Ketone Bodies Are Mildly Elevated in Subjects with Type 2 Diabetes Mellitus and Are Inversely Associated with Insulin Resistance as Measured by the Lipoprotein Insulin Resistance Index

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Materials and Specimen Collection
2.2. The Insulin Resistance Atherosclerosis Study (IRAS)
2.3. Acquisition of NMR Spectra
2.4. Quantification of Ketone Bodies by Signal Deconvolution Analysis
2.5. Determination of LP-IR Scores and GlycA Levels
2.6. Assay Performance Testing
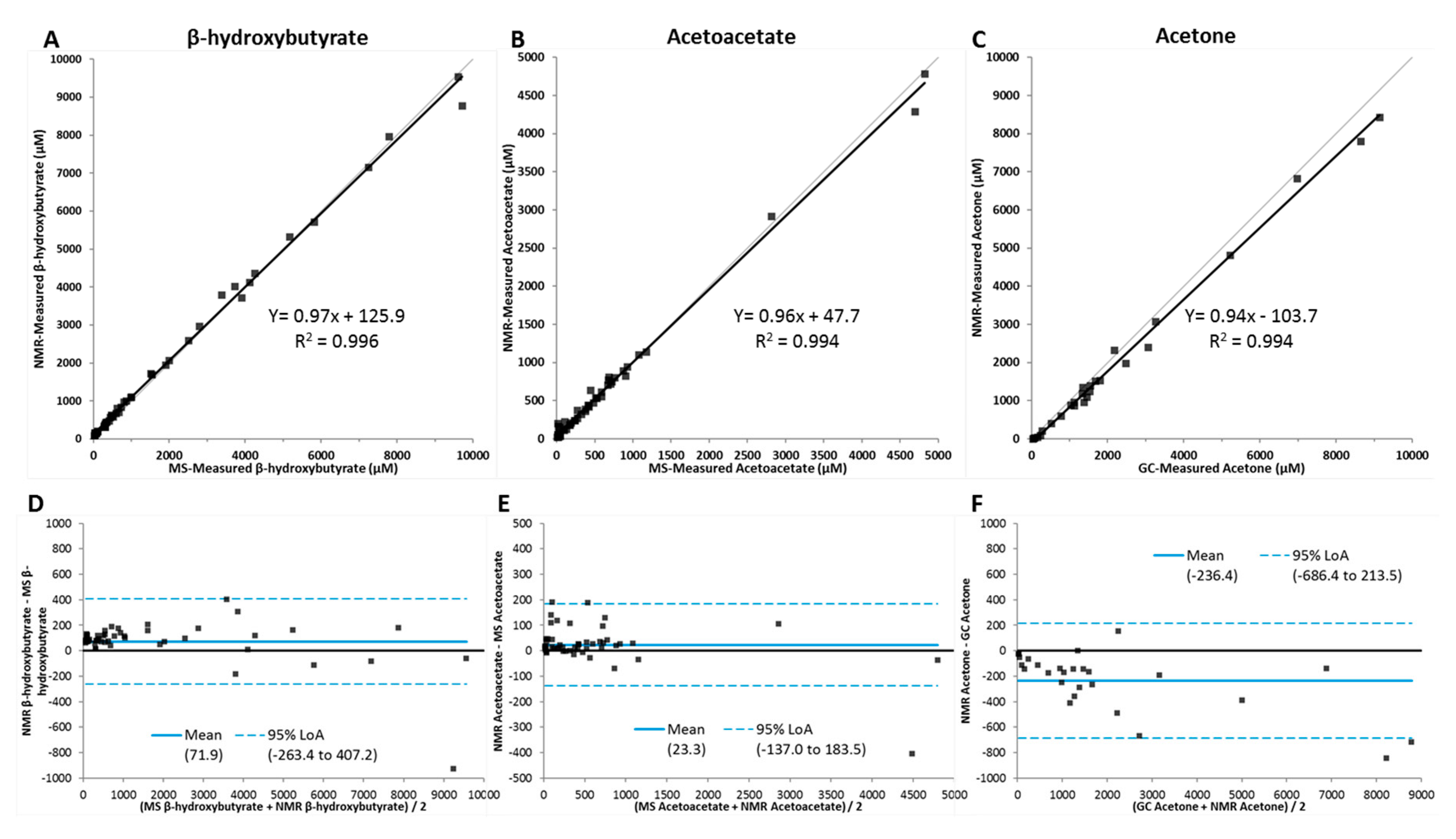
2.7. Method Comparison
2.8. Comparison of Specimen Collection Tubes and Stability Testing
2.9. Reference Interval Studies
2.10. Statistical Analyses
3. Results
3.1. Ketone Body Assay Development and Performance Characteristics
3.2. Cross-Sectional Analysis of Ketone Bodies in a Cohort of Subjects with Metabolic Disease
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
Abbreviations
| AcAc | acetoacetate |
| β-HB | β-hydroxybutyrate |
| BMI | body mass index |
| CLSI | Clinical and Laboratory Standards Institute |
| CV% | coefficient of variation |
| FFAs | free fatty acids |
| GC | gas chromatography |
| HOMA-IR | Homeostatic Model Assessment of Insulin Resistance |
| IRAS | Insulin Resistance Atherosclerosis Study |
| LC/MS/MS | liquid chromatography coupled to tandem mass spectrometry |
| LOAs | limits of agreement |
| LOB | limit of blank |
| LOD | limit of detection |
| LOQ | limit of quantitation |
| NMR | nuclear magnetic resonance spectroscopy |
| ppm | parts per million |
| T2DM | type 2 diabetes mellitus |
| TG | triglycerides |
References
- Laffel, L. Ketone bodies: A review of physiology, pathophysiology and application of monitoring to diabetes. Diabetes/Metab. Res. Rev. 1999, 15, 412–426. [Google Scholar] [CrossRef]
- McGuire, L.C.; Cruickshank, A.M.; Munro, P.T. Alcoholic ketoacidosis. Emerg. Med. J. EMJ 2006, 23, 417–420. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekara, H.; Fernando, P.; Danjuma, M.; Jayawarna, C. Ketoacidosis is not always due to diabetes. BMJ Case Rep. 2014, 2014. [Google Scholar] [CrossRef] [Green Version]
- Schade, D.S.; Eaton, R.P. Differential diagnosis and therapy of hyperketonemic state. JAMA J. Am. Med. Assoc. 1979, 241, 2064–2065. [Google Scholar] [CrossRef]
- Bienia, R.; Ripoll, I. Diabetic ketoacidosis. JAMA J. Am. Med Assoc. 1979, 241, 510–511. [Google Scholar] [CrossRef]
