Intraoperative Fluid Restriction is Associated with Functional Delayed Graft Function in Living Donor Kidney Transplantation: A Retrospective Cohort Analysis

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
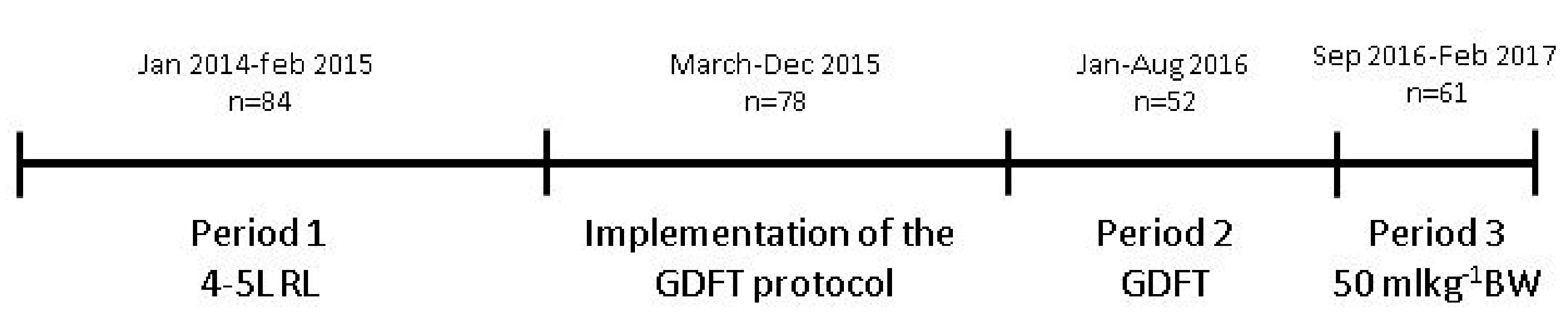
2.1. Study Design and Population
2.2. Definition of DGF
2.3. Intra- and Postoperative Management and Surgical Procedure
2.4. Goal-Directed Fluid Therapy Protocol.
2.5. Patient Data
2.6. Statistics
3. Results
3.1. Univariate Analysis
3.1.1. Patient Characteristics
3.1.2. Intra- and Postoperative Data
3.2. Multivariate Logistic Regression Analysis
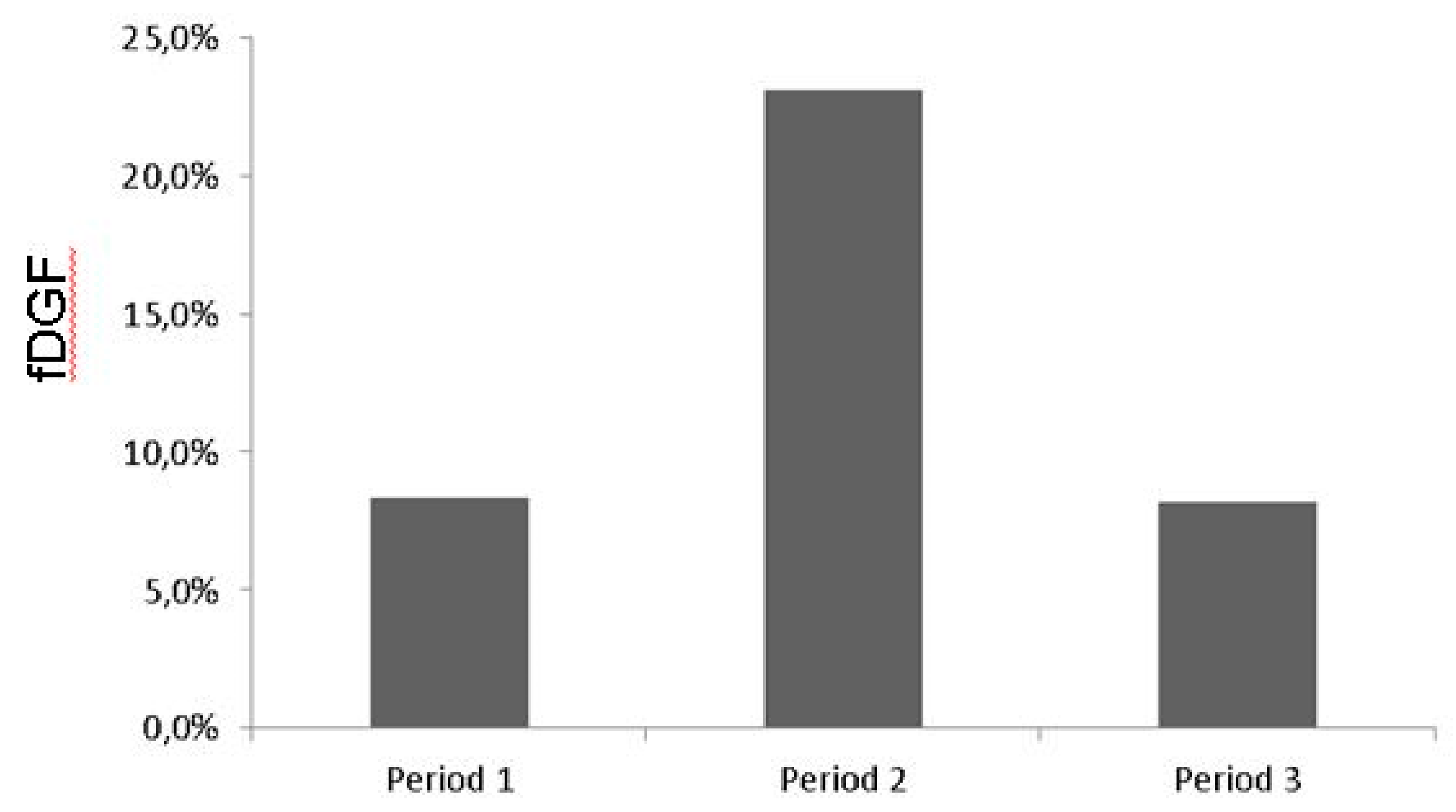
3.3. Influence of the GDFT Protocol on the Intraoperative Fluid Volume.
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nijboer, W.N.; Schuurs, T.A.; van der Hoeven, J.A.; Leuvenink, H.G.; van der Heide, J.J.; van Goor, H.; Ploeg, R.J. Effects of brain death on stress and inflammatory response in the human donor kidney. Transplant. Proc. 2005, 37, 367–369. [Google Scholar] [CrossRef] [PubMed]
- Salvadori, M.; Rosso, G.; Bertoni, E. Update on ischemia-reperfusion injury in kidney transplantation: Pathogenesis and treatment. World J. Transplant. 2015, 5, 52–67. [Google Scholar] [CrossRef] [PubMed]
- Simpkins, C.E.; Montgomery, R.A.; Hawxby, A.M.; Locke, J.E.; Gentry, S.E.; Warren, D.S.; Segev, D.L. Cold ischemia time and allograft outcomes in live donor renal transplantation: Is live donor organ transport feasible? Am. J. Transplant. 2007, 7, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Redfield, R.R.; Scalea, J.R.; Zens, T.J.; Muth, B.; Kaufman, D.B.; Djamali, A.; Astor, B.C.; Mohamed, M. Predictors and outcomes of delayed graft function after living-donor kidney transplantation. Transpl. Int. 2016, 29, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Siedlecki, A.; Irish, W.; Brennan, D.C. Delayed graft function in the kidney transplant. Am. J. Transplant. 2011, 11, 2279–2296. [Google Scholar] [CrossRef]
- Snoeijs, M.G.; Winkens, B.; Heemskerk, M.B.; Hoitsma, A.J.; Christiaans, M.H.; Buurman, W.A.; van Heurn, L.E. Kidney transplantation from donors after cardiac death: A 25-year experience. Transplantation 2010, 90, 1106–1112. [Google Scholar] [CrossRef]
- Perico, N.; Cattaneo, D.; Sayegh, M.H.; Remuzzi, G. Delayed graft function in kidney transplantation. Lancet 2004, 364, 1814–1827. [Google Scholar] [CrossRef]
