morbidity and mortality in two large diverse cohorts of general heart failure patients. Eur. J. Heart Fail. 2018, 20, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Andersen, C.L.; Jensen, J.L.; Orntoft, T.F. Normalization of real-time quantitative reverse transcription-PCR data: A model-based variance estimation approach to identify genes suited for normalization, applied to bladder and colon cancer data sets. Cancer Res. 2004, 64, 5245–5250. [Google Scholar] [CrossRef] [Green Version]
- Vandesompele, J.; De Preter, K.; Pattyn, F.; Poppe, B.; Van Roy, N.; De Paepe, A.; Speleman, F. Accurate normalization of real-time quantitative RT-PCR data by geometric averaging of multiple internal control genes. Genome Biol. 2002, 3, research0034-1. [Google Scholar] [CrossRef] [Green Version]
- Kernan, W.N.; Ovbiagele, B.; Black, H.R.; Bravata, D.M.; Chimowitz, M.I.; Ezekowitz, M.D.; Fang, M.C.; Fisher, M.; Furie, K.L.; Heck, D.V.; et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 2160–2236. [Google Scholar] [CrossRef]
- Maisel, A.S.; Krishnaswamy, P.; Nowak, R.M.; McCord, J.; Hollander, J.E.; Duc, P.; Omland, T.; Storrow, A.B.; Abraham, W.T.; Wu, A.H.; et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N. Engl. J. Med. 2002, 347, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Jung, J.H.; Choi, S.H.; Lee, N.; Park, W.J.; Oh, D.J.; Rhim, C.Y.; Lee, K.H. Determinants of brain natriuretic peptide levels in patients with lone atrial fibrillation. Circ. J. 2006, 70, 100–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellinor, P.T.; Low, A.F.; Patton, K.K.; Shea, M.A.; Macrae, C.A. Discordant atrial natriuretic peptide and brain natriuretic peptide levels in lone atrial fibrillation. J. Am. Coll. Cardiol. 2005, 45, 82–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, I.C.; Chen, L.Y.; Chong, J.P.; Austin, E.; Quay, C.N.; Gong, L.; Mark Richards, A.; Ling, L.H. Plasma mid-regional pro-atrial natriuretic peptide and N-terminal pro-brain natriuretic peptide improve discrimination of lone atrial fibrillation. Int. J. Cardiol. 2015, 188, 10–12. [Google Scholar] [CrossRef]
