Procedural Sedation Using a Propofol–Ketamine Combination (Ketofol) vs. Propofol Alone in the Loop Electrosurgical Excision Procedure (LEEP): A Randomized Controlled Trial

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
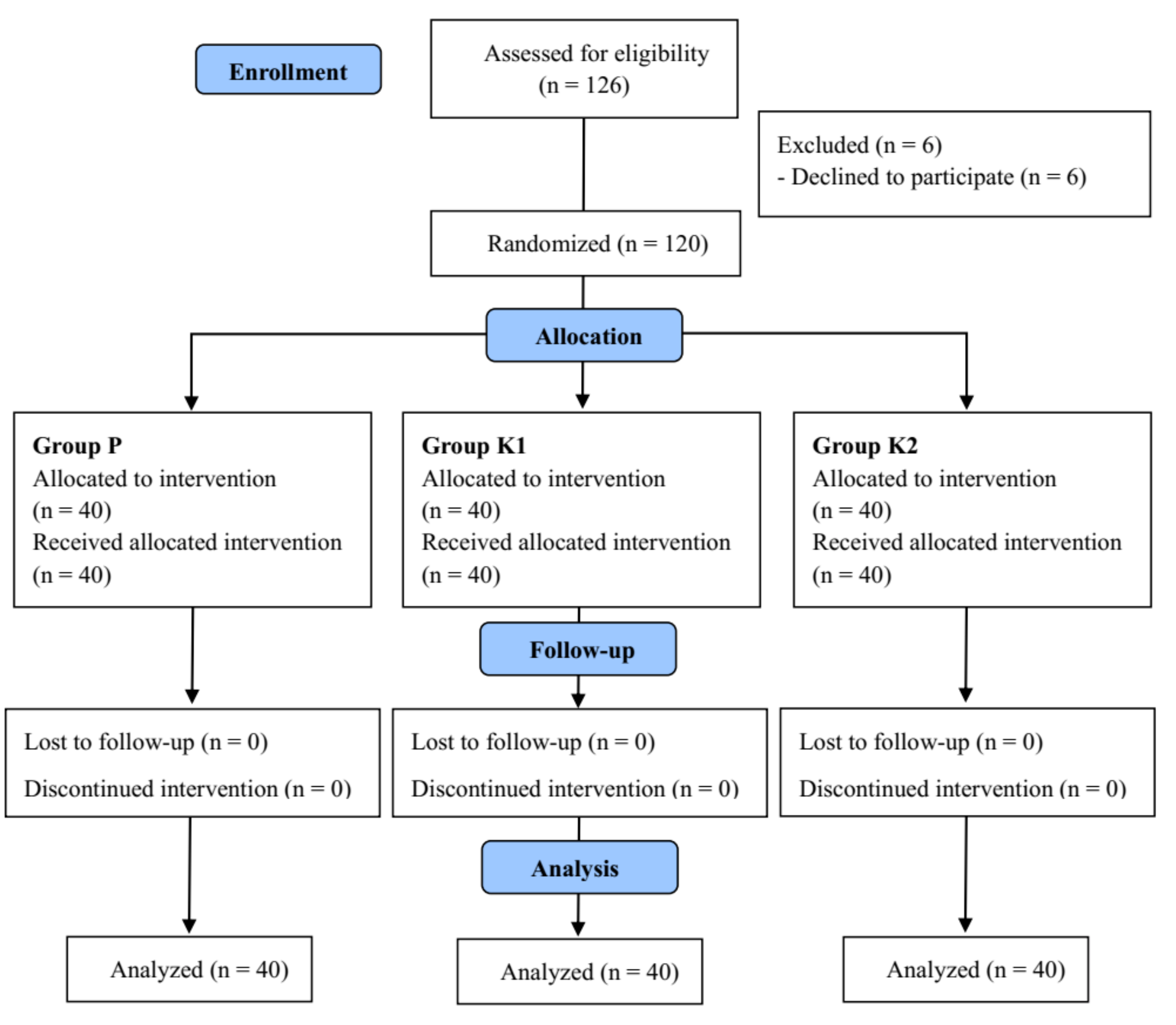
2.1. Study Design and Participants
2.2. Randomization and Minimization of Bias
2.3. Anesthetic Procedures
2.4. Outcome Assessments
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dobson, G.; Chong, M.A.; Chow, L.; Flexman, A.; Hurdle, H.; Kurrek, M.; Laflamme, C.; Perrault, M.-A.; Sparrow, K.; Stacey, S.; et al. Procedural sedation: A position paper of the Canadian Anesthesiologists’ Society. Can. J. Anesth. 2018, 65, 1372–1384. [Google Scholar] [CrossRef]
- Alletag, M.J.; Auerbach, M.A.; Baum, C.R. Ketamine, propofol, and ketofol use for pediatric sedation. Pediatr. Emerg. Care 2012, 28, 1391–1395. [Google Scholar] [CrossRef] [PubMed]
- Strayer, R.J.; Nelson, L.S. Adverse events associated with ketamine for procedural sedation in adults. Am. J. Emerg. Med. 2008, 26, 985–1028. [Google Scholar] [CrossRef] [PubMed]
- White, P.F.; Way, W.L.; Trevor, A.J. Ketamine—Its pharmacology and therapeutic uses. Anesthesiology 1982, 56, 119–136. [Google Scholar] [CrossRef] [PubMed]
- Akin, A.; Esmaoglu, A.; Guler, G.; Demircioglu, R.; Narin, N.; Boyaci, A. Propofol and propofol-ketamine in pediatric patients undergoing cardiac catheterization. Pediatr. Cardiol. 2005, 26, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Aouad, M.T.; Moussa, A.R.; Dagher, C.M.; Muwakkit, S.A.; Jabbour-Khoury, S.I.; Zbeidy, R.A.; Abboud, M.R.; Kanazi, G.E. Addition of ketamine to propofol for initiation of procedural anesthesia in children reduces propofol consumption and preserves hemodynamic stability. Acta Anaesthesiol. Scand. 2008, 52, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Arora, S. Combining ketamine and propofol (“ketofol”) for emergency department procedural sedation and analgesia: A review. West J. Emerg. Med. 2008, 9, 20–23. [Google Scholar] [PubMed]