- Wu, W.K.; Famure, O.; Li, Y.; Kim, S.J. Delayed graft function and the risk of acute rejection in the modern era of kidney transplantation. Kidney Int. 2015, 88, 851–858. [Google Scholar] [CrossRef] [Green Version]
- Fonseca, I.; Teixeira, L.; Malheiro, J.; Martins, L.S.; Dias, L.; Castro Henriques, A.; Mendonça, D. The effect of delayed graft function on graft and patient survival in kidney transplantation: An approach using competing events analysis. Transpl. Int. 2015, 28, 738–750. [Google Scholar] [CrossRef]
- Sharif, A.; Borrows, R. Delayed graft function after kidney transplantation: The clinical perspective. Am. J. Kidney Dis. 2013, 62, 150–158. [Google Scholar] [CrossRef]
- Othman, M.M.; Ismael, A.Z.; Hammouda, G.E. The impact of timing of maximal crystalloid hydration on early graft function during kidney transplantation. Anesth. Analg. 2010, 110, 1440–1446. [Google Scholar] [CrossRef] [PubMed]
- Bacchi, G.; Buscaroli, A.; Fusari, M.; Neri, L.; Cappuccilli, M.L.; Carretta, E.; Stefoni, S. The influence of intraoperative central venous pressure on delayed graft function in renal transplantation: A single-centre experience. Transplant. Proc. 2010, 42, 3387–3391. [Google Scholar] [CrossRef] [PubMed]
- Snoeijs, M.G.; Wiermans, B.; Christiaans, M.H.; van Hooff, J.P.; Timmerman, B.E.; Schurink, G.W.H.; Buurman, W.A.; Van Heurn, L.W.E. Recipient hemodynamics during non-heart-beating donor kidney transplantation are major predictors of primary nonfunction. Am. J. Transplant. 2007, 7, 1158–1166. [Google Scholar] [CrossRef] [PubMed]
- Aulakh, N.K.; Garg, K.; Bose, A.; Aulakh, B.S.; Chahal, H.S.; Aulakh, G.S. Influence of hemodynamics and intraoperative hydration on biochemical outcome of renal transplant recipients. J. Anaesthesiol. Clin. Pharmacol. 2015, 31, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Cavallazzi, R. Does the central venous pressure predict fluid responsiveness? An updated meta-analysis and a plea for some common sense. Crit. Care Med. 2013, 41, 1774–1781. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Kittur, D.S.; Wilasrusmee, C.; Shah, G.; Krause, E.; Ratner, L. Early hemodynamic changes after renal transplantation: Determinants of low central venous pressure in the recipients and correlation with acute renal dysfunction. Med. Sci. Monit. 2003, 9, 61–66. [Google Scholar]
