Influence of Fixation Methods on Prosthetic Joint Infection Following Primary Total Knee Replacement: Meta-Analysis of Observational Cohort and Randomised Intervention Studies

 , and
, and
Abstract
:1. Introduction
2. Experimental Section
2.1. Data sources and Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis
3. Results
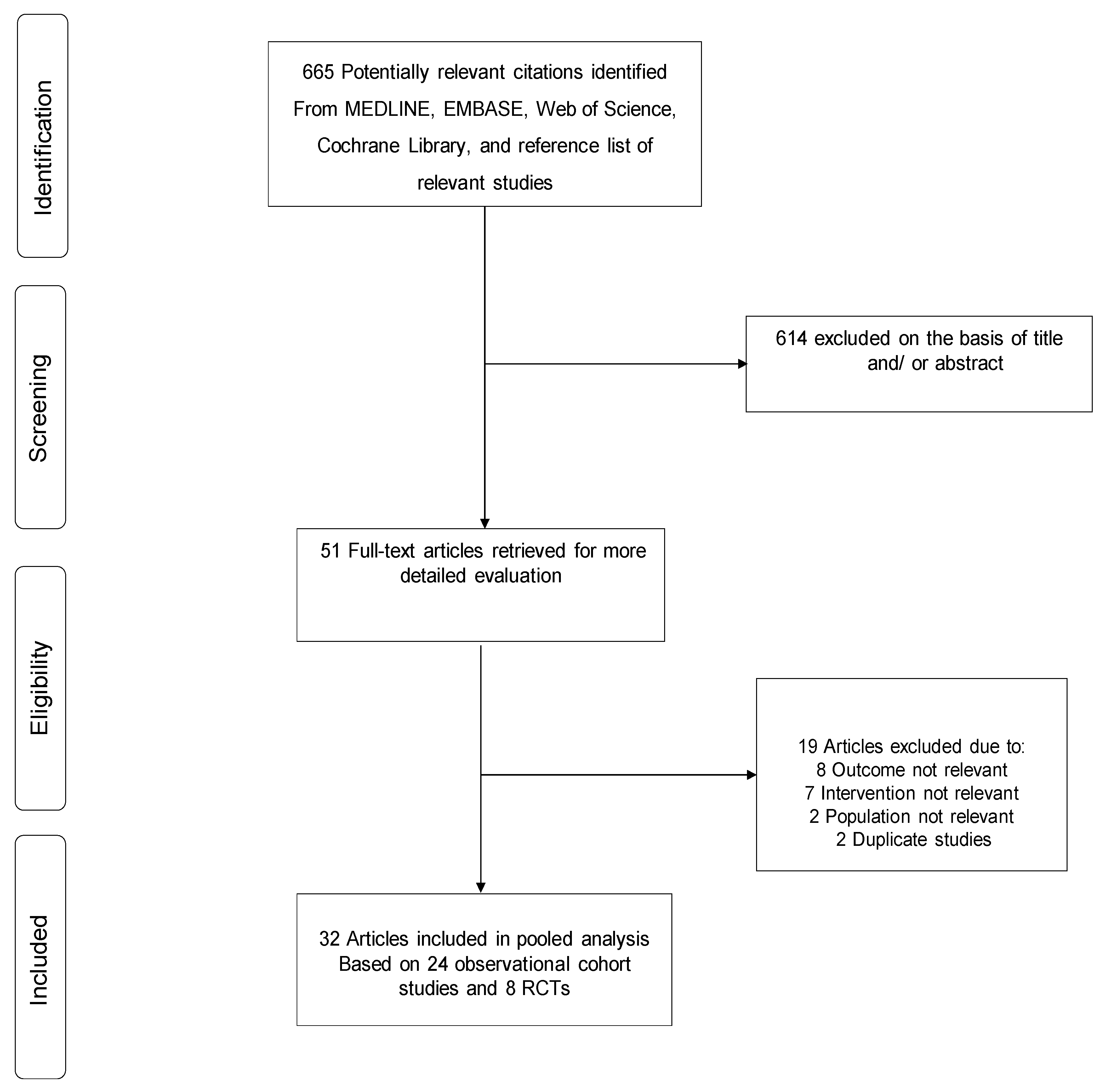
3.1. Study Identification and Selection
3.2. Study Characteristics and Study Quality
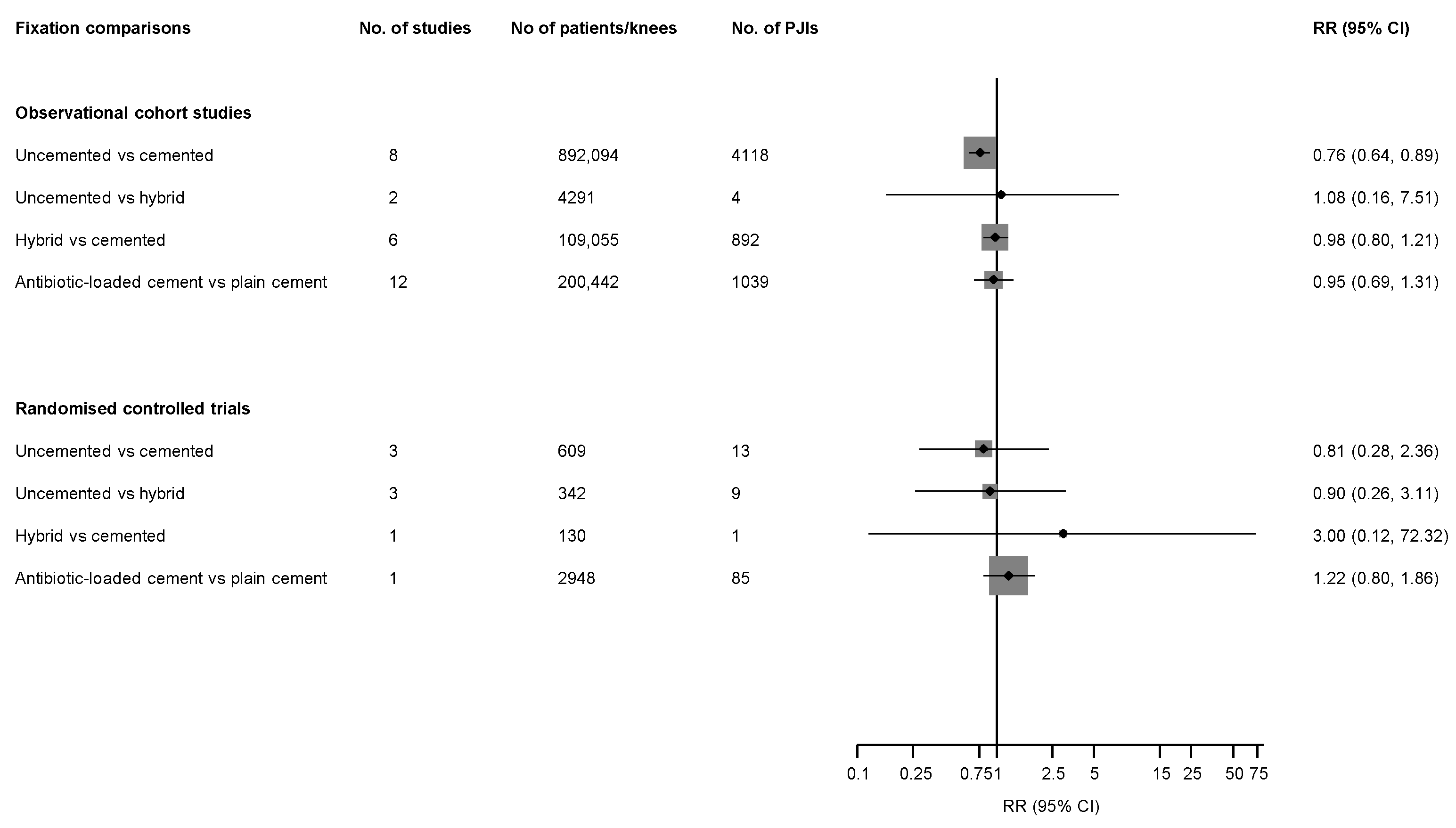
3.3. Fixation Types and PJI Risk
3.4. Publication Bias
4. Discussion
4.1. Key Findings
4.2. Comparison with Previous Work
4.3. Possible Explanations for Findings
4.4. Implications of our Findings
4.5. Study Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- NJR Steering Commitee. National Joint Registry for England, Wales, Northern Ireland and the Isle of Man: 15th Annual Report, 2017; National Joint Registry Centre: Hemel Hempstead, UK, 2018. [Google Scholar]
- Lenguerrand, E.; Wylde, V.; Gooberman-Hill, R.; Sayers, A.; Brunton, L.; Beswick, A.D.; Dieppe, P.; Blom, A.W. Trajectories of Pain and Function after Primary Hip and Knee Arthroplasty: The ADAPT Cohort Study. PLoS ONE 2016, 11, e0149306. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, E.M.; Parvizi, J.; Gehrke, T.; Aiyer, A.; Battenberg, A.; Brown, S.A.; Callaghan, J.J.; Citak, M.; Egol, K.; Garrigues, G.E.; et al. 2018 International Consensus Meeting on Musculoskeletal Infection: Research Priorities from the General Assembly Questions. J. Orthop. Res. 2019, 37, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Mallon, C.M.; Gooberman-Hill, R.; Moore, A.J. Infection after knee replacement: A qualitative study of impact of periprosthetic knee infection. BMC Musculoskelet. Disord. 2018, 19, 352. [Google Scholar] [CrossRef]
