Pregabalin Failed to Prevent Dry Eye Symptoms after Laser-Assisted in Situ Keratomileusis (LASIK) in a Randomized Pilot Study

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Intervention
2.3. Study Variables
2.3.1. DE Symptoms
2.3.2. Ocular Pain
2.3.3. Visual Acuity
2.3.4. Ocular Surface Testing
2.3.5. Assessed Co-Morbidities
2.3.6. Side Effects
2.3.7. Main Outcome Measures
2.4. Statistical Analysis
2.5. Power Calculation
3. Results
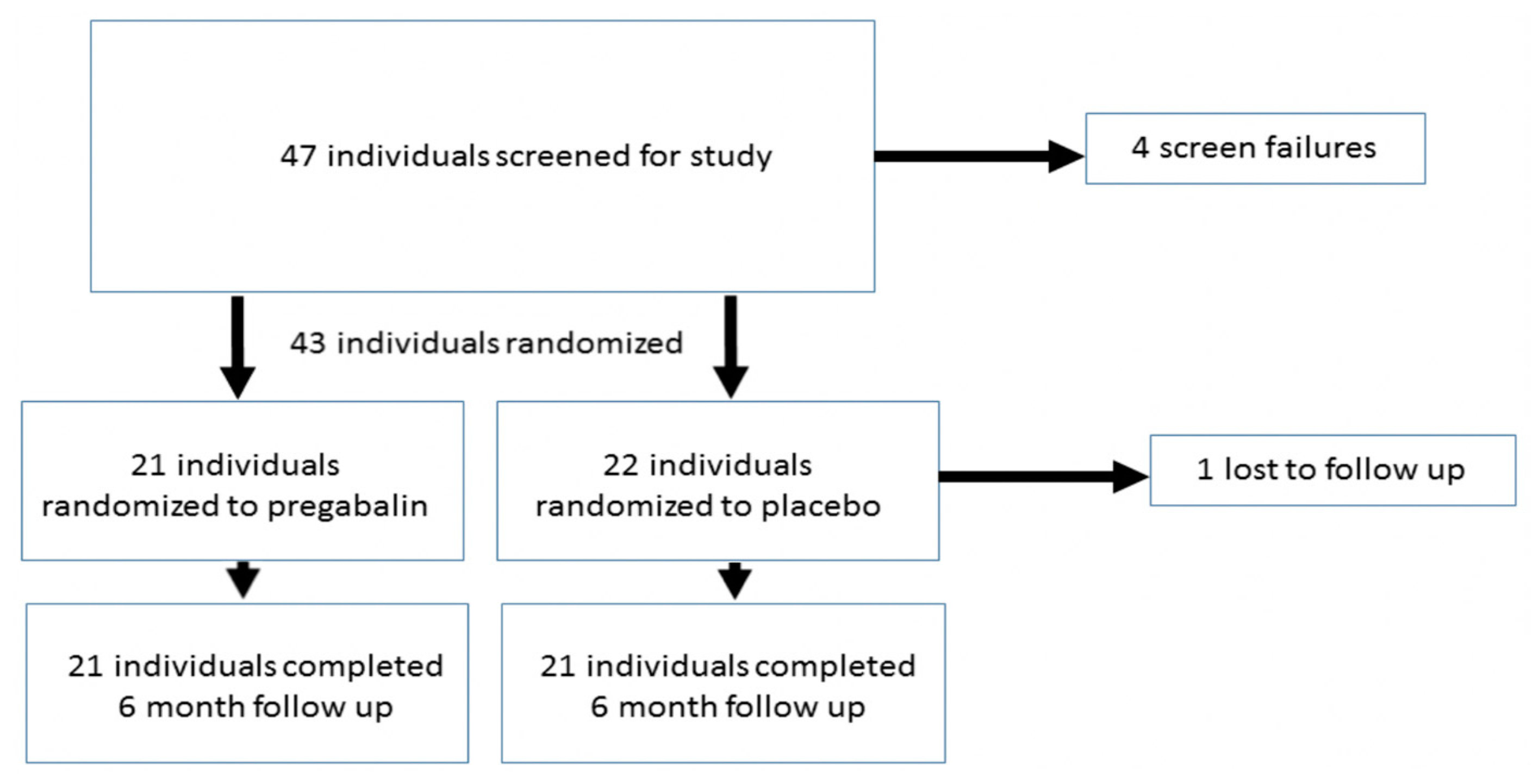
3.1. Study Population
3.2. Ocular Symptoms Three Months after LASIK
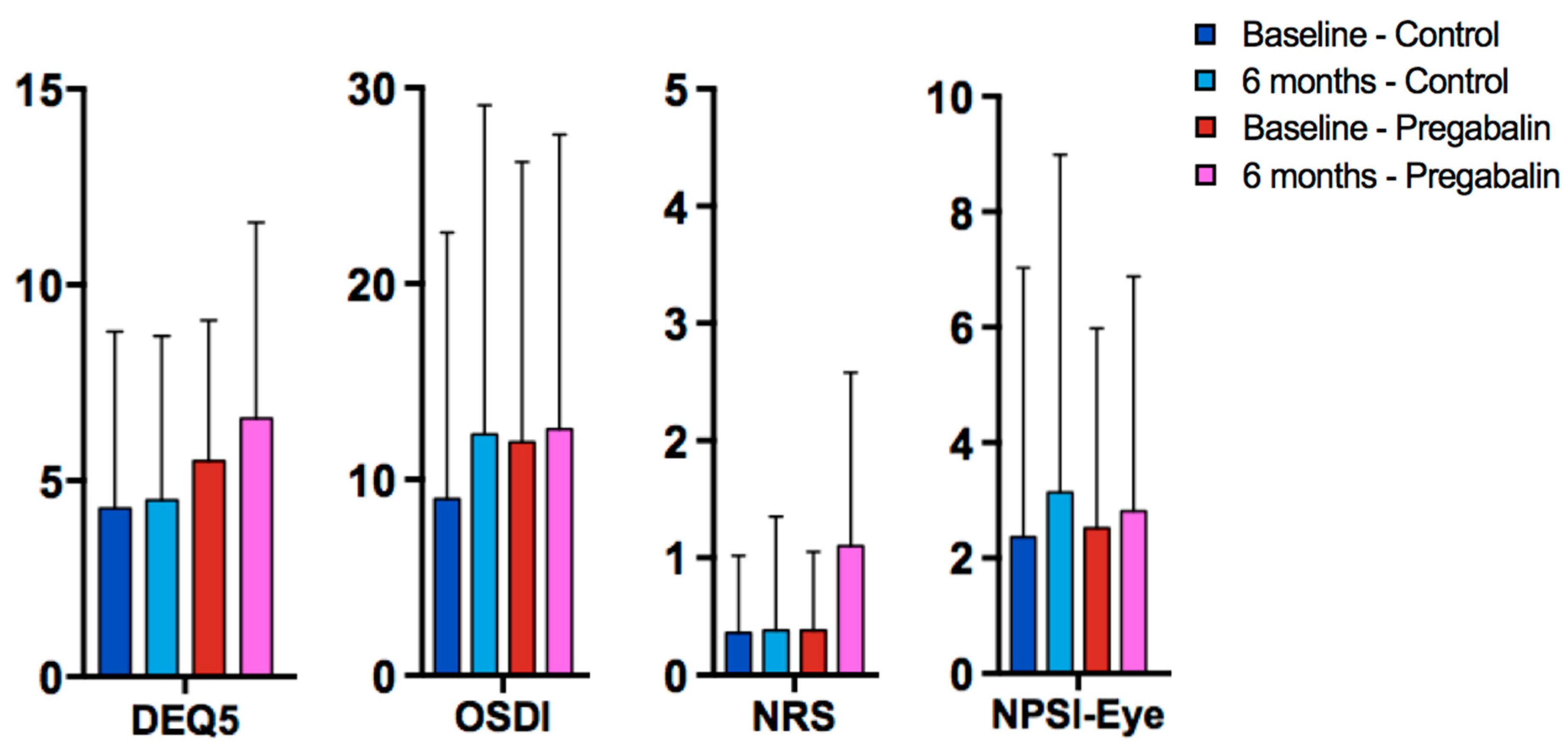
3.3. Ocular Symptoms and Signs at Six Months after LASIK
3.4. Factors Predictive of DE Symptom Frequency and Severity Six Months after Surgery
3.5. Visual Outcomes and Side Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Eydelman, M.; Hilmantel, G.; Tarver, M.E.; Hofmeister, E.M.; May, J.; Hammel, K.; Ferris, F.; Hays, R.D. Symptoms and Satisfaction of Patients in the Patient-Reported Outcomes with Laser in Situ Keratomileusis (PROWL) Studies. JAMA Ophthalmol. 2017, 135, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Levitt, A.E.; Galor, A.; Weiss, J.S.; Felix, E.R.; Martin, E.R.; Patin, D.J.; Sarantopoulos, K.D.; Levitt, R.C. Chronic Dry Eye Symptoms after LASIK: Parallels and Lessons to be Learned from other Persistent Post-Operative Pain Disorders. Mol. Pain 2015, 11, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shoja, M.; Besharati, M. Dry eye after LASIK for myopia: Incidence and risk factors. Eur. J. Ophthalmol. 2007, 17, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Hovanesian, J.A.; Shah, S.S.; Maloney, R.K. Symptoms of dry eye and recurrent erosion syndrome after refractive surgery. J. Cataract. Refract. Surg. 2001, 27, 577–584. [Google Scholar] [CrossRef]
- Albietz, J.M.; Lenton, L.M.; McLennan, S.G. Effect of Laser in situ Keratomileusis for Hyperopia on Tear Film and Ocular Surface. J. Refract. Surg. 2002, 18, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Tuisku, I.S.; Lindbohm, N.; Wilson, S.E.; Tervo, T.M. Dry eye and corneal sensitivity after high myopic LASIK. J. Refract. Surg. 2007, 23, 338–342. [Google Scholar] [CrossRef]
- De Paiva, C.S.; Chen, Z.; Koch, D.D.; Hamill, M.B.; Manuel, F.K.; Hassan, S.S.; Wilhelmus, K.R.; Pflugfelder, S.C. The Incidence and Risk Factors for Developing Dry Eye After Myopic LASIK. Am. J. Ophthalmol. 2006, 141, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Donnenfeld, E.D.; Solomon, K.; Perry, H.D.; Doshi, S.J.; Ehrenhaus, M.; Solomon, R.; Biser, S. The effect of hinge position on corneal sensation and dry eye after LASIK. Ophthalmology 2003, 110, 1023–1029. [Google Scholar] [CrossRef]
- Chao, C.; Golebiowski, B.; Stapleton, F. The Role of Corneal Innervation in LASIK-Induced Neuropathic Dry Eye. Ocul. Surf. 2014, 12, 32–45. [Google Scholar] [CrossRef]
- Galor, A.; Moein, H.R.; Lee, C.; Rodriguez, A.; Felix, E.R.; Sarantopoulos, K.; Levitt, R.C. Neuropathic pain and dry eye. Ocul. Surf. 2018, 16, 31–44. [Google Scholar] [CrossRef]