- Le Manach, Y.; Hofer, C.K.; Lehot, J.J.; Vallet, B.; Goarin, J.P.; Tavernier, B.; Cannesson, M. Can changes in arterial pressure be used to detect changes in Cardiac output during volume expansion in the perioperative period? Anesthesiology 2012, 117, 1165–1174. [Google Scholar] [CrossRef] [PubMed]
- Benes, J.; Giglio, M.; Brienza, N.; Michard, F. The effects of goal-directed fluid therapy based on dynamic parameters on post-surgical outcome: A meta-analysis of randomized controlled trials. Crit. Care 2014, 18, 584. [Google Scholar] [CrossRef] [PubMed]
- Ripollés-Melchor, J.; Espinosa, Á.; Martínez-Hurtado, E.; Abad-Gurumeta, A.; Casans-Frances, R.; Fernandez-Perez, C.; Lopez-Timoneda, F.; Calvo-Vecino, J.M. Perioperative goal-directed hemodynamic therapy in noncardiac surgery: A systematic review and meta-analysis. J. Clin. Anesth. 2016, 28, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Chai, F.; Pan, C.; Romeiser, J.L.; Gan, T.J. Effect of perioperative goal-directed hemodynamic therapy on postoperative recovery following major abdominal surgery-a systematic review and meta-analysis of randomized controlled trials. Crit. Care 2017, 21, 141. [Google Scholar] [CrossRef]
- Decruyenaere, P.; Decruyenaere, A.; Peeters, P.; Vermassen, F. A Single-Centre Comparison of 22 Competing Definitions of Delayed Graft Function After Kidney Transplantation. Ann. Transplant. 2016, 21, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Akkina, S.K.; Connaire, J.J.; Israni, A.K.; Snyder, J.J.; Matas, A.J.; Kasiske, B.L. Similar outcomes with different rates of delayed graft function may reflect centre practice, not centre performance. Am. J. Transplant. 2009, 9, 1460–1466. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.; Shabir, S.; Chand, S.; Bentall, A.; McClean, A.; Chan, W.; Jham, S.; Benavente, D.; Sharif, A.; Ball, S.; et al. Assessing and comparing rival definitions of delayed renal allograft function for predicting subsequent graft failure. Transplantation 2010, 90, 1113–1116. [Google Scholar] [CrossRef] [PubMed]
- Pearse, R.M.; Harrison, D.A.; McDonald, N. Effect of a perioperative, cardiac output guided hemodynamic therapy algorithm on outcomes following major gastrointestinal surgery: A randomized clinical trial and updated systematic review. JAMA 2014, 311, 2181–2190. [Google Scholar] [CrossRef] [PubMed]