- Hussein, A.A.; Saliba, W.I.; Martin, D.O.; Shadman, M.; Kanj, M.; Bhargava, M.; Dresing, T.; Chung, M.; Callahan, T.; Baranowski, B.; et al. Plasma B-type natriuretic peptide levels and recurrent arrhythmia after successful ablation of lone atrial fibrillation. Circulation 2011, 123, 2077–2082. [Google Scholar] [CrossRef] [Green Version]
- De Boer, R.A.; Yu, L.; van Veldhuisen, D.J. Galectin−3 in cardiac remodeling and heart failure. Curr. Heart Fail. Rep. 2010, 7, 1–8. [Google Scholar] [CrossRef]
- Hernandez-Romero, D.; Vilchez, J.A.; Lahoz, A.; Romero-Aniorte, A.I.; Jover, E.; Garcia-Alberola, A.; Jara-Rubio, R.; Martinez, C.M.; Valdes, M.; Marin, F. Galectin−3 as a marker of interstitial atrial remodelling involved in atrial fibrillation. Sci. Rep. 2017, 7, 40378. [Google Scholar] [CrossRef]
- Fashanu, O.E.; Norby, F.L.; Aguilar, D.; Ballantyne, C.M.; Hoogeveen, R.C.; Chen, L.Y.; Soliman, E.Z.; Alonso, A.; Folsom, A.R. Galectin−3 and incidence of atrial fibrillation: The Atherosclerosis Risk in Communities (ARIC) study. Am. Heart J. 2017, 192, 19–25. [Google Scholar] [CrossRef]
- Cardin, S.; Guasch, E.; Luo, X.; Naud, P.; Le Quang, K.; Shi, Y.; Tardif, J.C.; Comtois, P.; Nattel, S. Role for MicroRNA−21 in atrial profibrillatory fibrotic remodeling associated with experimental postinfarction heart failure. Circ. Arrhythmia Electrophysiol. 2012, 5, 1027–1035. [Google Scholar] [CrossRef] [Green Version]
- Galenko, O.; Jacobs, V.; Knight, S.; Taylor, M.; Cutler, M.J.; Muhlestein, J.B.; Carlquist, J.L.; Knowlton, K.U.; Jared Bunch, T. The role of microRNAs in the development, regulation, and treatment of atrial fibrillation. J. Interv. Card. Electrophysiol. 2019, 55, 297–305. [Google Scholar] [CrossRef]
