Neoadjuvant Chemoradiotherapy and Larynx-Preserving Surgery for Cervical Esophageal Cancer


Abstract
:1. Introduction
2. Experimental Section
2.1. Subjects
2.2. Radiotherapy
2.3. Chemotherapy
2.4. Acute Toxicity and Clinical Response Assessment
2.5. Surgery and Pathological Response Assessment
2.6. Follow-Up
2.7. Statistical Analysis
3. Results
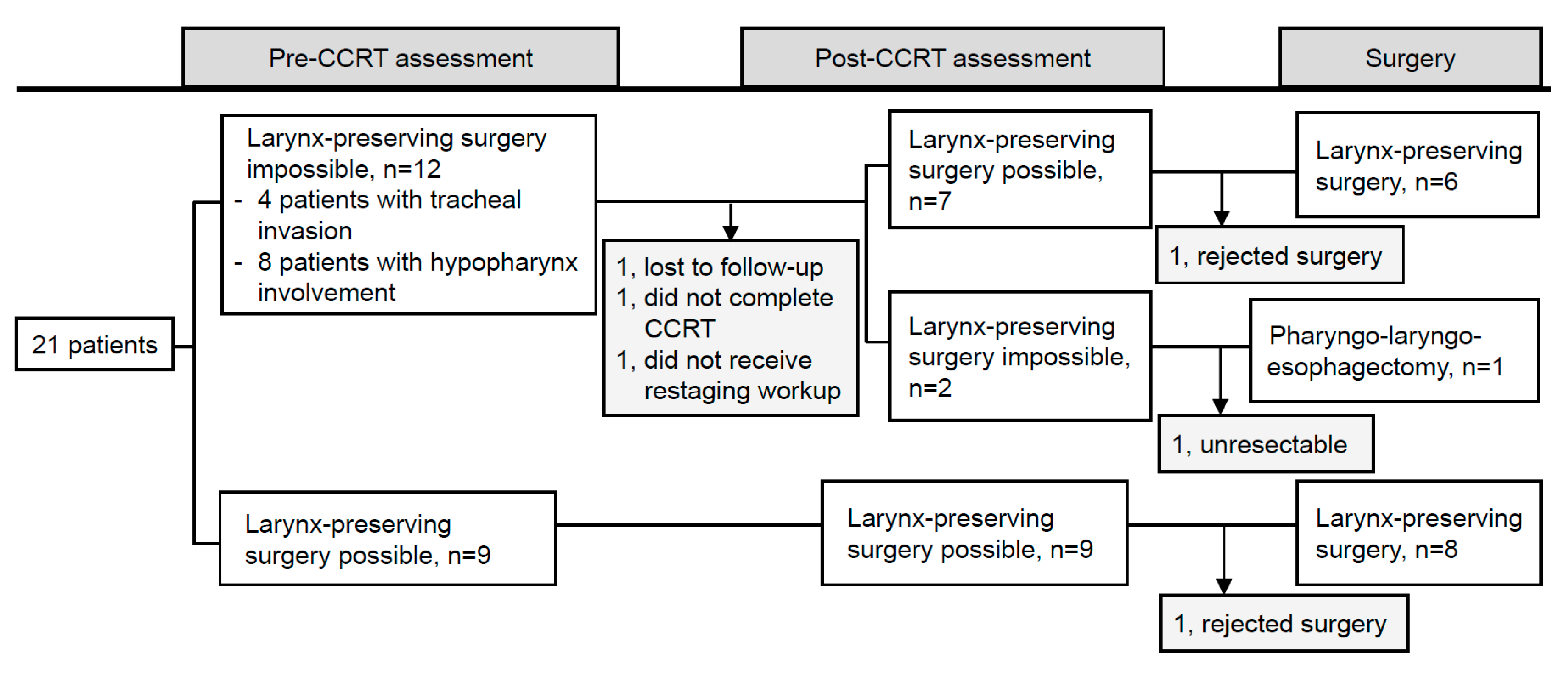
3.1. Patient Characteristics
3.2. Acute Toxicity of CCRT
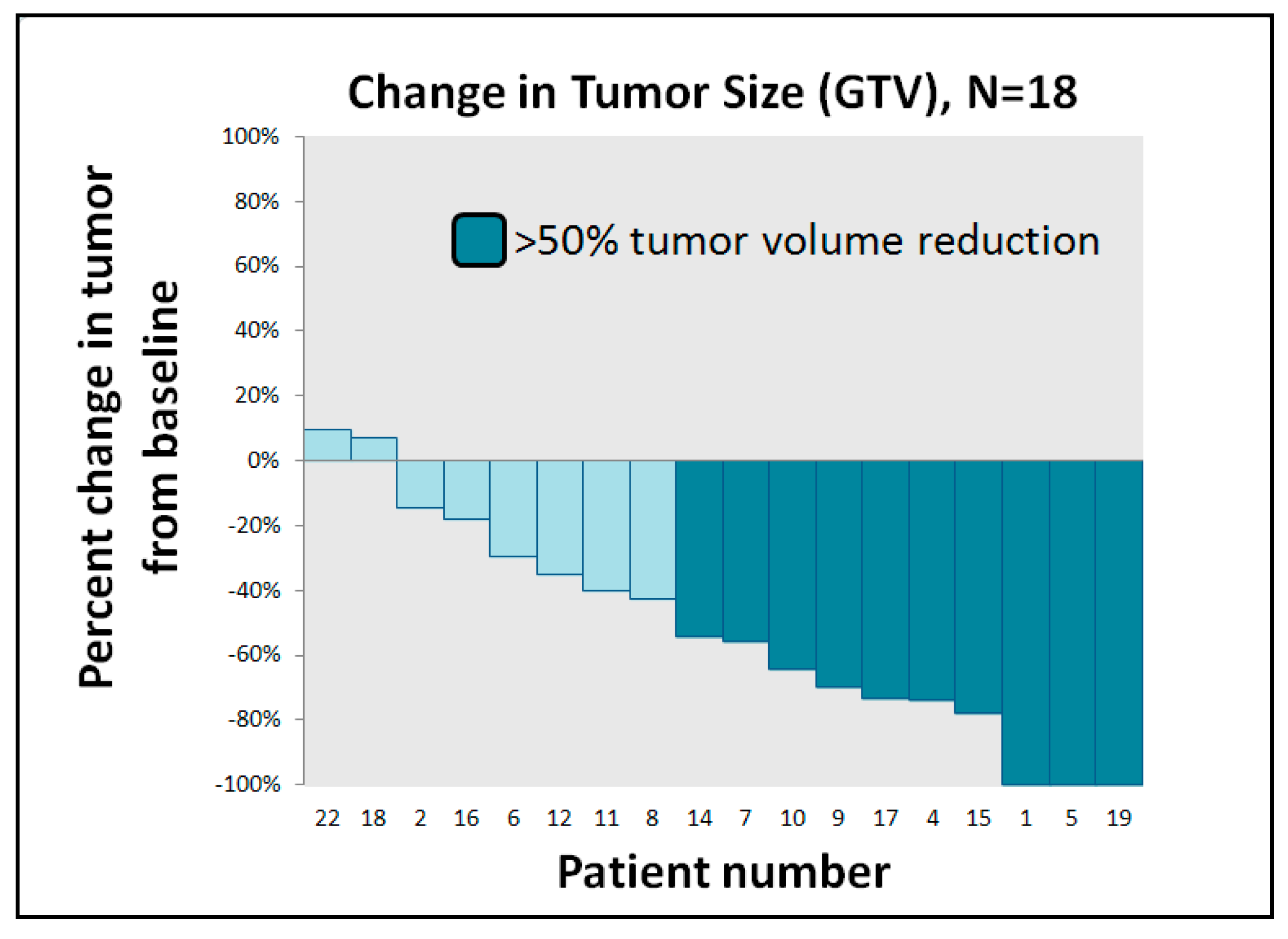
3.3. Clinical and Pathological Treatment Response
3.4. Surgical Complications
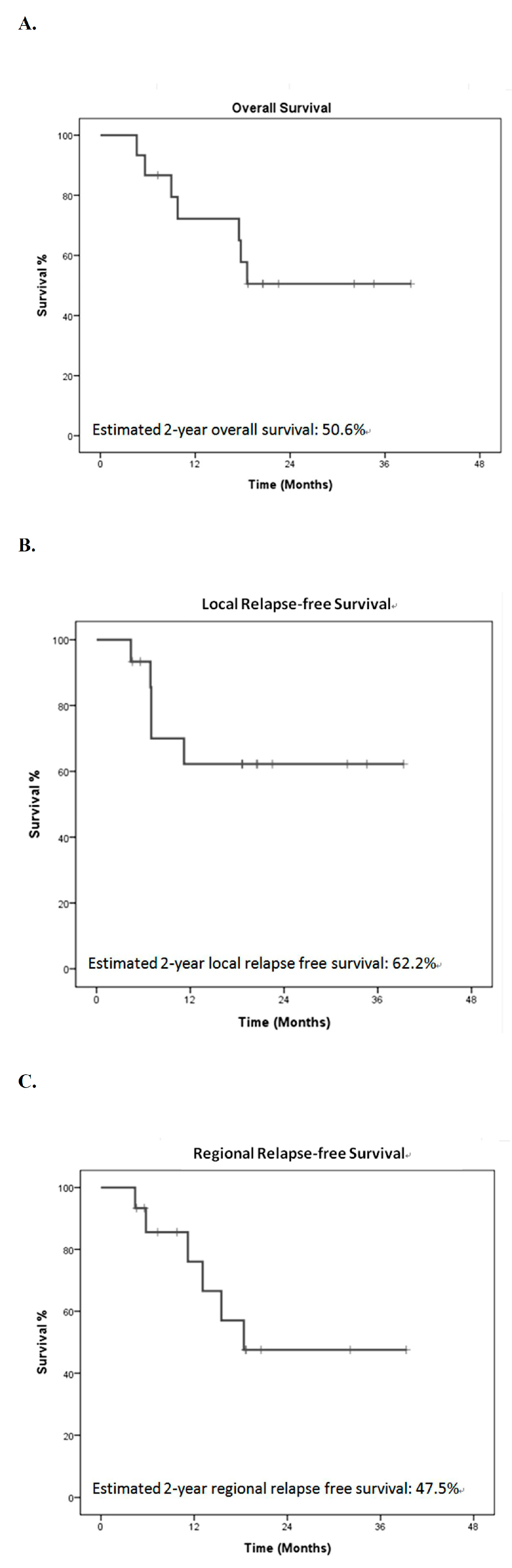
3.5. Treatment Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2017. Ca A Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.J.; Harris, A.; Gillette, A.; Munoz, L.; Kashima, H. Carcinoma of the cervical esophagus: Diagnosis, management, and results. South. Med. J. 1984, 77, 1365–1367. [Google Scholar] [CrossRef] [PubMed]
- Grass, G.D.; Cooper, S.L.; Armeson, K.; Garrett-Mayer, E.; Sharma, A. Cervical esophageal cancer: A population-based study. Head Neck 2015, 37, 808–814. [Google Scholar] [CrossRef]
- Cao, C.N.; Luo, J.W.; Gao, L.; Xu, G.Z.; Yi, J.L.; Huang, X.D.; Li, S.Y.; Xiao, J.P.; Liu, S.Y.; Xu, Z.G.; et al. Primary radiotherapy compared with primary surgery in cervical esophageal cancer. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 918–926. [Google Scholar] [CrossRef] [Green Version]
- Chou, S.H.; Li, H.P.; Lee, J.Y.; Huang, M.F.; Lee, C.H.; Lee, K.W. Radical resection or chemoradiotherapy for cervical esophageal cancer? World J. Surg. 2010, 34, 1832–1839. [Google Scholar] [CrossRef]
- Bardini, R.; Ruol, A.; Peracchia, A. Therapeutic options for cancer of the hypopharynx and cervical oesophagus. Ann. Chir. Et Gynaecol. 1995, 84, 202–207. [Google Scholar]
