NIV Is not Adequate for High Intensity Endurance Exercise in COPD
 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Experimental Section
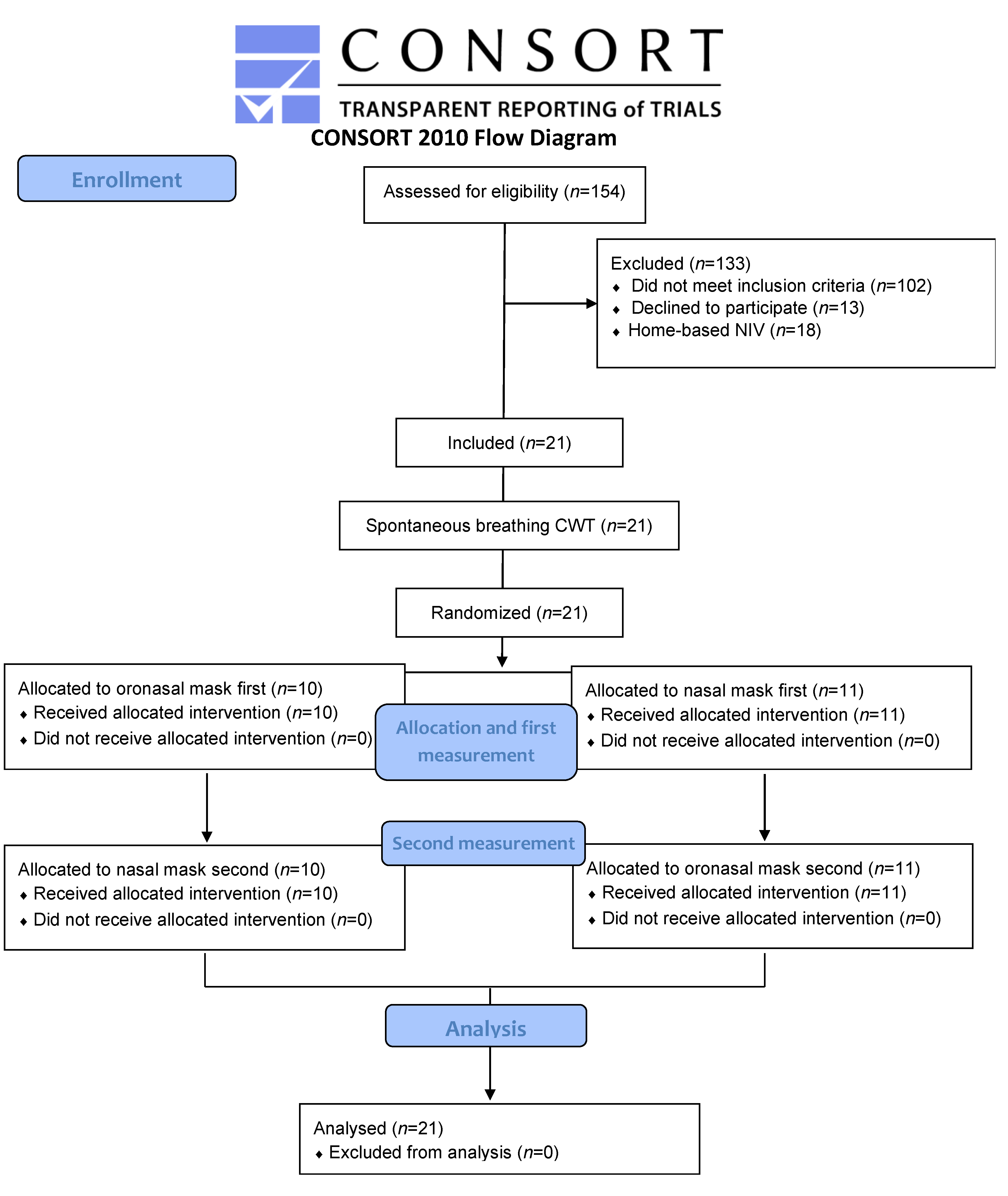
2.1. Study Design and Participants
2.2. Clinical and Functional Evaluation
2.3. Protocol
2.4. Randomization
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Patients
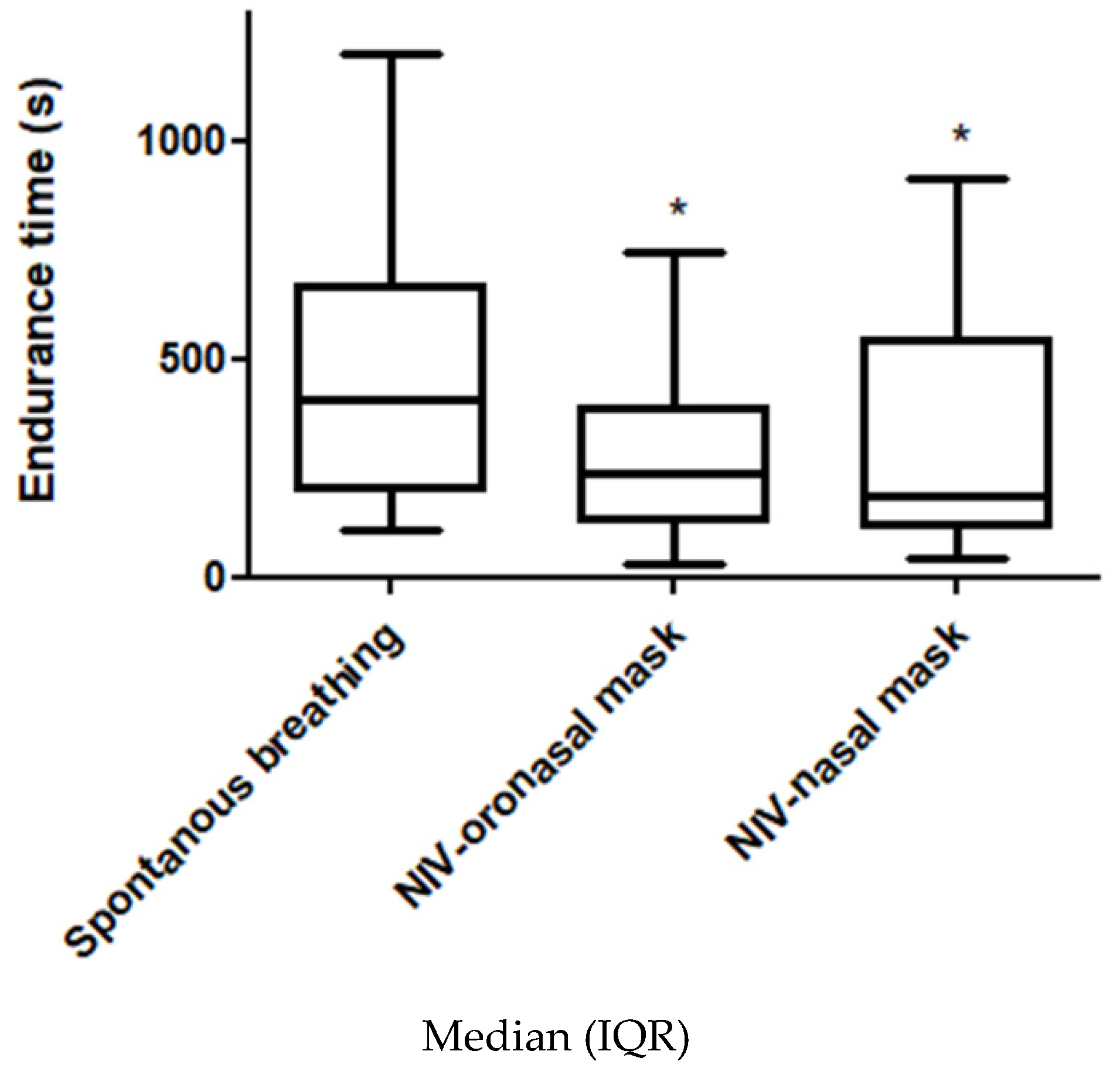
3.2. Primary Outcome
3.3. Secondary Outcomes
3.3.1. Patient-Ventilator Asynchrony
3.3.2. Flow and Pressure Tracing Analysis
3.3.3. Cardiopulmonary Outcomes
3.3.4. Interface Comfort
3.3.5. Perceived Exertion
3.3.6. Relationship between Outcomes
4. Discussion
4.1. Oronasal Interface
4.2. Nasal Interface
4.3. Implication for Practice and Research
4.4. Limits of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- Stable (on month) severe to very severe COPD referred for pulmonary rehabilitation. The clinical diagnosis of COPD was based on a ratio between forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) < 0.70;
- Age ≥ 18 years;
- FEV1 < 50% predicted;
- Eligible to home noninvasive ventilation according to [3]:
- PaCO2 ≥ 51.9 mmHg and pH > 7.35 at rest;
- Potential pregnancy;
- Under guardianship;
- Refusal to consent.
