Deep Brain Stimulation of the Subthalamic Nucleus Selectively Modulates Emotion Recognition of Facial Stimuli in Parkinson’s Patients


Abstract
:1. Introduction
2. Methods
2.1. Participants
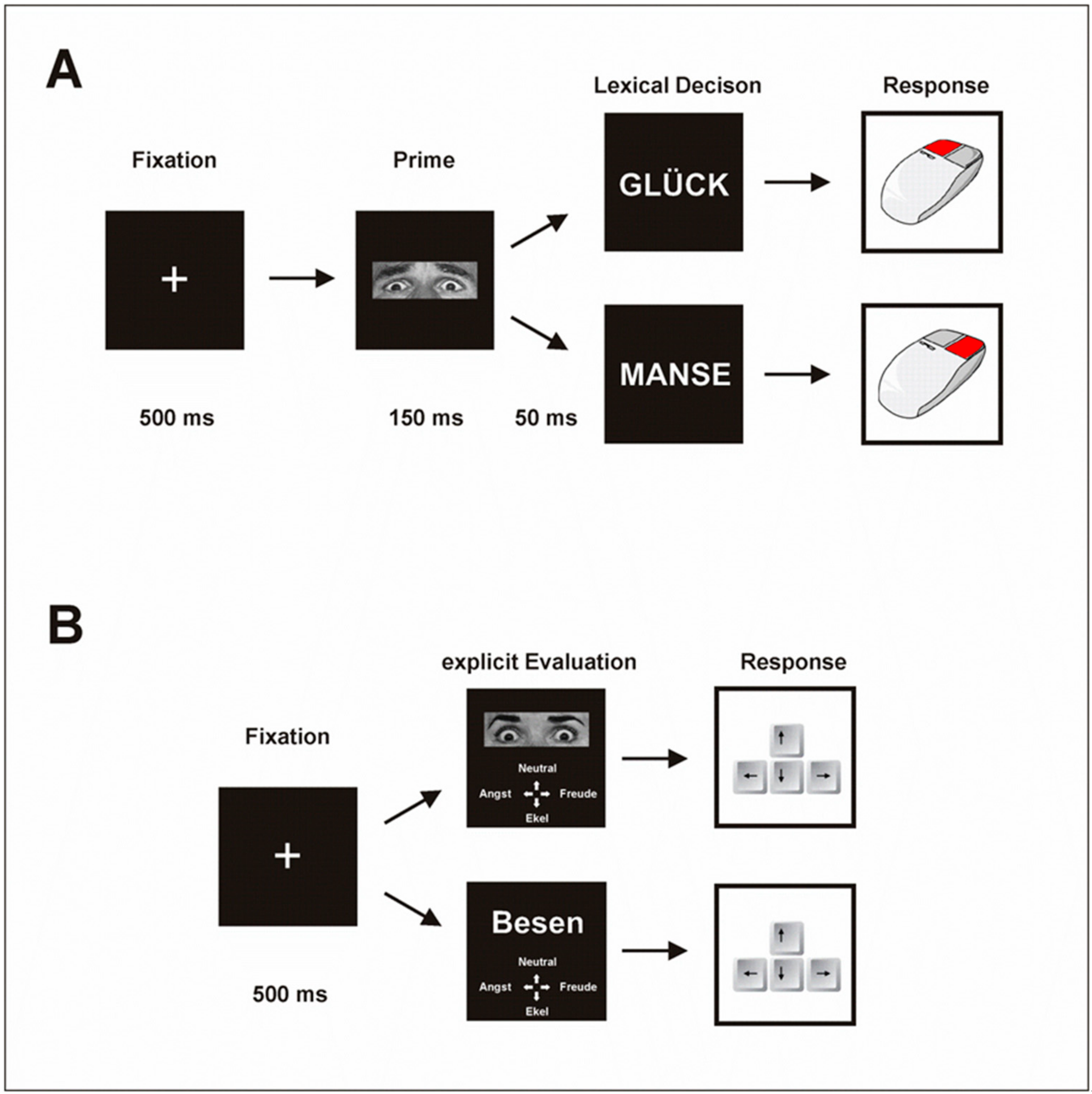
2.2. Experimental Procedure
2.3. Material
2.4. Task
2.5. Statistical Analysis
3. Results
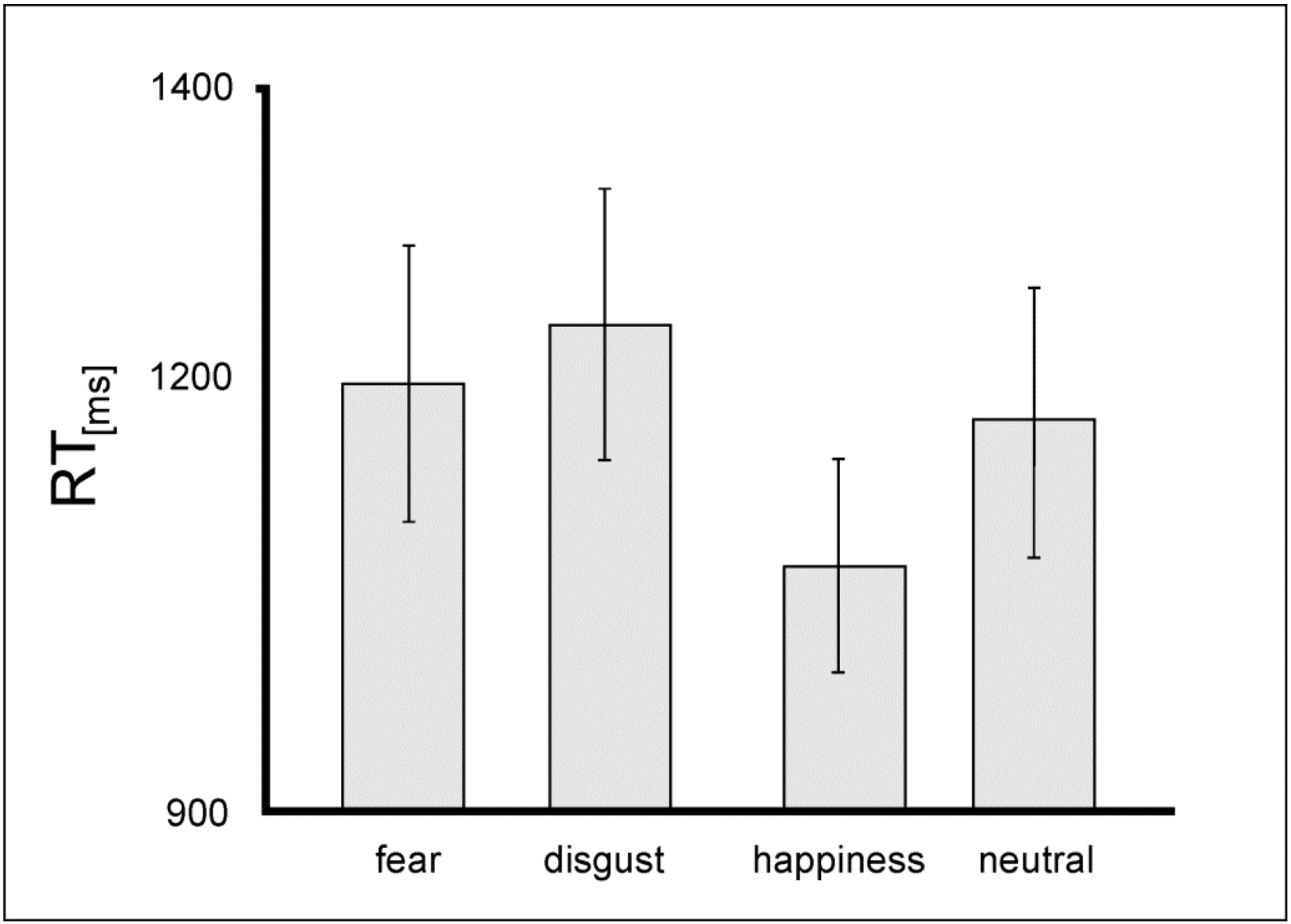
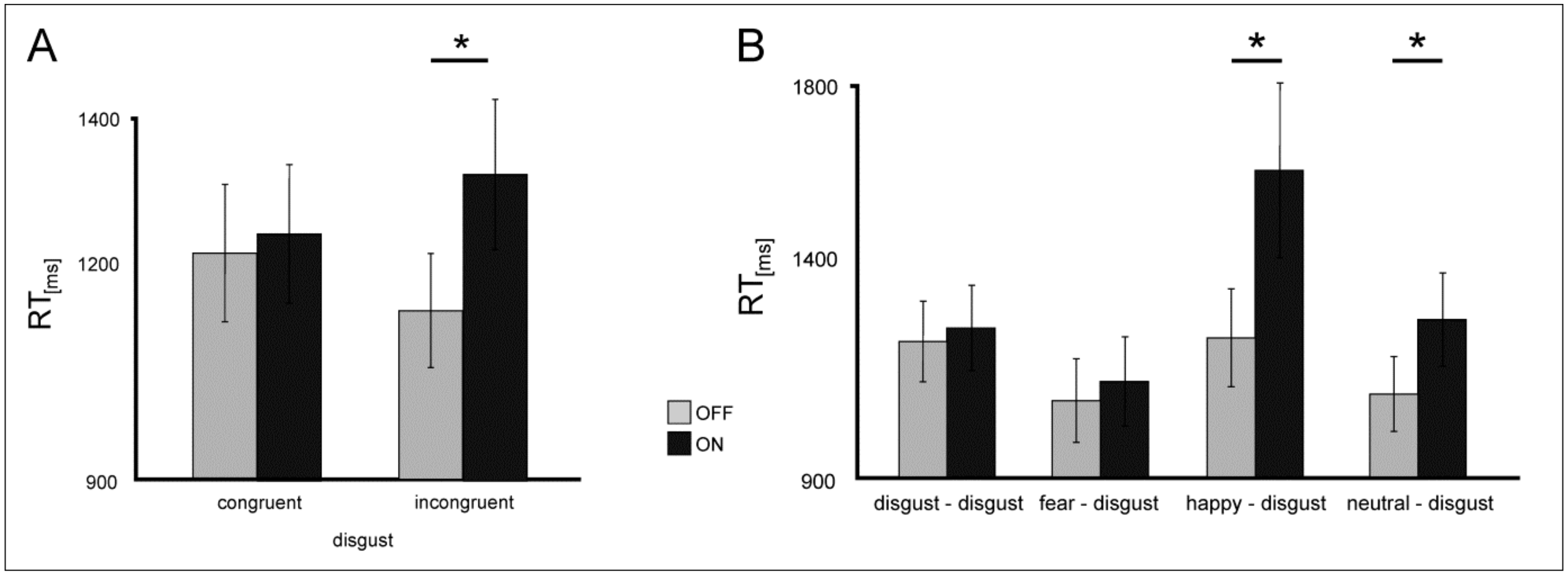
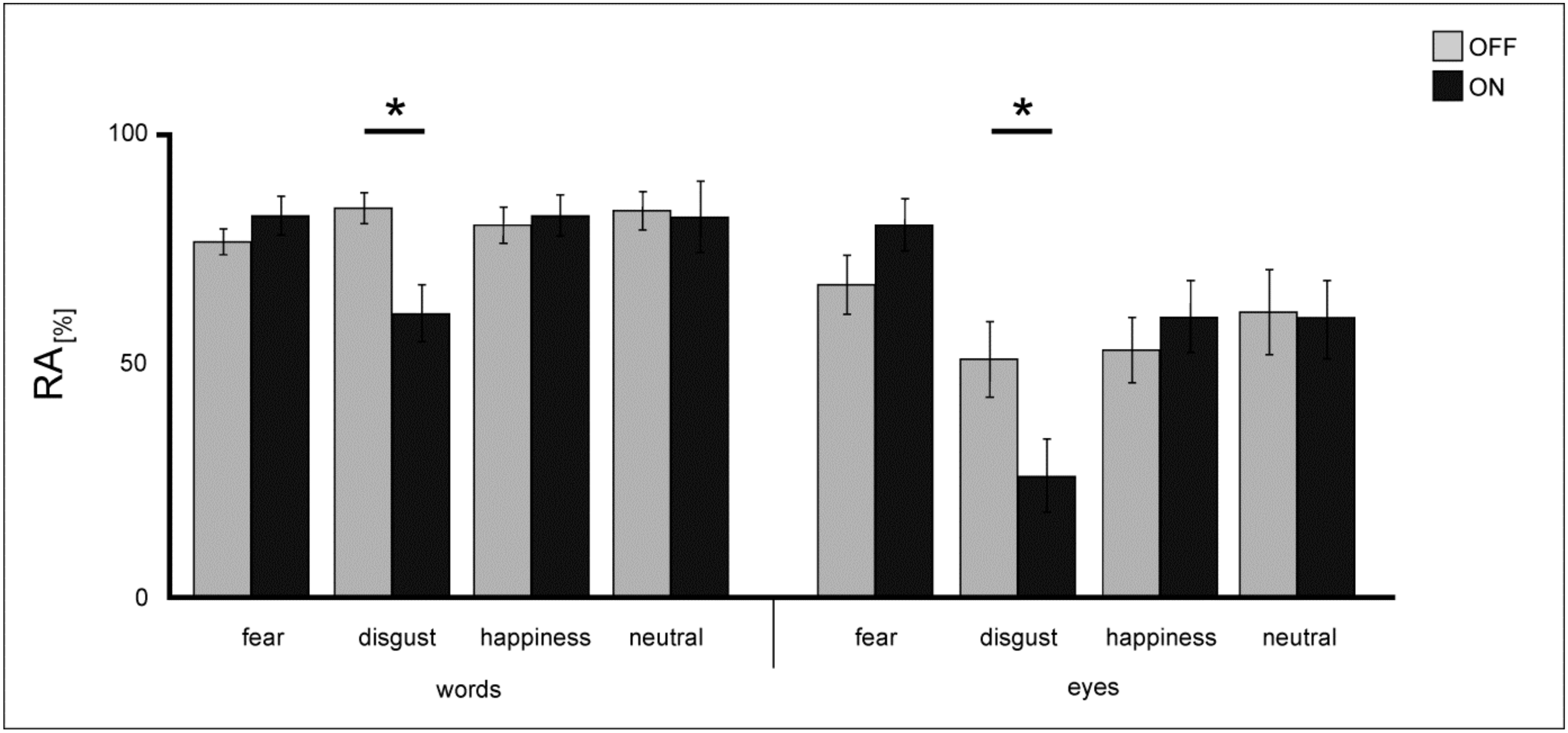
3.1. Implicit Emotional Processing
3.2. Summary Implicit Task
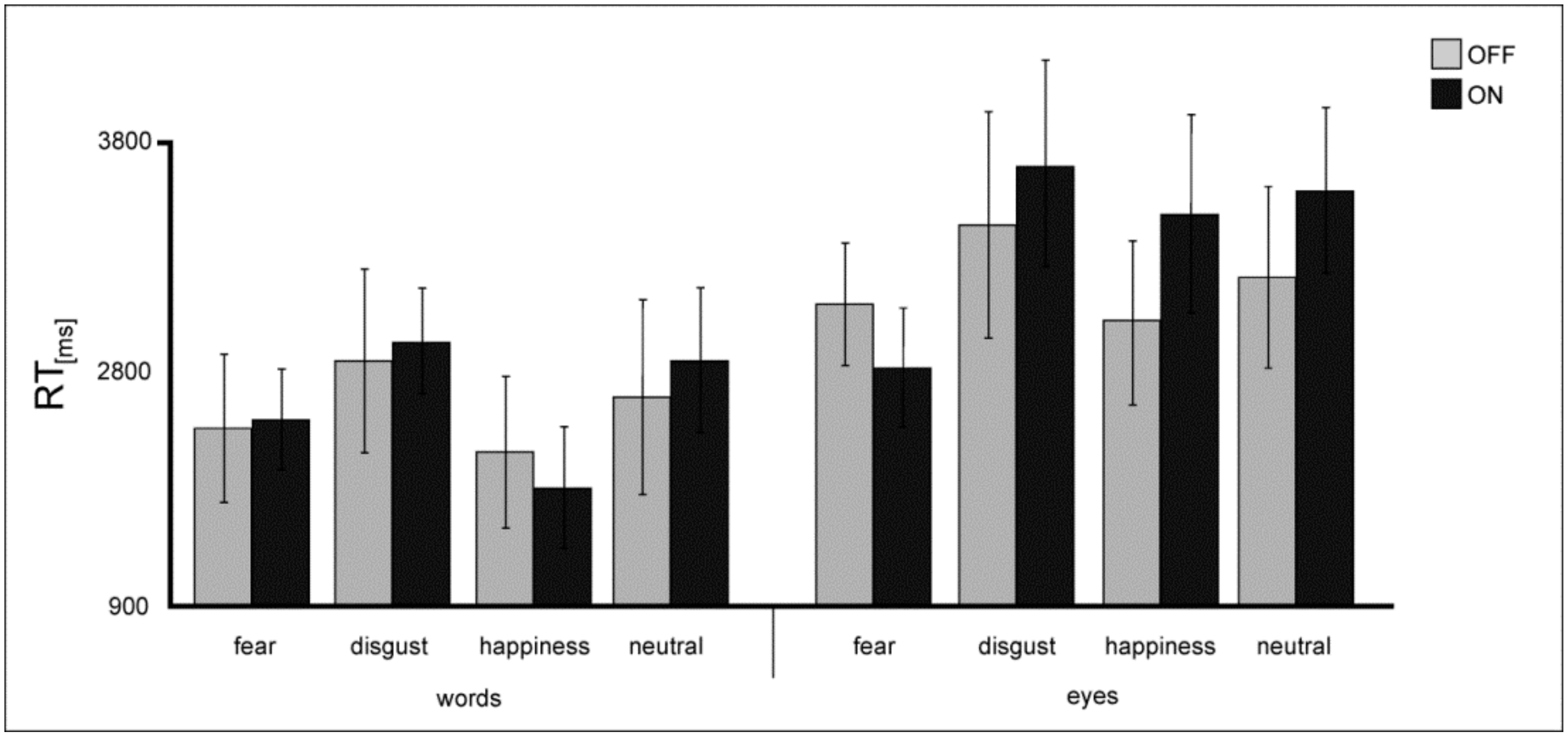
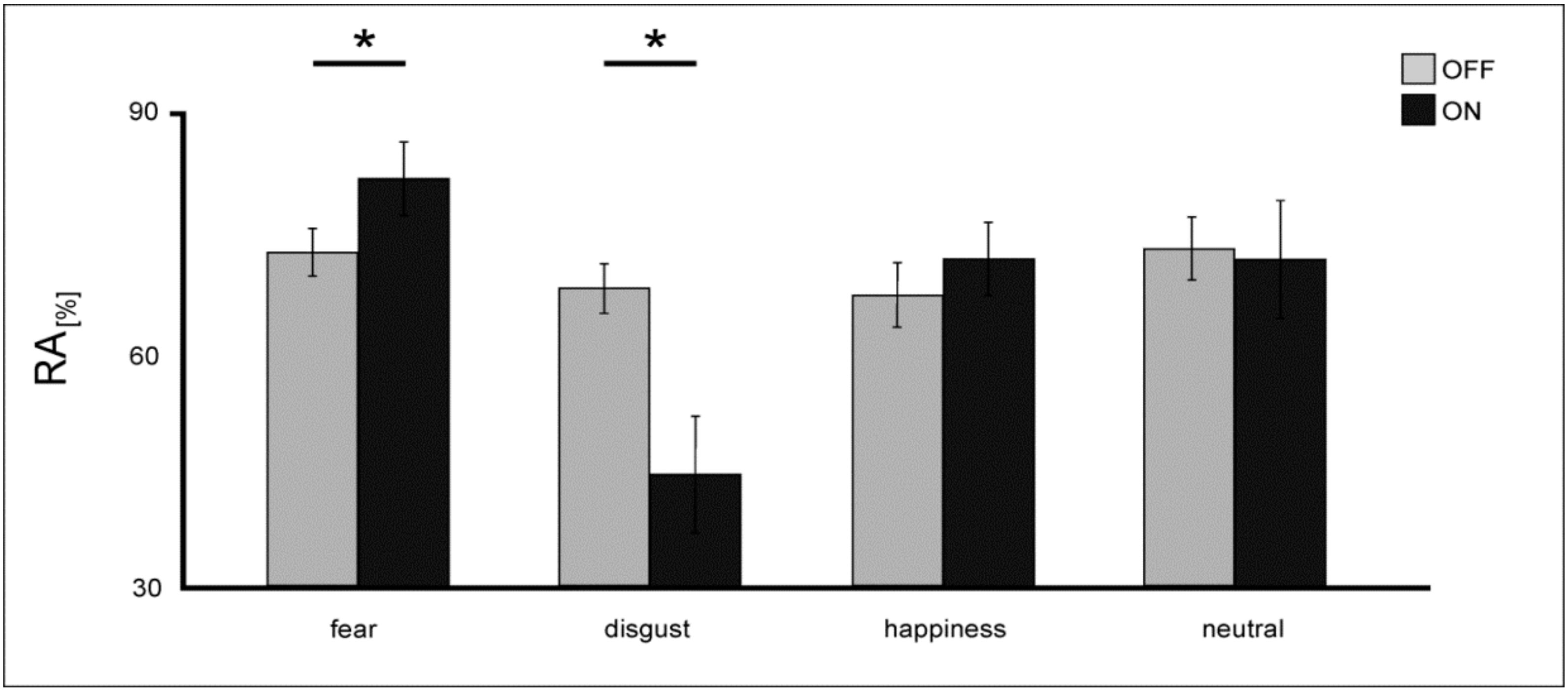
3.3. Explicit Emotional Processing
3.4. Summary Explicit Task
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of variance |
| BAWL-R | Berlin Affective Word List Reloaded |
| DBS | Deep brain stimulation |
| LDT | lexical decision task |
| MRI | Magnetic resonance imaging |
| OFC | orbitofrontal cortex |
| PD | Parkinson’s disease |
| RA | response accuracy |
| RT | reaction times |
| STN | Subthalamic nucleus |
References
- Enrici, I.; Adenzato, M.; Ardito, R.B.; Mitkova, A.; Cavallo, M.; Zibetti, M.; Lopiano, L.; Castelli, L. Emotion processing in Parkinson’s disease: A three-level study on recognition, representation and regulation. PLoS ONE 2015, 10, e0131470. [Google Scholar] [CrossRef] [PubMed]
- Yip, J.T.H.; Lee, T.M.C.; Ho, S.L.; Tsang, K.L.; Li, L.S.W. Emotion recognition in patients with idiopathic Parkinson’s Disease. Mov. Disord. 2003, 18, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Hoshini, T.; Shigemasu, K.; Kawamura, M. Disgust specific impairment of facial expression recognition in Parkinson’s disease. Brain 2006, 129, 707–717. [Google Scholar] [CrossRef] [PubMed]
- Sprengelmeyer, R.; Young, A.W.; Mahn, K.; Schroeder, U.; Woitalla, D.; Büttner, T.; Kuhn, W.; Przuntek, H. Facial expression recognition in people with medicated and unmedicated Parkinson’s disease. Neuropsychologia 2003, 41, 1047–1057. [Google Scholar] [CrossRef]
- Clark, U.S.; Neargarder, S.; Cronin-Golomb, A. Specific impairments in the recognition of emotional facial expressions in Parkinson’s disease. Neuropsychologia 2008, 46, 2300–2309. [Google Scholar] [CrossRef] [PubMed]