- Ong, G.B.; Lee, T.C. Pharyngogastric anastomosis after oesophago-pharyngectomy for carcinoma of the hypopharynx and cervical oesophagus. Br. J. Surg. 1960, 48, 193–200. [Google Scholar] [CrossRef]
- Triboulet, J.P.; Mariette, C.; Chevalier, D.; Amrouni, H. Surgical management of carcinoma of the hypopharynx and cervical esophagus: Analysis of 209 cases. Arch. Surg. 2001, 136, 1164–1170. [Google Scholar] [CrossRef] [Green Version]
- Lordick, F.; Mariette, C.; Haustermans, K.; Obermannova, R.; Arnold, D. Oesophageal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med Oncol. 2016, 27, v50–v57. [Google Scholar] [CrossRef]
- Stuschke, M.; Stahl, M.; Wilke, H.; Walz, M.K.; Oldenburg, A.R.; Stuben, G.; Jahnke, K.; Seeber, S.; Sack, H. Induction chemotherapy followed by concurrent chemotherapy and high-dose radiotherapy for locally advanced squamous cell carcinoma of the cervical oesophagus. Oncology 1999, 57, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Tong, D.K.; Law, S.; Kwong, D.L.; Wei, W.I.; Ng, R.W.; Wong, K.H. Current management of cervical esophageal cancer. World J. Surg. 2011, 35, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K.; Murakami, M.; Okamoto, Y.; Okuno, Y.; Nakajima, T.; Kusumi, F.; Takakuwa, H.; Matsusue, S. Treatment results of radiotherapy for carcinoma of the cervical esophagus. Acta Oncol. (Stockh. Swed.) 2006, 45, 1120–1125. [Google Scholar] [CrossRef]
- Zhang, P.; Xi, M.; Zhao, L.; Qiu, B.; Liu, H.; Hu, Y.H.; Liu, M.Z. Clinical efficacy and failure pattern in patients with cervical esophageal cancer treated with definitive chemoradiotherapy. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2015, 116, 257–261. [Google Scholar] [CrossRef]