- Cahill, J.L.; Shadbolt, B.; Scarvell, J.M.; Smith, P.N. Quality of life after infection in total joint replacement. J. Orthop. Surg. 2008, 16, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Andersson, A.E.; Bergh, I.; Karlsson, J.; Nilsson, K. Patients’ experiences of acquiring a deep surgical site infection: An interview study. Am. J. Infect. Control 2010, 38, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.J.; Blom, A.W.; Whitehouse, M.R.; Gooberman-Hill, R. Deep prosthetic joint infection: A qualitative study of the impact on patients and their experiences of revision surgery. BMJ Open 2015, 5, e009495. [Google Scholar] [CrossRef] [PubMed]
- Bozic, K.J.; Katz, P.; Cisternas, M.; Ono, L.; Ries, M.D.; Showstack, J. Hospital resource utilization for primary and revision total hip arthroplasty. J. Bone Jt. Surg. Am. Vol. 2005, 87, 570–576. [Google Scholar] [CrossRef] [PubMed]
- Ong, K.L.; Mowat, F.S.; Chan, N.; Lau, E.; Halpern, M.T.; Kurtz, S.M. Economic burden of revision hip and knee arthroplasty in Medicare enrollees. Clin. Orthop. Relat. Res. 2006, 446, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.M.; Lau, E.; Ong, K.; Zhao, K.; Kelly, M.; Bozic, K.J. Future young patient demand for primary and revision joint replacement: National projections from 2010 to 2030. Clin. Orthop. Relat. Res. 2009, 467, 2606–2612. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Jt. Surg. Am. 2007, 89-A, 780–785. [Google Scholar] [CrossRef]