- Dujardin, K.; Blairy, S.; Defebvre, L.; Krystkowiak, P.; Hess, U.; Blond, S.; Destee, A. Subthalamic nucleus stimulation induces deficits in decoding emotional facial expressions in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2004, 75, 202–208. [Google Scholar]
- Lawrence, A.D.; Goerendt, I.K.; Brooks, D.J. Impaired recognition of facial expressions of anger in Parkinson’s disease patients acutely withdrawn from dopamine replacement therapy. Neuropsychologia 2007, 45, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Kan, Y.; Kawamura, M.; Hasegawa, Y.; Mochizuki, S.; Nakamura, K. Recognition of emotion from facial, prosodic and written verbal stimuli in Parkinson’s disease. Cortex 2002, 38, 623–630. [Google Scholar] [CrossRef]
- Wagenbreth, C.; Wattenberg, L.; Heinze, H.J.; Zaehle, T. Implicit and explicit processing of emotional facial expressions in Parkinson’s disease. Behav. Brain Res. 2016, 303, 182–190. [Google Scholar] [CrossRef]
- Borg, C.; Bedoin, N.; Bogey, S.; Michael, G.A.; Poujois, A.; Laurent, B.; Thomas-Antérion, C. Implicit and explicit emotional processing in Parkinson’s disease. J. Clin. Exp. Neuropsychol. 2012, 34, 289–296. [Google Scholar] [CrossRef]
- Hershey, T.; Revilla, F.J.; Wernle, A.; Gibson, P.S.; Dowling, J.L.; Perlmutter, J.S. Stimulation of STN impairs aspects of cognitive control in PD. Neurology 2004, 62, 1110–1114. [Google Scholar] [CrossRef] [PubMed]
- Hershey, T.; Campbell, M.C.; Videen, T.O.; Lugar, H.M.; Weaver, P.M.; Hartlein, J.; Karimi, M.; Tabbal, S.D.; Perlmutter, J.S. Mapping Go-No-Go performance within the subthalamic nucleus region. Brain 2010, 133, 3625–3634. [Google Scholar] [CrossRef] [PubMed]
- Frank, M.J.; Seeberger, L.C.; O’Reilly, R.C. By carrot or by stick: Cognitive reinforcement learning in parkinsonism. Science 2004, 306, 1940–1943. [Google Scholar] [CrossRef] [PubMed]
- Zaehle, T.; Wagenbreth, C.; Voges, J.; Heinze, H.J.; Galazky, I. Effects of deep brain stimulation of the subthalamic nucleus on perceptual decision making. Neuroscience 2017, 343, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Irmen, F.; Huebl, J.; Schroll, H.; Brücke, C.; Schneider, G.H.; Hamker, F.H.; Kühn, A.A. Subthalamic nucleus stimulation impairs emotional conflict adaptation in Parkinson’s disease. Soc. Cogn. Affect. Neurosci. 2017, 12, 1594–1604. [Google Scholar] [CrossRef]