- Galor, A.; Levitt, R.C.; Felix, E.R.; Martin, E.R.; Sarantopoulos, C.D. Neuropathic ocular pain: An important yet underevaluated feature of dry eye. Eye 2015, 29, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Hayek, S.M.; Sweet, J.A.; Miller, J.P.; Sayegh, R.R. Successful Management of Corneal Neuropathic Pain with Intrathecal Targeted Drug Delivery. Pain Med. 2016, 17, 1302–1307. [Google Scholar] [CrossRef] [PubMed]
- Golan, O.; Randleman, J.B. Pain management after photorefractive keratectomy. Curr. Opin. Ophthalmol. 2018, 29, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, P.C.; Ruchelli, G.; Mackey, S.C.; Caroll, I.R. Perioperative gabapentinoids: Choice of agent, dose, timing, and effects on chronic postsurgical pain. Anesthesiology 2013, 119, 1215–1221. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, R.L.; Begley, C.G.; Caffery, B. Validation of the 5-Item Dry Eye Questionnaire (DEQ-5): Discrimination across self-assessed severity and aqueous tear deficient dry eye diagnoses. Contact Lens Anterior Eye 2010, 33, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and Validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Martinez, J.D.; Galor, A.; Ameusca, G.; Ramos, N.; Beltran, F.; Babayan, A.; Santacruz, C.; Ramirez, C.; Mora, E.; Hernandez, E. Transcultural validation of the 5-Item Dry Eye Questionnaire for the Mexican population. Int. Ophthalmol. 2019, 1–12. [Google Scholar] [CrossRef]
- Jensen, M.P.; Karoly, P.; Braver, S. The measurement of clinical pain intensity: A comparison of six methods. Pain 1986, 27, 117–126. [Google Scholar] [CrossRef]
- Jensen, M.P.; Turner, J.A.; Romano, J.M.; Fisher, L.D. Comparative reliability and validity of chronic pain intensity measures. Pain 1999, 83, 157–162. [Google Scholar] [CrossRef]
- Lovejoy, T.I.; Turk, D.C.; Morasco, B.J. Evaluation of the Psychometric Properties of the Revised Short-Form McGill Pain Questionnaire (SF-MPQ-2). J. Pain 2012, 13, 1250–1257. [Google Scholar] [CrossRef]
- Farhangi, M.; Feuer, W.; Galor, A.; Bouhassira, D.; Levitt, R.C.; Sarantopoulos, C.D.; Felix, E.R. Modification of the Neuropathic Pain Symptom Inventory for use in eye pain (NPSI-Eye). Pain 2019, 160, 1541–1550. [Google Scholar] [CrossRef] [PubMed]
- Bouhassira, D.; Attal, N.; Fermanian, J.; Alchaar, H.; Gautron, M.; Masquelier, E.; Rostaing, S.; Lanteri-Minet, M.; Collin, E.; Grisart, J.; et al. Development and validation of the Neuropathic Pain Symptom Inventory. Pain 2004, 108, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Turk, D.C.; Dworkin, R.H.; Allen, R.R.; Bellamy, N.; Brandenburg, N.; Carr, D.B.; Cleeland, C.; Dionne, R.; Farrar, J.T.; Galer, B.S.; et al. Core outcome domains for chronic pain clinical trials: IMMPACT recommendations. Pain 2003, 106, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; Turk, D.C.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Katz, N.P.; Kerns, R.D.; Stucki, G.; Allen, R.R.; Bellamy, N.; et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 2005, 113, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Farrar, J.T.; Young, J.P., Jr.; LaMoreaux, L.; Werth, J.L.; Poole, R.M. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 96, 410–411. [Google Scholar] [CrossRef]
