Impact of Sacubitril/Valsartan on the Long-Term Incidence of Ventricular Arrhythmias in Chronic Heart Failure Patients

 , ,
, ,
Abstract
:1. Introduction
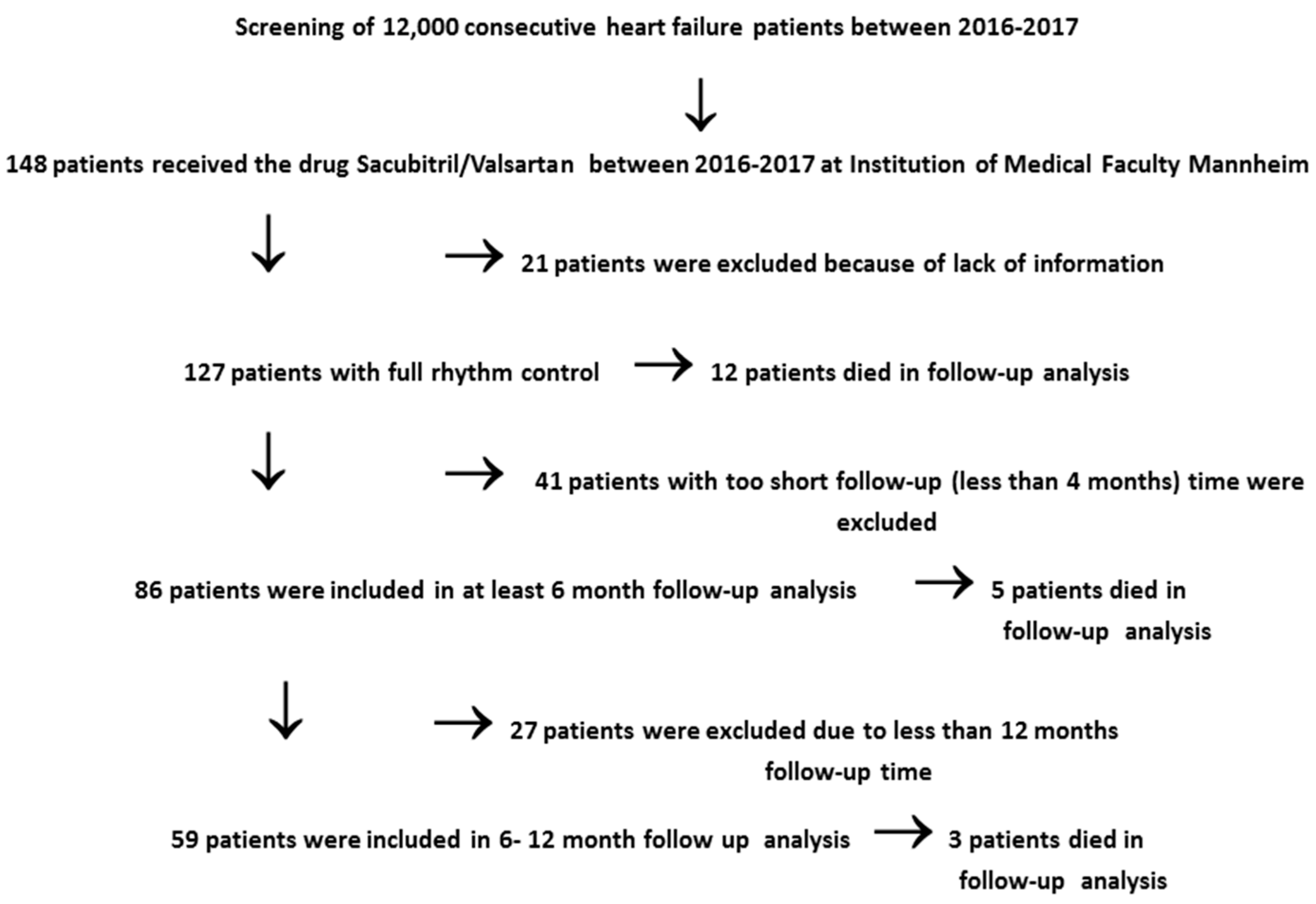
2. Methods
3. Statistics
4. Results
4.1. Characteristics of Patients Started on Sacubitril/Valsartan Treatment
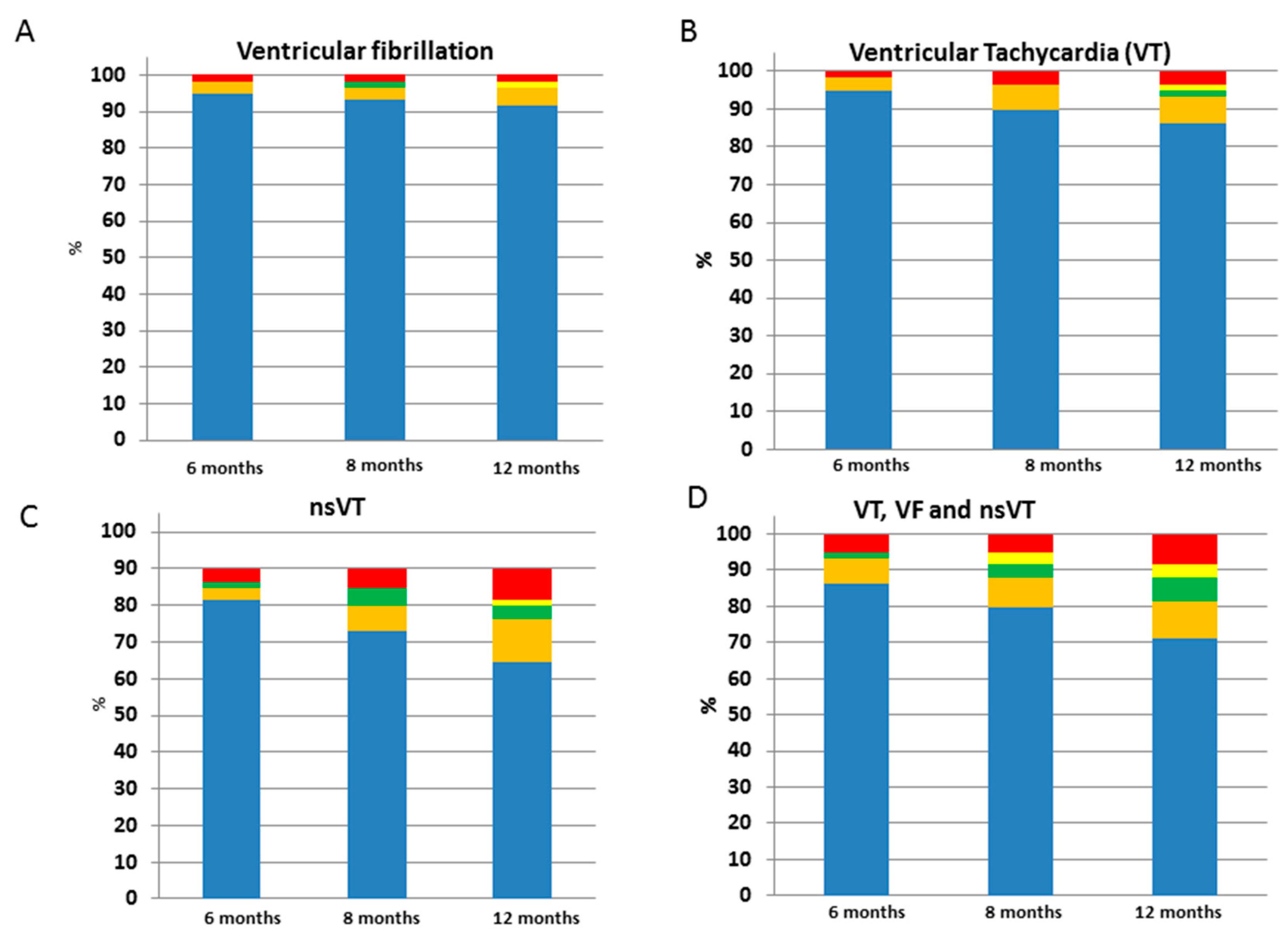
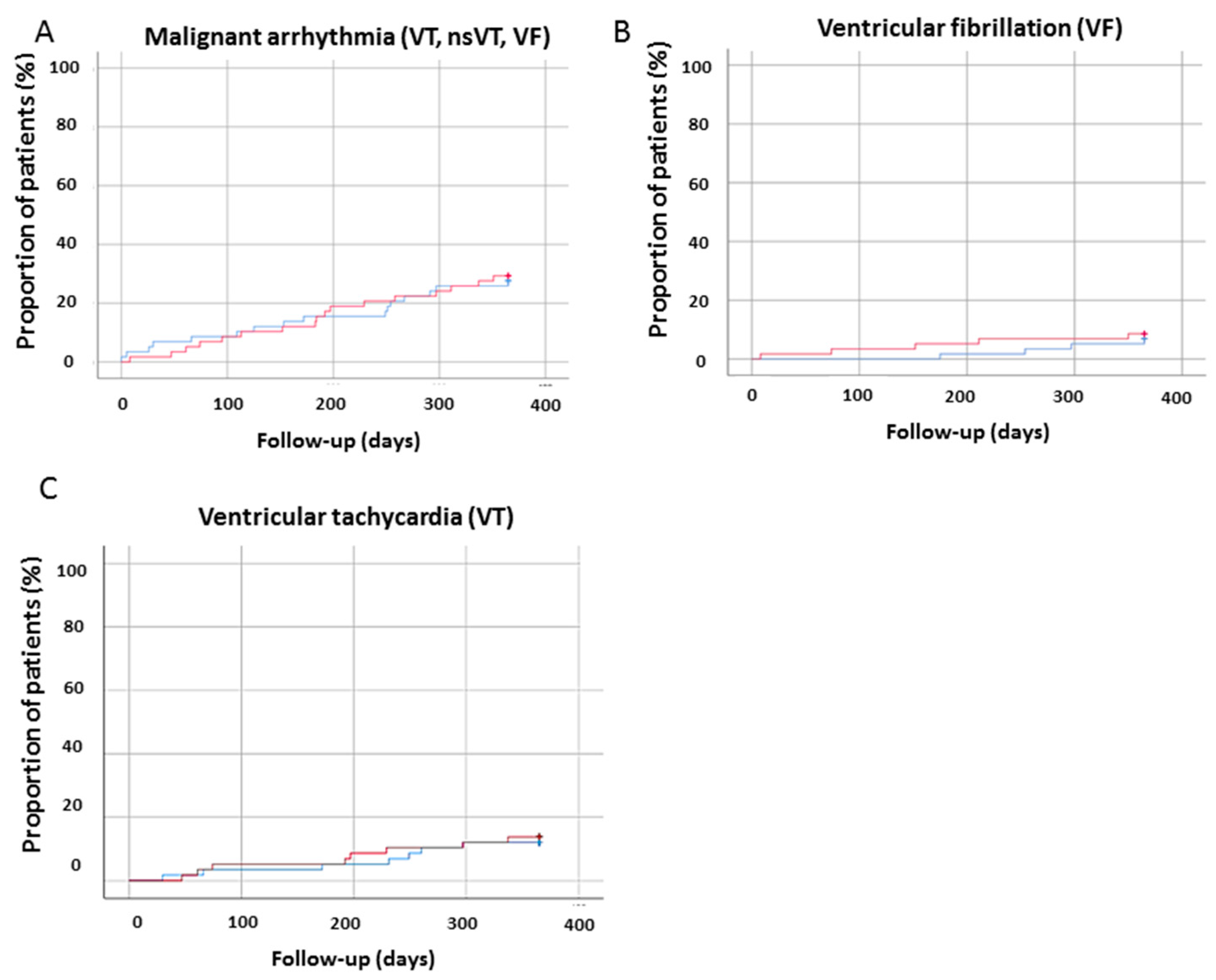
4.2. Incidence of Ventricular Arrhythmia after Sacubitril/Valsartan Use
5. Discussion
6. Conclusions
6.1. Study Limitations
6.2. Clinical Perspectives
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hubers, S.A.; Brown, N.J. Combined Angiotensin Receptor Antagonism and Neprilysin Inhibition. Circulation 2016, 133, 1115–1124. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- De Diego, C.; Gonzalez-Torres, L.; Núñez, J.M.; Inda, R.C.; Martin-Langerwerf, D.A.; Sangio, A.D.; Chochowski, P.; Casasnovas, P.; Blazquez, J.C.; Almendral, J. Effects of angiotensin-neprilysin inhibition compared to angiotensin inhibition on ventricular arrhythmias in reduced ejection fraction patients under continuous remote monitoring of implantable defibrillator devices. Heart Rhythm 2018, 15, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Vicent, L.; Juárez, M.; Martin, I.; García, J.; Gonzalez-Saldivar, H.; Bruña, V.; Devesa, C.; Sousa-Casasnovas, I.; Fernandez-Avilés, F.; Martínez-Sellés, M. Ventricular Arrhythmic Storm after Initiating Sacubitril/Valsartan. Cardiology 2018, 139, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 37, 2129–2200. [Google Scholar]
- ancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J. Am. Coll. Cardiol. 2017, 70, 776–803. [Google Scholar]
- Moss, A.J.; Hall, W.J.; Cannom, D.S.; Daubert, J.P.; Higgins, S.L.; Klein, H.; Levine, J.H.; Saksena, S.; Waldo, A.L.; Wilber, D.; et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. Multicenter Automatic Defibrillator Implantation Trial Investigators. N. Engl. J. Med. 1996, 335, 1933–1940. [Google Scholar] [CrossRef] [PubMed]