- Miller, V.J.; Villamena, F.A.; Volek, J.S. Nutritional Ketosis and Mitohormesis: Potential Implications for Mitochondrial Function and Human Health. J. Nutr. Metab. 2018, 2018, 5157645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhanpuri, N.H.; Hallberg, S.J.; Williams, P.T.; McKenzie, A.L.; Ballard, K.D.; Campbell, W.W.; McCarter, J.P.; Phinney, S.D.; Volek, J.S. Cardiovascular disease risk factor responses to a type 2 diabetes care model including nutritional ketosis induced by sustained carbohydrate restriction at 1 year: An open label, non-randomized, controlled study. Cardiovasc. Diabetol. 2018, 17, 56. [Google Scholar] [CrossRef] [Green Version]
- Polidori, D.; Iijima, H.; Goda, M.; Maruyama, N.; Inagaki, N.; Crawford, P.A. Intra- and inter-subject variability for increases in serum ketone bodies in patients with type 2 diabetes treated with the sodium glucose co-transporter 2 inhibitor canagliflozin. DiabetesObes. Metab. 2018, 20, 1321–1326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Min, S.H.; Oh, T.J.; Baek, S.I.; Lee, D.H.; Kim, K.M.; Moon, J.H.; Choi, S.H.; Park, K.S.; Jang, H.C.; Lim, S. Degree of ketonaemia and its association with insulin resistance after dapagliflozin treatment in type 2 diabetes. Diabetes Metab. 2018, 44, 73–76. [Google Scholar] [CrossRef]
- Monami, M.N.B.; Zannoni, S.; Lualdi, C.; Mannucci, E. Effects of SGLT-2 inhibitors on diabetic keto acidosis: A meta-analysis of randomized controlled trials. Diabetes Res. Clin. Pract. 2017, 130, 53–60. [Google Scholar] [CrossRef]
- Gupta, L.; Khandelwal, D.; Kalra, S.; Gupta, P.; Dutta, D.; Aggarwal, S. Ketogenic diet in endocrine disorders: Current perspectives. J. Postgrad. Med. 2017, 63, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Holmes, M.V.; Millwood, I.Y.; Kartsonaki, C.; Hill, M.R.; Bennett, D.A.; Boxall, R.; Guo, Y.; Xu, X.; Bian, Z.; Hu, R.; et al. Lipids, Lipoproteins, and Metabolites and Risk of Myocardial Infarction and Stroke. J. Am. Coll. Cardiol. 2018, 71, 620–632. [Google Scholar] [CrossRef] [PubMed]
- Wagenknecht, L.E.; Mayer, E.J.; Rewers, M.; Haffner, S.; Selby, J.; Borok, G.M.; Henkin, L.; Howard, G.; Savage, P.J.; Saad, M.F.; et al. The insulin resistance atherosclerosis study (IRAS) objectives, design, and recruitment results. Ann. Epidemiol. 1995, 5, 464–472. [Google Scholar] [CrossRef]
- Lorenzo, C.; Hartnett, S.; Hanley, A.J.; Rewers, M.J.; Wagenknecht, L.E.; Karter, A.J.; Haffner, S.M. Impaired fasting glucose and impaired glucose tolerance have distinct lipoprotein and apolipoprotein changes: The insulin resistance atherosclerosis study. J. Clin. Endocrinol. Metab. 2013, 98, 1622–1630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palaniappan, L.; Carnethon, M.R.; Wang, Y.; Hanley, A.J.; Fortmann, S.P.; Haffner, S.M.; Wagenknecht, L.; The Insulin Resistance Atherosclerosis Study. Predictors of the incident metabolic syndrome in adults. Diabetes Care 2004, 27, 788–793. [Google Scholar] [CrossRef] [Green Version]