- Castarlenas, E.; Jensen, M.P.; Von Baeyer, C.L.; Miró, J. Psychometric Properties of the Numerical Rating Scale to Assess Self-Reported Pain Intensity in Children and Adolescents. Clin. J. Pain 2017, 33, 376–383. [Google Scholar] [CrossRef]
- Safikhani, S.; Gries, K.S.; Trudeau, J.J.; Reasner, D.; Rüdell, K.; Coons, S.J.; Bush, E.N.; Hanlon, J.; Abraham, L.; Vernon, M. Response scale selection in adult pain measures: Results from a literature review. J. Patient-Rep. Outcomes 2018, 2, 40. [Google Scholar] [CrossRef]
- Wright, K.D.; Asmundson, G.J.; McCreary, D.R. Factorial validity of the short-form McGill pain questionnaire (SF-MPQ). Eur. J. Pain 2001, 5, 279–284. [Google Scholar] [CrossRef]
- Zinke, J.L.; Lam, C.S.; Harden, R.N.; Fogg, L. Examining the Cross-cultural Validity of the English Short-form McGill Pain Questionnaire Using the Matched Moderated Regression Methodology. Clin. J. Pain 2010, 26, 153–162. [Google Scholar] [CrossRef]
- Sommer, C.; Richter, H.; Rogausch, J.P.; Frettlöh, J.; Lungenhausen, M.; Maier, C. A modified score to identify and discriminate neuropathic pain: A study on the German version of the neuropathic pain symptom inventory (NPSI). BMC Neurol. 2011, 11, 104. [Google Scholar] [CrossRef]
- Galhardoni, R.; Teixeira, M.; Ferreira, K.; Cecilio, S.; Raicher, I.; Moscoso, A.; Pinto, L.; Nishimura, C.; Yeng, L.; Batista, A.; et al. F264 Psychometric Validation of the Portuguese Version of the Neuropathic Pain Symptoms Inventory (NPSI). Eur. J. Pain Suppl. 2011, 5, 143. [Google Scholar] [CrossRef]
- Matsubayashi, Y.; Takeshita, K.; Sumitani, M.; Oshima, Y.; Tonosu, J.; Kato, S.; Ohya, J.; Oichi, T.; Okamoto, N.; Tanaka, S. Psychometric Validation of the Japanese Version of the Neuropathic Pain Symptom Inventory. PLoS ONE 2015, 10, e0143350. [Google Scholar] [CrossRef] [PubMed]
- Bron, A.J.; Abelson, M.B.; Ousler, G.; Pearce, E.; Tomlinson, A.; Yokoi, N.; Smith, J.A.; Begley, C.; Caffery, B.; Nichols, K.; et al. Methodologies to Diagnose and Monitor Dry Eye Disease: Report of the Diagnostic Methodology Subcommittee of the International Dry Eye WorkShop (2007). Ocul. Surf. 2007, 5, 108–152. [Google Scholar]
- Tomlinson, A.; Bron, A.J.; Korb, D.R.; Amano, S.; Paugh, J.R.; Pearce, E.I.; Yee, R.; Yokoi, N.; Arita, R.; Dogru, M. The International Workshop on Meibomian Gland Dysfunction: Report of the Diagnosis Subcommittee. Investig. Opthalmol. Vis. Sci. 2011, 52, 2006–2049. [Google Scholar] [CrossRef] [PubMed]
