Nutrition in Cancer Patients


1
University Hospital of Santa Maria, 1649-035 Lisbon, Portugal
2
University of Lisbon, 1649-028 Lisbon, Portugal
3
Centre for Interdisciplinary Research in Health (CIIS) of the Portuguese Catholic University, 1649-023 Lisbon, Portugal
J. Clin. Med. 2019, 8(8), 1211; https://doi.org/10.3390/jcm8081211
Submission received: 3 July 2019
/
Revised: 31 July 2019
/
Accepted: 4 August 2019
/
Published: 14 August 2019
(This article belongs to the Special Issue Nutritional Management and Outcomes in Malnourished Medical Inpatients)
Abstract
:Background: Despite being recognised that nutritional intervention is essential, nutritional support is not widely accessible to all patients. Given the incidence of nutritional risk and nutrition wasting, and because cachexia management remains a challenge in clinical practice, a multidisciplinary approach with targeted nutrition is vital to improve the quality of care in oncology. Methods: A literature search in PubMed and Cochrane Library was performed from inception until 26 March. The search consisted of terms on: cancer, nutrition, nutritional therapy, malnutrition, cachexia, sarcopenia, survival, nutrients and guidelines. Key words were linked using “OR” as a Boolean function and the results of the four components were combined by utilizing the “AND” Boolean function. Guidelines, clinical trials and observational studies written in English, were selected. Seminal papers were referenced in this article as appropriate. Relevant articles are discussed in this article. Results: Recent literature supports integration of nutrition screening/assessment in cancer care. Body composition assessment is suggested to be determinant for interventions, treatments and outcomes. Nutritional intervention is mandatory as adjuvant to any treatment, as it improves nutrition parameters, body composition, symptoms, quality of life and ultimately survival. Nutrition counselling is the first choice, with/without oral nutritional supplements (ONS). Criteria for escalating nutrition measures include: (1) 50% of intake vs. requirements for more than 1–2 weeks; (2) if it is anticipated that undernourished patients will not eat and/or absorb nutrients for a long period; (3) if the tumour itself impairs oral intake. N-3 fatty acids are promising nutrients, yet clinically they lack trials with homogeneous populations to clarify the identified clinical benefits. Insufficient protein intake is a key feature in cancer; recent guidelines suggest a higher range of protein because of the likely beneficial effects for treatment tolerance and efficacy. Amino acids for counteracting muscle wasting need further research. Vitamins/minerals are recommended in doses close to the recommended dietary allowances and avoid higher doses. Vitamin D deficiency might be relevant in cancer and has been suggested to be needed to optimise protein supplements effectiveness. Conclusions: A proactive assessment of the clinical alterations that occur in cancer is essential for selecting the adequate nutritional intervention with the best possible impact on nutritional status, body composition, treatment efficacy and ultimately reducing complications and improving survival and quality of life.
Keywords:
cancer; nutrition; nutritional therapy; nutritional support; malnutrition; cachexia; sarcopenia; survival1. Introduction
Cancer is a complex disease that results from multiple interactions between genes and the environment, and is regarded as one of the current leading causes of mortality worldwide [1,2]. Metabolic and nutritional alterations can influence survival and recovery of cancer patients: malnutrition, sarcopenia and cachexia [3,4]. Malnutrition ensues from an inflammatory state that promotes anorexia and consequently, weight loss. It is highly prevalent in cancer patients [5] as 15 to 40% of patients report weight loss at diagnosis [6]. It is estimated that 40 to 80% of all cancer patients will be malnourished during the course of the disease. Furthermore, malnutrition can influence treatment outcomes, delay wound healing, worsen muscle function and increase the risk of post-operative complications. It can also impair tolerance and response to antineoplastic treatments, which can in turn lead to extended hospital stay, increase the risk for treatment interruptions, and possible reduced survival [7,8]. Sarcopenia is characterised by a decrease in lean body mass with an impact both on strength and physical function that may decrease the quality of life [9]. As cancer-related weight loss in obese patients cannot be identified by a low body mass index (BMI), sarcopenic obesity, defined as low lean body mass in obese patients, is frequently overlooked [10]. In these patients, changes in body composition result in an increased metabolic risk, and it seems to be a significant predictor of treatment related adverse events [11,12]. Cancer cachexia is a complex multifactorial syndrome that results from a combination of metabolic alterations, systemic inflammation and decreased appetite. It is characterised by an involuntary sustained weight loss and loss of skeletal muscle mass, with or without loss of fat mass that are irreversible by conventional nutritional support [13].
In addition to the disease, antineoplastic treatments and/or surgery have a significant impact on patients’ nutritional status [14,15,16]. During chemotherapy (CT), more than 50% of patients experience dysgeusia, nausea, vomiting and mucositis, and radiotherapy (RT) related complications are also common. It is also established that poor nutritional status increases surgical morbidity and post-surgical complications [17]. Nutritional intervention in cancer patients aim to identify, prevent and treat malnutrition through nutritional counselling with or without oral nutritional supplements (ONS) or via artificial nutrition, i.e., enteral or parenteral nutrition [18,19,20], as well as to address metabolic and nutritional alterations that influence patients’ recovery and survival [19,20]. Despite the fact that nutritional intervention is a key component, nutritional support is not widely accessible to all patients at nutritional risk [21,22,23]. Additionally, given the incidence of nutritional risk in cancer and the fact that the management of cachexia remains a challenge in clinical practice [24], a multidisciplinary approach is vital to define efficient strategies that can improve quality of care in cancer patients. According to the reviewed data and guidelines, nutritional intervention should be central and adjuvant to any treatment and should be included in the multidisciplinary approach mandatory in oncology. This will allow for more adequate and efficient results in these patients. Multidisciplinary follow-up, with early and regular nutritional intervention, is of major importance in oncology, thus being a key factor for successful treatment and recovery. The present article aims to provide insights and an overview of the most recent literature regarding key nutritional aspects in cancer patients.
Based on this framework, a literature search in PubMed and Cochrane Library was performed from inception until 26 March. The search consisted of terms: cancer, nutrition, nutritional therapy, malnutrition, cachexia, sarcopenia, survival, nutrients, guidelines. Key words were linked using “OR” as a Boolean function and the results of the four components were combined by utilizing the “AND” Boolean function. Guidelines, clinical trials and observational studies written in English, were selected. Seminal papers in the area, even if dated outside the search timeline, were referenced in this article as appropriate.