- Wolak-Dinsmore, J.; Gruppen, E.G.; Shalaurova, I.; Matyus, S.P.; Grant, R.P.; Gegen, R.; Bakker, S.J.L.; Otvos, J.D.; Connelly, M.A.; Dullaart, R.P.F. A novel NMR-based assay to measure circulating concentrations of branched-chain amino acids: Elevation in subjects with type 2 diabetes mellitus and association with carotid intima media thickness. Clin. Biochem. 2018, 54, 92–99. [Google Scholar] [CrossRef]
- Festa, A.; Williams, K.; Hanley, A.J.; Otvos, J.D.; Goff, D.C.; Wagenknecht, L.E.; Haffner, S.M. Nuclear magnetic resonance lipoprotein abnormalities in prediabetic subjects in the Insulin Resistance Atherosclerosis Study. Circulation 2005, 111, 3465–3472. [Google Scholar] [CrossRef] [Green Version]
- Jeyarajah, E.J.; Cromwell, W.C.; Otvos, J.D. Lipoprotein particle analysis by nuclear magnetic resonance spectroscopy. Clin. Lab. Med. 2006, 26, 847–870. [Google Scholar] [CrossRef]
- Matyus, S.P.; Braun, P.J.; Wolak-Dinsmore, J.; Jeyarajah, E.J.; Shalaurova, I.; Xu, Y.; Warner, S.M.; Clement, T.S.; Connelly, M.A.; Fischer, T.J. NMR measurement of LDL particle number using the Vantera Clinical Analyzer. Clin. Biochem. 2014, 47, 203–210. [Google Scholar] [CrossRef] [Green Version]
- Matyus, S.P.; Braun, P.J.; Wolak-Dinsmore, J.; Saenger, A.K.; Jeyarajah, E.J.; Shalaurova, I.; Warner, S.M.; Fischer, T.J.; Connelly, M.A. HDL particle number measured on the Vantera(R), the first clinical NMR analyzer. Clin. Biochem. 2015, 48, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Smallcombe, S.H.; Patt, S.L.; Keifer, P.A. WET solvent suppression and its applications to LC NMR and High-Resolution NMR spectroscopy. J. Magn. Reson. 1995, A117, 295–303. [Google Scholar] [CrossRef]
- Shalaurova, I.; Connelly, M.A.; Garvey, W.T.; Otvos, J.D. Lipoprotein insulin resistance index: A lipoprotein particle-derived measure of insulin resistance. Metab. Syndr. Relat. Disord. 2014, 12, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Mackey, R.H.; Mora, S.; Bertoni, A.G.; Wassel, C.L.; Carnethon, M.R.; Sibley, C.T.; Goff, D.C., Jr. Lipoprotein Particles and Incident Type 2 Diabetes in the Multi-Ethnic Study of Atherosclerosis. Diabetes Care 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dugani, S.B.A.; Glynn, R.J.; Ridker, P.M.; Mora, S. Lipoprotein Particle Characteristics and Incident Diabetes in the JUPITER Trial. Circulation 2014, 130, A16055. [Google Scholar]