- Liu, Z.; Zhou, C.; Liu, Y.; Wang, S.; Ye, P.; Miao, X.; Xia, J. The expression levels of plasma micoRNAs in atrial fibrillation patients. PLoS ONE 2012, 7, e44906. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Zhang, Y.; Wang, N.; Pan, Z.; Gao, X.; Zhang, F.; Zhang, Y.; Shan, H.; Luo, X.; Bai, Y.; et al. MicroRNA−328 contributes to adverse electrical remodeling in atrial fibrillation. Circulation 2010, 122, 2378–2387. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, Y.; Han, J.; Li, Y.; Xie, C.; Xie, L.; Shi, J.; Zhang, J.; Yang, B.; Chen, D.; et al. Integrated analysis of microRNA and mRNA expression profiles in the left atrium of patients with nonvalvular paroxysmal atrial fibrillation: Role of miR−146b−5p in atrial fibrosis. Heart Rhythm 2015, 12, 1018–1026. [Google Scholar] [CrossRef] [PubMed]
- Duisters, R.F.; Tijsen, A.J.; Schroen, B.; Leenders, J.J.; Lentink, V.; van der Made, I.; Herias, V.; van Leeuwen, R.E.; Schellings, M.W.; Barenbrug, P.; et al. miR−133 and miR−30 regulate connective tissue growth factor: Implications for a role of microRNAs in myocardial matrix remodeling. Circ. Res. 2009, 104, 170–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sardu, C.; Santamaria, M.; Paolisso, G.; Marfella, R. microRNA expression changes after atrial fibrillation catheter ablation. Pharmacogenomics J. 2015, 16, 1863–1877. [Google Scholar] [CrossRef]
- Goette, A.; Kalman, J.M.; Aguinaga, L.; Akar, J.; Cabrera, J.A.; Chen, S.A.; Chugh, S.S.; Corradi, D.; D’Avila, A.; Dobrev, D.; et al. EHRA/HRS/APHRS/SOLAECE expert consensus on atrial cardiomyopathies: Definition, characterization, and clinical implication. Europace 2016, 18, 1455–1490. [Google Scholar] [CrossRef]
- Schneider, C.; Malisius, R.; Krause, K.; Lampe, F.; Bahlmann, E.; Boczor, S.; Antz, M.; Ernst, S.; Kuck, K.H. Strain rate imaging for functional quantification of the left atrium: Atrial deformation predicts the maintenance of sinus rhythm after catheter ablation of atrial fibrillation. Eur. Heart J. 2008, 29, 1397–1409. [Google Scholar] [CrossRef] [Green Version]
- Huynh, Q.L.; Kalam, K.; Iannaccone, A.; Negishi, K.; Thomas, L.; Marwick, T.H. Functional and Anatomic Responses of the Left Atrium to Change in Estimated Left Ventricular Filling Pressure. J. Am. Soc. Echocardiogr. 2015, 28, 1428–1433. [Google Scholar] [CrossRef]