- Deyo, R.A.; Dworkin, S.F.; Amtmann, D.; Anderrson, G.; Borenstein, D.; Carragee, E.; Carrino, J.; Chou, R.; Cook, K.; DeLitto, A.; et al. Report of the NIH Task Force on Research Standards for Chronic Low Back Pain. Phys. Ther. 2016, 95, e1–e18. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, N.; Kirwan, J.; Boers, M.; Brooks, P.; Strand, V.; Tugwell, P.; Altman, R.; Brandt, K.; Dougados, M.; Lequesne, M. Recommendations for a core set of outcome measures for future phase III clinical trials in knee, hip, and hand osteoarthritis. Consensus development at OMERACT III. J. Rheumatol. 1997, 24, 799–802. [Google Scholar] [PubMed]
- Brooks, P.; Hochberg, M. Outcome measures and classification criteria for the rheumatic diseases. A compilation of data from OMERACT (Outcome Measures for Arthritis Clinical Trials), ILAR (International League of Associations for Rheumatology), regional leagues and other groups. Rheumatology 2001, 40, 896–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmedzai, S.; Cull, A.; Duez, N.J.; Filiberti, A.; Fleishman, S.B.; De Haes, J.C.J.M.; Klee, M.; Rofe, P.B.; Sneeuw, K.; Takeda, F.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar]
- Caraceni, A.; Cherny, N.; Fainsinger, R.; Kaasa, S.; Poulain, P.; Radbruch, L.; De Conno, F. Pain measurement tools and methods in clinical research in palliative care: Recommendations of an Expert Working Group of the European Association of Palliative Care. J. Pain Symptom Manag. 2002, 23, 239–255. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows; Version 22.0; IBM Corp: Armonk, NY, USA, 2013. [Google Scholar]
- Gilron, I.; Bailey, J.M.; Tu, D.; Holden, R.R.; Jackson, A.C.; Houlden, R.L. Nortriptyline and gabapentin, alone and in combination for neuropathic pain: A double-blind, randomised controlled crossover trial. Lancet 2009, 374, 1252–1261. [Google Scholar] [CrossRef]
- McGreevy, K.; Bottros, M.M.; Raja, S.N. Preventing Chronic Pain following Acute Pain: Risk Factors, Preventive Strategies, and their Efficacy. Eur. J. Pain Suppl. 2011, 5, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Lavand’homme, P.; Thienpont, E. Pain after total knee arthroplasty: A narrative review focusing on the stratification of patients at risk for persistent pain. Bone Jt. J. 2015, 97, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Butrick, C.W. Persistent Postoperative Pain: Pathophysiology, Risk Factors, and Prevention. Female Pelvic Med. Reconstr. Surg. 2016, 22, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Vadivelu, N.; Mitra, S.; Schermer, E.; Kodumudi, V.; Kaye, A.D.; Urman, R.D. Preventive analgesia for postoperative pain control: A broader concept. Local Reg. Anesth. 2014, 7, 17–22. [Google Scholar] [PubMed]
- Buvanendran, A.; Kroin, J.S. Multimodal analgesia for controlling acute postoperative pain. Curr. Opin. Anaesthesiol. 2009, 22, 588–593. [Google Scholar] [CrossRef] [PubMed]
- Al-Sabbagh, M.; Okeson, J.P.; Khalaf, M.W.; Bhavsar, I. Persistent pain and neurosensory disturbance after dental implant surgery: Pathophysiology, etiology, and diagnosis. Dent. Clin. N. Am. 2015, 59, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Niraj, G.; Rowbotham, D.J. Persistent postoperative pain: Where are we now? Br. J. Anaesth. 2011, 107, 25–29. [Google Scholar] [CrossRef]