- Acute exacerbation of COPD (according to the Anthonisen’s criteria [46]) before completion of the study.
Appendix B
Appendix C
- Ineffective effort (IE): IE is characterized by an inspiratory effort not assisted by the ventilator. It can be identified as a drop of airway pressure associated with increase or decrease of airflow (if occurring during expiratory or inspiratory phase respectively) [52];
- Double-triggering (DT): DT is characterized by two mechanical cycles triggered by the patient, separated by a very short expiratory time (< 30% of mean inspiratory time) [52];
- Auto-triggering (AT): AT is characterized by the presence of mechanical cycle unrelated to patient’s spontaneous breathing [52];
- Mean differential flow (Fdiff) = Fmax, mean − Fini, mean;
- Mean differential pressure (Pdiff) = Pmax, mean − Pmin, mean.
References
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- McCarthy, B.; Casey, D.; Devane, D.; Murphy, K.; Murphy, E.; Lacasse, Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2015, 2, CD003793. [Google Scholar] [CrossRef] [PubMed]
- Kohnlein, T.; Windisch, W.; Kohler, D.; Drabik, A.; Geiseler, J.; Hartl, S.; Karg, O.; Laier-Groeneveld, G.; Nava, S.; Schonhofer, B.; et al. Non-Invasive positive pressure ventilation for the treatment of severe stable chronic obstructive pulmonary disease: A prospective, multicentre, randomised, controlled clinical trial. Lancet Respir. Med. 2014, 2, 698–705. [Google Scholar] [CrossRef]
- Murphy, P.B.; Rehal, S.; Arbane, G.; Bourke, S.; Calverley, P.M.A.; Crook, A.M.; Dowson, L.; Duffy, N.; Gibson, G.J.; Hughes, P.D.; et al. Effect of Home Noninvasive Ventilation With Oxygen Therapy vs Oxygen Therapy Alone on Hospital Readmission or Death After an Acute COPD Exacerbation: A Randomized Clinical Trial. JAMA 2017, 317, 2177–2186. [Google Scholar] [CrossRef] [PubMed]
- Marquez-Martin, E.; Ruiz, F.O.; Ramos, P.C.; Lopez-Campos, J.L.; Azcona, B.V.; Cortes, E.B. Randomized trial of non-Invasive ventilation combined with exercise training in patients with chronic hypercapnic failure due to chronic obstructive pulmonary disease. Respir. Med. 2014, 108, 1741–1751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duiverman, M.L.; Wempe, J.B.; Bladder, G.; Jansen, D.F.; Kerstjens, H.A.; Zijlstra, J.G.; Wijkstra, P.J. Nocturnal non-Invasive ventilation in addition to rehabilitation in hypercapnic patients with COPD. Thorax 2008, 63, 1052–1057. [Google Scholar] [CrossRef] [Green Version]
- Menadue, C.; Piper, A.J.; van ‘t Hul, A.J.; Wong, K.K. Non-Invasive ventilation during exercise training for people with chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2014, 5, CD007714. [Google Scholar] [CrossRef] [Green Version]
- Vitacca, M.; Ambrosino, N. Non-Invasive Ventilation as an Adjunct to Exercise Training in Chronic Ventilatory Failure: A Narrative Review. Respir. Int. Rev. Thorac. Dis. 2018, 1–9. [Google Scholar] [CrossRef]
- Maltais, F.; LeBlanc, P.; Jobin, J.; Berube, C.; Bruneau, J.; Carrier, L.; Breton, M.J.; Falardeau, G.; Belleau, R. Intensity of training and physiologic adaptation in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 1997, 155, 555–561. [Google Scholar] [CrossRef]
- Maltais, F.; Reissmann, H.; Gottfried, S.B. Pressure support reduces inspiratory effort and dyspnea during exercise in chronic airflow obstruction. Am. J. Respir. Crit. Care Med. 1995, 151, 1027–1033. [Google Scholar] [CrossRef]