- Jalili, M.; Bahreini, M.; Doosti-Irani, A.; Masoomi, R.; Arbab, M.; Mirfazaelian, H. Ketamine-propofol combination (ketofol) vs. propofol for procedural sedation and analgesia: Systematic review and meta-analysis. Am. J. Emerg. Med. 2016, 34, 558–569. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.A.; Prakash, K.; Sharma, S.; Dhakate, G.; Bhatia, V. Comparison of propofol alone and in combination with ketamine or fentanyl for sedation in endoscopic ultrasonography. Korean J. Anesth. 2018, 71, 43–47. [Google Scholar] [CrossRef] [Green Version]
- Smischney, N.J.; Beach, M.L.; Loftus, R.W.; Dodds, T.M.; Koff, M.D. Ketamine/propofol admixture (ketofol) is associated with improved hemodynamics as an induction agent: A randomized, controlled trial. J. Trauma Acute Care Surg. 2012, 73, 94–101. [Google Scholar] [CrossRef]
- Yan, J.W.; McLeod, S.L.; Iansavitchene, A. Ketamine-Propofol Versus Propofol Alone for Procedural Sedation in the Emergency Department: A Systematic Review and Meta-analysis. Acad. Emerg. Med. 2015, 22, 1003–1013. [Google Scholar] [CrossRef] [PubMed]
- Ghojazadeh, M.; Sanaie, S.; Paknezhad, S.P.; Faghih, S.S.; Soleimanpour, H. Using Ketamine and Propofol for Procedural Sedation of Adults in the Emergency Department: A Systematic Review and Meta-Analysis. Adv. Pharm. Bull. 2019, 9, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Nazemroaya, B.; Majedi, M.A.; Shetabi, H.; Salmani, S. Comparison of Propofol and Ketamine Combination (Ketofol) and Propofol and Fentanyl Combination (Fenofol) on Quality of Sedation and Analgesia in the Lumpectomy: A Randomized Clinical Trial. Adv. Biomed. Res. 2018, 7, 134. [Google Scholar] [CrossRef] [PubMed]
- Limwatanapan, N.; Chalapati, W.; Songthamwat, S.; Saenpoch, S.; Buapaichit, K.; Songthamwat, M. Lidocaine Spray Versus Paracervical Block During Loop Electrosurgical Excision Procedure: A Randomized Trial. J. Low. Genit. Tract Dis. 2018, 22, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Vanichtantikul, A.; Charoenkwan, K. Lidocaine spray compared with submucosal injection for reducing pain during loop electrosurgical excision procedure: A randomized controlled trial. Obstet. Gynecol. 2013, 122, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Lowles, I.E.; Al-Kurdi, M.; Hare, M.J. Women’s recollection of pain during and after carbon dioxide laser treatment to the uterine cervix. Br. J. Obs. Gynaecol. 1983, 90, 1157–1159. [Google Scholar] [CrossRef]