2. Results
2.1. Nutritional Screening and Assessment
Screening for nutritional risk as early as possible allows for the identification of patients at risk of becoming malnourished [25]. Screening should be done as early as possible, and recent literature suggests that it should be done at diagnosis or at hospital admission; screening should be repeated in the course of treatment for referral for evaluation if needed [19,21,23,25,26,27]. Evidence supports the integration of malnutrition screening in cancer patients care. The adequate tool for screening undernutrition should be brief and easy to fill, inexpensive, highly sensitive and have good specificity [25]. MUST (Malnutrition Universal Screening Tool) and NRS-2002 (Nutritional Risk Screening-2002) are considered suitable [28,29,30]; the MNA (Mini Nutritional Assessment) is a suitable tool for nutritional assessment in the senior population [19,23].
When nutritional risk is present, screening should be followed by comprehensive nutritional assessment to better determine the course of nutritional intervention. It seems there is no consensus on the best method to perform this assessment, but SGA (Subjective Global Assessment) and PG-SGA (Patient Generated-Subjective Global Assessment) have been validated for nutritional assessment of adult oncology patients [25,26,31].
When used isolated, weight loss is ineffective to detect malnutrition, as it has low sensitivity for metabolic changes that occur in cancer patients. Yet, its early and regular assessment, combined with the evaluation of nutritional intake, BMI and inflammatory status is a standard clinical recommendation [19,26]. As for BMI, it has low sensitivity to detect changes in the nutritional status, especially in obese patients, thus it should only be used combined with other assessment tools [26,32].
Body composition provides valuable information in the management of cancer patients, as imaging methods detect loss of muscle mass as well as fatty muscle infiltration [2]. In cancer patients at risk for malnutrition, sarcopenia and cachexia, muscle mass should be assessed [19,21]. Methods available are dual X-ray absorptiometry (DEXA), computed tomography scans at the level of the 3rd vertebra or bioimpedance analysis (BIA). Additionally, it has been recommended that nutritional assessment should be performed for the stages of cancer cachexia, as nutritional intervention is most effective in the stages of precachexia and cachexia [13].
2.2. Nutritional Intervention
In order to tackle nutritional deterioration, gathering objective data on nutritional status and its evolution throughout the disease course is of prime concern. Different cancer types or locations display different nutritional patterns that require tailored nutritional therapy. Nutritional deterioration is a multifactorial end-result determined by cancer-related and nutrition- and/or metabolic-related factors. Proper nutrition can alleviate symptom burden, improve health across the cancer continuum, support cancer survivorship [33,34,35,36] and is a hallmark of successful cancer treatment.
Nutritional interventions will vary according to patients’ medical history, type and stage of cancer, as well as to the response to treatment. If the patient can eat and has a functional gastrointestinal tract, nutritional counselling, with or without ONS should be the elected intervention to address altered nutritional demands due to treatment or disease [19,21,26]. ONS may be necessary, as a means to compensate for lower food intake and to try to prevent nutritional deterioration during the course of treatments. Monitoring compliance with the selected nutritional intervention is essential.
2.2.1. Individualised Nutritional Counselling
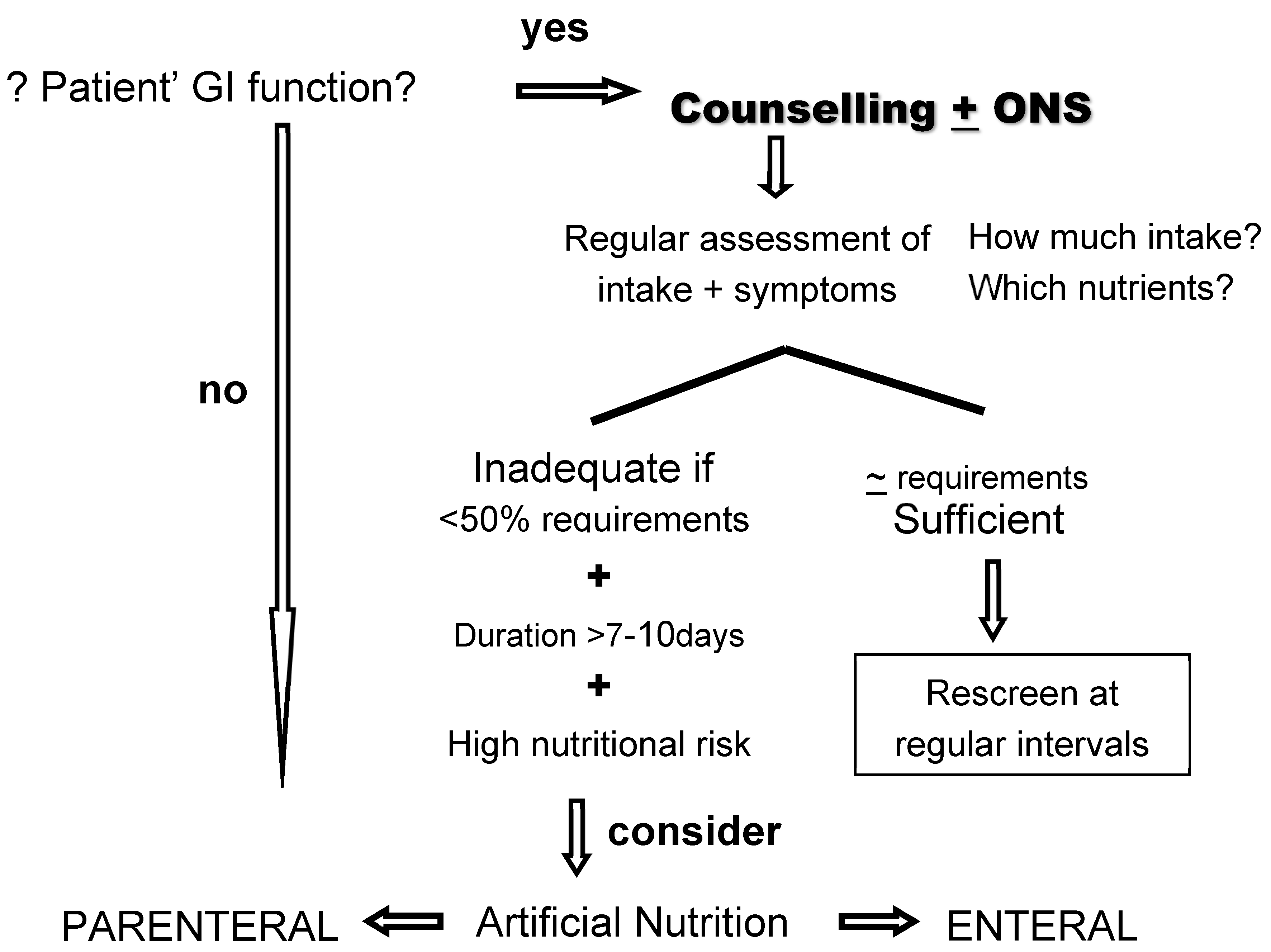
In clinical practice, oral nutrition is always the priority. Oral nutrition is the preferred route of feeding as it is a significant part of the patient’s daily routine and does contribute substantially to the patients’ autonomy [19]. It represents a privileged time to spend with family and friends, avoiding the tendency for isolation. The acknowledgement that the prescribed diet is individualized, adapted and adequate to individual needs, empowers the patient with a feeling of control, thus it is also a highly effective approach for psychological modulation. All these factors may potentially contribute to improve the patients’ quality of life, and may modulate acute and late treatment morbidity. The referral for a nutrition professional responsible for the individualised dietary counselling should always be based on decision-making plans (Figure 1).