- Borghi-Silva, A.; Oliveira, C.C.; Carrascosa, C.; Maia, J.; Berton, D.C.; Queiroga, F., Jr.; Ferreira, E.M.; Almeida, D.R.; Nery, L.E.; Neder, J.A.; et al. Respiratory muscle unloading improves leg muscle oxygenation during exercise in patients with COPD. Thorax 2008, 63, 910–915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koopman, M.; Spruit, M.A.; Franssen, F.M.E.; Delbressine, J.; Wouters, E.F.M.; Mathew, D.; Vink, A.; Vanfleteren, L. Effects of Non-Invasive Ventilation Combined with Oxygen Supplementation on Exercise Performance in COPD Patients with Static Lung Hyperinflation and Exercise-Induced Oxygen Desaturation: A Single Blind, Randomized Cross-Over Trial. J. Clin. Med. 2019, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anekwe, D.; de Marchie, M.; Spahija, J. Effects of Pressure Support Ventilation May Be Lost at High Exercise Intensities in People with COPD. COPD 2017, 14, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Société de Pneumologie de Langue Française. Recommendation for the clinical practice management of COPD. Rev. des Mal. Respir. 2010, 27, 522–548. [Google Scholar] [CrossRef]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.; et al. An official American Thoracic Society/European Respiratory Society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef]
- Reuveny, R.; Ben-Dov, I.; Gaides, M.; Reichert, N. Ventilatory support during training improves training benefit in severe chronic airway obstruction. Isr. Med Assoc. J. 2005, 7, 151–155. [Google Scholar] [CrossRef]
- Johnson, J.E.; Gavin, D.J.; Adams-Dramiga, S. Effects of training with heliox and noninvasive positive pressure ventilation on exercise ability in patients with severe COPD. Chest 2002, 122, 464–472. [Google Scholar] [CrossRef]
- Bianchi, L.; Foglio, K.; Porta, R.; Baiardi, R.; Vitacca, M.; Ambrosino, N. Lack of additional effect of adjunct of assisted ventilation to pulmonary rehabilitation in mild COPD patients. Respir. Med. 2002, 96, 359–367. [Google Scholar] [CrossRef] [Green Version]
- van ‘t Hul, A.; Gosselink, R.; Hollander, P.; Postmus, P.; Kwakkel, G. Training with inspiratory pressure support in patients with severe COPD. Eur. Respir. J. 2006, 27, 65–72. [Google Scholar] [CrossRef]
- van ‘t Hul, A.; Gosselink, R.; Hollander, P.; Postmus, P.; Kwakkel, G. Acute effects of inspiratory pressure support during exercise in patients with COPD. Eur. Respir. J. 2004, 23, 34–40. [Google Scholar] [CrossRef] [Green Version]
- Menadue, C.; Alison, J.A.; Piper, A.J.; Wong, K.K.; Hollier, C.; Ellis, E.R. High- and low-Level pressure support during walking in people with severe kyphoscoliosis. Eur. Respir. J. 2010, 36, 370–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nava, S.; Ambrosino, N.; Rubini, F.; Fracchia, C.; Rampulla, C.; Torri, G.; Calderini, E. Effect of nasal pressure support ventilation and external PEEP on diaphragmatic activity in patients with severe stable COPD. Chest 1993, 103, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Dolmage, T.E.; Goldstein, R.S. Proportional assist ventilation and exercise tolerance in subjects with COPD. Chest 1997, 111, 948–954. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic Society; American College of Chest Physicians. ATS/ACCP Statement on cardiopulmonary exercise testing. Am. J. Respir. Crit. Care Med. 2003, 167, 211–277. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Storre, J.H.; Steurer, B.; Kabitz, H.J.; Dreher, M.; Windisch, W. Transcutaneous PCO2 monitoring during initiation of noninvasive ventilation. Chest 2007, 132, 1810–1816. [Google Scholar] [CrossRef]
