LRRTM4 and PCSK5 Genetic Polymorphisms as Markers for Cognitive Impairment in A Hypotensive Aging Population: A Genome-Wide Association Study in Taiwan

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Phenotypic Data
2.2. Genome-Wide Association Study (GWAS) and Imputation
2.3. Statistics
3. Results
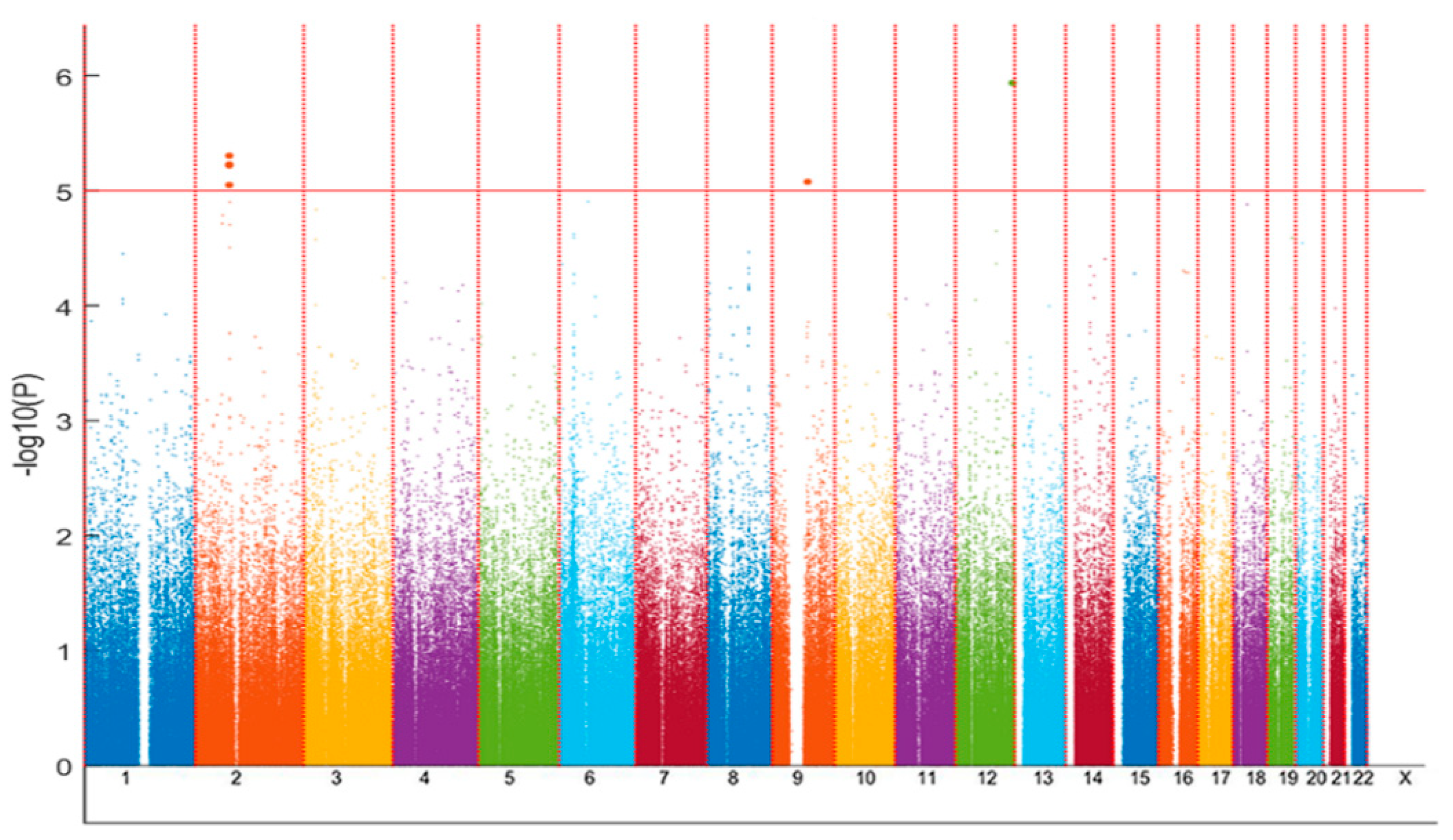
3.1. Discovery SNP-Based Association Analysis to Explore Candidate SNPs for Hypotension-Related CI
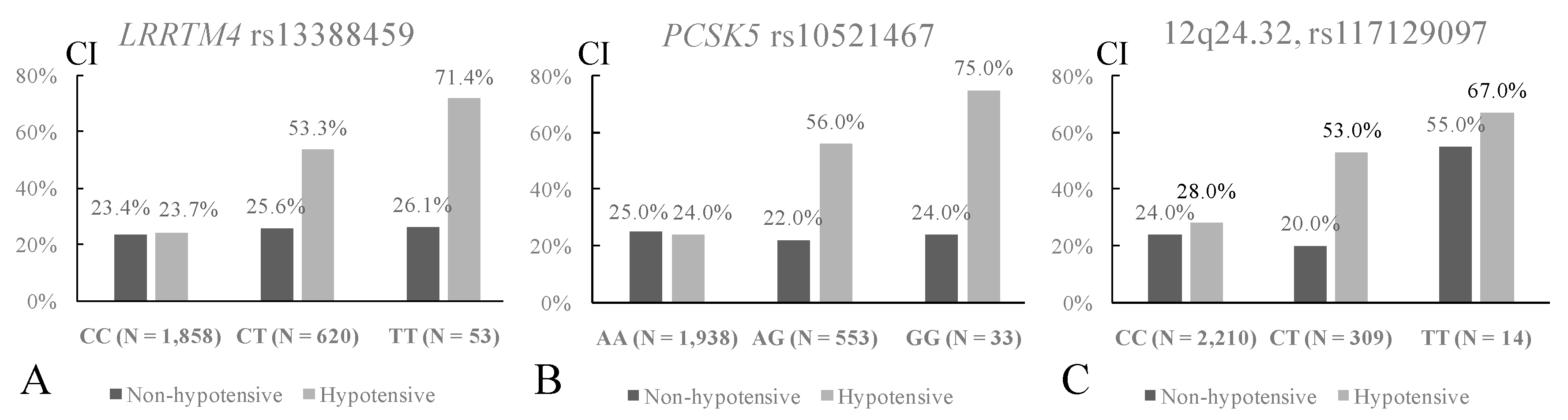
3.2. Associations of The Eight Identified SNPs with Hypotension or with CI in The Whole Cohort
3.3. Interaction Effects of SNPs and Hypotension on CI in the Whole Cohort
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Razay, G.; Williams, J.; King, E.; Smith, A.D.; Wilcock, G. Blood pressure, dementia and Alzheimer's disease: The OPTIMA Longitudinal Study. Dement. Geriatr. Cogn. Disord. 2009, 28, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C.; Scherr, P.A.; Hebert, L.E.; Glynn, R.J.; Bennett, D.A.; Evans, D.A. Association of incident Alzheimer disease and blood pressure measured from 13 years before to 2 years after diagnosis in a large community study. Arch. Neurol. 2001, 58, 1640–1646. [Google Scholar] [CrossRef] [PubMed]
- Gabin, J.M.; Tambs, K.; Saltvedt, I.; Sund, E.; Holmen, J. Association between blood pressure and Alzheimer disease measured up to 27 years prior to diagnosis: The HUNT Study. Alzheimers Res. Ther. 2017, 9, 37. [Google Scholar] [CrossRef] [PubMed]
- Moretti, R.; Torre, P.; Antonello, R.M.; Manganaro, D.; Vilotti, C.; Pizzolato, G. Risk factors for vascular dementia: Hypotension as a key point. Vasc. Health Risk Manag. 2008, 4, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Novak, V.; Hajjar, I. The relationship between blood pressure and cognitive function. Nat. Rev. Cardiol. 