- Dworkin, R.H.; Turk, D.C.; Wyrwich, K.W.; Beaton, D.; Cleeland, C.S.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Kerns, R.D.; Ader, D.N.; et al. Interpreting the Clinical Importance of Treatment Outcomes in Chronic Pain Clinical Trials: IMMPACT Recommendations. J. Pain 2008, 9, 105–121. [Google Scholar] [CrossRef]
- Nissman, S.A.; Tractenberg, R.E.; Babbar-Goel, A.; Pasternak, J.F. Oral Gabapentin for the Treatment of Postoperative Pain after Photorefractive Keratectomy. Am. J. Ophthalmol. 2008, 145, 623–629. [Google Scholar] [CrossRef]
- Woolf, C.J.; Chong, M.-S. Preemptive Analgesia—Treating Postoperative Pain by Preventing the Establishment of Central Sensitization. Anesth. Analg. 1993, 77, 362–379. [Google Scholar] [CrossRef]
- Kuhnle, M.D.; Ryan, D.S.; Coe, C.D.; Eaddy, J.; Kuzmowych, C.; Edwards, J.; Howard, R.S.; Bower, K.S. Oral gabapentin for photorefractive keratectomy pain. J. Cataract. Refract. Surg. 2011, 37, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Lichtinger, A.; Purcell, T.L.; Schanzlin, D.J.; Chayet, A.S. Gabapentin for Postoperative Pain After Photorefractive Keratectomy: A Prospective, Randomized, Double-blind, Placebo-controlled Trial. J. Refract. Surg. 2011, 27, 613–617. [Google Scholar] [CrossRef] [PubMed]
- Pakravan, M.; Roshani, M.; Yazdani, S.; Faramazi, A.; Yaseri, M. Pregabalin and Gabapentin for Post-Photorefractive Keratectomy Pain: A Randomized Controlled Trial. Eur. J. Ophthalmol. 2012, 22, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.L.; Eisenach, J.C.; Chen, S.R. Gabapentin suppresses ectopic nerve discharges and reverses allodynia in neuropathic rats. J. Pharmacol. Exp. Ther. 1999, 288, 1026. [Google Scholar] [PubMed]
- Bennett, M.I.; Simpson, K.H. Gabapentin in the treatment of neuropathic pain. Palliat. Med. 2004, 18, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Wang, H.; Chiang, C.-Y.; Dostrovsky, J.O.; Sessle, B.J. Pregabalin suppresses nociceptive behavior and central sensitization in a rat trigeminal neuropathic pain model. J. Pain 2013, 14, 193–204. [Google Scholar] [CrossRef]
- Chen, S.R.; Xu, Z.; Pan, H.L. Stereospecific effect of pregabalin on ectopic afferent discharges and neuropathic pain induced by sciatic nerve ligation in rats. Anesthesiology 2001, 95, 1473–1479. [Google Scholar] [CrossRef]
- Celik, M.; Kose, A.; Kose, D.; Karakus, E.; Akpinar, E.; Calik, M.; Dostbil, A.; Calikoglu, C.; Aksoy, M.; Ozel, L. The double-edged sword: Effects of pregabalin on experimentally induced sciatic nerve transection and crush injury in rats. Int. J. Neurosci. 2015, 125, 845–854. [Google Scholar] [CrossRef]
- Whitlock, E.; Moradzadeh, A.; Hunter, D.; MacKinnon, S. Pregabalin Does Not Impact Peripheral Nerve Regeneration after Crush Injury. J. Reconstr. Microsurg. 2007, 23, 263–268. [Google Scholar] [CrossRef]
- Khan, J.; Alghamdi, H.; Anwer, M.M.; Eliav, E.; Ziccardi, V. Role of Collagen Conduit with Duloxetine and/or Pregabalin in the Management of Partial Peripheral Nerve Injury. J. Oral Maxillofac. Surg. 2016, 74, 1120–1130. [Google Scholar] [CrossRef]