- Puente-Maestu, L.; Villar, F.; de Miguel, J.; Stringer, W.W.; Sanz, P.; Sanz, M.L.; de Pedro, J.G.; Martinez-Abad, Y. Clinical relevance of constant power exercise duration changes in COPD. Eur. Respir. J. 2009, 34, 340–345. [Google Scholar] [CrossRef] [Green Version]
- van ‘t Hul, A.; Kwakkel, G.; Gosselink, R. The acute effects of noninvasive ventilatory support during exercise on exercise endurance and dyspnea in patients with chronic obstructive pulmonary disease: A systematic review. J. Cardiopulm. Rehabil. 2002, 22, 290–297. [Google Scholar] [CrossRef]
- Gloeckl, R.; Andrianopoulos, V.; Stegemann, A.; Oversohl, J.; Schneeberger, T.; Schoenheit-Kenn, U.; Hitzl, W.; Dreher, M.; Rembert Koczulla, A.; Kenn, K.; et al. High-Pressure non-Invasive ventilation during exercise in COPD patients with chronic hypercapnic respiratory failure: A randomized, controlled, cross-Over trial. Respirology 2018, 24, 254–261. [Google Scholar] [CrossRef]
- Vogiatzis, I.; Chynkiamis, N.; Armstrong, M.; Lane, N.; Hartley, T.; Gray, W.; Bourke, S. Intermittent Use of Portable NIV Increases Exercise Tolerance in COPD: A Randomised, Cross-Over Trial. J. Clin. Med. 2019, 8, 94. [Google Scholar] [CrossRef] [Green Version]
- Moga, A.M.; de Marchie, M.; Saey, D.; Spahija, J. Bi-Level Positive Airway Pressure (BiPAP) with standard exhalation valve does not improve maximum exercise capacity in patients with COPD. COPD 2015, 12, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Highcock, M.P.; Shneerson, J.M.; Smith, I.E. Increased ventilation with NiIPPV does not necessarily improve exercise capacity in COPD. Eur. Respir. J. 2003, 22, 100–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricci, C.; Terzoni, S.; Gaeta, M.; Sorgente, A.; Destrebecq, A.; Gigliotti, F. Physical training and noninvasive ventilation in COPD patients: A meta-analysis. Respir. Care 2014, 59, 709–717. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, D.E.; Revill, S.M.; Webb, K.A. Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2001, 164, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Ou, Y.E.; Lin, Z.M.; Hua, D.M.; Jiang, Y.; Huo, Y.T.; Luo, Q.; Chen, R.C. Evaluation of carbon dioxide rebreathing during exercise assisted by noninvasive ventilation with plateau exhalation valve. Int. journal Chronic Obstr. Pulm. Dis. 2017, 12, 291–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, C.C.; Carrascosa, C.R.; Borghi-Silva, A.; Berton, D.C.; Queiroga, F., Jr.; Ferreira, E.M.; Nery, L.E.; Neder, J.A. Influence of respiratory pressure support on hemodynamics and exercise tolerance in patients with COPD. Eur. J. Appl. Physiol. 2010, 109, 681–689. [Google Scholar] [CrossRef] [PubMed]
- Costes, F.; Agresti, A.; Court-Fortune, I.; Roche, F.; Vergnon, J.M.; Barthelemy, J.C. Noninvasive ventilation during exercise training improves exercise tolerance in patients with chronic obstructive pulmonary disease. J. Cardiopulm. Rehabil. 2003, 23, 307–313. [Google Scholar] [CrossRef]
- Marrara, K.T.; Di Lorenzo, V.A.P.; Jaenisch, R.B.; Cabiddu, R.; de Oliveira Sato, T.; Mendes, R.G.; Oliveira, C.R.; Costa, D.; Borghi-Silva, A. Noninvasive Ventilation as an Important Adjunct to an Exercise Training Program in Subjects With Moderate to Severe COPD. Respir. Care 2018. [Google Scholar] [CrossRef] [Green Version]
- Vitacca, M.; Bianchi, L.; Zanotti, E.; Vianello, A.; Barbano, L.; Porta, R.; Clini, E. Assessment of physiologic variables and subjective comfort under different levels of pressure support ventilation. Chest 2004, 126, 851–859. [Google Scholar] [CrossRef] [Green Version]