- Von Lueder, T.G.; Wang, B.H.; Kompa, A.R.; Huang, L.; Webb, R.; Jordaan, P.; Atar, D.; Krum, H. Angiotensin receptor neprilysin inhibitor LCZ696 attenuates cardiac remodeling and dysfunction after myocardial infarction by reducing cardiac fibrosis and hypertrophy. Circ. Heart Fail. 2015, 8, 71–78. [Google Scholar] [PubMed]
- Podrid, P.J. Potassium and ventricular arrhythmias. Am. J. Cardiol. 1990, 65, 33E–44E. [Google Scholar] [CrossRef]
- Thune, J.J.; Videbæk, L.; Korup, E.; Jensen, G.; Hildebrandt, P.; Bruun, N.E.; Eiskjær, H.; Brandes, A.; Svendsen, J.H.; Høfsten, D.E.; et al. Defibrillator Implantation in Patients with Nonischemic Systolic Heart Failure. N. Engl. J. Med. 2016, 375, 1221–1230. [Google Scholar] [Green Version]
- Damman, K.; Gori, M.; Claggett, B.; Jhund, P.S.; Senni, M.; Lefkowitz, M.P.; Prescott, M.F.; Shi, V.C.; Rouleau, J.L.; Swedberg, K.; et al. Renal Effects and Associated Outcomes During Angiotensin-Neprilysin Inhibition in Heart Failure. JACC Heart Fail. 2018, 6, 489–498. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Before Sacubitril/Valsartan n = 127 | After Sacubitril/Valsartan n = 127 | p Value * |
|---|---|---|---|
| Demographics | |||
| BMI; median – IQR (min–max) | 30 (17.5–49.5) | 30 (17.5–64.20) | 0.04 |
| Clinical parameters | |||
| Systolic BP; mmHg; mean ± SD | 127.93 ± 22.01 | 118.36 ± 20.55 | 0.0035 |
| Diastolic BP; mmHg, median – IQR (min–max) | 80 (42–110) | 70 (30–113) | 0.01 |
| Heart rate; bpm, median – IQR (min–max) | 76 (51–140) | 70 (48–131) | 0.009 |
| Laboratory values | |||
| GFR (mL/min); median – IQR (min–max) | 55.50 (21.00–137.00) | 47.00 (13.00–116.00) | 0.83 |
| Creatinine (mg/dl); (median – IQR (min–max) | 1.31 (0.64–3.55) | 1.45 (0.10–7.10) | 0.32 |