- Wagenbreth, C.; Zaehle, T.; Galazky, I.; Voges, J.; Guitart-Masip, M.; Heinze, H.J.; Düzel, E. Deep brain stimulation of the subthalamic nucleus modulates reward processing and action selection in Parkinson patients. J. Neurol. 2015, 262, 1541–1547. [Google Scholar] [CrossRef] [PubMed]
- Fasano, A.; Romito, L.M.; Daniele, A.; Piano, C.; Zinno, M.; Bentivoglio, A.R.; Albanese, A. Motor and cognitive outcome in patients with Parkinson’s disease 8 years after subthalamic implants. Brain 2010, 133, 2664–2676. [Google Scholar] [CrossRef]
- Schneider, F.; Habel, U.; Volkmann, J.; Regel, S.; Kornischka, J.; Sturm, V.; Freund, H.J. Deep brain stimulation of the subthalamic nucleus enhances emotional processing in Parkinson disease. Arch. Gen. Psychiatry 2003, 60, 296–302. [Google Scholar] [CrossRef]
- McIntosh, L.G.; Mannavy, S.; Camalier, C.R.; Folley, B.S.; Albritton, A.; Konrad, P.E.; Charles, D.; Park, S.; Neimat, J.S. Emotion recognition in early Parkinson’s disease patients undergoing deep brain stimulation or dopaminergic therapy: A comparison to healthy participants. Front. Aging Neurosci. 2015, 6, 349. [Google Scholar] [CrossRef]
- Albuquerque, L.; Coelho, M.; Martins, M.; Martins, I.P. STN-DBS does not change emotion recognition in advanced Parkinson’s disease. Parkinsonism Relat. Disord. 2014, 20, 564–565. [Google Scholar] [CrossRef]
- Berney, A.; Panisset, M.; Sadikot, A.F.; Ptito, A.; Dagher, A.; Fraraccio, M.; Savard, G.; Pell, M.; Benkelfat, C. Mood stability during acute stimulator challenge in Parkinson’s disease patients under long-term treatment with subthalamic deep brain stimulation. Mov. Disord. 2007, 22, 1093–1096. [Google Scholar] [CrossRef] [PubMed]