- Kanda, H.; Hirasaki, Y.; Iida, T.; Kanao-Kanda, M.; Toyama, Y.; Kunisawa, T.; Iwasaki, H. Effect of fluid loading on left ventricular volume and stroke volume variability in patients with end-stage renal disease: A pilot study. Ther. Clin. Risk Manag. 2015, 11, 1619–1625. [Google Scholar] [CrossRef] [PubMed]
- Chappell, D.; Jacob, M.; Hofmann-Kiefer, K.; Conzen, P.; Rehm, M. A rational approach to perioperative fluid management. Anesthesiology 2008, 109, 723–740. [Google Scholar] [CrossRef] [PubMed]
- Shin, C.H.; Long, D.R.; McLean, D.; Grabitz, S.D.; Ladha, K.; Timm, F.P.; Thevathasan, T.; Pieretti, A.; Ferrone, C.; Hoeft, A.; et al. Effects of intraoperative Fluid Management on Postoperative Outcomes: A Hospital Registry Study. Ann. Surg. 2018, 267, 1084–1092. [Google Scholar] [CrossRef]
- Myles, P.S.; Bellomo, R.; Corcoran, T.; Forbes, A.; Peyton, P.; Story, D.; Christophi, C.; Leslie, K.; McGuinness, S.; Parke, R.; et al. Restrictive versus Liberal Fluid Therapy for Major Abdominal Surgery. N. Engl. J. Med. 2018, 378, 2263–2274. [Google Scholar] [CrossRef] [PubMed]
- Adams, P.L.; Adams, F.F.; Bell, P.D.; Navar, L.G. Impaired renal blood flow autoregulation in ischemic acute renal failure. Kidney Int. 1980, 18, 68–76. [Google Scholar] [CrossRef] [Green Version]
- Shannon, J.L.; Headland, R.; MacIver, A.G.; Ferryman, S.R.; Barber, P.C.; Howie, A.J. Studies on the innervation of human renal allografts. J. Pathol. 1998, 186, 109–115. [Google Scholar] [CrossRef]
- Thomas, M.C.; Mathew, T.H.; Russ, G.R.; Rao, M.M.; Moran, J. Perioperative blood pressure control, delayed graft function and acute rejection after renal transplantation. Transplantation 2003, 75, 1989–1995. [Google Scholar] [CrossRef] [PubMed]
- Alejandro, V.; Scandling, J.D., Jr.; Sibley, R.K.; Dafoe, D.; Alfrey, E.; Deen, W.; Myers, B.D. Mechanisms of filtration failure during postischemic injury of the human kidney. A study of the reperfused renal allograft. J. Clin. Investig. 1995, 95, 820–831. [Google Scholar] [PubMed]
- Wilhelm, S.M.; Simonson, M.S.; Robinson, A.V.; Stowe, N.T.; Schulak, J.A. Endothelin up-regulation and localization following renal ischemia and reperfusion. Kidney Int. 1999, 55, 1011–1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavaleri, M.; Veroux, M.; Palermo, F.; Vasile, F.; Mineri, M.; Palumbo, J.; Salemi, L.; Astuto, M.; Murabito, P. Perioperative Goal-Directed Therapy during Kidney Transplantation: An Impact Evaluation on the Major Postoperative Complications. J. Clin. Med. 2019, 8, 80. [Google Scholar] [CrossRef]