| Alanine transaminase (U/L); median – IQR (min–max) | 25 (5.90–707.00) | 24 (7.00–2532.00) | 0.34 |
| Aspartate transaminase (U/L); median – IQR (min–max) | 23 (11.00–1147.00) | 21 (10.00–6866.00) | 0.03 |
| Gamma-glutamyltransferase (U/L); median – IQR (min–max) | 50.50 (14–488) | 45 (10–913) | 0.06 |
| Bilirubin (mg/dl); median – IQR (min–max) | 0.59 (0.07–2.74) | 0.52 (0.21–5.22) | 0.28 |
| Potassium (mmol/l); mean ± SD | 4.17 ± 0.57 | 4.37 ± 0.65 | 0.0014 |
| LDH; median – IQR (min–max) | 227 (88–1776) | 223 (156–5550) | 0.93 |
| TNI (µg/L); median – IQR (min–max) | 0.08 (0.01–103) | 0.01 (0.01–44.00) | 0.15 |
| CK (U/L); median – IQR (min–max) | 89 (31–971) | 74 (28–624) | 0.18 |
| CK-MB (U/L); mean ± SD | 19 (5–55) | 16 (13–27) | 1.00 |
| proBNP (ng/L); median – IQR (min–max) | 1778 (100–74,676) | 1248 (12.9–25,877) | 0.27 |
| Hemoglobin (g/dl); median – IQR (min–max) | 13.5 (8.2–16.8) | 13.7 (7.7–18.9) | 0.94 |
| C-reactive protein (mg/L); median – IQR (min–max) | 5.00 (0.90–100) | 6.4 (0.2–183) | 0.75 |
| HBA1c (%); median – IQR (min–max) | 7.00 (4.9–12) | 6 (5–8.10) | 0.21 |
| ECG Data. Mean ± SD | |||
| PQ time | 176.85 ± 33.79 | 179.43 ± 41.88 | 0.78 |
| QT time | 433.44 ± 60.73 | 442.48 ± 45.67 | 0.40 |
| QTc time | 475.38 ± 48.48 | 471.36 ± 39.47 | 0.33 |
| Medical history. n (%) | |||
| Smoking | 22 (23.9) | 18 (19.6) | 0.16 |
| Diabetes mellitus type 2 | 43 (35.8) | 45 (37.50) | 0.69 |
| Hypertension | 77(71.96) | 79 (73.8) | 0.59 |
| COPD | 17 (14.6) | 19 (16.3) | 0.41 |
| Asthma | 1 (0.9) | 1 (0.9) | 1.00 |
| History of malignancy | 11 (9.67) | 11 (9.67) | 1.00 |
| Stroke | 10 (8.7) | 11 (9.56) | 0.56 |
| Bleeding | 4 (3.36) | 3 (2.52) | 0.65 |
| Ischemic CMP | 53 (53) | 53 (52) | 1.00 |
| NYHA-Classification | |||
| 1 | 0 (0.00) | 7 (10.14) | 0.22 |
| 2 | 20 (28.99) | 20 (28.99) | 0.22 |
| 3 | 43 (62.31) | 36 (52.17) | 0.22 |
| 4 | 6 (8.7) | 6 (8.7) | 0.22 |
| Echocardiography data. n (%) | |||