2010, 7, 686–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glynn, R.J.; Beckett, L.A.; Hebert, L.E.; Morris, M.C.; Scherr, P.A.; Evans, D.A. Current and remote blood pressure and cognitive decline. JAMA 1999, 281, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Waldstein, S.R.; Giggey, P.P.; Thayer, J.F.; Zonderman, A.B. Nonlinear relations of blood pressure to cognitive function: The Baltimore Longitudinal Study of Aging. Hypertension 2005, 45, 374–379. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.; Viitanen, M.; Fratiglioni, L.; Winblad, B. Low blood pressure and dementia in elderly people: The Kungsholmen project. BMJ 1996, 312, 805–808. [Google Scholar] [CrossRef]
- Qiu, C.; von Strauss, E.; Fastbom, J.; Winblad, B.; Fratiglioni, L. Low blood pressure and risk of dementia in the Kungsholmen project: A 6-year follow-up study. Arch. Neurol. 2003, 60, 223–228. [Google Scholar] [CrossRef]
- Qiu, C.; von Strauss, E.; Winblad, B.; Fratiglioni, L. Decline in blood pressure over time and risk of dementia: A longitudinal study from the Kungsholmen project. Stroke 2004, 35, 1810–1815. [Google Scholar] [CrossRef]
- Skoog, I.; Lernfelt, B.; Landahl, S.; Palmertz, B.; Andreasson, L.A.; Nilsson, L.; Persson, G.; Oden, A.; Svanborg, A. 15-year longitudinal study of blood pressure and dementia. Lancet 1996, 347, 1141–1145. [Google Scholar] [CrossRef]
- Verghese, J.; Lipton, R.B.; Hall, C.B.; Kuslansky, G.; Katz, M.J. Low blood pressure and the risk of dementia in very old individuals. Neurology 2003, 61, 1667–1672. [Google Scholar] [CrossRef]
- Swan, G.E.; Carmelli, D.; Larue, A. Systolic blood pressure tracking over 25 to 30 years and cognitive performance in older adults. Stroke 1998, 29, 2334–2340. [Google Scholar] [CrossRef]