As clinicians we have to recognise the dimensions that are determinant for the patients. Indeed, the diet is the only factor that the patient feels he/she can control during the whole course of treatments and interventions. Also, an adequate food intake is recognised by the patient as well as by the family and caregivers, as essential to maintain the daily activity, energy, functional capacity and to overcome treatments more successfully. Notably, nutritional wasting is common regardless of the cancer stage (curative, adjuvant, to palliative) and is an independent predictor of poor physical function, lower quality of life, surgical complications, and reduced survival [3,10,13,37]. Cancer wasting is characterised by muscle mass deterioration that occurs in more than 50% of newly diagnosed cancer patients, in comparison with 15% prevalence in healthy individuals of similar age [38]. Since both muscle mass and adipose tissue play a role in oncological outcomes, strategies to optimize body composition are an important part of successful cancer therapy. Hence, a major goal of nutrition intervention is to favourably influence body composition, with the potential to improve cancer therapy outcomes, morbidities and ultimately, prognosis.
To be effective, individualised counselling has to be based on a thorough assessment of various nutritional and clinical parameters: nutritional status and dietary intake, usual dietary pattern, intolerances or food aversions, patients’ psychological status, autonomy, cooperation, need for help or support of others in the act of eating. A thorough symptom assessment is also mandatory (Table 1).
Individualised nutritional counselling taking into consideration patients’ clinical condition and symptoms, was the most effective nutrition intervention, assuring a sustained and adequate diet, which was able to overcome the predictable deterioration subsequent to RT [35,36,39,40,41,42]. Positive effects were experienced in the long term with a possible impact of patients’ prognosis [43] as recently showed in a randomized trial, the preliminary results of which were presented in the ESPEN Congress in 2018. Another randomised trial of nutritional therapy showed that intervention had an impact in maintaining patients’ nutritional status and function [39]. In this study, individualised intensive nutrition counselling was compared with individualised on-demand nutrition counselling by a dietician prior to and during oncologic treatment. On-demand nutrition counselling requested by physician/nurse referral, seemed not inferior to intensive counselling; thus, these results do emphasise the importance of establishing multimodal nutrition teams to effectively and timely screen and orient patients for adequate nutrition [39]. Several guidelines to date do include nutritional counselling as their standard of care for malnourished patients or at risk of malnutrition [19,20,21,23,26,27] or during anti-neoplastic treatments in head-neck (HNC), oesophageal and colorectal cancers as these patients are in particular risk of malnutrition due to tumour location and irradiated area [14].
If/when oral nutrition is inadequate/insufficient, artificial nutrition should be considered [19,20,21,23,26,27]. Criteria for the escalation in nutritional measures are: (1) inadequate food intake (<50% of requirements) is anticipated for more than 10 days due to surgery or chemotherapy (CT)/radiotherapy (RT); (2) if food intake is less than 50% of the requirements for more than one to two weeks; (3) if it is anticipated that undernourished patients will not be able to eat and/or absorb the adequate amount of nutrients for a long period time, due to antineoplastic treatments; (4) if the tumour mass itself impairs oral intake and food progression through the upper GI tract. The decision between enteral nutrition (EN) and parenteral nutrition (PN) must take into account the site of the tumour, its extent, complications, treatment plan and intent, prognosis, patients’ overall physical status and the duration of the nutritional support [19,20,21,23,26,27,44].
2.2.2. Artificial Nutrition
If the intestinal functions are preserved, EN should be preferred in order to maintain gut integrity and reduce bacterial translocation [45], as well as to reduce infectious complications [19,20,21,23,26]. A standard polymeric feeding formula should be preferred. EN is recommended in undernourished or at-risk patients during CT if undernutrition is present or if inadequate food intake is present or anticipated [19,22,23,27,46]. Systematic artificial nutrition during CT treatment is not recommended [19,20,21,23,26]. In radiation-induced severe mucositis or in obstructive tumours of the head-neck or thorax, either PEG or nasogastric tube are recommended [19,20]. EN is contraindicated in: intestinal obstruction or ileus, severe shock, intestinal ischaemia, high output fistula, severe intestinal haemorrhage, intestinal insufficiency due to radiation enteritis, short bowel syndrome, peritoneal carcinomatosis chylothorax [19,21,23,26]. In these situations, or whenever EN is insufficient, a combination of EN and PN or PN alone should be considered [19,21,23,26]. As for PN, it should be initiated early [19,21,23,26] whenever indicated. PN is the first option of nutritional support in cases of intestinal failure; whenever macro and micronutrient’ requirements can only be fulfilled via the parenteral route, long term artificial nutrition as home parenteral nutrition (HPN) is standard recommendation [19,44,47,48].
As for the macronutrients in PN, amino acids (AA) requirement of cancer patients relies on: negative balance between whole body protein synthesis and breakdown, doses of AA closer to 2 g/kg/day may be required to control catabolism and stimulate synthesis vs. 0.8 g/kg/day as recommended for healthy subjects [49], and for older subjects and chronic disease, most recent clinical guidelines recommend >1.0 g/kg/day of protein. Hence, to support protein balance, up to 1.5 g/kg/day or more of protein is the consensual recommendation. In the nutritive PN admixtures, essential AA should be present in approximately 50% of AA and branched chain AA should account for the remainder 50% of total AA [50]. In what concerns fat as an energy substrate, the most consensual regimens have fat accounting for ≈50% of non-protein calories [51,52].
Recently, PN as a supplemental route of nutrient administration (SHPN) emerged as a possible resource to optimise nutrient delivery. Prospective studies [53,54,55,56,57] on SHPN suggest a possible benefit in energy balance, increased body fat, greater maximum exercise capacity and QoL. A recent randomised trial showed that SHPN may prevent loss of MM in patients with incurable gastrointestinal cancer [57]. Hence, there is yet insufficient evidence to recommend SHPN in cancer patients to improve QoL and nutrition parameters. Additionally, practice of HPN differs between countries; most do not consider the use of PN if there is a functional gastrointestinal tract, while others may consider its use if it is according to the will of the patient [58,59,60].