- Denoyer, A.; Landman, E.; Trinh, L.; Faure, J.F.; Auclin, F.; Baudouin, C. Dry Eye Disease after Refractive Surgery: Comparative Outcomes of Small Incision Lenticule Extraction versus LASIK. Ophthalmology 2015, 122, 669–676. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Pregabalin | Control | p-Value | |
|---|---|---|---|
| Number | 21 | 22 | |
| Demographics | |||
| Age, years, mean (SD) | 37.8 (9.8) | 33.0 (0.6) | 0.12 |
| Female, n (%) | 14 (67%) | 8 (36%) | 0.047 |
| Race, white, n (%) | 18 (86%) | 18 (82%) | 0.92 |
| Hispanic, n (%) | 11 (52%) | 11 (50%) | 0.88 |
| Surgical information, mean (SD) | |||
| Spherical equivalent of treatment, D * | −3.48 (3.25) | −3.95 (1.79) | 0.56 |
| Flap depth, microns, mean (SD) | 117 (21) | 109 (30) | 0.34 |
| Eye co-morbidities, n (%) | |||
| Self-reported eye allergies | 1 (5%) | 2 (9%) | 1.0 |
| Contact lens wear prior to surgery | 16 (76%) | 13 (59%) | 0.23 |
| Artificial tears use prior to surgery | 4 (19%) | 5 (23%) | 1.0 |
| Eye symptoms | |||
| DEQ5, mean (SD), range 0–22 | 5.5 (3.6) | 4.3 (4.5) | 0.34 |
| DEQ5, mild symptoms ≥6, n (%) | 10 (48%) | 9 (41%) | 0.66 |
| DEQ5, severe symptoms ≥12, n (%) | 2 (10%) | 2 (10%) | 0.96 |
| OSDI, mean (SD), range 0-100 | 11.9 (14.3) | 9.0 (13.6) | 0.50 |
| Ocular pain, worst over one week recall, mean (SD), range 0–10 | 0.48 (0.75) | 0.64 (0.75) | 0.61 |
| Ocular pain, average over one week recall, mean (SD), range 0–10 | 0.38 (0.67) | 0.36 (0.66) | 0.93 |
| Sf-MPQ sensory, mean (SD), range 0–33 | 0.90 (1.84) | 0.09 (0.29) | 0.06 |
| Sf-MPQ affective, mean (SD), range 0–12 | 0.43 (0.68) | 0.23 (0.61) | 0.31 |
| Intensity of burning over one day recall, mean (SD), range 0–10 | 0.10 (0.30) | 0.27 (0.63) | 0.25 |
| Intensity of wind sensitivity one day recall, mean (SD), range 0–10 | 0.48 (0.68) | 0.36 (1.09) | 0.69 |
| Intensity of light sensitivity one day recall, mean (SD), range 0–10 | 0.86 (1.42) | 0.68 (1.81) | 0.73 |
| NPSI-Eye total, mean (SD), range 0–100 | 2.52 (3.46) | 2.36 (4.67) | 0.90 |
| Eye signs * | |||
| Any eyelid laxity, n (%) | 3 (14%) | 2 (9%) | 0.66 |
| Inflammadry score ≥2, n (%) | 4 (19%) | 3 (14%) | 0.63 |
| Inflammadry positive, n (%) | 11 (52%) | 15 (68%) | 0.07 |
| TBUT, seconds, mean (SD) | 10.9 (7.3) | 9.1 (6.2) | 0.67 |
| Conjunctivochalasis, n (%) | 12 (57%) | 16 (73%) | 0.28 |
| Corneal staining, mean (SD) | 2.2 (2.5) | 2.6 (2.7) | 0.66 |
| Anterior blepharitis, mean (SD) | 0.95 (0.80) | 1.00 (0.82) | 0.85 |
| Eyelid vascularity, mean (SD) | 1.00 (0.95) | 0.77 (0.81) | 0.40 |
| Meibomian plugging, mean (SD) | 1.33 (0.91) | 1.41 (0.91) | 0.79 |
| Meibomian gland drop, mean (SD) | 1.24 (1.04) | 0.91 (0.75) | 0.24 |
| Schirmers test, mm wetting, mean (SD) | 12.8 (7.4) | 17.0 (9.0) | 0.10 |
| Meibomian quality, mean (SD) | 1.95 (1.32) | 1.59 (1.18) | 0.35 |
| Conjunctival papillae, ≥mild, n (%) | 15 (71%) | 14 (64%) | 0.86 |
| Co-morbidities | |||