- Harada, P.H.N.; Demler, O.V.; Dugani, S.B.; Akinkuolie, A.O.; Moorthy, M.V.; Ridker, P.M.; Cook, N.R.; Pradhan, A.D.; Mora, S. Lipoprotein insulin resistance score and risk of incident diabetes during extended follow-up of 20 years: The Women’s Health Study. J. Clin. Lipidol. 2017, 11, 1257–1267.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flores-Guerrero, J.L.; Connelly, M.A.; Shalaurova, I.; Gruppen, E.G.; Kieneker, L.M.; Dullaart, R.P.F.; Bakker, S.J.L. Lipoprotein insulin resistance index, a high-throughput measure of insulin resistance, is associated with incident type II diabetes mellitus in the Prevention of Renal and Vascular End-Stage Disease study. J. Clin. Lipidol. 2019, 13, 129–137.e1. [Google Scholar] [CrossRef] [Green Version]
- Otvos, J.D.; Shalaurova, I.; Wolak-Dinsmore, J.; Connelly, M.A.; Mackey, R.H.; Stein, J.H.; Tracy, R.P. GlycA: A Composite Nuclear Magnetic Resonance Biomarker of Systemic Inflammation. Clin. Chem. 2015, 61, 714–723. [Google Scholar] [CrossRef] [Green Version]
- Connelly, M.A.; Gruppen, E.G.; Otvos, J.D.; Dullaart, R.P.F. Inflammatory glycoproteins in cardiometabolic disorders, autoimmune diseases and cancer. Clin. Chim. Acta; Int. J. Clin. Chem. 2016, 459, 177–186. [Google Scholar] [CrossRef] [Green Version]
- Connelly, M.A.; Otvos, J.D.; Shalaurova, I.; Playford, M.P.; Mehta, N.N. GlycA, a novel biomarker of systemic inflammation and cardiovascular disease risk. J. Transl. Med. 2017, 15, 219. [Google Scholar] [CrossRef]
- CLSI document EP17-A: Protocols for Determination of Limits of Detection and Limits of Quantitation; Approved Guideline; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2004.
- CLSI document EP6-A: Evaluation of the Linearity of Quantitative Measurement Procedures: A Statistical Approach; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2003.
- CLSI document EP5-A2: Evaluation of Precision Performance of Quantitative Measurements Methods, Approved Guideline-Second ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2004.
- CLSI document EP9-A2: Method Comaprison and Bias Estimation Using Patient Samples, Approved Guideline-Second ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2002.
- CLSI document C28-A3: Defining, Establishing, and Verifying Reference Intervals in the Clinical Laboratory, Approved Guideline-Third ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2008.