- Pathan, F.; D’Elia, N.; Nolan, M.T.; Marwick, T.H.; Negishi, K. Normal Ranges of Left Atrial Strain by Speckle-Tracking Echocardiography: A Systematic Review and Meta-Analysis. J. Am. Soc. Echocardiogr. 2017, 30, 59–70. [Google Scholar] [CrossRef]
- Sardu, C.; Santamaria, M.; Rizzo, M.R.; Barbieri, M.; di Marino, M.; Paolisso, G.; Santulli, G.; Marfella, R. Telemonitoring in heart failure patients treated by cardiac resynchronisation therapy with defibrillator (CRT-D): The TELECART Study. Int. J. Clin. Pract. 2016, 70, 569–576. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| microRNA | Sequence |
|---|---|
| hsa-miR−21−5p | UAGCUUAUCAGACUGAUGUUGA |
| hsa-miR−29a−3p | UAGCACCAUCUGAAAUCGGUUA |
| hsa-miR−133a−3p | UUUGGUCCCCUUCAACCAGCUG |
| hsa-miR−146b−5p | UGAGAACUGAAUUCCAUAGGCUG |
| hsa-miR−328−3p | CUGGCCCUCUCUGCCCUUCCGU |
| hsa-miR−486−5p | UCCUGUACUGAGCUGCCCCGAG |
| Cel-miR−39−3p | UCACCGGGUGUAAAUCAGCUUG |
| Parameter | All Patients | w/o Stroke | Stroke | ||||||
|---|---|---|---|---|---|---|---|---|---|
| −AF (n = 60) | +AF (n = 21) | p −AF vs. +AF | −AF, Young (n = 13) | −AF, Old (n = 10) | +AF (n = 11) | −AF (n = 37) | +AF (n = 10) | ||
| Age (years) | 58.2 ± 19 | 71.8 ± 11.3 | 0.005 | 30.1 ± 6.6 | 65.5 ± 10.3 # | 67.7 ± 12.7 # | 65.8 ± 13.9 $ | 76.2 ± 8 | |
| Male | 42 (70%) | 14 (66.7%) | 0.853 | 10 (76.9%) | 6 (60%) | 9 (81.8%) | 26 (70.3%) | 5 (50%) | |
| Height (cm) | 173.5 ± 9.6 | 170.6 ± 10.7 | 0.246 | 180.5 ± 6.5 | 171.3 ± 8.9 | 173.1 ± 11.01 | 171.7 ± 9.7 | 167.8 ± 10.2 | |
| Weight (kg) | 79.3 ± 13.2 | 76.1 ± 16.6 | 0.667 | 78.1 ± 10.2 | 78.4 ± 14.3 | 79 ± 18.1 | 79.6 ± 14.4 | 72.9 ± 15.0 | |
| Pre-existing Conditions | |||||||||
| Hypertension | 31 (50.8%) | 17 (81.0%) | 0.016 | 0 (0.0%) | 3 (30%) | 8 (72.7%) ## | 26 (70.3%) | 9 (90%) | |
| Diabetes | 11 (18.0%) | 5 (23.8%) | 0.565 | 0 (0.0%) | 1 (10%) | 0 (0.0%) | 10 (27%) | 4 (40%) | |
| Smoking | 13 (21.3%) | 4 (19.0%) | 0.852 | 1 (7.7%) | 3 (30%) | 3 (27.3%) | 9 (24.3%) | 1 (10%) | |
| Stroke | 13 (21.3%) | 4 (19.0%) | 0.811 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 11 (29.7%) | 3 (30%) | |