- Ricci, F.; De Caterina, R.; Fedorowski, A. Orthostatic Hypotension: Epidemiology, Prognosis, and Treatment. J. Am. Coll. Cardiol. 2015, 66, 848–860. [Google Scholar] [CrossRef]
- De La Torre, J.C. Impaired cerebromicrovascular perfusion: Summary of evidence in support of its causality in Alzheimer's disease. Ann. N. Y. Acad. Sci. 2000, 924, 136–152. [Google Scholar] [CrossRef]
- Toth, P.; Tarantini, S.; Csiszar, A.; Ungvari, Z. Functional vascular contributions to cognitive impairment and dementia: Mechanisms and consequences of cerebral autoregulatory dysfunction, endothelial impairment, and neurovascular uncoupling in aging. Am. J. Physiol. Heart. Circ. Physiol. 2017, 312, H1–H20. [Google Scholar] [CrossRef]
- Allan, L.M.; Ballard, C.G.; Allen, J.; Murray, A.; Davidson, A.W.; McKeith, I.G.; Kenny, R.A. Autonomic dysfunction in dementia. J. Neurol. Neurosurg. Psychiatry 2007, 78, 671–677. [Google Scholar] [CrossRef]
- McGrath, E.R.; Beiser, A.S.; DeCarli, C.; Plourde, K.L.; Vasan, R.S.; Greenberg, S.M.; Seshadri, S. Blood pressure from mid- to late life and risk of incident dementia. Neurology 2017, 89, 2447–2454. [Google Scholar] [CrossRef]
- Walker, K.A.; Power, M.C.; Gottesman, R.F. Defining the Relationship between Hypertension, Cognitive Decline, and Dementia: A Review. Curr. Hypertens. Rep. 2017, 19, 24. [Google Scholar] [CrossRef]
- Rahman, F.; McEvoy, J.W. The J-shaped Curve for Blood Pressure and Cardiovascular Disease Risk: Historical Context and Recent Updates. Curr. Atheroscler. Rep. 2017, 19, 34. [Google Scholar] [CrossRef]
- Waldstein, S.R.; Brown, J.R.; Maier, K.J.; Katzel, L.I. Diagnosis of hypertension and high blood pressure levels negatively affect cognitive function in older adults. Ann. Behav. Med. 2005, 29, 174–180. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar]
- Franceschini, N.; Le, T.H. Genetics of hypertension: Discoveries from the bench to human populations. Am J. Physiol. Renal Physiol. 2014, 306, F1–F11. [Google Scholar] [CrossRef]