- Van Loo, A.A.; Vanholder, R.C.; Bernaert, P.R.; Vermassen, F.E.; van der Vennet, M.; Lameire, N.H. Pretransplantation hemodialysis strategy influences early renal graft function. J. Am. Soc. Nephrol. 1998, 9, 473–481. [Google Scholar]
- Snyder, J.J.; Kasiske, B.L.; Gilbertson, D.T.; Collins, A.J. A comparison of transplant outcomes in peritoneal and hemodialysis patients. Kidney Int. 2002, 62, 1423–1430. [Google Scholar] [CrossRef] [Green Version]
- Bogaard, H.J.; de Vries, J.P.; de Vries, P.M. Assessment of refill and hypovolaemia by continuous surveillance of blood volume and extracellular fluid volume. Nephrol. Dial. Transplant. 1994, 9, 1283–1287. [Google Scholar]
- Morita, K.; Seki, T.; Nonomura, K.; Koyanagi, T.; Yoshioka, M.; Saito, H. Changes in renal blood flow in response to sympathomimetics in the rat transplanted and denervated kidney. Int. J. Urol. 1999, 6, 24–32. [Google Scholar] [CrossRef] [Green Version]
- Alejandro, V.S.; Nelson, W.J.; Huie, P.; Sibley, R.K.; Dafoe, D.; Kuo, P.; Scandling, J.D., Jr.; Myers, B.D. Postischemic injury, delayed function and Na+/K+-ATPase distribution in the transplanted kidney. Kidney Int. 1995, 48, 1308–1315. [Google Scholar] [CrossRef]
- Tanner, G.A.; Sloan, K.L.; Sophasan, S. Effects of renal artery occlusion on kidney function in the rat. Kidney Int. 1973, 4, 377–389. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| nofDGF | fDGF | p | |
|---|---|---|---|
| Donor | N = 244 | N = 31 | |
| Age year | 54 (11.6) | 51 (12.4) | 0.104 |
| Gender male | 117 (48%) | 20 (65%) | 0.089 |
| BMI | 26.1 (3.0) | 25.1 (2.7) | 0.075 |
| Smoking | 67 (27%) | 13 (42%) | 0.140 |
| Blood pressure | |||
| S-RR mmHg | 136 (15.3) | 136 (11.8) | 0.848 |
| D-RR mmHg | 79 (73–84) | 81 (73–86) | 0.548 |
| MAP mmHg | 98 (9.4) | 98 (6.7) | 0.897 |
| Hypertension | 38 (16%) | 2 (6%) | 0.277 |
| Anti-hypertensive drugs | |||
| Diuretics | 11 | 1 | >0.999 |
| Β-blocker | 13 | 1 | >0.999 |
| Ca antagonist | 10 | 0 | 0.610 |
| ACE-I | 4 | 0 | >0.999 |
| AT-II-ant. | 16 | 1 | 0.703 |
| mGFR | |||
| Non-stimulated mL/min | 109 (97–23) | 107 (95–128) | 0.846 |
| Stimulated mL/min | 116 (103–133) | 118 (100–140) | 0.764 |
| ∆GFR | 7 (2–12) | 7 (−1–12) | 0.810 |
| Recipient | N = 244 | N = 31 | |
| Age year | 54 (41−61) | 55 (43−62) | 0.991 |
| Gender male | 138 (57%) | 21 (68%) | 0.254 |