| CKI | 5 (8.2%) | 1 (4.8%) | 0.602 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 5 (13.5%) | 1 (10%) | |
| CAD | 9 (14.8%) | 6 (28.6%) | 0.158 | 0 (0.0%) | 2 (20%) | 3 (27.3%) | 7 (18.9%) | 3 (30%) | |
| PAD | 5 (8.2%) | 2 (9.5%) | 0.851 | 0 (0.0%) | 1 (10%) | 2 (18.2) | 4 (10.8%) | 0 (0.0%) | |
| Echocardiographic Parameters | |||||||||
| LVEF (%) | 60.3 ± 4.9 | 59.4 ± 7.66 | 0.840 | 61.2 ± 2.7 | 59.0 ± 6.8 | 62.1 ± 6.2 | 60.4 ± 5.0 | 58.9 ± 8.3 | |
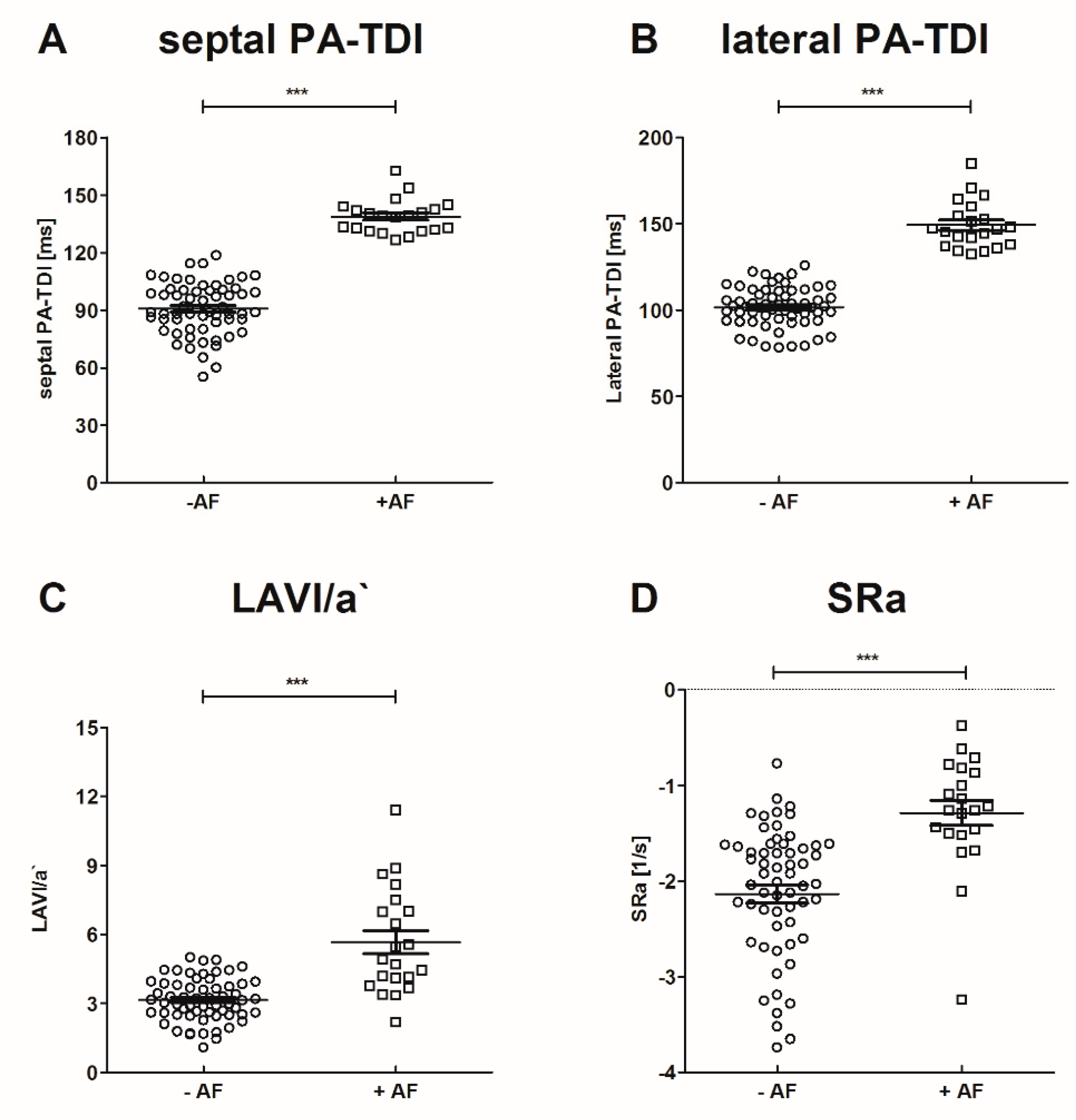
| PA-TDI septal (ms) | 90.8 ± 13.6 | 138.8 ± 8.9 | <0.001 | 85.5 ± 13.2 | 92.7 ± 17.7 | 140.4 ± 11.2 ###§§§ | 91.8 ± 12.7 $$$ | 137 ± 5.5 | |
| PA-TDI lateral (ms) | 101.6 ± 11.7 | 149.2 ± 13.7 | <0.001 | 97.3 ± 9 | 101.7 ± 9.9 | 154.5 ± 16.2 ###§§§ | 102.5 ± 12.8 $$$ | 143.4 ± 7.6 | |
| LAVI/a′ | 3.1 ± 0.9 | 5.7 ± 3.4 | <0.001 | 3.7 ± 0.6 | 3.1 ± 1.2 | 4.3 ± 1.5 § | 3.0 ± 0.9 $$$ | 7.2 ± 4.3 | |
| SRa (s−1) | −2.1 ± 0.7 | −1.3 ± 0.6 | <0.001 | −1.9 ± 0.4 | −2.0 ± 1.0 | −1.5 ± 0.7 | −2.3 ± 0.7 $$$ | −1.1 ± 0.3 | |
| Parameter | All Patients | w/o Stroke | Stroke | |||||
|---|---|---|---|---|---|---|---|---|
| −AF (n = 60) | +AF (n = 21) | p −AF vs. +AF | −AF, Young (n = 13) | −AF, Old (n = 10) | +AF (n = 11) | −AF (n= 37) | +AF (n = 10) | |
| s-ST2 (ng/mL) | 24.9 ± 12.8 | 29.3 ± 10.1 | 0.038 | 21 ± 7.12 | 22.1 ± 8.3 | 26 ± 9.3 | 24.7 ± 9 $ | 31.6 ± 11.4 |
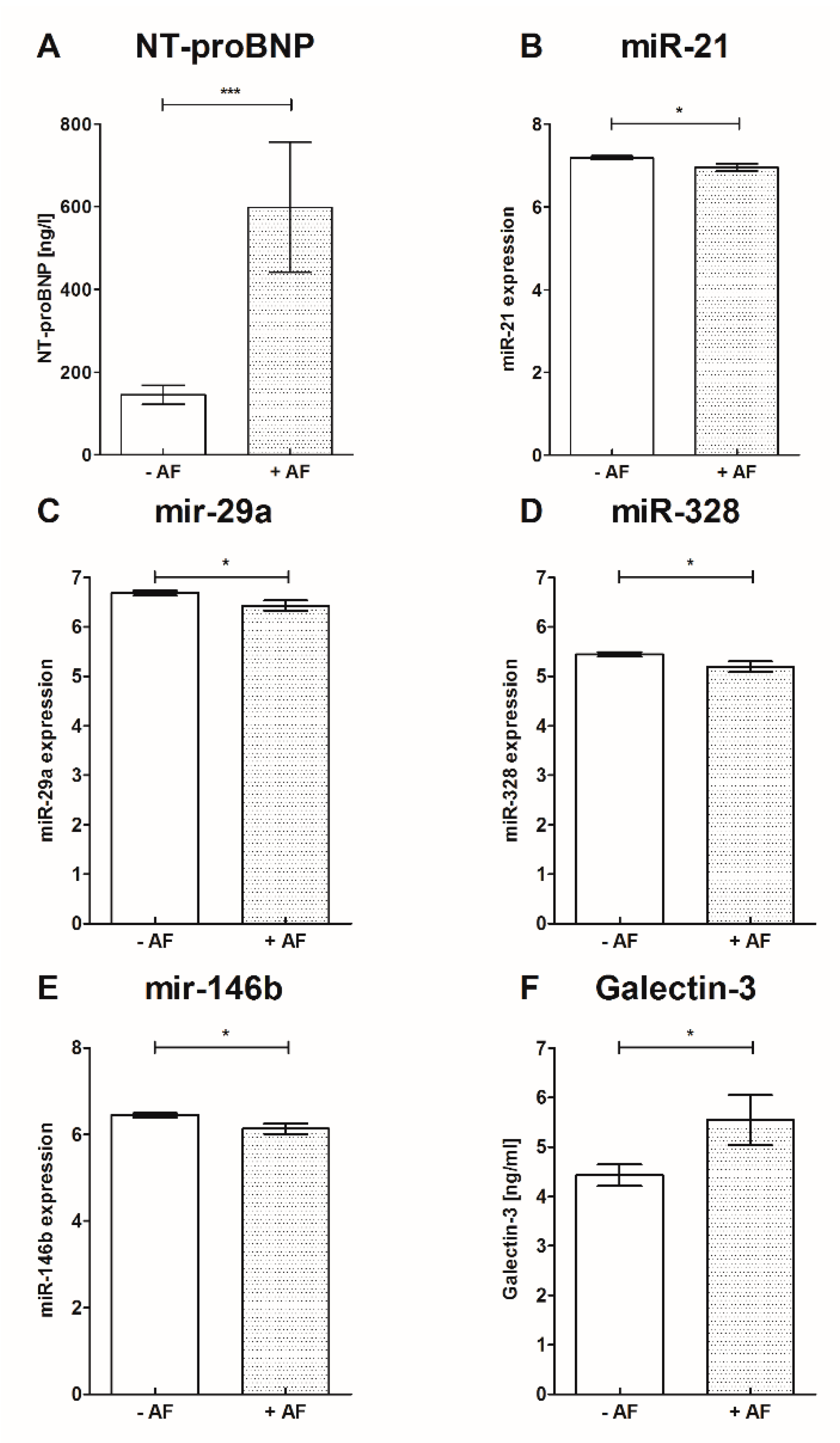
| Galectin−3 [ng/mL] | 4.4 ± 1.7 | 5.5 ± 2.3 | 0.015 | 3.8 ± 1.3 | 4.3 ± 1.4 | 4.4 ± 1.3 | 4.6 ± 1.7 $ | 6.4 ± 1.7 |
| miR−21 | 7.2 ± 0.4 | 7 ± 0.4 | 0.013 | 7.2 ± 0.3 * | 7.2 ± 0.4 | 6.9 ± 0.3 | 7.2 ± 0.4 | 7.0 ± 0.4 |
| miR−29a | 6.7 ± 0.4 | 6.4 ± 0.5 | 0.015 | 6.7 ± 0.4 | 6.7 ± 0.4 | 6.4 ± 0.4 | 6.7 ± 0.3 | 6.4 ± 0.3 |
| miR−133a | 5.7 ± 0.5 | 5.6 ± 0.6 | 0.389 | 5.9 ± 0.5 | 5.8 ± 0.5 | 5.5 ± 0.5 | 5.7 ± 0.5 | 5.6 ± 0.7 |
| miR−146b | 6.5 ± 0.4 | 6.1 ± 0.6 | 0.026 | 6.6 ± 0.4 ** | 6.3 ± 0.4 | 6.1 ± 0.5 | 6.4 ± 0.4 | 6.2 ± 0.6 |
| miR−328 | 5.5 ± 0.4 | 5.2 ± 0.5 | 0.014 | 5.5 ± 0.3 * | 5.3 ± 0.2 | 5.1 ± 0.4 | 5.4 ± 0.4 | 5.2 ± 0.6 |