- Cao, C.; Luo, J.; Gao, L.; Xu, G.; Yi, J.; Huang, X.; Wang, K.; Zhang, S.; Qu, Y.; Li, S.; et al. Definitive radiotherapy for cervical esophageal cancer. Head Neck 2015, 37, 151–155. [Google Scholar] [CrossRef]
- Cao, C.N.; Luo, J.W.; Gao, L.; Xu, G.Z.; Yi, J.L.; Huang, X.D.; Wang, K.; Zhang, S.P.; Qu, Y.; Li, S.Y.; et al. Intensity-modulated radiotherapy for cervical esophageal squamous cell carcinoma: Clinical outcomes and patterns of failure. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 741–747. [Google Scholar] [CrossRef]
- Li, H.X.; Liu, J.; Cheng, Y.; Liu, M.N.; Fang, W.T.; Lv, C.X. Concurrent chemoradiotherapy for cervical esophageal squamous cell carcinoma: Treatment results from a prospective observational study. Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus 2018, 31. [Google Scholar] [CrossRef]
- Ott, K.; Lordick, F.; Molls, M.; Bartels, H.; Biemer, E.; Siewert, J.R. Limited resection and free jejunal graft interposition for squamous cell carcinoma of the cervical oesophagus. Br. J. Surg. 2009, 96, 258–266. [Google Scholar] [CrossRef]
- Tepper, J.; Krasna, M.J.; Niedzwiecki, D.; Hollis, D.; Reed, C.E.; Goldberg, R.; Kiel, K.; Willett, C.; Sugarbaker, D.; Mayer, R. Phase III trial of trimodality therapy with cisplatin, fluorouracil, radiotherapy, and surgery compared with surgery alone for esophageal cancer: CALGB 9781. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2008, 26, 1086–1092. [Google Scholar] [CrossRef] [Green Version]
- Sjoquist, K.M.; Burmeister, B.H.; Smithers, B.M.; Zalcberg, J.R.; Simes, R.J.; Barbour, A.; Gebski, V. Survival after neoadjuvant chemotherapy or chemoradiotherapy for resectable oesophageal carcinoma: An updated meta-analysis. Lancet. Oncol. 2011, 12, 681–692. [Google Scholar] [CrossRef]