| BMI | 25.6 (22.6–28.4) | 25.8 (24.0–29.8) | 0.267 |
| Smoking | 45 (18%) | 7 (23%) | 0.626 |
| Blood pressure | |||
| S-RR mmHg | 143 (20.4) | 138 (23.7) | 0.196 |
| D-RR mmHg | 79 (73–84) | 81 (73–86) | 0.548 |
| MAP mmHg | 97 (9.4) | 98 (6.6) | 0.897 |
| ∆ blood pressure with donor | |||
| ∆ S-RR mmHg | 7.1 (22.8) | 2.5 (29.1) | 0.308 |
| ∆ D-RR mmHg | 3.1 (13.9) | 1.0 (15.0) | 0.336 |
| ∆ MAP mmHg | 4 (−6–14) | 8 (−10–12) | 0.756 |
| Hypertension | 175 (72%) | 21 (68%) | 0.675 |
| Antihypertensive drugs | |||
| Diuretics | 84 (34%) | 8 (25%) | 0.421 |
| Β-blocker | 124 (51%) | 10 (32%) | 0.058 |
| Ca antagonist | 131 (54%) | 15 (48%) | 0.703 |
| ACE-I. | 46 (19%) | 5 (16%) | 0.811 |
| AT-II-ant | 55 (23%) | 7 (23%) | >0.999 |
| CCI | 3 (2–4) | 3 (2–6) | 0.157 |
| Underlying kidney disease | |||
| DM | 15 (6%) | 5 (16%) | 0.358 |
| PKD | 57 (23%) | 5 (16%) | 0.495 |
| Systemic autoimmune diseases | 25 (10%) | 3 (10%) | >0.999 |
| Glomerulonephritis | 47 (19%) | 4 (13%) | 0.4713 |
| Other | 100 (41%) | 14 (45%) | 0.701 |
| HLA mm < 3 | 55 (23%) | 8 (25%) | 0.655 |
| Dialysis dependent | 105 (43%) | 25 (81%) | <0.001 * |
| LURD | 164 (67%) | 19 (61%) | 0.547 |
| nofDGF | fDGF | p | |
|---|---|---|---|
| Donor | n = 244 | n = 31 | |
| Duration min | 227 (38.2) | 216 (36.8) | 0.134 |
| Fluid | |||
| Total mL | 3845 (799.1) | 3545 (778.2) | 0.050* |
| mL/kg BW | 49 (11.4) | 45 (10.3) | 0.053 |
| Intraoperative blood pressure | |||
| S-RR ≤ 80 mmHG | 137 (56%) | 21 (68%) | 0.251 |
| Cumulative duration (min) | 10 (5–15) | 10 (5–15) | 0.772 |
| Vasoactive substances | |||
| Ephedrine | 178 (73%) | 25 (71%) | 0.515 |
| Phenylephrine | 22 (9%) | 4 (13%) | 0.512 |
| Noradrenaline | 61 (25%) | 11 (35%) | 0.277 |
| Recipient | n = 244 | n = 31 | |
| Duration min | 212 (189–239) | 224 (190–260) | 0.390 |
| Fluid | |||
| Total mL | 3500 (2900–4075) | 3000 (2250–3680) | 0.023* |
| mL/kg BW | 47 (37.3–55.6) | 36 (25.9–50.0) | 0.007* |
| Intraoperative blood pressure | |||
| S-RR < 80 mmHg | 49 (20%) | 6 (19%) | >0.999 |
| Cumulative duration min | 5 (5–10) | 7.5 (4.5–11.2) | 0.679 |
| MAP < 60 mmHg | 93 (38%) | 11 (35%) | 0.846 |
| Cumulative duration min | 10 (5–10) | 5 (5–20) | 0.759 |
| Vasoactive substances | |||
| Ephedrine | 93 (38%) | 16 (52%) | 0.174 |
| Phenylephrine | 26 (11%) | 3 (10%) | >0999 |
| Noradrenaline | 129 (53%) | 23 (74%) | 0.034* |