| Average daily screen time, hours, mean (SD) | 8.7 (4.1) | 7.9 (3.0) | 0.44 |
| Depression via Scl-90, mean (SD), range 0–4 | 0.32 (0.33) | 0.28 (0.64) | 0.82 |
| Anxiety via Scl-90, mean (SD), range 0–4 | 0.24 (0.29) | 0.13 (0.24) | 0.16 |
| Carpet at home, n (%) | 5 (24%) | 4 (18%) | 0.65 |
| Non-ocular allergies, n (%) | 5 (24%) | 5 (23%) | 0.93 |
| Chronic pain in any area, n (%) | 5 (24%) | 4 (18%) | 0.72 |
| Headache (including migraine), n (%) | 3 (14%) | 2 (9%) | 0.66 |
| No of chronic pain conditions (headache, low back pain, sciatica, irritable bowel), mean (SD) | 0.52 (1.33) | 0.23 (0.61) | 0.35 |
| Average non-ocular pain intensity, one week recall, mean (SD) | 0.71 (1.62) | 0.50 (1.19) | 0.62 |
| Pregabalin | Control | p-Value | |
|---|---|---|---|
| Number | 21 | 22 | |
| Eye symptoms | |||
| DEQ5, mean (SD), range 0–22 | 6.6 (3.9) | 4.7 (4.4) | 0.14 |
| DEQ5, mild symptoms ≥6, n (%) | 14 (67%) | 10 (46%) | 0.16 |
| DEQ5, severe symptoms ≥12, n (%) | 1 (5%) | 2 (9%) | 1.00 |
| Change in DEQ5 from baseline, mean (SD) | 1.1 (3.9) | 0.4 (4.0) | 0.54 |
| OSDI, mean (SD), range 0–100 | 11.9 (11.5) | 11.0 (16.6) | 0.84 |
| Change in OSDI from baseline, mean (SD) | −0.01 (15.6) | 2.0 (15.1) | 0.67 |
| Ocular pain, worst over one week recall, mean (SD), range 0–10 | 1.25 (1.52) | 0.50 (1.01) | 0.07 |
| Ocular pain, average over one week recall, mean (SD), range 0–10 | 0.85 (0.27) | 0.27 (0.55) | 0.07 |
| Sf-MPQ sensory, mean (SD), range 0–33 | 0.65 (1.23) | 0.36 (0.66) | 0.35 |
| Sf-MPQ affective, mean (SD), range 0–12 | 0.30 (0.66) | 0.18 (0.39) | 0.48 |
| Intensity of burning over one day recall, mean (SD), range 0–10 | 0.15 (0.67) | 0.64 (1.76) | 0.24 |
| Intensity of wind sensitivity one day recall, mean (SD), range 0–10 | 0.70 (1.56) | 0.36 (0.95) | 0.40 |
| Intensity of light sensitivity one day recall, mean (SD), range 0–10 | 0.90 (1.83) | 0.64 (1.62) | 0.62 |
| NPSI-Eye total, mean (SD), range 0–100 | 2.70 (4.55) | 1.86 (4.07) | 0.53 |
| Pregabalin | Control | p-Value | |
|---|---|---|---|
| Number (n) | 21 | 21 | |
| Eye symptoms | |||
| DEQ5, mean (SD), range 0–22 | 6.6 (5.0) | 4.5 (4.2) | 0.14 |
| DEQ5, mild symptoms ≥6, n (%) | 12 (57%) | 7 (33%) | 0.12 |
| DEQ5, severe symptoms ≥12, n (%) | 4 (19%) | 1 (5%) | 0.34 |
| Change in DEQ5 from baseline, mean (SD) | 1.1 (3.9) | 0.1 (3.6) | 0.42 |
| OSDI, mean (SD), range 0–100 | 12.6 (15.0) | 12.3 (16.8) | 0.96 |
| Change in OSDI from baseline, mean (SD) | -0.30 (14.4) | 2.9 (15.9) | 0.51 |
| Ocular pain, worst over one week recall, mean (SD), range 0–10 | 1.38 (1.75) | 0.76 (1.38) | 0.21 |
| Ocular pain, average over one week recall, mean (SD), range 0–10 | 1.10 (1.48) | 0.38 (0.97) | 0.08 |
| Intensity of burning over one day recall, mean (SD), range 0–10 | 0.43 (0.87) | 0.62 (1.28) | 0.58 |
| Any burning pain, n (%) | 5 (24%) | 5 (24%) | 1.00 |
| Intensity of wind sensitivity one day recall, mean (SD), range 0–10 | 1.00 (1.95) | 0.57 (0.93) | 0.37 |
| Any sensitivity to wind, n (%) | 7 (33%) | 7 (33%) | 1.00 |