Refeeding syndrome can occur when severe shifts in fluids and electrolytes happen in severely malnourished patients receiving EN or PN, and it may cause hypophosphatemia, hypokalaemia, hypomagnesaemia, thiamine deficiency, changes in sodium, glucose and fluid balance and also in protein and lipid metabolism [19,21]. Its prevention is recommended when BMI < 16 kg/m2 or in the presence of unintentional weight loss >15% within the last three to six months or whenever there is little or no nutritional intake for more than 10 days or if there are decreased levels of potassium, phosphate or magnesium prior to feeding. If a severe decrease in food intake occurs for at least five days, it is recommended a gradual increase in nutrition over several days, and no more than 50% of the calculated energy requirements should be supplied during the first two days of feeding [19,25]. The identified fluid and electrolytes imbalances should be corrected, and the circulatory volume, fluid balance, heart rate and rhythm, as well as clinical status, should be monitored closely. Attention to the refeeding syndrome risk is currently contemplated in guidelines for cancer management [19,20,21,22,23,26,27].
2.2.3. Surgery
In order to minimise the metabolic stress response and catabolism associated with surgery in undernourished patients, the enhanced recovery after surgery program (ERAS) is recommended for all cancer patients undergoing curative or palliative surgery [18,22,61]. Within ERAS protocol the following principles should be followed: Screening for malnutrition and give additional nutritional support if necessary [18,22]; avoid preoperative fasting; preoperative carbohydrate treatment should be considered as well as the reestablishment of oral feeding on the first postoperative day; and early mobilisation [18,22]. To avoid preoperative fasting, patients with no risk of aspiration, are allowed to eat solid food until six hours and drink clear fluids until two hours before anaesthesia [18].
In oncologic surgical patients, with moderate to severe nutritional risk, nutritional support is recommended before and after surgery [18,25]. If severe malnutrition is present, delaying surgery may be necessary [18,25]. When submitted to major surgery, nutritional support should be provided routinely, with particular attention to elderly sarcopenic patients.
Besides the ERAS protocol, an early start of nutritional supplementation can significantly diminish the degree of weight loss and incidence of complications [22,25]. If it is anticipated that after surgery, the patient will be unable to eat for more than seven days, it is advised to start nutrition therapy even in well-nourished patients [18,22,25]. After surgery, oral nutrition should also be preferred to EN and the latter should be preferred to PN. If oral intake is possible, it should start after surgery without interruption, after assessing individual tolerance. If oral nutrition is not possible, EN should be initiated within 24 h, preferring standard polymeric enteral formulae if adequate [25].
2.2.4. Radiotherapy and Chemotherapy
Oral mucositis, dysphagia and diarrhoea are common complications of RT and/or CT treatments [12,13,14,15,16,17,18,19,20,21,22]. During RT, nutritional counselling is also recommended, especially in HNC, thorax and gastrointestinal (GI) tract cancers [12,13,14,15,16,17,18,19,20,21,22,23]. When deemed necessary, ONS should be provided [62], and when severe mucositis is present, artificial nutrition should be considered [23]. When dietary counselling and ONS are insufficient to reduce weight loss or if in the presence of severe mucositis or obstructive tumours of the head or neck or thorax, artificial nutrition should be considered [19,20,23]. In patients treated with RT or chemoradiotherapy, PN is not recommended [19], and it should only be considered when adequate nutrition cannot be assured with oral or EN [19].
2.3. Specific Nutrients
Nutritional strategies that potentially allow better management of cancer have been widely investigated, but few have reached conclusive results.
2.3.1. Protein
Many patients with cancer do not meet the recommended intake (1.2–1.5 g/kg/day), and not even the one for healthy individuals (0.8 g/kg/day) [63]. Limited protein intake ensues mainly from nutrition impact symptoms that affect dietary intake [64]. Recent guidelines do suggest a higher range of protein intake (1.2–1.5 g/kg/day), because of the positive results of higher protein intake in protein balancing and in maintaining muscle mass. Of additional interest is a recent study showing an inverse association between red meat consumption and seven-year mortality among 992 individuals with stage III colon cancer [65], suggesting that higher protein intake may actually be beneficial in cancer.
Interventions with amino acids have been tested in cancer, aiming to optimise nutritional status and counteract muscle mass wasting. They include supplementation with branched chain amino acids (leucine, isoleucine and valine) [63], β-hydroxy β-methyl butyrate, carnitine and creatine. Yet further research is needed to clarify potential benefits.
As for glutamine, its supplementation in cases of oral mucositis or to prevent/treat diarrhoea during pelvic RT, is not recommended [19,22,26]. As for its use when PN is required for patients undergoing haematopoietic stem cell transplant, guidelines are not identical: there is a fair graded recommendation for eventual use of 0.2–0.5 g/kg/day [26], and the indication that there is not enough evidence to recommend for or against glutamine to reduce anticancer therapy side effects, especially in high dose protocols [19]. In what concerns its potential to improve muscle mass, there is not enough data to support it.
2.3.2. Eicosapentaenoic Acid and Fish Oil
Eicosapentaenoic acid (EPA) has been identified as a promising nutrient with appointed clinical benefits. Several mechanisms have been proposed to explain the potential benefits of EPA on the body composition: inhibition of catabolic stimuli by modulating the production of pro-inflammatory cytokines and enhancing insulin sensitivity that induces protein synthesis. Intervention studies showed that EPA may attenuate deterioration of nutritional status and may aid in improving calorie and protein intake. Recent systematic reviews found that EPA can reduce inflammation and has a potential to modulate the nutritional status/body composition [66,67]. Furthermore, some studies suggest that n−3 fatty acids inhibit proliferation of cancer cells [68] and might decrease CT toxicity [69]. Given the large number of studies reporting a positive impact of n−3 fatty acids on the muscle mass, it is likely that this would be a practical and effective intervention for preventing loss of muscle without significant side effects [19]. It is noteworthy that the strength of recommendation somewhat differs for the use of n−3 fatty acids supplementation in weight losing cancer patients not responding to standard nutritional therapy. This recommendation has been rated as strong [26] and weak [19]. Nevertheless, both guidelines are inclined to consider supplementation with long chain fatty acids and fish oil to decrease systemic inflammation and improve appetite, food intake and body weight.
Trials with homogeneous patient populations regarding cancer type, stage, anti-neoplastic regimens, supplement dosage and modality of administration are needed to clarify clinical benefits. Indeed, it is noteworthy that in view of the modest survival benefits of CT/RT in some cancers, important issues for physicians are to optimize well-being, quality of life via nutritional status and adequate body composition [70].