- Shapiro, J.; van Lanschot, J.J.B.; Hulshof, M.; van Hagen, P.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.L.; van Laarhoven, H.W.M.; Nieuwenhuijzen, G.A.P.; Hospers, G.A.P.; Bonenkamp, J.J.; et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): Long-term results of a randomised controlled trial. Lancet. Oncol. 2015, 16, 1090–1098. [Google Scholar] [CrossRef]
- Hofstetter, W.; Swisher, S.G.; Correa, A.M.; Hess, K.; Putnam, J.B., Jr.; Ajani, J.A.; Dolormente, M.; Francisco, R.; Komaki, R.R.; Lara, A.; et al. Treatment outcomes of resected esophageal cancer. Ann. Surg. 2002, 236, 376–384, discussion 384-375. [Google Scholar] [CrossRef] [PubMed]
- Mulligan, E.D.; Dunne, B.; Griffin, M.; Keeling, N.; Reynolds, J.V. Margin involvement and outcome in oesophageal carcinoma: A 10-year experience in a specialist unit. Eur. J. Surg. Oncol. 2004, 30, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Shuangba, H.; Jingwu, S.; Yinfeng, W.; Yanming, H.; Qiuping, L.; Xianguang, L.; Weiqing, X.; Shengjun, W.; Zhenkun, Y. Complication following gastric pull-up reconstruction for advanced hypopharyngeal or cervical esophageal carcinoma: A 20-year review in a Chinese institute. Am. J. Otolaryngol. 2011, 32, 275–278. [Google Scholar] [CrossRef]
- Miyata, H.; Yamasaki, M.; Takahashi, T.; Kurokawa, Y.; Nakajima, K.; Takiguchi, S.; Mori, M.; Doki, Y. Larynx-preserving limited resection and free jejunal graft for carcinoma of the cervical esophagus. World J. Surg. 2013, 37, 551–557. [Google Scholar] [CrossRef]
- Sun, F.; Li, X.; Lei, D.; Jin, T.; Liu, D.; Zhao, H.; Yang, Q.; Li, G.; Pan, X. Surgical management of cervical esophageal carcinoma with larynx preservation and reconstruction. Int. J. Clin. Exp. Med. 2014, 7, 2771–2778. [Google Scholar]