- Lenguerrand, E.; Whitehouse, M.R.; Beswick, A.D.; Toms, A.D.; Porter, M.L.; Blom, A.W.; National Joint Registry for England, Wales, Northern Ireland and the Isle of Man. Description of the rates, trends and surgical burden associated with revision for prosthetic joint infection following primary and revision knee replacements in England and Wales: An analysis of the National Joint Registry for England, Wales, Northern Ireland and the Isle of Man. BMJ Open 2017, 7, e014056. [Google Scholar] [CrossRef] [PubMed]
- Kunutsor, S.K.; Whitehouse, M.R.; Blom, A.W.; Beswick, A.D.; INFORM Team. Patient-related risk factors for periprosthetic joint infection after total joint arthroplasty: A systematic review and meta-analysis. PLoS ONE 2016, 11, e0150866. [Google Scholar] [CrossRef] [PubMed]
- Lenguerrand, E.; Whitehouse, M.R.; Beswick, A.D.; Kunutsor, S.K.; Foguet, P.; Porter, M.; Blom, A.W. Risk factors associated with revision for prosthetic joint infection (PJI) following knee replacement: An observational cohort study from the National Joint Registry for England, Wales, Northern Ireland and the Isle of Man. Lancet Infect. Dis. 2019, 19, 589–600. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Beswick, A.D.; Whitehouse, M.R.; Blom, A.W.; Lenguerrand, E. Implant fixation and risk of prosthetic joint infection following primary total hip replacement: Meta-analysis of observational cohort and randomised intervention studies. J. Clin. Med. 2019, 8, 722. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B.; et al. Meta-analysis of Observational Studies in Epidemiology. JAMA J. Am. Med Assoc. 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 20 August 2018).