| EF(%); median – IQR (min–max) | 25 (5.00–45.00) | 30 (10.00–55.00) | <0.0005 |
| Mitral valve regurgitation | |||
| 0 = none | 12 (14.46) | 13 (15.66) | 0.26 |
| 1 = mild | 27 (32.53) | 34 (40.96) | 0.26 |
| 2 = moderate | 23 (27.71) | 20 (24.1) | 0.26 |
| 3 = severe | 21 (25.3) | 16 (19.28) | 0.26 |
| Tricuspid valve regurgitation | |||
| 0 = none | 25 (37.31) | 22 (32.83) | 0.07 |
| 1 = mild | 21 (31.34) | 29 (43.28) | 0.07 |
| 2 = moderate | 12 (17.91) | 8 (11.94) | 0.07 |
| 3 = severe | 9 (13.43) | 8 11.94) | 0.07 |
| Aortic valve regurgitation | |||
| 0 = none | 51 (79.68) | 51 (79.69) | 0.25 |
| 1 = mild | 7 (10.93) | 11 (10.94) | 0.25 |
| 2 = moderate | 6 (9.38) | 2 (3.13) | 0.25 |
| Electronic cardiac device | |||
| CRT | 36 (29.03) | 44 (35.48) | 0.0047 |
| ICD | 71(57.72) | 79 (64.22) | 0.02 |
| SM | 7 (5.6) | 8 (6.4) | 0.56 |
| CCM | 28 (22.58) | 35 (28.23) | 0.05 |
| Vagus stimulation | 1 (0.826) | 1 (0.826) | 1.00 |
| Variables | Before Sacubitril/Valsartan n = 127 | After Sacubitril/Valsartan n = 127 | p Value * |
|---|---|---|---|
| Drugs on admission. n (%) | |||
| Antidiabetic drugs | |||
| Metfomin | 11 (8.94) | 11 (8.94) | 1.00 |
| Insulin | 19 (15.32) | 17 (13.71) | 0.32 |
| DPP-4 Inhibitor | 11 (8.94) | 10 (8.13) | 0.65 |
| Sulfonylureas | 4 (12.9) | 0 (0.00) | 0.05 |
| SGLT2 Inhibitor | 1 (0.81) | 5 (4.07) | 0.10 |
| GLP-1 Agonist | 0 (0.00) | 1 (0.8) | 0.32 |
| Beta Blocker | 114 (95.7) | 116 (97.5) | 0.48 |
| AT-II Antagonist | 32 (26.7) | 0 (0.00) | <0.0001 |
| Aldosterone Antagonist | 86 (71.1) | 88 (72.7) | 0.71 |
| Spironolactone | 55 (46.4) | 25 (21.07) | 0.35 |
| Eplerenone | 30 (25.4) | 39 (33.1) | 0.03 |
| ACE Inhibitor | 67 (58.8) | 2 (1.75) | <0.0001 |
| Ramipril | 67 (52.7) | 0 (0.00) | <0.0001 |
| Enalapril | 3 (2.7) | 0 (0.00) | 0.08 |
| Lisinopril | 2 (2.7) | 0 (0.00) | 0.16 |
| Diuretics | 101 (82.8) | 105 (86.1) | 0.16 |