| NT-proBNP (ng/L) | 75.7 (34.7–198.9) | 199.6 (96.2–1225) | <0.001 | 35.9 ± 24.9 | 90 (35.1–215) | 156.1 (77.8–1190) ## | 139.3 (49.1–302.6) $ | 346.6 (156.5–1489) |
| Parameter | Univariate Regression Analysis | Multivariate Regression Analysis | ||
|---|---|---|---|---|
| Hazard Ratio (95% Confidence Interval) | p | Hazard Ratio (95% Confidence Interval) | p | |
| s-ST2 (ng/mL) | 1.03 (0.99–1.07) | 0.179 | ||
| Galectin−3 (ng/mL) | 1.33 (1.02–1.73) | 0.04 | 1.20 (0.86–1.67) | 0.27 |
| miR−21 | 0.17 (0.04–0.74) | 0.02 | 0.16 (0.04–0.7) | 0.009 |
| miR−29a | 0.22 (0.06–0.78) | 0.02 | 1.16 (0.03–52−2) | 0.941 |
| miR−133a | 0.55 (0.2–1.45) | 0.23 | ||
| miR−146b | 0.25 (0.08–0.74) | 0.01 | 0.71 (0.01–64.3) | 0.71 |
| miR−328 | 0.21 (0.06–0.8) | 0.02 | 1.33 (0.09–20.7) | 0.44 |
| NT-proBNP (ng/L) | 1.002 (1.001–1.004) | 0.003 | 1.002 (1.001–1.004) | 0.006 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sieweke, J.-T.; Pfeffer, T.J.; Biber, S.; Chatterjee, S.; Weissenborn, K.; Grosse, G.M.; Hagemus, J.; Derda, A.A.; Berliner, D.; Lichtinghagen, R.; et al. miR−21 and NT-proBNP Correlate with Echocardiographic Parameters of Atrial Dysfunction and Predict Atrial Fibrillation. J. Clin. Med. 2020, 9, 1118. https://doi.org/10.3390/jcm9041118
Sieweke J-T, Pfeffer TJ, Biber S, Chatterjee S, Weissenborn K, Grosse GM, Hagemus J, Derda AA, Berliner D, Lichtinghagen R, et al. miR−21 and NT-proBNP Correlate with Echocardiographic Parameters of Atrial Dysfunction and Predict Atrial Fibrillation. Journal of Clinical Medicine. 2020; 9(4):1118. https://doi.org/10.3390/jcm9041118
Chicago/Turabian StyleSieweke, Jan-Thorben, Tobias Jonathan Pfeffer, Saskia Biber, Shambhabi Chatterjee, Karin Weissenborn, Gerrit M. Grosse, Jan Hagemus, Anselm A. Derda, Dominik Berliner, Ralf Lichtinghagen, and et al. 2020. "miR−21 and NT-proBNP Correlate with Echocardiographic Parameters of Atrial Dysfunction and Predict Atrial Fibrillation" Journal of Clinical Medicine 9, no. 4: 1118. https://doi.org/10.3390/jcm9041118