- Wang, Q.; Jokelainen, J.; Auvinen, J.; Puukka, K.; Keinänen-Kiukaanniemi, S.; Järvelin, M.-R.; Kettunen, J.; Mäkinen, V.-P.; Ala-Korpela, M. Insulin resistance and systemic metabolic changes in oral glucose tolerance test in 5340 individuals: An interventional study. BMC Med. 2019, 17, 217. [Google Scholar] [CrossRef]
- Fritzsche, I.; Buhrdel, P.; Melcher, R.; Bohme, H.J. Stability of ketone bodies in serum in dependence on storage time and storage temperature. Clin. Lab. 2001, 47, 399–403. [Google Scholar] [PubMed]
- McNeil, C.A.; Pramfalk, C.; Humphreys, S.M.; Hodson, L. The storage stability and concentration of acetoacetate differs between blood fractions. Clin. Chim. Acta; Int. J. Clin. Chem. 2014, 433, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Schutten, J.C.; Gomes-Neto, A.W.; Navis, G.; Gansevoort, R.T.; Dullaart, R.P.F.; Kootstra-Ros, J.E.; Danel, R.M.; Goorman, F.; Gans, R.O.B.; Borst, M.H.; et al. Lower Plasma Magnesium, Measured by Nuclear Magnetic Resonance Spectroscopy, is Associated with Increased Risk of Developing Type 2 Diabetes Mellitus in Women: Results from a Dutch Prospective Cohort Study. J. Clin. Med. 2019, 8, 169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, K.J.; Alberti, K.G.; Hinks, L.; Lloyd, B.; Postle, A.; Smythe, P.; Turnell, D.C.; Walton, R. Blood intermediary metabolite and insulin concentrations after an overnight fast: Reference ranges for adults, and interrelations. Clin. Chem. 1978, 24, 1568–1572. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| β-hydroxybutyrate (µM) | Acetoacetate (µM) | Acetone (µM) | |||||
|---|---|---|---|---|---|---|---|
| Low | Medium | High | Low | High | Low | High | |
| Within-laba | |||||||
| Mean | 129.5 | 219.0 | 1188.9 | 127.1 | 182.9 | 106.5 | 187.9 |
| SD | 12.0 | 12.9 | 27.5 | 9.8 | 11.2 | 9.7 | 12.4 |
| CV (%) | 9.3 | 5.9 | 2.3 | 7.7 | 6.1 | 9.1 | 6.6 |
| Within-runb | |||||||
| Mean | 127.5 | 214.8 | 1168.2 | 127.0 | 180.3 | 105.2 | 178.2 |
| SD | 10.8 | 12.5 | 15.6 | 9.1 | 5.6 | 6.4 | 6.8 |
| CV (%) | 8.5 | 5.8 | 1.3 | 7.1 | 3.1 | 6.1 | 3.8 |
| Percentile | Total Ketone Bodies (µM) | β-hydroxybutyrate (µM) | Acetoacetate (µM) | Acetone (µM) |
|---|---|---|---|---|
| 0% | <65.0 | <45.0 | <26.3 | <19.7 |
| 2.5% | 88.8 | 48.6 | <26.3 | <19.7 |
| 25.0% | 136.9 | 88.8 | <26.3 | <19.7 |
| 50.0% | 174.1 | 111.3 | 35.7 | 26.8 |
| 75.0% | 235.8 | 154.1 | 49.7 | 37.8 |
| 97.5% | 623.2 | 396.4 | 120.0 | 78.6 |
| 100% | 1130 | 714.7 | 279.8 | 271.8 |
| Characteristics | Non-Diabetic Subjects (n = 825) | T2DM Subjects (n = 373) | p-Value |
|---|---|---|---|
| Age (years) | 55 ± 8 | 57 ± 8 | <0.0001 |
| Sex, men (%) | 467 (57) | 194 (52) | 0.14 |
| Race | |||
| Non-Hispanic white (%) | 334 (40) | 128 (34) | 0.04 |
| Hispanic (%) | 272 (33) | 119 (32) | 0.72 |
| African American (%) | 219 (27) | 126 (34) | 0.01 |
| SBP (mmHg) | 122 ± 17 | 129 ± 18 | <0.0001 |
| DBP (mmHg) | 78 ± 9 | 78 ± 9.9 | 0.42 |
| BMI (kg/m2) | 28.4 ± 5.6 | 31.5 ± 5.6 | <0.0001 |
| Waist circumference (cm) | 90 ± 13 | 99 ± 12 | <0.0001 |
| Fasting glucose (mmol/L) | 5.5 ± 0.6 | 9.7 ± 3.2 | <0.0001 |
| 2 Hour glucose (mmol/L) | 6.9 ± 1.9 | 17.7 ± 4.8 | <0.0001 |