- Chen, C.H.; Yang, J.H.; Chiang, C.W.K.; Hsiung, C.N.; Wu, P.E.; Chang, L.C.; Chu, H.W.; Chang, J.; Song, I.W.; Yang, S.L.; et al. Population structure of Han Chinese in the modern Taiwanese population based on 10,000 participants in the Taiwan Biobank project. Hum. Mol. Genet. 2016, 25, 5321–5331. [Google Scholar] [CrossRef] [Green Version]
- Fan, C.T.; Lin, J.C.; Lee, C.H. Taiwan Biobank: A project aiming to aid Taiwan's transition into a biomedical island. Pharmacogenomics 2008, 9, 235–246. [Google Scholar] [CrossRef]
- Chen, Y.C.; Tsao, H.H.; Chu, Y.C.; Wang, J.J.; Lee, J.D.; Chang, P.Y.; Hsu, W.C. Exploring the Spectrum of Subcortical Hyperintensities and Cognitive Decline. J. Neuropsychiatry Clin. Neurosci. 2018, 30, 130–138. [Google Scholar] [CrossRef]
- Purcell, S.; Neale, B.; Todd-Brown, K.; Thomas, L.; Ferreira, M.A.; Bender, D.; Maller, J.; Sklar, P.; de Bakker, P.I.; Daly, M.J.; et al. PLINK: A tool set for whole-genome association and population-based linkage analyses. Am. J. Hum. Genet. 2007, 81, 559–575. [Google Scholar] [CrossRef]
- Chang, C.C.; Chow, C.C.; Tellier, L.C.; Vattikuti, S.; Purcell, S.M.; Lee, J.J. Second-generation PLINK: Rising to the challenge of larger and richer datasets. Gigascience 2015, 4, 7. [Google Scholar] [CrossRef]
- Ranganathan, P.; Pramesh, C.S.; Aggarwal, R. Common pitfalls in statistical analysis: Logistic regression. Perspect Clin. Res. 2017, 8, 148–151. [Google Scholar]
- Zlokovic, B.V. Neurovascular pathways to neurodegeneration in Alzheimer's disease and other disorders. Nat. Rev. Neurosci. 2011, 12, 723–738. [Google Scholar] [CrossRef]
- Roppongi, R.T.; Karimi, B.; Siddiqui, T.J. Role of LRRTMs in synapse development and plasticity. Neurosci. Res. 2017, 116, 18–28. [Google Scholar] [CrossRef]