- Kadota, H.; Sakuraba, M.; Kimata, Y.; Hayashi, R.; Ebihara, S.; Kato, H. Larynx-preserving esophagectomy and jejunal transfer for cervical esophageal carcinoma. Laryngoscope 2009, 119, 1274–1280. [Google Scholar] [CrossRef]
- Cooper, J.S.; Guo, M.D.; Herskovic, A.; Macdonald, J.S.; Martenson, J.A., Jr.; Al-Sarraf, M.; Byhardt, R.; Russell, A.H.; Beitler, J.J.; Spencer, S.; et al. Chemoradiotherapy of locally advanced esophageal cancer: Long-term follow-up of a prospective randomized trial (RTOG 85-01). Radiation Therapy Oncology Group. JAMA 1999, 281, 1623–1627. [Google Scholar] [CrossRef]
- Burmeister, B.H.; Dickie, G.; Smithers, B.M.; Hodge, R.; Morton, K. Thirty-four patients with carcinoma of the cervical esophagus treated with chemoradiation therapy. Arch. Otolaryngol. Head Neck Surg. 2000, 126, 205–208. [Google Scholar] [CrossRef] [Green Version]
- Vellayappan, B.A.; Soon, Y.Y.; Ku, G.Y.; Leong, C.N.; Lu, J.J.; Tey, J.C. Chemoradiotherapy versus chemoradiotherapy plus surgery for esophageal cancer. Cochrane Database Syst. Rev. 2017, 8, CD010511. [Google Scholar] [CrossRef]
- Valmasoni, M.; Pierobon, E.S.; Zanchettin, G.; Briscolini, D.; Moletta, L.; Ruol, A.; Salvador, R.; Merigliano, S. Cervical Esophageal Cancer Treatment Strategies: A Cohort Study Appraising the Debated Role of Surgery. Ann. Surg. Oncol. 2018, 25, 2747–2755. [Google Scholar] [CrossRef] [PubMed]
- Dataset for Histopathological Reporting of Oesophageal and Gastric Carcinoma. Available online: https://www.rcpath.org/uploads/assets/f8b1ea3d-5529-4f85-984c8d4d8556e0b7/068e9093-0aea-4316-bdd49771564784b9/g006-dataset-for-histopathological-reporting-of-oesophageal-and-gastric-carcinoma.pdf (accessed on 1 October 2019).