| Hydrochlorothiazide | 16 (13.3) | 19 (15.8) | 0.47 |
| Xipamid | 2 (1.67) | 2 (1.67) | 1.00 |
| Torasemid | 91 (75.2) | 95 (78.5) | 0.25 |
| Furosemid | 6 (4.96) | 6 (4.96) | 1.00 |
| Platelet aggregation inhibitors | 57 (47.5) | 53 (44.2) | 0.43 |
| Ticagrelor | 4 (3.31) | 1 (0.83) | 0.08 |
| Aspirin | 51 (42.1) | 47 (38.8) | 0.39 |
| Clopidogrel | 17 (14.4) | 16 (13.6) | 0.78 |
| Prasugrel | 3 (2.48) | 1 (0.83) | 0.16 |
| Anticoagulation | 58 (47.9) | 63 (52.1) | 0.20 |
| Warfarin | 27 (25.96) | 26 (25) | 0.74 |
| Dabigatran | 8 (6.72) | 10 (8.4) | 0.16 |
| Edoxaban | 1 (0.85) | 1 (0.85) | 1.00 |
| Rivaroxaban | 11 (9.24) | 9 (7.56) | 0.41 |
| Apixaban | 10 (8.47) | 17 (14.4) | 0.02 |
| Statin | 79 (66.9) | 83 (70.33) | 0.32 |
| Anti-arrhythmic drugs | |||
| Amiodarone | 19 (15.7) | 26 (21.5) | 0.09 |
| Sotalol | 0/121 (0) | 0 (0) | 1.00 |
| Mexiletine | 0 (0) | 1 (0.83) | 1.00 |
| Variables | Before Sacubitril/Valsartan n = 59 | After Sacubitril/Valsartan n = 59 | p Value * |
|---|---|---|---|
| BMI > 25 kg/m². mean ± SD | 30 (17.8–40.8) | 30.4 (17.47–49) | 0.01 |
| Clinical parameters | |||
| Systolic BP; mmHg; mean ± SD | 129 ± 21 | 121 ± 18 | 0.05 |
| Diastolic BP; mmHg; median – IQR (min–max) | 78 (53–100) | 70 (50–113) | 0.34 |
| Heart rate. Bpm; median – IQR (min–max) | 74 (55–115) | 69 (48–131) | 0.95 |
| Laboratory values | |||
| GFR (ml/min); median – IQR (min–max) | 57.5 (25.0–105.0) | 47.8 (15.0–100) | 0.88 |
| Creatinine (mg/dl); median – IQR (min–max) | 1.38 (0.80–3.55) | 1.4 (0.10–7.1) | 0.41 |
| Alanine transaminase (U/L); median – IQR (min–max) | 24 (13–193) | 24 (10–52) | 0.74 |
| Aspartate transaminase (U/L); median – IQR (min–max) | 24 (12–80) | 22 (10–73) | 0.48 |
| Gamma-GT (U/L); median – IQR (min–max) | 58 (15–280) | 55 (15–261) | 0.09 |
| Bilirubin (mg/dl); median – IQR (min–max) | 0.45 (0.07–1.59) | 0.48 (0.25–1.25) | 0.65 |