2.3.3. Micronutrients
Because of the adverse effects of therapy and restricted diet of many patients, the American Institute for Cancer Research [71], American Cancer Society [72] and the European Society for Clinical Nutrition and Metabolism—ESPEN [19] support the use of a multivitamin-multimineral supplement in doses close to the recommended dietary allowance. High doses of vitamins and minerals are discouraged in the absence of specific deficiencies [19,20]. Vitamin D deficiency might be relevant in cancer [19]; also, an association has been reported between low vitamin D and muscle wasting. As a consequence, vitamin D may be needed to optimise protein supplements effectiveness. In light of the recent literature, vitamin D supplementation with 600–800 international units (RDA) in cancer patients can be beneficial in the context of preventing muscle wasting, but further research is needed.
3. Discussion
In cancer, deterioration and muscle wasting result from the combination of reduced nutrient absorption, alterations in appetite, taste and/or dietary intake, hormone-induced metabolic changes and cancer-related immune activation with cytokine release. Regardless of the underlying mechanisms, cancer-related weight loss is a multidimensional manifestation that worsens patients’ well-being, tolerance to antineoplastic therapies and prognosis. Clinically speaking, weight loss is frequent in cancer patients, and depending on the location of the tumour, it is present in 15 to 40% of cancer patients at diagnosis. Weight loss is frequently the first sign of the nutritional alterations that occur in the course of the disease and is associated with poor prognosis, reduced quality of life and morbidity [62]. Cancer cachexia can be defined as ‘a multi-factorial syndrome defined by an ongoing loss of skeletal muscle mass (with or without loss of fat mass) that cannot be fully reversed by conventional nutritional support. It leads to progressive functional impairment. Its pathophysiology is characterized by a negative protein and energy balance driven by a variable combination of reduced food intake and abnormal metabolism’. The agreed diagnostic criterion for cachexia was weight loss >5%, or weight loss >2% in individuals already showing depletion of body weight (BMI < 20 kg/m2) or of skeletal muscle (sarcopenia). Assessment for classification and clinical management should also include the following domains: ‘anorexia/reduced food intake, catabolic drive, muscle mass and strength, functional and psychosocial impairment’ [13].
The main nutritional problem in cancer is wasting of muscle mass, acknowledged to be a predictor of lower quality of life, impaired functionality, surgical complications and shortened survival [10,63,73,74]. Of note that sarcopenia occurs independently of loss of weight or of fat mass. Thus, a clinically relevant phenotype that also emerged in cancer is characterised by sarcopenia with excessive fat mass. Additionally, to the previous studies demonstrating the major impact of muscle mass depletion on survival and treatment toxicity [73,74], a recent study in a cohort of head-neck cancer patients, showed that patients with cachexia had a worse disease-free survival compared with non-cachectic patients [12,39].
Bearing this in mind, the clinical efforts and priority given to improve treatment outcomes, will logically have to include nutritional intervention and adequacy of body composition. The search for an effective nutritional intervention that improves body composition (preservation of muscle mass and muscle quality) is of utmost importance for clinicians and patients, given the implications for prognosis. Early detection of malnutrition and cachexia should be part of a multimodal approach to improve both patient-centred and oncology outcomes [47].
4. Conclusions
In the present article, the most recent guidelines for the management of cancer patients, as well as original studies in nutrition and cancer, were included. Nutrition is a central factor in oncology, influencing the development of the disease, tumour inherent symptoms, response to, and recovery after anti-neoplastic treatment(s), thus having a strong impact on the quality of life and prognosis of the disease. A main nutritional feature is wasting of muscle mass, strongly associated with decreased functional capacity, higher incidence of chemotherapy toxicity, increased hospitalization and complication rate, as well as mortality. Nutritional risk screening and assessment in cancer patients allows for the early detection of malnourished patients and also for a prompt nutritional intervention aiming to prevent nutritional deterioration and muscle wasting. A proactive assessment of the clinical alterations that occur during treatments and during the disease course, is essential for selecting the adequate nutritional intervention, aiming for the best impact on patients’ outcomes. Early tailored intervention has the potential to improve body composition and treatment’ efficacy, and as evidence stands, it is an obligatory adjuvant intervention, with the likelihood of improving prognosis of the disease itself.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Fearon, K.; Barber, M. Moses A: The cancer cachexia syndrome. Surg. Oncol. Clin. N. Am. 2001, 10, 109–126. [Google Scholar] [CrossRef]
- Mattox, T.W. Cancer Cachexia: Cause, Diagnosis, and Treatment. Nutr. Clin. Pract. 2017, 32, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.C.; Caan, B.J.; Meyerhardt, J.A.; Weltzien, E.; Xiao, J.; Feliciano, E.M.C.; Kroenke, C.H.; Castillo, A.; Kwan, M.L.; Prado, C.M. The deterioration of muscle mass and radiodensity is prognostic of poor survival in stage I–III colorectal cancer: A population-based cohort study (C-SCANS). J. Cachex Sarcopenia Muscle 2018, 9, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Demark-Wahnefried, W.; Peterson, B.L.; Winer, E.P.; Marks, L.; Aziz, N.; Marcom, P.K.; Blackwell, K.; Rimer, B.K. Changes in Weight, Body Composition, and Factors Influencing Energy Balance Among Premenopausal Breast Cancer Patients Receiving Adjuvant Chemotherapy. J. Clin. Oncol. 2001, 19, 2381–2389. [Google Scholar] [CrossRef] [PubMed]