- Péron, J.; Biseul, I.; Leray, E.; Vicente, S.; Le Jeune, F.; Drapier, S.; Drapier, D.; Sauleau, P.; Haegelen, C.; Vérin, M. Subthalamic nucleus stimulation affects fear and sadness recognition in Parkinson’s disease. Neuropsychology 2010, 24, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Geday, J.; Ostergaard, K.; Gjedde, A. Stimulation of subthalamic nucleus inhibits emotional activation of fusiform gyrus. Neuroimage 2006, 33, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Serranová, T.; Jech, R.; Dusek, P.; Sieger, T.; Ruzicka, F.; Urgosik, D.; Ruzicka, E. Subthalamic nucleus stimulation affects incentive salience attribution in Parkinson’s disease. Mov. Disord. 2011, 26, 2260–2266. [Google Scholar] [CrossRef] [PubMed]
- Aiello, M.; Eleopra, R.; Lettieri, C.; Mndani, M.; D’Auria, S.; Belgrado, E.; Piani, A.; De Simone, L.; Rinaldo, S.; Rumiati, R.I. Emotion recognition in Parkinson’s disease after subthalamic deep brain stimulation: Differential effects of microlesion and STN stimulation. Cortex 2014, 51, 35–45. [Google Scholar] [CrossRef]
- Mondillon, L.; Mermillod, M.; Musca, S.C.; Rieu, I.; Vidal, T.; Chambres, P.; Auxiette, C.; Dalens, H.; Marie Coulangeon, L.; Jalenques, I.; et al. The combined effect of subthalamic nuclei deep brain stimulation and L-dopa increases emotion recognition in Parkinson’s disease. Neuropsychologia 2012, 50, 2868–2879. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, U.; Kuehler, A.; Hennenlotter, A.; Haslinger, B.; Tronnier, V.M.; Krause, M.; Pfister, R.; Sprengelmeyer, R.; Lange, K.W.; Ceballos-Baumann, A.O. Facial expression recognition and subthalamic nucleus stimulation. J. Neurol. Neurosurg. Psychiatry 2004, 75, 648–650. [Google Scholar] [CrossRef]
- Drapier, D.; Péron, J.; Leray, E.; Sauleau, P.; Biseul, I.; Drapier, S.; Le Jeune, F.; Travers, D.; Bourguignon, A.; Haegelen, C.; et al. Emotion recognition impairment and apathy after subthalamic nucleus stimulation in Parkinson’s disease have separate neural substrates. Neuropsychologia 2008, 46, 2796–2801. [Google Scholar] [CrossRef]
- Biseul, I.; Sauleau, P.; Haegelen, C.; Trebon, P.; Drapier, D.; Raoul, S.; Drapier, S.; Lallement, F.; Rivier, I.; Lajat, Y.; et al. Fear recognition is impaired by subthalamic nucleus stimulation in Parkinson’s disease. Neuropsychologia 2005, 43, 1054–1059. [Google Scholar] [CrossRef]