| Fasting FFAs (mmol/L) | 0.47 ± 0.19 | 0.60 ± 0.23 | <0.0001 |
| Total cholesterol (mmol/L) | 5.44 ± 1.11 | 5.51 ± 1.12 | 0.33 |
| HDL-C (mmol/L) | 1.21 ± 0.39 | 1.05 ± 0.30 | <0.0001 |
| Triglycerides (mmol/L) | 1.24 (0.88–1.81) | 1.77 (1.19–2.46) | <0.0001 |
| GlycA (µM) | 346 ± 70 | 373 ± 71 | <0.0001 |
| LP-IR score (0–100) | 50 ± 21 | 62 ± 18 | <0.0001 |
| Total ketone bodies (µM) | 142 (98–208) | 182 (116–269) | <0.0001 |
| β-hydroxybutyrate (µM) | 100 (67–154) | 131 (79–193) | <0.0001 |
| Acetoacetate (µM) | 26 (13–44) | 32 (15–52) | 0.011 |
| Acetone (µM) | 15 (8–24) | 18 (10–30) | 0.0004 |
| Total KB | β-HB | AcAc | Acetone | |||||
|---|---|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | r | p-Value | |
| Age | 0.057 | 0.050 | 0.057 | 0.048 | 0.028 | 0.328 | 0.004 | 0.884 |
| Sex (men/women) | 0.161 | <0.0001 | 0.210 | <0.0001 | 0.014 | 0.624 | −0.028 | 0.337 |
| Glucose | 0.162 | <0.0001 | 0.137 | <0.0001 | 0.139 | <0.0001 | 0.137 | <0.0001 |
| FFAs | 0.294 | <0.0001 | 0.306 | <0.0001 | 0.155 | <0.0001 | 0.176 | <0.0001 |
| TG | −0.078 | 0.007 | −0.099 | 0.0007 | −0.178 | 0.541 | 0.047 | 0.104 |
| LP-IR score | −0.134 | <0.0001 | −0.157 | <0.0001 | −0.063 | 0.028 | −0.000 | 0.990 |
| T2DM (yes/no) | 0.152 | <0.0001 | 0.145 | <0.0001 | 0.087 | 0.003 | 0.115 | <0.0001 |
| Total KB | β-HB | AcAc | Acetone | |||||
|---|---|---|---|---|---|---|---|---|
| β | p-Value | β | p-Value | β | p-Value | β | p-Value | |
| Age | −0.036 | 0.188 | −0.030 | 0.273 | −0.020 | 0.494 | −0.073 | 0.011 |
| Sex (men/women) | 0.013 | 0.820 | 0.064 | 0.265 | −0.079 | 0.191 | −0.136 | 0.026 |
| FFAs | 0.326 | <0.0001 | 0.336 | <0.0001 | 0.215 | <0.0001 | 0.199 | <0.0001 |
| TG | −0.132 | <0.0001 | −0.168 | <0.0001 | −0.035 | 0.301 | 0.019 | 0.581 |
| LP-IR score | −0.115 | 0.0005 | −0.108 | 0.0009 | −0.110 | 0.001 | −0.072 | 0.037 |
| T2DM (yes/no) | 0.231 | 0.0003 | 0.240 | 0.0001 | 0.131 | 0.049 | 0.168 | 0.012 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia, E.; Shalaurova, I.; Matyus, S.P.; Oskardmay, D.N.; Otvos, J.D.; Dullaart, R.P.F.; Connelly, M.A. Ketone Bodies Are Mildly Elevated in Subjects with Type 2 Diabetes Mellitus and Are Inversely Associated with Insulin Resistance as Measured by the Lipoprotein Insulin Resistance Index. J. Clin. Med. 2020, 9, 321. https://doi.org/10.3390/jcm9020321
Garcia E, Shalaurova I, Matyus SP, Oskardmay DN, Otvos JD, Dullaart RPF, Connelly MA. Ketone Bodies Are Mildly Elevated in Subjects with Type 2 Diabetes Mellitus and Are Inversely Associated with Insulin Resistance as Measured by the Lipoprotein Insulin Resistance Index. Journal of Clinical Medicine. 2020; 9(2):321. https://doi.org/10.3390/jcm9020321
Chicago/Turabian StyleGarcia, Erwin, Irina Shalaurova, Steven P. Matyus, David N. Oskardmay, James D. Otvos, Robin P.F. Dullaart, and Margery A. Connelly. 2020. "Ketone Bodies Are Mildly Elevated in Subjects with Type 2 Diabetes Mellitus and Are Inversely Associated with Insulin Resistance as Measured by the Lipoprotein Insulin Resistance Index" Journal of Clinical Medicine 9, no. 2: 321. https://doi.org/10.3390/jcm9020321