- Bolton, C.E.; Bevan-Smith, E.F.; Blakey, J.D.; Crowe, P.; Elkin, S.L.; Garrod, R.; Greening, N.J.; Heslop, K.; Hull, J.H.; Man, W.D.; et al. British Thoracic Society guideline on pulmonary rehabilitation in adults. Thorax 2013, 68, ii1–ii30. [Google Scholar] [CrossRef] [Green Version]
- Nici, L.; Donner, C.; Wouters, E.; Zuwallack, R.; Ambrosino, N.; Bourbeau, J.; Carone, M.; Celli, B.; Engelen, M.; Fahy, B.; et al. American Thoracic Society/European Respiratory Society statement on pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2006, 173, 1390–1413. [Google Scholar] [CrossRef]
- Casaburi, R.; Patessio, A.; Ioli, F.; Zanaboni, S.; Donner, C.F.; Wasserman, K. Reductions in exercise lactic acidosis and ventilation as a result of exercise training in patients with obstructive lung disease. Am. Rev. Respir. Dis. 1991, 143, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Gimenez, M.; Servera, E.; Vergara, P.; Bach, J.R.; Polu, J.M. Endurance training in patients with chronic obstructive pulmonary disease: A comparison of high versus moderate intensity. Arch. Phys. Med. Rehabil. 2000, 81, 102–109. [Google Scholar] [CrossRef]
- Borel, J.C.; Sabil, A.; Janssens, J.P.; Couteau, M.; Boulon, L.; Levy, P.; Pepin, J.L. Intentional leaks in industrial masks have a significant impact on efficacy of bilevel noninvasive ventilation: A bench test study. Chest 2009, 135, 669–677. [Google Scholar] [CrossRef] [PubMed]
- Contal, O.; Vignaux, L.; Combescure, C.; Pepin, J.L.; Jolliet, P.; Janssens, J.P. Monitoring of noninvasive ventilation by built-In software of home bilevel ventilators: A bench study. Chest 2012, 141, 469–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anthonisen, N.R.; Manfreda, J.; Warren, C.P.; Hershfield, E.S.; Harding, G.K.; Nelson, N.A. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Ann. Intern. Med. 1987, 106, 196–204. [Google Scholar] [CrossRef]
- Quanjer, P.H.; Tammeling, G.J.; Cotes, J.E.; Pedersen, O.F.; Peslin, R.; Yernault, J.C. Lung volumes and forced ventilatory flows. Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory Society. Eur. Respir. J. Suppl. 1993, 16, 5–40. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-Minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Puente-Maestu, L.; Palange, P.; Casaburi, R.; Laveneziana, P.; Maltais, F.; Neder, J.A.; O’Donnell, D.E.; Onorati, P.; Porszasz, J.; Rabinovich, R.; et al. Use of exercise testing in the evaluation of interventional efficacy: An official ERS statement. Eur. Respir. J. 2016, 47, 429–460. [Google Scholar] [CrossRef]
- Vignaux, L.; Vargas, F.; Roeseler, J.; Tassaux, D.; Thille, A.W.; Kossowsky, M.P.; Brochard, L.; Jolliet, P. Patient-Ventilator asynchrony during non-Invasive ventilation for acute respiratory failure: A multicenter study. Intensive Care Med. 2009, 35, 840–846. [Google Scholar] [CrossRef]
- Thille, A.W.; Rodriguez, P.; Cabello, B.; Lellouche, F.; Brochard, L. Patient-Ventilator asynchrony during assisted mechanical ventilation. Intensive Care Med. 2006, 32, 1515–1522. [Google Scholar] [CrossRef] [PubMed]
- Garofalo, E.; Bruni, A.; Pelaia, C.; Liparota, L.; Lombardo, N.; Longhini, F.; Navalesi, P. Recognizing, quantifying and managing patient-ventilator asynchrony in invasive and noninvasive ventilation. Expert Rev. Respir. Med. 2018, 12, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Bermejo, J.; Janssens, J.P.; Rabec, C.; Perrin, C.; Lofaso, F.; Langevin, B.; Carlucci, A.; Lujan, M.; Somno, N.I.V.G. Framework for patient-Ventilator asynchrony during long-term non-Invasive ventilation. Thorax 2019, 74, 715–717. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable, (Units) | Participants (n = 21) |