- Gajjar, K.; Martin-Hirsch, P.P.; Bryant, A.; Owens, G.L. Pain relief for women with cervical intraepithelial neoplasia undergoing colposcopy treatment. Cochrane Database Syst. Rev. 2016, 7, Cd006120. [Google Scholar] [CrossRef] [PubMed]
- Frey, K.; Sukhani, R.; Pawlowski, J.; Pappas, A.L.; Mikat-Stevens, M.; Slogoff, S. Propofol versus propofol-ketamine sedation for retrobulbar nerve block: Comparison of sedation quality, intraocular pressure changes, and recovery profiles. Anesth. Analg. 1999, 89, 317–321. [Google Scholar]
- Badrinath, S.; Avramov, M.N.; Shadrick, M.; Witt, T.R.; Ivankovich, A.D. The use of a ketamine-propofol combination during monitored anesthesia care. Anesth. Analg. 2000, 90, 858–862. [Google Scholar] [CrossRef]
- Abdellatif, A.A. Ketofol for outpatient transrectal ultrasound guided prostate biopsy. Ain Shams J. Anesth. 2012, 5, 11–22. [Google Scholar]
- Andolfatto, G.; Abu-Laban, R.B.; Zed, P.J.; Staniforth, S.M.; Stackhouse, S.; Moadebi, S.; Willman, E. Ketamine-propofol combination (ketofol) versus propofol alone for emergency department procedural sedation and analgesia: A randomized double-blind trial. Ann. Emerg. Med. 2012, 59, 504.e2–512.e2. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, I.; Bell, A.; Treston, G.; New, L.; Ding, M.; Holdgate, A. Propofol or Ketofol for Procedural Sedation and Analgesia in Emergency Medicine-The POKER Study: A Randomized Double-Blind Clinical Trial. Ann. Emerg. Med. 2016, 68, 574–582. [Google Scholar] [CrossRef] [PubMed]
- David, H.; Shipp, J. A randomized controlled trial of ketamine/propofol versus propofol alone for emergency department procedural sedation. Ann. Emerg. Med. 2011, 57, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Miner, J.R.; Moore, J.C.; Austad, E.J.; Plummer, D.; Hubbard, L.; Gray, R.O. Randomized, double-blinded, clinical trial of propofol, 1:1 propofol/ketamine, and 4:1 propofol/ketamine for deep procedural sedation in the emergency department. Ann. Emerg. Med. 2015, 65, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Green, S.M.; Andolfatto, G.; Krauss, B. Ketofol for procedural sedation? Pro and con. Ann. Emerg. Med. 2011, 57, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Green, S.M.; Roback, M.G.; Kennedy, R.M.; Krauss, B. Clinical practice guideline for emergency department ketamine dissociative sedation: 2011 update. Ann. Emerg Med. 2011, 57, 449–461. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group P | Group K1 | Group K2 | ||
|---|---|---|---|---|
| (n = 40) | (n = 40) | (n = 40) | p | |
| ASA 1/2 | 12/28 | 10/30 | 9/31 | 0.738 |
| Age (years) | 44.0 [36.0; 50.5] | 48.5 [36.0; 54.5] | 38.0 [34.5; 56.0] | 0.620 |
| Height (cm) | 159.1 ± 5.3 | 157.3 ± 5.8 | 159.2 ± 7.0 | 0.964 |
| Weight (kg) | 58.0 [54.9; 68.2] | 58.2 [55.7; 64.0] | 58.6 [53.6; 66.3] | 0.695 |
| BMI (kg/m2) | 24.6 [21.4; 26.4] | 23.8 [21.4; 25.5] | 23.2 [20.6; 25.8] | 0.515 |
| Cervical cytology | 0.782 | |||
| ASC-US | 1 (2.5) | 3 (7.5) | 1 (2.5) | |
| LSIL | 3 (7.5) | 1 (2.5) | 2 (5.0) | |
| ASC-H | 10 (25.0) | 6 (15.0) | 4 (10.0) | |
| HSIL AIS | 24 (60.0) 0 (0.0) | 26 (65.0) 1 (2.5) | 28 (70.0) 0 (0.0) | |
| SCC | 1 (2.5) | 1 (2.5) | 1 (2.5) | |
| Adenocarcinoma | 0 (0.0) | 0 (0.0) | 1 (2.5) | |
| Unknown | 1 (2.5) | 2 (5.0) | 3 (7.5) | |
| Final histology | 0.810 | |||
| Normal or cervicitis | 1 (2.5) | 2 (5.0) | 0 (0.0) | |
| CIN 1 | 4 (10.0) | 3 (7.5) | 2 (5.0) | |
| CIN 2 | 11 (27.5) | 10 (25.0) | 14 (35.0) | |
| CIN 3 | 19 (47.5) | 18 (45.0) | 19 (47.5) | |
| CIS AIS | 1 (2.5) 0 (0.0) | 0 (0.0) 2 (5.0) | 1 (2.5) 0 (0.0) | |
| ASC-US | 3 (7.5) | 2 (5.0) | 1 (2.5) | |
| ASC-H | 0 (0.0) | 1 (2.5) | 0 (0.0) | |
| Adenocarcinoma | 0 (0.0) | 0 (0.0) | 2 (5.0) | |
| SCC | 1 (2.5) | 2 (5.0) | 1 (2.5) |
| Group P | Group K1 | Group K2 | p | P vs. K1 | P vs. K2 | K1 vs. K2 | |
|---|---|---|---|---|---|---|---|
| Outcome | RR (95% CI) | RR (95% CI) | RR (95% CI) | ||||
| p | p | p | |||||
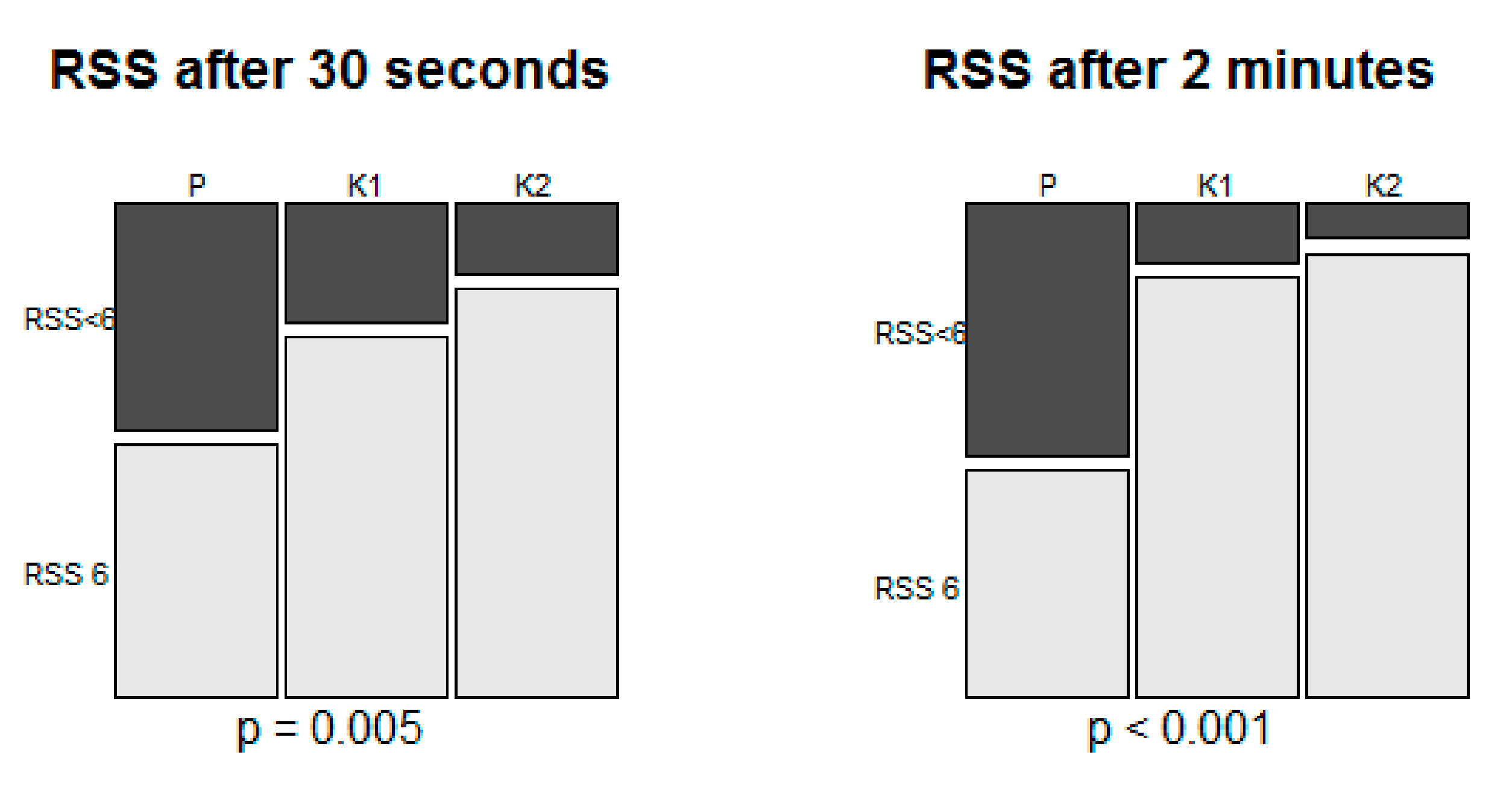
| Adduction | 27 (67.5%) | 13 (32.5%) | 4 (10%) | <0.001 | 2.08 (1.27 ~ 3.41) | 6.75 (2.60 ~ 17.53) | 3.25 (1.16 ~ 9.12) |
| No movement | 13 (32.5%) | 27 (67.5%) | 36 (90.0%) | 0.004 | < 0.001 | 0.029 |