- De Wys, W.D.; Begg, C.; Lavin, P.T.; Band, P.R.; Bennett, J.M.; Bertino, J.R.; Cohen, M.H.; Douglass, H.O., Jr.; Engstrom, P.F.; Ezdinli, E.Z.; et al. Prognostic effect of weight loss prior to chemotherapy in cancer patients. Am. J. Med. 1980, 69, 491–497. [Google Scholar] [CrossRef]
- Wigmore, S.J.; Plester, C.E.; Ross, J.A.; Fearon, K.C.H.; Wigmore, S. Contribution of anorexia and hypermetabolism to weight loss in anicteric patients with pancreatic cancer. BJS 1997, 84, 196–197. [Google Scholar] [CrossRef]
- Belghiti, J.; Langonnet, F.; Bourstyn, E.; Fekete, F. Surgical implications of malnutrition and immunodeficiency in patients with carcinoma of the esophagus. Br. J. Surg. 1983, 70, 339–341. [Google Scholar] [CrossRef]
- Mantzorou, M.; Koutelidakis, A.; Theocharis, S.; Giaginis, C. Clinical Value of Nutritional Status in Cancer: What is its Impact and how it Affects Disease Progression and Prognosis? Nutr. Cancer 2017, 69, 1–26. [Google Scholar] [CrossRef]
- Ravasco, P.; Grillo, I.M.; Vidal, P.; Camilo, M. Nutritional Deterioration in Cancer: The Role of Disease and Diet. Clin. Oncol. 2003, 15, 443–450. [Google Scholar] [CrossRef]
- Prado, C.M.; Cushen, S.J.; Orsso, C.E.; Ryan, A.M. Sarcopenia and cachexia in the era of obesity: Clinical and nutritional impact. Proc. Nutr. Soc. 2016, 75, 188–198. [Google Scholar] [CrossRef]
- Bazzan, A.J.; Newberg, A.B.; Cho, W.C.; Monti, D.A. Diet and nutrition in cancersurvivorship and palliative care. Evid. Based Complement. Alternat. Med. 2013, 2013, 917647. [Google Scholar] [CrossRef] [PubMed]
- Orell-Kotikangas, H.; Österlund, P.; Mäkitie, O.; Saarilahti, K.; Ravasco, P.; Schwab, U.; Mäkitie, A.A. Cachexia at diagnosis is associated with poor survival in head and neck cancer patients. Acta Oto-Laryngol. 2017, 137, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G.; et al. Definition and classification of cancer cachexia: An international consensus statement. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef]
- Donaldson, S. Nutritional consequences of radiotherapy. Cancer Res. 1997, 37, 2407–2413. [Google Scholar]
- Chao, K.S.C.; Perez, C.A.; Brady, L.W. (Eds.) Fundamentals of patient management. In Radiation Oncology: Management Decisions; Lippincot-Raven: Philadelphia, PA, USA, 2014; pp. 1–13. [Google Scholar]
- Blauwhoff-Buskermolen, S.; Versteeg, K.S.; De Van Der Schueren, M.A.; Braver, N.R.D.; Berkhof, J.; Langius, J.A.; Verheul, H.M. Loss of Muscle Mass During Chemotherapy Is Predictive for Poor Survival of Patients with Metastatic Colorectal Cancer. J. Clin. Oncol. 2016, 34, 1339–1344. [Google Scholar] [CrossRef]
- Van der Schueren, M.A.; Van Leeuwen, P.A.; Sauerwein, H.P.; Kuik, D.J.; Snow, G.B.; Quak, J.J. Assessment of malnutrition parameters in head and neck cancer patients and their relation to postoperative complications. Head Neck 1997, 19, 419–425. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. ESPEN guideline: Clinical nutrition in surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef] [Green Version]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef]
- Arends, J.; Baracos, V.; Bertz, H.; Bozzetti, F.; Calder, P.; Deutz, N.; Erickson, N.; Laviano, A.; Lisanti, M.; Lobo, D.; et al. ESPEN expert group recommendations for action against cancer-related malnutrition. Clin. Nutr. 2017, 36, 1187–1196. [Google Scholar] [CrossRef] [Green Version]
- De Las Peñas, R.; Majem, M.; Perez-Altozano, J.; Virizuela, J.A.; Cancer, E.; Diz, P.; Donnay, O.; Hurtado, A.; Jimenez-Fonseca, P.; Ocon, M.J. SEOM clinical guidelines on nutrition in cancer patients (2018). Clin. Transl. Oncol. 2019, 21, 87–93. [Google Scholar] [CrossRef] [Green Version]
- Raspé, C.; Flöther, L.; Schneider, R.; Bucher, M.; Piso, P. Best practice for perioperative management of patients with cytoreductive surgery and HIPEC. Eur. J. Surg. Oncol. 2017, 43, 1013–1027. [Google Scholar] [CrossRef]
- French Speaking Society of Clinical Nutrition and Metabolism (SFNEP). Clinical nutrition guidelines of the French Speaking Society of Clinical Nutrition and Metabolism (SFNEP): Summary of recommendations for adults undergoing non-surgical anticancer treatment. Dig. Liver Dis. 2014, 46, 667–674. [Google Scholar] [CrossRef]
- Prado, C.M.; Sawyer, M.B.; Ghosh, S.; Lieffers, J.R.; Esfandiari, N.; Antoun, S.; Baracos, V. Central tenet of cancer cachexia therapy: Do patients with advanced cancer have exploitable anabolic potential? Am. J. Clin. Nutr. 2013, 98, 1012–1019. [Google Scholar] [CrossRef]
- Benoist, S.; Brouquet, A. Nutritional assessment and screening for malnutrition. J. Visc. Surg. 2015, 152 (Suppl. 1), S3–S7. [Google Scholar] [CrossRef]
- Thompson, K.L.; Elliott, L.; Fuchs-Tarlovsky, V.; Levin, R.M.; Voss, A.C.; Piemonte, T. Rd Oncology Evidence-Based Nutrition Practice Guideline for Adults. J. Acad. Nutr. Diet. 2017, 117, 297–310. [Google Scholar] [CrossRef]
- Talwar, B.; Donnelly, R.; Skelly, R.; Donaldson, M. Nutritional management in head and neck cancer: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S32–S40. [Google Scholar] [CrossRef] [Green Version]
- Orell-Kotikangas, H.; Österlund, P.; Saarilahti, K.; Ravasco, P.; Schwab, U.; Mäkitie, A.A. NRS-2002 for pre-treatment nutritional risk screening and nutritional status assessment in head and neck cancer patients. J. Support. Care Cancer 2015, 23, 1495–1502. [Google Scholar] [CrossRef]
- Boléo-Tomé, C.; Monteiro Grillo, I.; Camilo, M.E.; Ravasco, P. Validation of the Malnutrition Universal Screening Tool (MUST) in cancer. Br. J. Nutr. 2012, 108, 343–348. [Google Scholar] [CrossRef]