- Fagerberg, L.; Hallstrom, B.M.; Oksvold, P.; Kampf, C.; Djureinovic, D.; Odeberg, J.; Habuka, M.; Tahmasebpoor, S.; Danielsson, A.; Edlund, K.; et al. Analysis of the human tissue-specific expression by genome-wide integration of transcriptomics and antibody-based proteomics. Mol. Cell Proteomics 2014, 13, 397–406. [Google Scholar] [CrossRef]
- Laurén, J.; Airaksinen, M.S.; Saarma, M.; Timmusk, T. A novel gene family encoding leucine-rich repeat transmembrane proteins differentially expressed in the nervous system. Genomics 2003, 81, 411–421. [Google Scholar] [CrossRef]
- Siddiqui, T.J.; Tari, P.K.; Connor, S.A.; Zhang, P.; Dobie, F.A.; She, K.; Kawabe, H.; Wang, Y.T.; Brose, N.; Craig, A.M. An LRRTM4-HSPG complex mediates excitatory synapse development on dentate gyrus granule cells. Neuron 2013, 79, 680–695. [Google Scholar] [CrossRef]
- Choi, S.; Korstanje, R. Proprotein convertases in high-density lipoprotein metabolism. Biomark Res. 2013, 1, 27. [Google Scholar] [CrossRef]
- Turpeinen, H.; Seppala, I.; Lyytikainen, L.P.; Raitoharju, E.; Hutri-Kahonen, N.; Levula, M.; Oksala, N.; Waldenberger, M.; Klopp, N.; Illig, T.; et al. A genome-wide expression quantitative trait loci analysis of proprotein convertase subtilisin/kexin enzymes identifies a novel regulatory gene variant for FURIN expression and blood pressure. Hum. Genet. 2015, 134, 627–636. [Google Scholar] [CrossRef]
- Chen, S.; Cao, P.; Dong, N.; Peng, J.; Zhang, C.; Wang, H.; Zhou, T.; Yang, J.; Zhang, Y.; Martelli, E.E.; et al. PCSK6-mediated corin activation is essential for normal blood pressure. Nat. Med. 2015, 21, 1048–1053. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Non-Hypotensive n = 2367 | Hypotensive n = 166 | p-Value |
|---|---|---|---|
| Age (years) | 64.01 ± 2.89 | 64.43 ± 2.95 | 0.07 |