|---|---|
| Female (n) | 9 (43) a |
| Age (years) | 58.9(10.7) b |
| Height (cm) | 170 (8.9) b |
| Body mass (kg) | 66.1 (11.9) b |
| BMI (kg/m²) | 22.8 (3) b |
| FEV1 (L) | 0.9 (0.8–1.3) c |
| FEV1 (%) | 35.3 (8.3) b |
| FVC (L) | 2.6 (0.8) b |
| FEV1/FVC (% ratio) | 40.2 (8.8) b |
| RV (L) | 4.5 (0.9) b |
| RV (%) | 216 (43) b |
| TLC (L) | 7.4 (1.3) b |
| RV/TLC | 0.6 (0.1) b |
| IC (L) | 1.7 (0.6) b |
| IC (%) | 65 (17) b |
| VO2 peak (mL/kg/min) | 12.1 (2.8) b |
| Arterial blood gas | 50 (40–70) c |
| PaO2 (mmHg) | 67.5 (12) b |
| PaCO2 (mmHg) | 38.3 (4.5) b |
| pH | 7.44 (0) b |
| HCO3- (mmol/L) | 24.8 (23–25) c |
| Wmax (W) | 50 (40–70) c |
| 6MWT (m) | 413.5 (99.1) b |
| LTO (n) | 5 (24) a |
| BODE | 4.3 (1.7) b |
| Event (%) | Interface | Between-Group Comparison | |
|---|---|---|---|
| Oronasal Mask (n = 21) | Nasal Mask (n = 21) | p | |
| Normal cycles | 95.5 (91.6–97.0) | 82.5 (47.1–95.5) | p < 0.01 |
| Ineffective triggerings | 0 (0–0.1) | 2.1 (0–21.5) | p < 0.01 |
| Double-triggerings | 0.2 (0–1.6) | 2.7 (0.7–8.6) | p < 0.01 |
| Auto-triggerings | 1.7 (0–3.6) | 1.7 (0.4–2.5) | NS |
| Premature cyclings | 0.2 (0.0–1.9) | 0.9 (0.0–6.9) | NS |
| Delayed cyclings | 0.0 (0.0–0.8) | 0.0 (0.0–2.3) | NS |
| NDP | 96.6 (94.8–98.3) | 87.2 (68.4–96.8) | p < 0.01 |
| Total major asynchrony events | 3.4 (1.7–5.2) | 12.8 (3.2–31.6) | p < 0.01 |
| Variables, (Units) | Constant Workload Exercise Testing | Between-Group Comparison | ||
|---|---|---|---|---|
| Spontaneous Breathing (n = 21) | Oronasal Mask (n = 21) | Nasal Mask (n = 21) | p | |
| Iso-time | ||||
| Heart rate (bpm) | 111.6 (17) | 118.2 (13.4)* | 116.5 (11.1) | p < 0.05 |
| SpO2 (%) | 93.1 (3) | 93.5 (2.4) | 93.4 (2.4) | NS |
| TcPCO2 (mmHg) | 39.1 (4.4) | 40.2 (3.2) | 39.9 (3.9) | NS |
| Respiratory rate (cpm) | 27.6 (6.7) | 24.7 (8.6) | NS | |
| Vt (mL) | 1333.6 (486.2) | 784.3 (486.2) | p < 0.01 | |
| Unintentional leaks (L/min) | 12.2 (9.6) | 28.3 (29.8) | p < 0.03 | |
| Time limit | ||||
| Heart rate (bpm) | 121.1 (15.3) | 120.5 (13.7) | 120 (13.7) | NS |
| SpO2 (%) | 92.8 (3.2) | 93.1 (2.6) | 93.1 (2.9) | NS |
| TcPCO2 (mmHg) | 38.5 (4.5) | 39.5 (2.9) | 40 (4) | NS |
| Respiratory rate (cpm) | 30.3 (5.4) | 24.9 (9.6) | p < 0.01 | |
| Vt (mL) | 1225.6 (494.2) | 828.3 (506.2) | p < 0.01 | |
| Unintentional leaks (L/min) | 11.7 (9.6) | 28.9 (31.3) | p < 0.04 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonnevie, T.; Gravier, F.-E.; Fresnel, E.; Kerfourn, A.; Medrinal, C.; Prieur, G.; Combret, Y.; Muir, J.-F.; Cuvelier, A.; Debeaumont, D.; et al. NIV Is not Adequate for High Intensity Endurance Exercise in COPD. J. Clin. Med. 2020, 9, 1054. https://doi.org/10.3390/jcm9041054
Bonnevie T, Gravier F-E, Fresnel E, Kerfourn A, Medrinal C, Prieur G, Combret Y, Muir J-F, Cuvelier A, Debeaumont D, et al. NIV Is not Adequate for High Intensity Endurance Exercise in COPD. Journal of Clinical Medicine. 2020; 9(4):1054. https://doi.org/10.3390/jcm9041054
Chicago/Turabian StyleBonnevie, Tristan, Francis-Edouard Gravier, Emeline Fresnel, Adrien Kerfourn, Clément Medrinal, Guillaume Prieur, Yann Combret, Jean-François Muir, Antoine Cuvelier, David Debeaumont, and et al. 2020. "NIV Is not Adequate for High Intensity Endurance Exercise in COPD" Journal of Clinical Medicine 9, no. 4: 1054. https://doi.org/10.3390/jcm9041054