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Cornfield, J. A method of estimating comparative rates from clinical data; applications to cancer of the lung, breast, and cervix. J. Natl. Cancer Inst. 1951, 11, 1269–1275. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Thompson, S.G.; Sharp, S.J. Explaining heterogeneity in meta-analysis: A comparison of methods. Stat. Med. 1999, 18, 2693–2708. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Horan, T.C.; Andrus, M.; Dudeck, M.A. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am. J. Infect. Control 2008, 36, 309–332. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Zmistowski, B.; Berbari, E.F.; Bauer, T.W.; Springer, B.D.; Della Valle, C.J.; Garvin, K.L.; Mont, M.A.; Wongworawat, M.D.; Zalavras, C.G. New definition for periprosthetic joint infection: From the Workgroup of the Musculoskeletal Infection Society. Clin. Orthop. 2011, 469, 2992–2994. [Google Scholar] [CrossRef] [PubMed]
- Schrama, J.C.; Fenstad, A.M.; Dale, H.; Havelin, L.; Hallan, G.; Overgaard, S.; Pedersen, A.B.; Karrholm, J.; Garellick, G.; Pulkkinen, P.; et al. Increased risk of revision for infection in rheumatoid arthritis patients with total hip replacements. Acta Orthop. 2015, 86, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Qadir, R.; Sidhu, S.; Ochsner, J.L.; Meyer, M.S.; Chimento, G.F. Risk stratified usage of antibiotic-loaded bone cement for primary total knee arthroplasty: Short term infection outcomes with a standardized cement protocol. J. Arthroplast. 2014, 29, 1622–1624. [Google Scholar] [CrossRef] [PubMed]
- Gutowski, C.J.; Zmistowski, B.M.; Clyde, C.T.; Parvizi, J. The economics of using prophylactic antibiotic-loaded bone cement in total knee replacement. Bone Jt. J. 2014, 96-B, 65–69. [Google Scholar] [CrossRef]
- Tayton, E.R.; Frampton, C.; Hooper, G.J.; Young, S.W. The impact of patient and surgical factors on the rate of infection after primary total knee arthroplasty: An analysis of 64,566 joints from the New Zealand Joint Registry. Bone Jt. J. 2016, 98-B, 334–340. [Google Scholar] [CrossRef]
- Hinarejos, P.; Guirro, P.; Leal, J.; Montserrat, F.; Pelfort, X.; Sorli, M.L.; Horcajada, J.P.; Puig, L. The use of erythromycin and colistin-loaded cement in total knee arthroplasty does not reduce the incidence of infection: A prospective randomized study in 3000 knees. J. Bone Jt. Surg. Am. Vol. 2013, 95, 769–774. [Google Scholar] [CrossRef]
- Gandhi, R.; Tsvetkov, D.; Davey, J.R.; Mahomed, N.N. Survival and clinical function of cemented and uncemented prostheses in total knee replacement: A meta-analysis. J. Bone Jt. Surg. Br. 2009, 91, 889–895. [Google Scholar] [CrossRef]
- Mont, M.A.; Pivec, R.; Issa, K.; Kapadia, B.H.; Maheshwari, A.; Harwin, S.F. Long-term implant survivorship of cementless total knee arthroplasty: A systematic review of the literature and meta-analysis. J. Knee Surg. 2014, 27, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Lou, H.; Zhang, H.; Jiang, J.; Liu, K. Similar survival between uncemented and cemented fixation prostheses in total knee arthroplasty: A meta-analysis and systematic comparative analysis using registers. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 3191–3197. [Google Scholar] [CrossRef] [PubMed]