| Male sex (n, %) | 1243, 52.5 | 45, 27.1 | <0.0001 |
| Education (years) | 4.91 ± 1.24 | 4.80 ± 1.40 | 0.24 |
| Self-reported HTN (n, %) | 656, 27.7 | 20, 12.1 | <0.0001 |
| Self-report DM (n, %) | 267, 11.3 | 23, 13.9 | 0.31 |
| Alcohol (n, %) | 158, 6.7 | 5, 3.0 | 0.06 |
| Smoking (n, %) | 736, 31.1 | 35, 21.1 | 0.007 |
| Body mass index (kg/m2) | 24.54 ± 3.10 | 22.82 ± 3.05 | <0.0001 |
| Resting SBP (mmHg) | 133.57 ± 19.84 | 108.74 ± 15.97 | <0.0001 |
| Resting DBP (mmHg) | 78.39 ± 11.28 | 56.42 ± 5.04 | <0.0001 |
| Pulse pressure (mmHg) | 55.18 ± 13.78 | 52.33 ± 14.6 | 0.015 |
| HR (/min) | 69.46 ± 9.16 | 68.58 ± 9.40 | 0.235 |
| MMSE < 26 (n, %) | 568, 24.0 | 56, 33.7 | 0.0049, 0.029 * |
| Gene | Locus | SNP | Position | A1/A2 | MAF (hypotensive CI/NC) | OR (95% CI), p-Value, p-Value * |
|---|---|---|---|---|---|---|
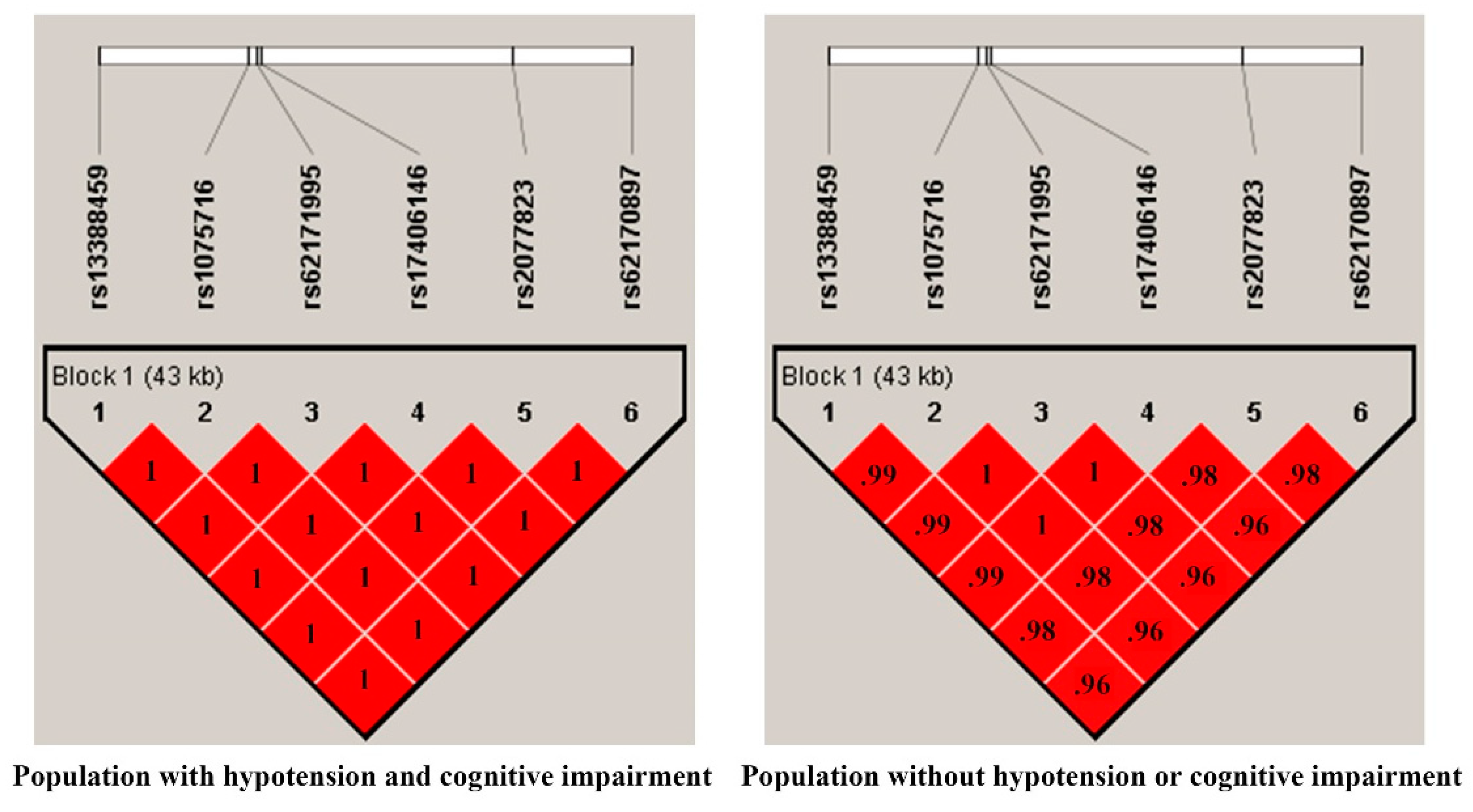
| LRRTM4 (intron variations) | 2p12 | rs13388459 | 77215497 | T/C | 0.30/0.14 | 2.85 (1.81–4.49), 6.07 × 10−6, 6.08 × 10−6 |
| rs1075716 | 77227586 | C/T | 0.30/0.14 | 2.85 (1.81–4.49), 5.99 × 10−6, 5.96 × 10−6 | ||
| rs62171995 | 77228320 | A/G | 0.30/0.14 | 2.86 (1.81–4.50), 5.86 × 10−6, 5.79 × 10−6 | ||
| rs17406146 | 77228667 | G/A | 0.30/0.14 | 2.84 (1.81–4.46), 5.97 × 10−6, 6.48 × 10−6 | ||
| rs2077823 | 77248912 | G/A | 0.30/0.14 | 2.88 (1.83–4.53), 4.99 × 10−6, 4.49 × 10−6 | ||
| rs62170897 | 77258540 | G/A | 0.30/0.14 | 2.78 (1.77–4.36), 9.01 × 10−6, 6.78 × 10−6 | ||
| PCSK5 (intron variation) | 9q21.13 | rs10521467 | 78651491 | G/A | 0.27/0.12 | 2.94 (1.83–4.75), 8.41 × 10−6, 1.94 × 10−5 |
| Unknown (intergenic region) | 12q24.32 | rs117129097 | 128539282 | T/C | 0.19/0.06 | 4.03 (2.30–7.08), 1.17 × 10−6 1.56 × 10−6 |
| Hypotensive (n = 166)/Non-Hypotensive (n = 2,367) | CI (n = 624)/Non-CI (n = 1,909) | |||||
|---|---|---|---|---|---|---|