| Potassium (mmol/l); mean±SD | 4.14 (3.00–5.40) | 4.42 (3.10–5.50) | 0.08 |
| LDH; median – IQR (min–max) | 226 (88–353) | 241 (165–305) | 0.51 |
| TNI (µg/L); median – IQR (min–max) | 0.093 (0.01–103) | 44 (44–44) | 0.32 |
| CK (U/L); median – IQR (min–max) | 96 (31–249) | 81 (28–432) | 0.87 |
| proBNP (ng/L); median – IQR (min–max) | 1735 (156–74676) | 1845 (43–25877) | 0.18 |
| Hemoglobin (g/dl); median – IQR (min–max) | 13.3 (8.2–16.8) | 13.95 (8.3–18.9) | 0.55 |
| C-reactive protein (mg/L); median – IQR (min–max) | 7.8 (2.4–100) | 6.5 (0.40–181) | 0.97 |
| HBA1c (%); median – IQR (min–max) | 7 (5–8) | 6.1 (5.00–8.1) | 0.23 |
| ECG Data. | |||
| PQ-Time; median – IQR (min–max) | 184 (142–230) | 178 (136–278) | 1.00 |
| QT-Time; median – IQR (min–max) | 422 (334–508) | 436 (354–548) | 0.48 |
| QTc-time; median – IQR (min–max) | 465 (396–555) | 455 (416- 552) | 0.04 |
| Medical history. n (%) | |||
| Smoking | 11/47 (23.4) | 9/47 (19.1) | 0.41 |
| Diabetes mellitus type 2 | 18/56 (32.14) | 21/56 (37.50) | 0.25 |
| Hypertension | 40/51 (78.4) | 42/51 (82.3) | 0.41 |
| COPD | 9/53 (16.98) | 11/53 (20.8) | 0.32 |
| Asthma | 0/51 (0) | 0 /51 (0) | 1.00 |
| History of malignancy | 4/53 (7.55) | 5/53 (9.43) | 0.56 |
| Stroke | 5/55 (9.09) | 5/55 (9.09) | 1.00 |
| Bypass | 10/56 (17.85) | 10/56 (17.85) | 1.00 |
| Bleeding | 4/56 (7.14) | 2/56 (7.14) | 0.32 |
| Ischemic cardiomyopathy | 29/48 (60.41) | 29/48 (60.41) | 0.32 |
| NYHA-Classification | |||
| 1 | 0/34 (0) | 3/34 (8.82) | 0.81 |
| 2 | 12/34 (35.29) | 11/34 (32.35) | 0.81 |
| 3 | 19/34 (55.89) | 17/34 (0.50) | 0.81 |
| 4 | 3/34 (8.82) | 3/34 (8.82) | 0.81 |
| Echocardiography data. n (%) | |||
| EF(%) | 26 (15–40) | 30 (14–55) | 0.10 |
| Mitral valve regurgitation | |||
| 0 = none | 5/35 (14.28) | 5/35 (14.28) | 0.76 |
| 1 = mild | 11/35 (31.42) | 12/35 (34.29) | 0.76 |
| 2 = moderate | 9/35 (25.71) | 9/35 (25.71) | 0.76 |