- Schiavone Panni, A.; Corona, K.; Giulianelli, M.; Mazzitelli, G.; Del Regno, C.; Vasso, M. Antibiotic-loaded bone cement reduces risk of infections in primary total knee arthroplasty? A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3168–3174. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhu, C.; Cheng, T.; Peng, X.; Zhang, W.; Qin, H.; Zhang, X. A systematic review and meta-analysis of antibiotic-impregnated bone cement use in primary total hip or knee arthroplasty. PLoS ONE 2013, 8, e82745. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Li, L.; Zhou, Q.; Yuan, S.; Wu, Y.; Zhao, H.; Wu, H. Lack of efficacy of prophylactic application of antibiotic-loaded bone cement for prevention of infection in primary total knee arthroplasty: Results of a meta-analysis. Surg. Infect. (Larchmt.) 2015, 16, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Whitehouse, M.R.; Atwal, N.S.; Pabbruwe, M.; Blom, A.W.; Bannister, G.C. Osteonecrosis with the use of polymethylmethacrylate cement for hip replacement: Thermal-induced damage evidenced in vivo by decreased osteocyte viability. Eur. Cells Mater. 2014, 27, 50–62, discussion 62–53. [Google Scholar] [CrossRef]
- Van Jonbergen, J.P.; Anderson, P.G.; Faber, F.W. Total hip arthroplasty with Boneloc cement: Unsatisfactory results in 163 hips after 9 to 11 years. HIP Int. 2004, 14, 229–232. [Google Scholar] [CrossRef]
- Mjoberg, B. The theory of early loosening of hip prostheses. Orthopedics 1997, 20, 1169–1175. [Google Scholar]
- Aprato, A.; Risitano, S.; Sabatini, L.; Giachino, M.; Agati, G.; Masse, A. Cementless total knee arthroplasty. Ann. Transl. Med. 2016, 4, 129. [Google Scholar] [CrossRef]
- Engesaeter, L.B.; Espehaug, B.; Lie, S.A.; Furnes, O.; Havelin, L.I. Does cement increase the risk of infection in primary total hip arthroplasty? Revision rates in 56,275 cemented and uncemented primary THAs followed for 0–16 years in the Norwegian Arthroplasty Register. Acta Orthop. 2006, 77, 351–358. [Google Scholar] [CrossRef]
- Ueng, S.W.; Hsieh, P.H.; Shih, H.N.; Chan, Y.S.; Lee, M.S.; Chang, Y. Antibacterial activity of joint fluid in cemented total-knee arthroplasty: An in vivo comparative study of polymethylmethacrylate with and without antibiotic loading. Antimicrob. Agents Chemother. 2012, 56, 5541–5546. [Google Scholar] [CrossRef] [PubMed]
- van de Belt, H.; Neut, D.; Schenk, W.; van Horn, J.R.; van der Mei, H.C.; Busscher, H.J. Gentamicin release from polymethylmethacrylate bone cements and Staphylococcus aureus biofilm formation. Acta Orthop. Scand. 2000, 71, 625–629. [Google Scholar] [CrossRef] [PubMed]
- Kendall, R.W.; Duncan, C.P.; Smith, J.A.; Ngui-Yen, J.H. Persistence of bacteria on antibiotic loaded acrylic depots. A reason for caution. Clin. Orthop. Relat. Res. 1996, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Hope, P.G.; Kristinsson, K.G.; Norman, P.; Elson, R.A. Deep infection of cemented total hip arthroplasties caused by coagulase-negative staphylococci. J. Bone Jt. Surg. Am. 1989, 71-B, 851–855. [Google Scholar] [CrossRef] [Green Version]
- Thomes, B.; Murray, P.; Bouchier-Hayes, D. Development of resistant strains of Staphylococcus epidermidis on gentamicin-loaded bone cement in vivo. J. Bone Jt. Surg. Br. 2002, 84, 758–760. [Google Scholar] [Green Version]