- Castner, J.E.; Chenery, H.J.; Copland, D.A.; Coyne, T.J.; Sinclair, F.; Silburn, P.A. Semantic and affective priming as a function of stimulation of the subthalamic nucleus in Parkinson’s disease. Brain 2007, 130, 1395–1407. [Google Scholar] [CrossRef]
- Elias, W.J.; Fu, K.M.; Frysinger, R.C. Cortical and subcortical brain shift during stereotactic procedures. J. Neurosurg. 2007, 107, 983–988. [Google Scholar] [CrossRef] [PubMed]
- Hristova, A.; Lyons, K.; Tröster, A.I.; Pahwa, R.; Wilkinson, S.B.; Koller, W.C. Effect and time course of deep brain stimulation of the globus pallidus and subthalamus on motor features of Parkinson’s disease. Clin. Neuropharmacol. 2000, 23, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Lopiano, L.; Torre, E.; Benedetti, F.; Bergamasco, B.; Perozzo, P.; Pollo, A.; Rizzone, M.; Tavella, A.; Lanotte, M. Temporal changes in movement time during the switch of the stimulators in Parkinson’s disease patients treated by subthalamic nucleus stimulation. Eur. Neurol. 2003, 50, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Võ, M.L.H.; Conrad, M.; Kuchinke, L.; Urton, K.; Hofmann, M.J.; Jacobs, A.M. The Berlin Affective Word List Reloaded (BAWL-R). Behav. Res. Methods 2009, 41, 534–538. [Google Scholar] [CrossRef] [PubMed]
- Briesemeister, B.B.; Kuchinke, L.; Jacobs, A.M. Discrete emotion norms for nouns: Berlin Affective Word List (DENN-BAWL). Behav. Res. Methods 2011, 43, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Ekman, P.; Friesen, W. Pictures of Facial Affect; Consulting Psychologists Press: Palo Alto, CA, USA, 1976. [Google Scholar]
- Vicente, S.; Biseul, I.; Péron, J.; Philippot, P.; Drapier, S.; Drapier, D.; Sauleau, P.; Haegelen, C.; Vérin, M. Subthalamic nucleus stimulation affects subjective emotional experience in Parkinson’s disease patients. Neuropsychologia 2009, 47, 1928–1937. [Google Scholar] [CrossRef] [PubMed]
- Wagenbreth, C.; Rieger, J.; Heinze, H.J.; Zaehle, T. Seeing emotions in the eyes—Inverse priming effects induced by eyes expressing mental states. Front. Psychol. 2014, 5, 1039. [Google Scholar] [CrossRef]