| 0.02–0.10 mg h−1 | 37 (15%) | 10 (32%) | 0.024* |
| 0.10–0.20 mg h−1 | 42 (17%) | 7 (23%) | 0.459 |
| >0.20 mg h−1 | 49 (20%) | 6 (19%) | >0.999 |
| Ischemia times (min) | |||
| WIT | 3 (3–4) | 3 (3–4) | 0.724 |
| CIT | 154 (140–173) | 158 (141–178) | 0.646 |
| WIT2 | 39 (33–45) | 38 (33–45) | 0.982 |
| Kidney left | 177 (73%) | 19 (61%) | 0.209 |
| Right fossa | 203 (83%) | 26 (84%) | >0.999 |
| >1 artery | 49 (20%) | 8 (26%) | 0.482 |
| Artery sacrificed | 11 (5%) | 4 (13%) | 0.074 |
| Blood loss (mL) | 250 (150–400) | 250 (162.5–500) | 0.499 |
| Urineproduction | n = 230 | n = 30 | |
| 1st h (mL) | 405 (250–675) | 255 (75–512) | 0.005* |
| 2nd h (mL) | 350 (250–550) | 183 (64–462) | 0.002* |
| n = 244 | n = 31 | ||
| Dialysis after transplantation | 0 (0%) | 10 (32%) | <0.001* |
| Length of hospital stay days | 9 (7–13) | 14 (10–20) | <0.001* |
| Model | Odds ratio (95% CI) | p |
|---|---|---|
| 1. Unadjusted analysis, model 1 | ||
| 0.967 (0.941–0.993) | 0.015 |
| 2. Adjusted analysis, model 2 | ||
| 0.970 (0.943–0.998) | 0.036 |
| 0.186 (0.073–0.475) | <0.001 |
| 2.018 (0.834–4.878) | 0.119 |
| 3. Adjusted analysis, model 3 | ||
| 0.969 (0.941–0.997) | 0.029 |
| 0.181 (0.071–0.464) | <0.001 |
| 0.978 (0.942–1.014) | 0.231 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nieuwenhuijs-Moeke, G.J.; Huijink, T.M.; Pol, R.A.; El Moumni, M.; Burgerhof, J.G.; Struys, M.M.; Berger, S.P. Intraoperative Fluid Restriction is Associated with Functional Delayed Graft Function in Living Donor Kidney Transplantation: A Retrospective Cohort Analysis. J. Clin. Med. 2019, 8, 1587. https://doi.org/10.3390/jcm8101587
Nieuwenhuijs-Moeke GJ, Huijink TM, Pol RA, El Moumni M, Burgerhof JG, Struys MM, Berger SP. Intraoperative Fluid Restriction is Associated with Functional Delayed Graft Function in Living Donor Kidney Transplantation: A Retrospective Cohort Analysis. Journal of Clinical Medicine. 2019; 8(10):1587. https://doi.org/10.3390/jcm8101587
Chicago/Turabian StyleNieuwenhuijs-Moeke, Gertrude J, Tobias M Huijink, Robert A Pol, Mostafa El Moumni, Johannes GM Burgerhof, Michel MRF Struys, and Stefan P Berger. 2019. "Intraoperative Fluid Restriction is Associated with Functional Delayed Graft Function in Living Donor Kidney Transplantation: A Retrospective Cohort Analysis" Journal of Clinical Medicine 8, no. 10: 1587. https://doi.org/10.3390/jcm8101587