- Protocol for the Examination of Specimens from Patients with Carcinoma of the Esophagus. Available online: https://documents.cap.org/protocols/cp-esophagus-17protocol-4000.pdf (accessed on 1 June 2017).
- Biere, S.S.; Maas, K.W.; Cuesta, M.A.; van der Peet, D.L. Cervical or thoracic anastomosis after esophagectomy for cancer: a systematic review and meta-analysis. Dig. Surg. 2011, 28, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Szturz, P.; Wouters, K.; Kiyota, N.; Tahara, M.; Prabhash, K.; Noronha, V.; Castro, A.; Licitra, L.; Adelstein, D.; Vermorken, J.B. Weekly Low-Dose Versus Three-Weekly High-Dose Cisplatin for Concurrent Chemoradiation in Locoregionally Advanced Non-Nasopharyngeal Head and Neck Cancer: A Systematic Review and Meta-Analysis of Aggregate Data. Oncologist 2017, 22, 1056–1066. [Google Scholar] [CrossRef] [Green Version]
- Jacinto, J.K.; Co, J.; Mejia, M.B.; Regala, E.E. The evidence on effectiveness of weekly vs triweekly cisplatin concurrent with radiotherapy in locally advanced head and neck squamous cell carcinoma (HNSCC): A systematic review and meta-analysis. Br. J. Radiol. 2017, 90, 20170442. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Liao, Z.; Chen, Y.; Chang, J.Y.; Jeter, M.; Guerrero, T.; Ajani, J.; Phan, A.; Swisher, S.; Allen, P.; et al. Esophageal cancer located at the neck and upper thorax treated with concurrent chemoradiation: A single-institution experience. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2006, 1, 252–259. [Google Scholar] [CrossRef] [Green Version]
- Uno, T.; Isobe, K.; Kawakami, H.; Ueno, N.; Shimada, H.; Matsubara, H.; Okazumi, S.; Nabeya, Y.; Shiratori, T.; Kawata, T.; et al. Concurrent chemoradiation for patients with squamous cell carcinoma of the cervical esophagus. Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus 2007, 20, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.H.; Lockwood, G.; Brierley, J.; Cummings, B.; Kim, J.; Wong, R.; Bayley, A.; Ringash, J. Effect of concurrent high-dose cisplatin chemotherapy and conformal radiotherapy on cervical esophageal cancer survival. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 735–740. [Google Scholar] [CrossRef]
- Gkika, E.; Gauler, T.; Eberhardt, W.; Stahl, M.; Stuschke, M.; Pottgen, C. Long-term results of definitive radiochemotherapy in locally advanced cancers of the cervical esophagus. Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus 2014, 27, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, E.; Mertineit, N.; De Bari, B.; Hoeng, L.; Caparotti, F.; Leiser, D.; Jumeau, R.; Cihoric, N.; Jensen, A.D.; Aebersold, D.M.; et al. Outcome of proximal esophageal cancer after definitive combined chemo-radiation: A Swiss multicenter retrospective study. Radiat. Oncol. (Lond. Engl.) 2017, 12, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, L.; Zhou, Y.; Mu, Y.; Chai, G.; Xiao, F.; Tan, L.; Lin, S.H.; Shi, M. Patterns of failure and clinical outcomes of definitive radiotherapy for cervical esophageal cancer. Oncotarget 2017, 8, 21852–21860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daiko, H.; Hayashi, R.; Saikawa, M.; Sakuraba, M.; Yamazaki, M.; Miyazaki, M.; Ugumori, T.; Asai, M.; Oyama, W.; Ebihara, S. Surgical management of carcinoma of the cervical esophagus. J. Surg. Oncol. 2007, 96, 166–172. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Number of Patients |
|---|---|
| Median age (years) | 57 (range: 40–82) |
| Female/Male | 0/21 |
| Performance status (ECOG 0–1/2) | 21/0 |
| Clinical stage (I/II/III/IV) a | 0/6/15/0 |
| T status (1/2/3/4) | 1/3/12/5 |
| N status (0/1/2/3) | 5/9/6/1 |
| M status (0/1) | 21/0 |
| Tumor extension | |
| CE | 1 |
| HP+CE | 7 |
| CE+TE | 8 |
| HP+CE+TE | 5 |
| Resectable/unresectable before CCRT b | 17/4 |
| Concurrent chemotherapy (with/without) | 21/0 |
| Grade 0 a | Grade 1 | Grade2 | Grade 3 | Grade 4 | |
|---|---|---|---|---|---|
| Pneumonitis | 20 | 0 | 1 | 0 | 0 |
| Cough | 9 | 4 | 7 | 1 | 0 |
| Esophagitis | 9 | 7 | 5 | 0 | 0 |
| Dermatitis | 8 | 12 | 1 | 0 | 0 |
| Anemia | 1 | 12 | 7 | 1 | 0 |
| Leukocytopenia | 9 | 7 | 4 | 1 | 0 |
| Neutropenia | 16 | 2 | 2 | 1 | 0 |
| Thrombocytopenia | 16 | 3 | 2 | 0 | 0 |
| Nausea | 10 | 10 | 1 | 0 | 0 |
| Vomiting | 17 | 4 | 0 | 0 | 0 |
| Complication | Numbers of Patient (n = 15) |
|---|---|
| Abdominal wound problem | 3 |
| Neck wound infection | 1 |
| Pharyngocutaneous fistula | 1 |
| Anastomotic leakage | 2 |
| Graft failure | 1 |
| Pneumonia | 2 |
| Chylothorax | 1 |
| Operative mortality | 1 |
| Definitive CCRT for Cervical Esophageal Cancer | |||||||
| Author | Patients, No. | Con-CT, % | Dose of RT, Gy | Treatment-Related Mortality (%) | LC, % | Overall Survival (%) | |
| 2-Year | 5-Year | ||||||
| Stuschke et al. 1999 [11] | 17 | Yes a | 60–66 Gy | 0 | 33 (2 y) b | 24 | NA |
| Burmeister et al. 2000 [29] | 34 | Yes, 100 | 50.4–65 Gy (mean 61.2) | 5.9 | 88 | NA | 55 |
| Yamada et al. 2006 [13] | 27 | Yes, 85.2 | 44–73.7 Gy(mean 66) | NA | 52 | NA | 37.9 |
| Wang et al.2006 [37] | 22 (13) c | Yes d | 24.5–64.8 Gy (median 50.4) | NA | 47.7 (5 y) c | NA | 18.6 c |
| Uno et al. 2007 [38] | 21 | Yes, 90.5 | 60–74 Gy (median 64) | 4.8 | NA | 41 | 27 |