- Phillips, M.L.; Young, A.W.; Senior, C.; Brammer, M.; Andrew, C.; Calder, A.J.; Bullmore, E.T.; Perrett, D.I.; Rowland, D.; Williams, S.C.; et al. A specific neural substrate for perceiving facial expressions of disgust. Nature 1997, 389, 495–498. [Google Scholar] [CrossRef]
- Baggio, H.C.; Segura, B.; Ibarretxe-Bilbao, N.; Valldeoriola, F.; Marti, M.J.; Compta, Y.; Tolosa, E.; Junqué, C. Structural correlates of facial emotion recognition deficits in Parkinson’s disease patients. Neuropsychologia 2012, 50, 2121–2128. [Google Scholar] [CrossRef]
- Calder, A.J.; Keane, J.; Manes, F.; Antoun, N.; Young, A.W. Impaired recognition and experience of disgust following brain injury. Nat. Neurosci. 2000, 3, 1077–1078. [Google Scholar] [CrossRef]
- Leppänen, J.; Hietanen, J.K. Is there more in a happy face than just a big smile? Vis. Cogn. 2007, 15, 468–490. [Google Scholar] [CrossRef]
- Kissler, J.; Koessler, S. Emotionally positive stimuli facilitate lexical decisions-an ERP study. Biol. Psychol. 2011, 86, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Ibarretxe-Bilbao, N.; Junqué, C.; Tolosa, E.; Marti, M.J.; Valldeoriola, F.; Bargallo, N.; Zarei, M. Neuroanatomical correlates of impaired decision-making and facial emotion recognition in early Parkinson’s disease. Eur. J. Neurosci. 2009, 30, 1162–1171. [Google Scholar] [CrossRef] [PubMed]
- Polosan, M.; Droux, F.; Kibleur, A.; Chabardes, S.; Bougerol, T.; David, O.; Krack, P.; Voon, V. Affective modulation of the associative-limbic subthalamic nucleus: Deep brain stimulation in obsessive-compulsive disorder. Transl. Psychiatry 2019, 9, 73. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.L.; Young, A.W.; Scott, S.K.; Calder, A.J.; Andrew, C.; Giampietro, V.; Williams, S.C.; Bullmore, E.T.; Brammer, M.; Gray, J.A. Neural responses to facial and vocal expressions of fear and disgust. Proc. Biol. Sci. 1998, 265, 1809–1817. [Google Scholar] [CrossRef] [Green Version]
- Whalen, P.J.; Rauch, S.L.; Etcoff, N.L.; McInerney, S.C.; Lee, M.B.; Jenike, M.A. Masked presentations of emotional facial expressions modulate amygdala activity without explicit knowledge. J. Neurosci. 1998, 18, 411–418. [Google Scholar] [CrossRef]