| Gene | SNP | A1/A2 | MAF | OR (95% CI), p-Value | MAF | OR (95% CI), p-Value |
| LRRTM4 | rs13388459 | T/C | 0.18/0.14 | 1.32 (0.98–1.77), 0.07 | 0.16/0.14 | 1.22 (1.01–1.48), 0.04 |
| rs1075716 | C/T | 0.18/0.14 | 1.32 (0.98–1.77), 0.07 | 0.16/0.14 | 1.22 (1.00–1.48), 0.05 | |
| rs62171995 | A/G | 0.18/0.14 | 1.32 (0.98–1.77), 0.07 | 0.16/0.14 | 1.23 (1.02–1.49), 0.03 | |
| rs17406146 | G/A | 0.18/0.14 | 1.30 (0.97–1.75), 0.08 | 0.16/0.14 | 1.23 (1.01–1.49), 0.04 | |
| rs2077823 | G/A | 0.18/0.14 | 1.34 (1.00–1.80), 0.05 | 0.17/0.14 | 1.27 (1.05–1.54), 0.02 | |
| rs62170897 | G/A | 0.18/0.14 | 1.29 (0.96–1.73), 0.09 | 0.17/0.14 | 1.27 (1.05–1.54), 0.01 | |
| PCSK5 | rs10521467 | G/A | 0.15/0.12 | 1.35 (0.98–1.86), 0.06 | 0.13/0.12 | 1.05 (0.85–1.30), 0.66 |
| Unknown * | rs117129097 | T/C | 0.11/0.06 | 1.90 (1.33–2.72), 0.0005 | 0.07/0.07 | 1.08 (0.82–1.43), 0.57 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-C.; Liu, Y.-L.; Tsai, S.-J.; Kuo, P.-H.; Huang, S.-S.; Lee, Y.-S. LRRTM4 and PCSK5 Genetic Polymorphisms as Markers for Cognitive Impairment in A Hypotensive Aging Population: A Genome-Wide Association Study in Taiwan. J. Clin. Med. 2019, 8, 1124. https://doi.org/10.3390/jcm8081124
Chen Y-C, Liu Y-L, Tsai S-J, Kuo P-H, Huang S-S, Lee Y-S. LRRTM4 and PCSK5 Genetic Polymorphisms as Markers for Cognitive Impairment in A Hypotensive Aging Population: A Genome-Wide Association Study in Taiwan. Journal of Clinical Medicine. 2019; 8(8):1124. https://doi.org/10.3390/jcm8081124
Chicago/Turabian StyleChen, Yi-Chun, Yu-Li Liu, Shih-Jen Tsai, Po-Hsiu Kuo, Shih-Sin Huang, and Yun-Shien Lee. 2019. "LRRTM4 and PCSK5 Genetic Polymorphisms as Markers for Cognitive Impairment in A Hypotensive Aging Population: A Genome-Wide Association Study in Taiwan" Journal of Clinical Medicine 8, no. 8: 1124. https://doi.org/10.3390/jcm8081124