| Outcome | Group P | Group K1 | Group K2 | p | P vs. K1 | P vs. K2 | K1 vs. K2 |
|---|---|---|---|---|---|---|---|
| p | p | p | |||||
| Jaw thrust maneuver | 8 (20.0) | 4 (10.0) | 17 (42.5) | 0.002 | 0.348 | 0.054 | 0.002 |
| Bag-mask ventilation | 6 (15.0) | 2 (5.0) | 2 (5.0) | 0.215 | |||
| Additional propofol | 39 (97.5) | 23 (57.5) | 12 (30.0) | < 0.001 | < 0.001 | < 0.001 | 0.024 |
| 1 | 7 (17.5) | 10 (25.0) | 4 (10.0) | ||||
| 2 | 32 (80.0) | 13 (32.5) | 8 (20.0) | ||||
| Sevoflurane inhalation | 6 (15.0) | 2 (5.0) | 1 (2.5) | 0.144 | |||
| Pain recall | 3 (7.5) | 3 (7.5) | 0 (0.0) | 0.244 | |||
| Recovery agitation | 3 (7.5) | 2 (5.0) | 0 (0.0) | 0.368 | |||
| Patient’s satisfaction | 5 [4.5; 5.0] | 5 [4.0; 5.0] | 5 [5.5; 5.0] | 0.322 | |||
| Surgeon’s satisfaction | 3 [2.0; 4.5] | 4 [4.0; 5.0] | 5 [4.0; 5.0] | < 0.001 | 0.001 | < 0.001 | 0.403 |
| Procedure duration (sec) | 495 [395.0; 595.0] | 440 [384.0;519.0] | 422 [390.0;485.0] | 0.196 | |||
| PACU stay time (min) | 30.3 ± 12.9 | 28.6 ± 11.7 | 27.8 ± 11.8 | 0.357 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, C.; Kim, Y.; Eom, H.; Youn, S.; Lee, S.; Ko, Y.-B.; Yoo, H.J.; Chung, W.; Lim, C.; Hong, B. Procedural Sedation Using a Propofol–Ketamine Combination (Ketofol) vs. Propofol Alone in the Loop Electrosurgical Excision Procedure (LEEP): A Randomized Controlled Trial. J. Clin. Med. 2019, 8, 943. https://doi.org/10.3390/jcm8070943
Oh C, Kim Y, Eom H, Youn S, Lee S, Ko Y-B, Yoo HJ, Chung W, Lim C, Hong B. Procedural Sedation Using a Propofol–Ketamine Combination (Ketofol) vs. Propofol Alone in the Loop Electrosurgical Excision Procedure (LEEP): A Randomized Controlled Trial. Journal of Clinical Medicine. 2019; 8(7):943. https://doi.org/10.3390/jcm8070943
Chicago/Turabian StyleOh, Chahyun, Yeojung Kim, Hongsik Eom, Sookyoung Youn, Sangmin Lee, Young-Bok Ko, Heon Jong Yoo, Woosuk Chung, ChaeSeong Lim, and Boohwi Hong. 2019. "Procedural Sedation Using a Propofol–Ketamine Combination (Ketofol) vs. Propofol Alone in the Loop Electrosurgical Excision Procedure (LEEP): A Randomized Controlled Trial" Journal of Clinical Medicine 8, no. 7: 943. https://doi.org/10.3390/jcm8070943