- Boléo-Tomé, C.; Chaves, M.; Monteiro-Grillo, I.; Camilo, M.; Ravasco, P. Teaching Nutrition Integration: MUST Screening in Cancer. Oncologist 2011, 16, 239–245. [Google Scholar] [CrossRef] [Green Version]
- Ottery, F. Definition of standardised nutritional assessment and interventional pathways in oncology. Nutrition 1996, 12, s15–s19. [Google Scholar] [CrossRef]
- Ortiz, C. Analysis of clinical guidelines in oncology. Nutr. Hosp. 2016, 33 (Suppl. 1), 40–49. [Google Scholar]
- Ravasco, P.; Monteiro-Grillo, I.; Camilo, M.E. Does nutrition influence quality of life in cancer patients undergoing radiotherapy? Radiother. Oncol. 2003, 67, 213–220. [Google Scholar] [CrossRef]
- Monteiro-Grillo, I.; Vidal, P.M.; Camilo, M.E.; Ravasco, P. Cancer: Disease and nutrition are key determinants of patients’ quality of life. Support. Care Cancer 2004, 12, 246–252. [Google Scholar] [CrossRef]
- Ravasco, P.; Monteiro Grillo, I.; Marques Vidal, P.; Camilo, M.E. Dietary conseling improves patient outcomes: A prospective, randomized, controlled trial in colorectal cancer patients undergoing radiotherapy. J. Clin. Oncol. 2005, 23, 1431–1438. [Google Scholar] [CrossRef]
- Ravasco, P.; Vidal, P.M.; Camilo, M.E.; Monteiro-Grillo, I.; Monteiro-Grillo, I. Impact of nutrition on outcome: A prospective randomized controlled trial in patients with head and neck cancer undergoing radiotherapy. Head Neck 2005, 27, 659–668. [Google Scholar] [CrossRef]
- Martin, L.; Senesse, P.; Gioulbasanis, I.; Antoun, S.; Bozzetti, F.; Deans, C.; Strasser, F.; Thoresen, L.; Jagoe, R.T.; Chasen, M.; et al. Diagnostic criteria for the classification of cancer-associated weight loss. J. Clin. Oncol. 2015, 33, 90–99. [Google Scholar] [CrossRef]
- Von Haehling, S.; Morley, J.E.; Anker, S.D. An overview of sarcopenia: Facts and numbers on prevalence and clinical impact. J. Cachexia Sarcopenia Muscle 2010, 1, 129–133. [Google Scholar] [CrossRef]
- Orell-Kotikangas, H.; Österlund, P.; Saarilahti, K.; Ravasco, P.; Schwab, U.; Mäkitie, A.A. Nutritional Counseling for Head and Neck Cancer Patients Undergoing (Chemo) Radiotherapy-A Prospective Randomized Trial. Front. Nutr. 2019, 18, 22. [Google Scholar] [CrossRef]
- Van Bokhorst-de van der Schueren, M.A. Nutritional support strategies for malnourished cancer patients. Eur. J. Oncol. Nurs. 2005, 9 (Suppl. 2), S74–S83. [Google Scholar] [CrossRef]
- Bauer, J.; Isenring, E.; Ferguson, M. Dietary counseling: Evidence in chemotherapy patients. Support. Oncol. 2008, 6, 354–355. [Google Scholar]
- Isenring, E.A.; Bauer, J.D.; Capra, S. Nutrition Support Using the American Dietetic Association Medical Nutrition Therapy Protocol for Radiation Oncology Patients Improves Dietary Intake Compared with Standard Practice. J. Am. Diet. Assoc. 2007, 107, 404–412. [Google Scholar] [CrossRef] [Green Version]
- Ravasco, P.; Monteiro Grillo, I.; Camilo, M. Dietary individualized counseling benefits in colorectal cancer: The long term follow-up of a randomized controlled trial of nutritional therapy. Am. J. Clin. Nutr. 2012, 96, 1346–1353. [Google Scholar] [CrossRef]
- Staun, M.; Pironi, L.; Bozzetti, F.; Baxter, J.; Forbes, A.; Joly, F.; Jeppesena, P.; Morenog, J.; Hebuterne, X.; Pertkiewicz, M.; et al. ESPEN Guidelines on Parenteral Nutrition: Home Parenteral Nutrition (HPN) in Adult Patients. Available online: http://espen.info/documents/0909/Home Parenteral Nutrition in adults.pdf (accessed on 17 July 2019).
- Souza, N.C.S.; Simões, B.P.; Júnior, A.A.J.; Chiarello, P.G. Changes in Intestinal Permeability and Nutritional Status after Cytotoxic Therapy in Patients with Cancer. Nutr. Cancer 2014, 66, 576–582. [Google Scholar] [CrossRef]
- O’Reilly, D.; Fou, L.; Hasler, E.; Hawkins, J.; O’Connell, S.; Pelone, F.; Callaway, M.; Campbell, F.; Capel, M.; Charnley, R.; et al. Diagnosis and management of pancreatic cancer in adults: A summary of guidelines from the UK National Institute for Health and Care Excellence. Pancreatology 2018, 18, 962–970. [Google Scholar] [CrossRef]
- Lis, C.G.; Gupta, D.; Lammersfeld, C.A.; Markman, M.; Vashi, P.G. Role of nutritional status in predicting quality of life outcomes in cancer—A systematic review of the epidemiological literature. Nutr. J. 2012, 11, 27. [Google Scholar] [CrossRef]
- Nightingale, J.; Young, A.; Hawthorne, B.; McKee, R.; McKinlay, A.; Rafferty, G.; Protheroe, S.; Culkin, A.; Eastwood, J.; Farrer, K.; et al. Position Statement from BIFA Committee. Available online: https://www.bapen.org.uk/nutrition-support/parenteral-nutrition/position-statement-from-bifa-committee (accessed on 17 July 2019).
- Bozzetti, F.; Bozzetti, V. Is the intravenous supplementation of amino acid to cancer patients adequate? A critical appraisal of literature. Clin. Nutr. 2013, 32, 142–146. [Google Scholar] [CrossRef]
- Wolfe, R.R. The 2017 Sir David P Cuthbertson lecture. Amino acids and muscle protein metabolism in critical care. Clin. Nutr. 2018, 37, 1093–1100. [Google Scholar] [CrossRef]
- Körber, J.; Pricelius, S.; Heidrich, M.; Muller, M.J. Increased lipid utilization in weight losing and weight stable cancer patients with normal body weight. Eur. J. Clin. Nutr. 1999, 53, 740–745. [Google Scholar] [CrossRef] [Green Version]
- Cao, D.-X.; Wu, G.-H.; Zhang, B.; Quan, Y.-J.; Wei, J.; Jin, H.; Jiang, Y.; Yang, Z.-A. Resting energy expenditure and body composition in patients with newly detected cancer. Clin. Nutr. 2010, 29, 72–77. [Google Scholar] [CrossRef]
- Finocchiaro, C.; Gervasio, S.; Agnello, E.; Appiano, S.; Bertetto, O.; Ciuffreda, L.; Montrucchio, G.; Luisa, A.M.; D’andrea, F.; Domeniconi, D.; et al. Multicentric study on home parenteral nutrition in advanced cancer patients. Riv. Ital. Nutr. Parenter. Enter. 2002, 20, 98–107. [Google Scholar]
- Seys, P.; Tadmouri, A.; Senesse, P.; Radji, A.; Rotarski, M.; Balian, A.; Culine, S.; Dufour, P.; Chambrier, C. Home parenteral nutrition in elderly patients with cancer: An observational prospective study. Bull. Cancer 2014, 101, 243–249. [Google Scholar] [CrossRef]