- Berger, R.A.; Lyon, J.H.; Jacobs, J.J.; Barden, R.M.; Berkson, E.M.; Sheinkop, M.B.; Rosenberg, A.G.; Galante, J.O. Problems with cementless total knee arthroplasty at 11 years followup. Clin. Orthop. Relat. Res. 2001, 196–207. [Google Scholar] [CrossRef] [PubMed]
- Cadambi, A.; Engh, G.A.; Dwyer, K.A.; Vinh, T.N. Osteolysis of the distal femur after total knee arthroplasty. J. Arthroplast. 1994, 9, 579–594. [Google Scholar] [CrossRef]
- Brown, T.E.; Harper, B.L.; Bjorgul, K. Comparison of cemented and uncemented fixation in total knee arthroplasty. Orthopedics 2013, 36, 380–387. [Google Scholar] [CrossRef]
- Matassi, F.; Carulli, C.; Civinini, R.; Innocenti, M. Cemented versus cementless fixation in total knee arthroplasty. Joints 2013, 1, 121–125. [Google Scholar] [CrossRef] [Green Version]
- Leskinen, J.; Eskelinen, A.; Huhtala, H.; Paavolainen, P.; Remes, V. The incidence of knee arthroplasty for primary osteoarthritis grows rapidly among baby boomers: A population-based study in Finland. Arthritis Rheumatol. 2012, 64, 423–428. [Google Scholar] [CrossRef]
- Wang, H.; Qiu, G.X.; Lin, J.; Jin, J.; Qian, W.W.; Weng, X.S. Antibiotic Bone Cement Cannot Reduce Deep Infection After Primary Total Knee Arthroplasty. Orthopedics 2015, 38, e462–e466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bistolfi, A.; Massazza, G.; Verne, E.; Masse, A.; Deledda, D.; Ferraris, S.; Miola, M.; Galetto, F.; Crova, M. Antibiotic-loaded cement in orthopedic surgery: A review. ISRN Orthop. 2011, 2011, 290851. [Google Scholar] [CrossRef] [PubMed]
- Namba, R.S.; Chen, Y.; Paxton, E.W.; Slipchenko, T.; Fithian, D.C. Outcomes of routine use of antibiotic-loaded cement in primary total knee arthroplasty. J. Arthroplast. 2009, 24, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Hinarejos, P.; Guirro, P.; Puig-Verdie, L.; Torres-Claramunt, R.; Leal-Blanquet, J.; Sanchez-Soler, J.; Monllau, J.C. Use of antibiotic-loaded cement in total knee arthroplasty. World J. Orthop. 2015, 6, 877–885. [Google Scholar] [CrossRef] [PubMed]
- Gundtoft, P.H.; Overgaard, S.; Schonheyder, H.C.; Moller, J.K.; Kjaersgaard-Andersen, P.; Pedersen, A.B. The “true” incidence of surgically treated deep prosthetic joint infection after 32,896 primary total hip arthroplasties. Acta Orthop. 2015, 86, 326–334. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author, Year of Publication | Year of Study | Country | Indication for Total Hip Replacement | Average Age (Years) | Design, Source of Data | Fixation Types Compared | Mean/Median Follow-Up Duration, Years | No. of Participants/Knees | Infection Outcome Reported (Definition) | No. of PJIs | Study Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Wilson, 1990 | 1973–1987 | U.S. | NR | NR | Observational cohort, Hospital | Uncemented, cemented, hybrid | Up to 6.0 years | 4171 | Deep infection (Purulent material obtained from joint and positive bacterial culture) | 67 | 4 |
| Duffy, 1998 | 1985–1987 | U.S. | Uncemented (OA 76.4%; RA 16.4%; PTA 5.5%; ankylosing spondylitis 1.8%); Cemented (OA 82.4%; RA 11.8%; ancient sepsis 3.9%; osteonecrosis 2.0%) | 59.6 | Retrospective cohort | Uncemented, cemented | 10.0 | 106 | Revision for infection (NR) | 1 | 4 |