| 3 = severe | 10/35 (28.57) | 9/35 (25.71) | 0.76 |
| Tricuspid valve regurgitation | |||
| 0 = none | 11/27 (40.74) | 10/27 (37.04) | 0.91 |
| 1 = mild | 10/27 (37.04) | 12/27 (44.44) | 0.91 |
| 2 = moderate | 2/27 (7.04) | 2/27 (7.04) | 0.91 |
| 3 = severe | 4/27 (14.81) | 3/27 (11.11) | 0.91 |
| Aortic valve regurgitation | |||
| 0 = none | 23/26 (88.46) | 21/26 (80.77) | 0.57 |
| 1 = mild | 1/26 (3.85) | 4/26 (15.38) | 0.57 |
| 2 = moderate | 2/26 (7.69) | 1/26 (3.85) | 0.57 |
| Cardiac electronic device | |||
| CRT | 11/57 (19.30) | 14/57 (24.56) | 0.08 |
| ICD | 38/57 (66.67) | 41/57 (71.93) | 0.18 |
| SM | 2/58 (3.45) | 1/58 (1.72) | 0.32 |
| CCM | 21/57 (36.84) | 24/57 (42.11) | 0.32 |
| Vagus stimulator | 0/58 (0) | 0/58 (0) | 1.00 |
| Variables | Before Sacubitril/Valsartan n = 59 | After Sacubitril/Valsartan n = 59 | p Value * |
|---|---|---|---|
| Drugs on admission. n (%) | |||
| Antidiabetic therapy | |||
| Metfomin | 6/58 (10.34) | 7/58 (12.07) | 0.65 |
| Insulin | 10/58 (17.24) | 7/58 ((12.07) | 0.08 |
| DPP-4 Inhibitor | 4/58 (6.90) | 5/58 (8.62) | 0.56 |
| Sulfonylureas | 3/58 (5.17) | 0/58 (0) | 0.08 |
| SGLT2 Inhibitor | 0/58 (0) | 5/58 (8.62) | 0.03 |
| -GLP-1-Agonist | 0/58 (0) | 1/58 (1.72) | 0.32 |
| Beta Blocker | 56/57 (89.24) | 56/57 (98.25) | 1.00 |
| AT-II Antagonist | 17/58 (29.31) | 0/58 (0) | <0.001 |
| Aldosterone Antagonist | 46/58 (79.31) | 44/58 (75.86) | 0.59 |
| Aldactone | 29/57 (50.80) | 20/57 (35.08) | 0.38 |
| Eplerenone | 17/57 (29.82) | 24/57 (42.11) | 0.035 |
| ACE Inhibitor | 30/57 (52.63) | 0/57 (0) | <0.001 |
| Ramipril | 31/55 (56.3) | 0/55 (0) | <0.001 |
| Enalapril | 1/56 ((1.78) | 0/56 (0) | 0.32 |
| Lisinopril | 0/55 (0) | 0/55 (0) | 1.00 |
| Diuretics | 50/58 (86.20) | 53/58 (91.38) | 0.08 |
| Hydrochlorothiazide | 8/57 (14.04) | 8/58 (13.79) | 1.00 |
| Xipamid | 0/57 (0) | 1/57 (1.75) | 0.32 |