- Adolphs, R.; Tranel, D.; Damasio, H.; Damasio, A.R. Fear and human amgydala. J. Neurosci. 1994, 15, 5879–5891. [Google Scholar] [CrossRef]
- Hariri, A.R.; Mattay, V.S.; Tessitore, A.; Fera, F.; Weinberger, D.R. Neocortical modulation of the amygdale response to fearful stimuli. Biol. Psychiatry 2003, 53, 494–501. [Google Scholar] [CrossRef]
- Marinkovic, K.; Trebon, P.; Chauvel, P.; Halgren, E. Localised face processing by the human prefrontal cortex: Face-selective intracerebral potentials and post-lesion deficits. Cogn. Neuropsychol. 2000, 17, 187–199. [Google Scholar] [CrossRef]
- Le Jeune, F.; Péron, J.; Biseul, I.; Fournier, S.; Sauleau, P.; Drapier, S.; Haegelen, C.; Drapier, D.; Millet, B.; Garin, E.; et al. Subthalamic nucleus stimulation affects orbitofrontal cortex in facial emotion recognition: A PET study. Brain 2008, 131, 1599–1608. [Google Scholar] [CrossRef]
- Delaveau, P.; Salgado-Pineda, P.; Witjas, T.; Micallef-Roll, J.; Fakra, E.; Azulay, J.P.; Blin, O. Dopaminergic modulation of amgydala activity during emotion recognition in patients with Parkinson disease. J. Clin. Psychopharamcol. 2009, 29, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Owen, A.M. Cognitive dysfunction in Parkinson’s disease: The role of frontostriatal circuitry. Neuroscientist 2004, 10, 525–537. [Google Scholar] [CrossRef] [PubMed]
- Cools, R. Dopaminergic modulation of cognitive function-implications for L-DOPA treatment in Parkinson’s disease. Neurosci. Biobehav. Rev. 2006, 30, 1–23. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient # | Gender | Age | Disease Duration (years) | Time Since Surgery (months) | LED (mg) | UPDRS- III ON | UPDRS- III OFF | DBS Contacts (l/r) | DBS Voltage (V), Frequency (Hz), Pulse Width (μs) left/right |
|---|---|---|---|---|---|---|---|---|---|
| 1 | female | 74 | 16 | 3 | 225 | 16 | 38 | 1 − G+ / 10 − G+ | 2.5 V, 130 Hz, 60 µs / 2,0 V; 130 Hz, 60 µs |
| 2 | female | 59 | 13 | 4 | 500 | 20 | 2 − 3 − G+ / 10 − 9+ | 2.8 V, 60 Hz, 210 µs / 1,5 V, 60 Hz, 210 µs | |
| 3 | male | 67 | 18 | 77 | 630 | 9 | 3 − G+ / 4 − 5 − 6+ | 4.8 V, 130 Hz, 60 µs / 3,4 V, 130 Hz, 60 µs | |