| Huang et al. 2008 [39] | 21 | Yes | 54 Gy/20 fx | NA | 48 (2 y) | 52 | NA |
| 29 | Yes | 70 Gy/30 fx | NA | 46 (2 y) | 43 | NA | |
| Tong et al. 2011 [12] | 21 | Yes, 100 | 60–68 Gy | 4.8 | NA | 46.9 | NA |
| Gkika et al. 2013 [40] | 55 | Yes, 100 | 50–70 Gy (median 60) | 0 | 55 (2 y) b | 35 | 25 |
| Cao et al. 2014 [5] | 161 | Yes, 23.4 | 59.4–80 Gy | NA | 69.9 (2 y) | 51 | NA |
| Grass et al. 2015 [4] | 240 | NA | NA | NA | NA | 40 | 28 |
| Cao et al. 2015 [15] | 115 | Yes, 30 | 59.4–80 Gy | 1.7 | 68.3 (2 y) | 47.6 | NA |
| Zhang et al. 2015 [14] | 102 | Yes, 100 | 50–70 Gy | 0 | 35.3 (3 y) e | NA | NA |
| Cao et al. 2016 [16] | 64 | Yes, 34.4 | 60–80 Gy (median 62) | 1.6 | 74.5 (2 y) | 42.5 | NA |
| Herrmann et al. 2017 [41] | 55 | Yes, 92.7 f | 28–72 Gy (median 56) | 0 | 52 (3 y) b | NA | NA |
| Zhao et al. 2017 [42] | 86 | Yes, 70 | 50–70 Gy (median 61.6) | 0 | 57.9 (3 y) e | NA | NA |
| Li et al. 2018 [17] | 92 | Yes, 100 | 60 Gy | 4.3 | NA | 66.3 | NA |
| Primary Surgery for squamous cell carcinoma (SCC) of the Cervical Esophagus | |||||||
| Author | Patients, No. | RT/CRT, % | Treatment-Related Mortality (%) | LC, % | Overall Survival (%) | ||
| Neoadjuvant | Adjuvant | 2-Year | 5-Year | ||||
| Triboulet et al. 2001 [9] | 78 (131) g | 12.9 g | 73 g | 4.8 g | 78 g | NA | 14 |
| Daiko et al. 2007 [43] | 74 | 0 | 14.9 | 4 | 51.4 b | NA | 33 |
| Kadota et al. 2009 [27] | 32 | 0 | NA | 0 | 79.1 (low-tumor group)71.8 (high-tumor group) (5 y) | NA | NA |
| Ott et al. 2009 [18] | 109 | 86 | 0 | 2.8 | 70 h | 61.8 | 47 |
| Tong et al. 2011 [12] | 62 | 0 | 61 | 7.1 | NA | 37.6 | NA |
| Cao et al. 2014 [5] | 63 | 0 | 57.1 | 1.5 | 68.6 (2 y) | 50.7 | NA |
| Grass et al. 2015 [4] | 32 | 44 | 31 | NA | NA | 64 | 43 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dai, K.-Y.; Yu, Y.-C.; Leu, Y.-S.; Chi, C.-W.; Chan, M.-L.; Tsai, C.-H.; Lin, H.-C.; Huang, W.-C.; Chen, Y.-J. Neoadjuvant Chemoradiotherapy and Larynx-Preserving Surgery for Cervical Esophageal Cancer. J. Clin. Med. 2020, 9, 387. https://doi.org/10.3390/jcm9020387
Dai K-Y, Yu Y-C, Leu Y-S, Chi C-W, Chan M-L, Tsai C-H, Lin H-C, Huang W-C, Chen Y-J. Neoadjuvant Chemoradiotherapy and Larynx-Preserving Surgery for Cervical Esophageal Cancer. Journal of Clinical Medicine. 2020; 9(2):387. https://doi.org/10.3390/jcm9020387
Chicago/Turabian StyleDai, Kun-Yao, Yu-Chao Yu, Yi-Shing Leu, Chih-Wen Chi, Mei-Lin Chan, Chung-Hsin Tsai, Huan-Chau Lin, Wen-Chien Huang, and Yu-Jen Chen. 2020. "Neoadjuvant Chemoradiotherapy and Larynx-Preserving Surgery for Cervical Esophageal Cancer" Journal of Clinical Medicine 9, no. 2: 387. https://doi.org/10.3390/jcm9020387