| McCaskie, 1998 | 1987–1990 | U.K. | Cemented (OA 84%); Uncemented (OA 86%) | 68.8–70.2 | RCT, Hospital | Uncemented, cemented | 5.0 | 113 | Infection (NR) | 1 | NA |
| Pecina, 2000 | 1985–1991 | Croatia | OA 68.3%; RA 31.7% | 61.0 | Observational cohort | Uncemented, cemented, hybrid | 7.3 | 142 | Revision for infection (NR) | 5 | 5 |
| Eveillard, 2003 | 1995–1999 | France | NR | NR | Observational cohort, Hospital | Antibiotic loaded cement, plain cement | At least 1 year | 167 | Infection (Isolation of organisms from tissue sample; confirmed by surgeon) | 9 | 5 |
| Baker, 2007 | 1987–1997 | U.K. | OA 91.4%; RA 7.6%; other 1.0% | 70.5 | RCT | Uncemented, cemented | 8.7–8.9 | 396 | Revision for infection (NR) | 11 | NA |
| Beaupre, 2007 | 1996–2000 | Canada | Non-inflammatory arthritis 100% | 63.4 | RCT | Uncemented, hybrid | 5.0 | 81 | Infection (NR) | 6 | NA |
| Jamsen, 2009 | 1997–2004 | Finland | Primary OA 87.9%; secondary OA 2.7%; RA 7.6%; other arthritis 1.0%; other 0.8% | 71.0 | Retrospective cohort, FAR and FHDR | Uncemented, cemented, hybrid | 3.1 | 40,135 | Revision for infection (NR) | 387 | 7 |
| Dowsey, 2009 | 1998–2005 | Australia | OA 91.8%; RA 7.8%; osteonecrosis 0.2%; trauma 0.2% | 72.0 | Retrospective cohort, Institutional database | Antibiotic loaded cement, plain cement | 1.0 | 1214 | PJI (CDC criteria) | 18 | 6 |
| Ghandi, 2009 | 1998–2006 | Canada | Primary or secondary OA; RA | 66.1 | Retrospective cohort, Hospital | Antibiotic loaded cement, plain cement | 1.0 | 1625 | Deep infection (CDC criteria) | 43 | 5 |
| Namba, 2009 | 2003–2007 | U.S. | OA 92.4%; other 7.6% | 68.0 | Retrospective cohort, community-based registry | Antibiotic loaded cement, plain cement | NR | 22,889 | Deep infection (CDC criteria) | 182 | 8 |
| Demey, 2011 | 2004–2005 | France | OA (96.9%); chondrocalcinosis (3.1%) | 72.3 | RCT | Hybrid, cemented | 2.7–2.8 | 130 | Deep infection (NR) | 1 | NA |
| Namba, 2013 | 2001–2009 | U.S. | OA 96.8%; PTA 1.2%; RA 2.2%; osteonecrosis 0.4%; other 0.9% | 67.4 | Retrospective cohort, Registry | Antibiotic loaded cement, plain cement | NR | 56,216 | Deep SSI (CDC criteria) | 404 | 8 |
| Lass, 2013 | 2003–2007 | Austria | Idiopathic arthritis 88.3%; PTA 5.0%; RA 3.3%; avascular necrosis 0.8% | 66.9 | Observational cohort | Uncemented, hybrid | 5.0 | 120 | Revision for infection (NR) | 1 | 5 |
| Pelt, 2013 | NR | U.S. | Hybrid (OA 95%; RA 2%; PTA 3%; other 0%); Cemented (OA 90%; RA 7%; PTA 2%; other 1%) | 59.3–65.9 | Observational cohort | Hybrid, cemented | 3.2–4.1 | 304 | Revision for sepsis (NR) | 5 | 5 |
| Hinarejos, 2013 | 2005–2010 | Spain | NR | 75.9 | RCT | Antibiotic loaded cement, plain cement | 3.2 | 2948 | Deep and superficial infection (CDC criteria) | 85 | NA |
| Qadir, 2014 | 2000–2010 | U.S. | NR | 68.1 | Retrospective cohort, Institutional registry | Antibiotic loaded cement, plain cement | 1.0 | 2511 | Infection (CDC criteria) | 17 | 6 |
| Gutowski, 2014 | 2000–2002; 2004–2007 | U.S. | NR | 65.8 | Retrospective cohort, Hospital | Antibiotic loaded cement, plain cement | Over a 3.0-year period | 7878 | PJI (MSIS criteria) | 63 | 5 |
| Bohm, 2014 | 2003–2008 | Canada | OA 100% | 70.0 | Retrospective cohort, CIHI and CJRR | Antibiotic loaded cement, plain cement | 2.0 | 36,681 | Revision for infection (NR) | 36 | 6 |