| Intensity of light sensitivity one day recall, mean (SD), range 0–10 | 0.48 (1.25) | 0.86 (1.49) | 0.38 |
| Any sensitivity to light, n (%) | 4 (19%) | 8 (38%) | 0.17 |
| NPSI-Eye total, mean (SD), range 0–100 | 2.81 (4.07) | 3.14 (5.85) | 0.83 |
| Eye signs * | |||
| Inflammadry score ≥2, n (%) | 2 (10%) | 4 (20%) | 0.66 |
| Inflammadry positive, n (%) | 10 (50%) | 7 (35%) | 0.34 |
| TBUT, seconds, mean (SD) | 8.35 (2.46) | 9.05 (5.93) | 0.62 |
| Corneal staining, mean (SD) | 2.43 (2.58) | 2.05 (1.94) | 0.59 |
| Schirmer score, mm wetting, mean (SD) | 15.45 (8.17) | 15.05 (8.64) | 0.88 |
| Pearson r | OSDI | NRS | sf-MPQ | NPSI-Eye | DEQ5 |
|---|---|---|---|---|---|
| OSDI | r = 1 | r = 0.12 p = 0.45 | r = 0.26 p = 0.11 | r = 0.20 p = 0.22 | r = 0.34 p = 0.03 |
| NRS | r = 1 | r = 0.56 p < 0.0005 | r = 0.68 p < 0.0005 | r = 0.38 p = 0.01 | |
| sf-MPQ | r = 1 | r = 0.75 p < 0.0005 | r = 0.20 p = 0.22 | ||
| NPSI-Eye | r = 1 | r = 0.28 p = 0.08 | |||
| DEQ5 | r = 1 |
| Model Outcome | Predictor Variable(s) | β | p-Value |
|---|---|---|---|
| DEQ5 at six months | DEQ5 (Baseline) | 0.74 | <0.0005 |
| Age | 0.13 | 0.03 | |
| OSDI at six months | OSDI (Baseline) | 0.33 | 0.04 |
| NRS at six months | Scl-90 Anxiety (Baseline) | 0.61 | <0.0005 |
| sf-MPQ at six months | Scl-90 Depression (Baseline) | 0.73 | <0.0005 |
| NPSI-Eye at six months | Scl-90 Depression (Baseline) | 0.50 | <0.0005 |
| NRS (Baseline) | 0.45 | <0.0005 |
| Pregabalin | Control | p-Value | |
|---|---|---|---|
| Any side effects, n (%) | 13 (62%) | 10 (46%) | 0.28 |
| Tiredness | 8 (38%) | 2 (9%) | 0.03 |
| Dizziness | 6 (29%) | 1 (5%) | 0.05 |
| Headache | 3 (14%) | 3 (14%) | 1.0 |
| Nausea | 1 (5%) | 2 (9%) | 1.0 |
| Dry mouth | 3 (14%) | 0 (0%) | 0.11 |
| Constipation | 3 (14%) | 1 (5%) | 0.35 |
| Bloating | 3 (14%) | 4 (18%) | 1.0 |
| High or elevated mood | 4 (19%) | 1 (5%) | 0.19 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galor, A.; Patel, S.; Small, L.R.; Rodriguez, A.; Venincasa, M.J.; Valido, S.E.; Feuer, W.; Levitt, R.C.; Sarantopoulos, C.D.; Felix, E.R. Pregabalin Failed to Prevent Dry Eye Symptoms after Laser-Assisted in Situ Keratomileusis (LASIK) in a Randomized Pilot Study. J. Clin. Med. 2019, 8, 1355. https://doi.org/10.3390/jcm8091355
Galor A, Patel S, Small LR, Rodriguez A, Venincasa MJ, Valido SE, Feuer W, Levitt RC, Sarantopoulos CD, Felix ER. Pregabalin Failed to Prevent Dry Eye Symptoms after Laser-Assisted in Situ Keratomileusis (LASIK) in a Randomized Pilot Study. Journal of Clinical Medicine. 2019; 8(9):1355. https://doi.org/10.3390/jcm8091355
Chicago/Turabian StyleGalor, Anat, Sneh Patel, Leslie R. Small, Adriana Rodriguez, Michael J. Venincasa, Stephen E. Valido, William Feuer, Roy C. Levitt, Constantine D. Sarantopoulos, and Elizabeth R. Felix. 2019. "Pregabalin Failed to Prevent Dry Eye Symptoms after Laser-Assisted in Situ Keratomileusis (LASIK) in a Randomized Pilot Study" Journal of Clinical Medicine 8, no. 9: 1355. https://doi.org/10.3390/jcm8091355