| Torasemid | 46/58 (79.31) | 49/58 (84.48) | 0.26 |
| Furosemid | 2/58 (3.45) | 3/58 (5.17) | 0.56 |
| Platelet aggregation inhibitors | 35/58 (0.60) | 32/58 (55.17) | 0.44 |
| Brilique | 1/58 (1.72) | 0/58 (0) | 0.32 |
| Aspirin | 31/58 (53.45) | 29/58 (50) | 0.59 |
| Clopidogrel | 10/56 (17.86) | 8/56 (14.29) | 0.41 |
| Prasugrel | 3/59 (5.08) | 1/59 (1.69) | 0.16 |
| Anticoagulation | 21/58 (36.21) | 25/58 (43.10) | 0.16 |
| Warfarin | 11/48 (22.92) | 12/48 (25) | 0.56 |
| Dabigatran | 3/56 (5.36) | 5/56 (8.93) | 0.16 |
| Edoxaban | 0/56 (0) | 0/56 (0) | 1.00 |
| Rivaroxaban | 3/56 (5.36) | 3/56 (5.36) | 1.00 |
| Apixaban | 4/57 (7.02) | 8/57 (14.04) | 0.10 |
| Statin | 40/56 (41.43) | 43/56 (76.79) | 0.41 |
| Antiarrhythmic drugs | |||
| Amiodarone | 9/57 (15.79) | 15/57 (26.31) | 0.07 |
| Sotalol | 0/57 (0) | 0/57 (0) | 1.00 |
| Mexiletine | 0/57 (0) | 1/57 (1.75) | 1.00 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Battrawy, I.; Pilsinger, C.; Liebe, V.; Lang, S.; Kuschyk, J.; Zhou, X.; Borggrefe, M.; Röger, S.; Akin, I. Impact of Sacubitril/Valsartan on the Long-Term Incidence of Ventricular Arrhythmias in Chronic Heart Failure Patients. J. Clin. Med. 2019, 8, 1582. https://doi.org/10.3390/jcm8101582
El-Battrawy I, Pilsinger C, Liebe V, Lang S, Kuschyk J, Zhou X, Borggrefe M, Röger S, Akin I. Impact of Sacubitril/Valsartan on the Long-Term Incidence of Ventricular Arrhythmias in Chronic Heart Failure Patients. Journal of Clinical Medicine. 2019; 8(10):1582. https://doi.org/10.3390/jcm8101582
Chicago/Turabian StyleEl-Battrawy, Ibrahim, Christina Pilsinger, Volker Liebe, Siegfried Lang, Jürgen Kuschyk, Xiaobo Zhou, Martin Borggrefe, Susanne Röger, and Ibrahim Akin. 2019. "Impact of Sacubitril/Valsartan on the Long-Term Incidence of Ventricular Arrhythmias in Chronic Heart Failure Patients" Journal of Clinical Medicine 8, no. 10: 1582. https://doi.org/10.3390/jcm8101582