| Choy, 2014 | 2002–2004 | Korea | OA 100% | 67.8 | RCT | Uncemented, hybrid | 9.5 | 168 | SSI (NR) | 2 | NA |
| Lizaur-Utrilla, 2014 | 1999–2007 | Spain | OA (92.5%); PTA (7.5%) | 51.7 | RCT | Uncemented, hybrid | 7.1 | 93 | Deep wound infection (NR) | 1 | NA |
| Petursson, 2015 | 1999–2012 | Norway | Primary OA 90%; other 10% | 69.0 | Observational cohort, NAR | Hybrid, cemented | 11.0 | 24,680 | Revision for infection (NR) | 217 | 7 |
| Wang, 2015 | 2003–2012 | China | OA 87.8%; other 12.2% | 64.8 | Retrospective cohort, Hospital | Antibiotic loaded cement, plain cement | 1.0 | 2293 | Deep infection (CDC criteria) | 10 | 6 |
| Fricka, 2015 | 2010–2012 | U.S. | NR | 58.6–60.2 | RCT | Uncemented, cemented | 2.0 | 100 | PJI (NR) | 1 | NA |
| Tayton, 2016 | 1999–2012 | New Zealand | OA 95%; AVN 0.3%; Trauma 1.2%; RA 3.4%; other 0.2% | <55 to >75 * | Prospective cohort, New Zealand Joint Registry | Antibiotic-loaded cement, plain cement | 1.0 | 64,566 | Revision for infection (NR) | 179 | 7 |
| Wu, 2016 | 2009–2013 | Taiwan | OA, RA, PTA | 69.7 | Retrospective cohort | Antibiotic-loaded cement, plain cement | 1.0–5.0 | 3152 | SSI (CDC criteria) | 48 | 6 |
| Prudhon, 2017 | 2003–2006 | France | OA 88.5%; post-traumatic OA 3.0%; RA 4.5%; patellofemoral OA 4.0% | 73.0 | Observational cohort | Uncemented, cemented | 12.1–13.7 | 200 | Infection (NR) | 1 | 5 |
| Sanz-Ruiz, 2017 | 2009–2012 | Spain | NR | 76.1–76.4 | Prospective cohort | Antibiotic-loaded cement, plain cement | 2.0 (minimum) | 1250 | Infection (MSIS criteria) | 30 | 4 |
| Vertullo, 2018 | 1999–2015 | Australia | OA 100% | 69.0 | Observational cohort, Registry | Hybrid, cemented | 13.0 | 39,623 | Revision for infection (NR) | 215 | 7 |
| Gwam, 2018 | 2015 | U.S. | OA 100% | 65.8 | Retrospective cohort, NIS database | Uncemented, cemented | NR | 167,930 | SSI (NR) | NR | 5 |
| Lenguerrand, 2018 | 2003–2013 | U.K. | OA (97.3%); other (2.7%) | 69.0 | Prospective cohort, Registry | Uncemented, cemented | 4.6 | 679,010 | Revision for infection (NR) | 3227 | 7 |
| Miller, 2018 | 2013–2014 | U.S. | NR | 64.4 | Institutional database | Uncemented, cemented | 2.4–5.3 | 400 | Infection (NR) | 1 | 5 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kunutsor, S.K.; Wylde, V.; Whitehouse, M.R.; Beswick, A.D.; Lenguerrand, E.; Blom, A.W. Influence of Fixation Methods on Prosthetic Joint Infection Following Primary Total Knee Replacement: Meta-Analysis of Observational Cohort and Randomised Intervention Studies. J. Clin. Med. 2019, 8, 828. https://doi.org/10.3390/jcm8060828
Kunutsor SK, Wylde V, Whitehouse MR, Beswick AD, Lenguerrand E, Blom AW. Influence of Fixation Methods on Prosthetic Joint Infection Following Primary Total Knee Replacement: Meta-Analysis of Observational Cohort and Randomised Intervention Studies. Journal of Clinical Medicine. 2019; 8(6):828. https://doi.org/10.3390/jcm8060828
Chicago/Turabian StyleKunutsor, Setor K., Vikki Wylde, Michael R. Whitehouse, Andrew D. Beswick, Erik Lenguerrand, and Ashley W. Blom. 2019. "Influence of Fixation Methods on Prosthetic Joint Infection Following Primary Total Knee Replacement: Meta-Analysis of Observational Cohort and Randomised Intervention Studies" Journal of Clinical Medicine 8, no. 6: 828. https://doi.org/10.3390/jcm8060828