| 4 | male | 65 | 16 | 15 | 325 | 18 | 32 | G+ 0 − / 8–9 − G+ | 2.7 V, 150 Hz, 60 µs / 3,1 V; 150 Hz, 60 µs |
| 5 | female | 71 | 20 | 7 | 350 | 23 | 38 | 1–2 − G+ / 10 − G+ | 1.3 V, 130 Hz, 60 µs / 1,5 V, 130 Hz, 60 µs |
| 6 | male | 61 | 10 | 16 | 850 | 12 | 32 | 2 − G+ / 10 − G+ | 3.6 V, 110 Hz, 90 µs / 3,4 V, 110 Hz, 90 µs |
| 7 | female | 66 | 11 | 77 | 200 | 16 | 27 | 1 − G+ / 6 − G+ | 2.0 V, 190 Hz, 60 µs / 2,5 V, 190 Hz, 60 µs |
| 8 | male | 63 | 10 | 4 | 200 | 4 | 19 | 2 − G+ / 10 − G+ | 3.1 V, 130 Hz, 90 µs / 3,1 V, 130 Hz, 90 µs |
| 9 | male | 36 | 6 | 14 | 0 | 13 | 38 | 2 − G+ / 10 − G+ | 2.5 V, 200 Hz, 90 µs / 2,7 V, 200 Hz, 90 µs |
| 10 | male | 53 | 10 | 54 | 385 | 15 | 29 | 1 − 2+ / 9 − 11+ | 2.5 V, 180 Hz, 60 µs / 4,4 V, 180 Hz, 60 µs |
| 11 | male | 74 | 13 | 8 | 800 | 22 | 1 − G+ / 5–6 − G+ | 4.5 V, 130 Hz, 60 µs / 5,0 V, 130 Hz, 60 µs | |
| 12 | male | 41 | 7 | 6 | 350 | 19 | 32 | 2 − G+ / 8–10 − G+ | 2.0 V, 130 Hz, 60 µs / 2,1 V, 130 Hz, 60 µs |
| 13 | male | 66 | 8 | 3 | 600 | 11 | 26 | 0 − G+ / 8 − G+ | 1.5 V, 130 Hz, 60 µs / 1,5 V, 130 Hz, 60 µs |
| 14 | male | 70 | 6 | 4 | 0 | 17 | 24 | 1 − 2 + / 9 − 10 + | 3.5 V, 130 Hz, 60 µs / 3,5 V, 130 Hz, 60 µs |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagenbreth, C.; Kuehne, M.; Voges, J.; Heinze, H.-J.; Galazky, I.; Zaehle, T. Deep Brain Stimulation of the Subthalamic Nucleus Selectively Modulates Emotion Recognition of Facial Stimuli in Parkinson’s Patients. J. Clin. Med. 2019, 8, 1335. https://doi.org/10.3390/jcm8091335
Wagenbreth C, Kuehne M, Voges J, Heinze H-J, Galazky I, Zaehle T. Deep Brain Stimulation of the Subthalamic Nucleus Selectively Modulates Emotion Recognition of Facial Stimuli in Parkinson’s Patients. Journal of Clinical Medicine. 2019; 8(9):1335. https://doi.org/10.3390/jcm8091335
Chicago/Turabian StyleWagenbreth, Caroline, Maria Kuehne, Jürgen Voges, Hans-Jochen Heinze, Imke Galazky, and Tino Zaehle. 2019. "Deep Brain Stimulation of the Subthalamic Nucleus Selectively Modulates Emotion Recognition of Facial Stimuli in Parkinson’s Patients" Journal of Clinical Medicine 8, no. 9: 1335. https://doi.org/10.3390/jcm8091335