- Culine, S.; Chambrier, C.; Tadmouri, A.; Senesse, P.; Seys, P.; Radji, A.; Rotarski, M.; Balian, A.; Dufour, P. Home parenteral nutrition improves quality of life and nutritional status in patients with cancer: A French observational multicentre study. Support. Care Cancer 2014, 22, 1867–1874. [Google Scholar] [CrossRef]
- Vashi, P.G.; Dahlk, S.; Popiel, B.; Lammersfeld, C.A.; Ireton-Jones, C.; Gupta, D. A longitudinal study investigating quality of life and nutritional outcomes in advanced cancer patients receiving home parenteral nutrition. BMC Cancer 2014, 14, 593. [Google Scholar] [CrossRef]
- Girke, J.; Seipt, C.; Markowski, A.; Luettig, B.; Schettler, A.; Momma, M.; Schneider, A.S. Quality of Life and Nutrition Condition of Patients Improve Under Home Parenteral Nutrition: An Exploratory Study. Nutr. Clin. Pract. 2016, 31, 659–665. [Google Scholar] [CrossRef]
- Keane, N.; Fragkos, K.C.; Patel, P.S.; Bertsch, F.; Mehta, S.J.; Di Caro, S.; Rahman, F. Performance status, prognostic scoring, and parenteral nutrition requirements predict survival in patients with advanced cancer receiving home parenteral nutrition. Nutr. Cancer 2018, 70, 73–82. [Google Scholar] [CrossRef]
- Bozzetti, F.; Arends, J.; Lundholm, K.; Micklewright, A.; Zürcher, G.; Muscaritoli, M. ESPEN Guidelines on Parenteral Nutrition: Non-surgical oncology. Clin. Nutr. 2009, 28, 445–454. [Google Scholar] [CrossRef]
- Scolapio, J.; Picco, M.; Tarrosa, V. Enteral versus parenteral nutrition: The patient’s preference. J. Parenter. Enter. Nutr. 2002, 26, 248–250. [Google Scholar] [CrossRef]
- Obermair, A.; Simunovic, M.; Isenring, L.; Janda, M. Nutrition interventions in patients with gynecological cancers requiring surgery. Gynecol. Oncol. 2017, 145, 192–199. [Google Scholar] [CrossRef]
- Baldwin, C.; Weekes, C.E. Dietary counselling with or without oral nutritional supplements in the management of malnourished patients: A systematic review and meta-analysis of randomised controlled trials. J. Hum. Nutr. Diet. 2012, 25, 411–426. [Google Scholar] [CrossRef]
- Deutz, N.E.; Safar, A.; Schutzler, S.; Memelink, R.; Ferrando, A.; Spencer, H.; Van Helvoort, A.; Wolfe, R.R. Muscle protein synthesis in cancer patients can be stimulated with a specially formulated medical food. Clin. Nutr. 2011, 30, 759–768. [Google Scholar] [CrossRef] [Green Version]
- Omlin, A.; Blum, D.; Wierecky, J.; Haile, S.R.; Ottery, F.D.; Strasser, F. Nutrition impact symptoms in advanced cancer patients: Frequency and specific interventions, a case–control study. J. Cachex Sarcopenia Muscle 2013, 4, 55–61. [Google Scholar] [CrossRef]
- Van Blarigan, E.L.; Fuchs, C.S.; Niedzwiecki, D.; Zhang, S.; Saltz, L.B.; Mayer, R.J.; Mowat, R.B.; Whittom, R.; Hantel, A.; Benson, A.; et al. Association of Survival with Adherence to the American Cancer Society Nutrition and Physical Activity Guidelines for Cancer Survivors After Colon Cancer Diagnosis: The CALGB 89803/Alliance Trial. JAMA Oncol. 2018, 4, 783–790. [Google Scholar] [CrossRef]
- Papallardo, G.; Almeida, A.; Ravasco, P. Eicosapentaenoic acid in cancer: Does it improve body composition and modulate metabolism? Nutrition 2015, 31, 549–555. [Google Scholar] [CrossRef]
- Ravasco, P.; Lavriv, D.; Neves, P. Should omega-3 be used in cancer cachexia? Clin. Nutr. ESPEN 2018, 25, 18–25. [Google Scholar]
- Hering, J.; Garrean, S.; Dekoj, T.R.; Razzak, A.; Saied, A.; Trevino, J.; Babcock, T.A.; Espat, N.J. Inhibition of Proliferation by Omega-3 Fatty Acids in Chemoresistant Pancreatic Cancer Cells. Ann. Surg. Oncol. 2007, 14, 3620–3628. [Google Scholar] [CrossRef]
- Murphy, R.A.; Mourtzakis, M.; Mazurak, V.C. n-3 polyunsaturated fatty acids: The potential role for supplementation in cancer. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 246–251. [Google Scholar] [CrossRef]
- Geisler, C.; Prado, C.; Müller, M. Inadequacy of Body Weight-Based Recommendations for Individual Protein Intake—Lessons from Body Composition Analysis. Nutrients 2017, 9, 23. [Google Scholar] [CrossRef]
- Norman, H.A.; Butrum, R.R.; Feldman, E.; Picciano, M.F.; Rivlin, R.; Simopoulos, A.; Wargovich, M.J.; Weisburger, E.K.; Zeisel, S.H.; Heber, D.; et al. The Role of Dietary Supplements during Cancer Therapy. J. Nutr. 2003, 133, 3794S–3799S. [Google Scholar] [CrossRef] [Green Version]
- Rock, C.L.; Doyle, C.; Demark-Wahnefried, W.; Meyerhardt, J.; Courneya, K.S.; Schwartz, A.L.; Bandera, E.V.; Hamilton, K.K.; Grant, B.; McCullough, M.; et al. Nutrition and physical activity guidelines for cancer survivors. CA Cancer J. Clin. 2012, 62, 242–274. [Google Scholar] [CrossRef] [Green Version]
- Stene, G.B.; Helbostad, J.L.; Amundsen, T.; Sørhaug, S.; Hjelde, H.; Kaasa, S.; Grønberg, B.H. Changes in skeletal muscle mass during palliative chemotherapy in patients with advanced lung cancer. Acta Oncol. 2015, 54, 340–348. [Google Scholar] [CrossRef]
- Lieffers, J.R.; Bathe, O.F.; Fassbender, K.; Winget, M.; Baracos, V.E. Sarcopenia is associated with postoperative infection and delayed recovery from colorectal cancer resection surgery. Br. J. Cancer 2012, 107, 931–936. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Evidence based decision making plan.


{kind=link}
Table 1.
Common causes for a poor nutrient intake in cancer patients.
|
© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ravasco, P. Nutrition in Cancer Patients. J. Clin. Med. 2019, 8, 1211. https://doi.org/10.3390/jcm8081211
AMA Style
Ravasco P. Nutrition in Cancer Patients. Journal of Clinical Medicine. 2019; 8(8):1211. https://doi.org/10.3390/jcm8081211
Chicago/Turabian StyleRavasco, Paula. 2019. "Nutrition in Cancer Patients" Journal of Clinical Medicine 8, no. 8: 1211. https://doi.org/10.3390/jcm8081211
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.