Relevance of Targeting the Distal Renal Artery and Branches with Radiofrequency Renal Denervation Approaches—A Secondary Analysis from a Hypertensive CKD Patient Cohort

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Participants
2.2. Study Procedures and Assessment
2.3. Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
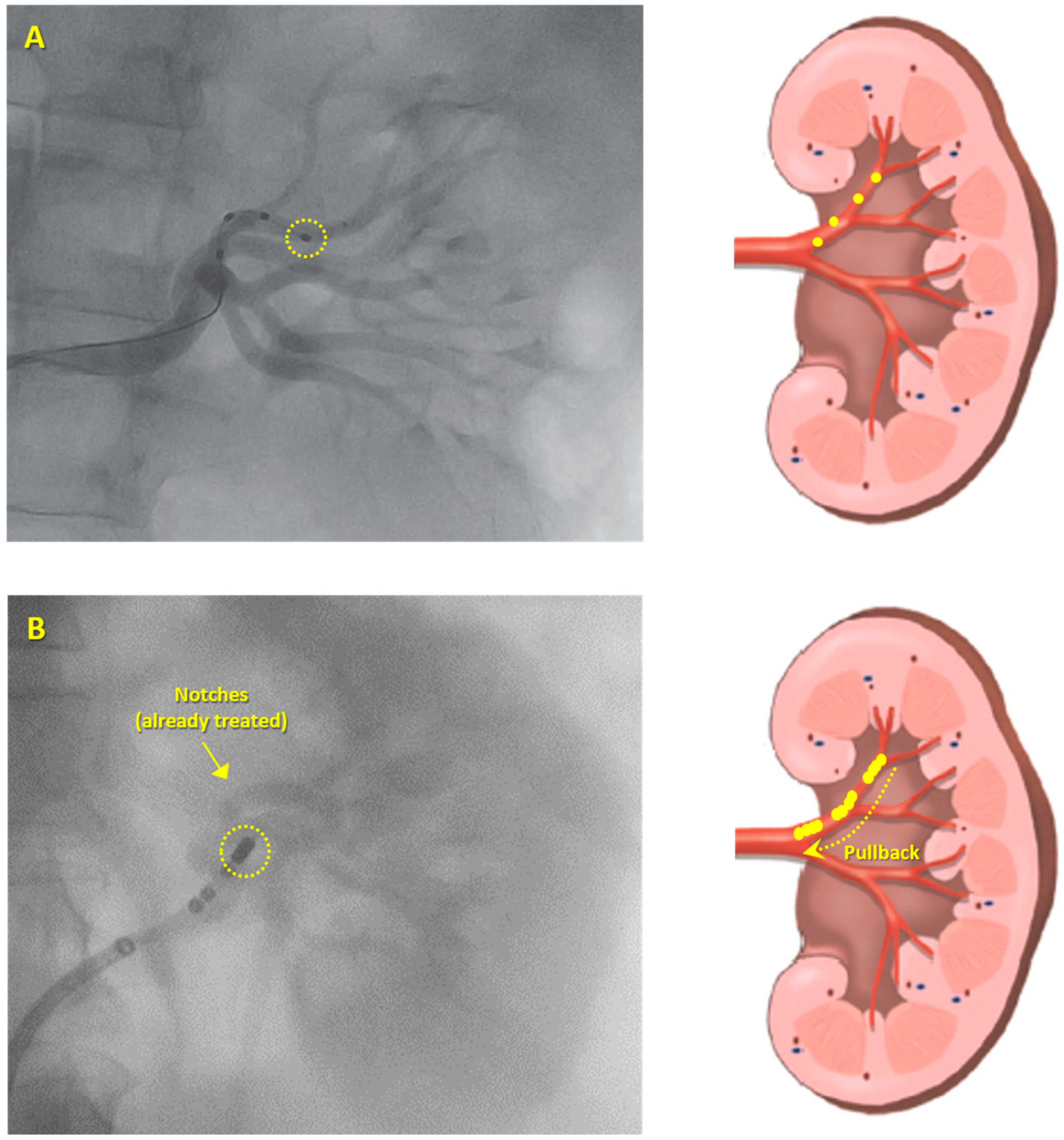
3.2. Ablation Procedure
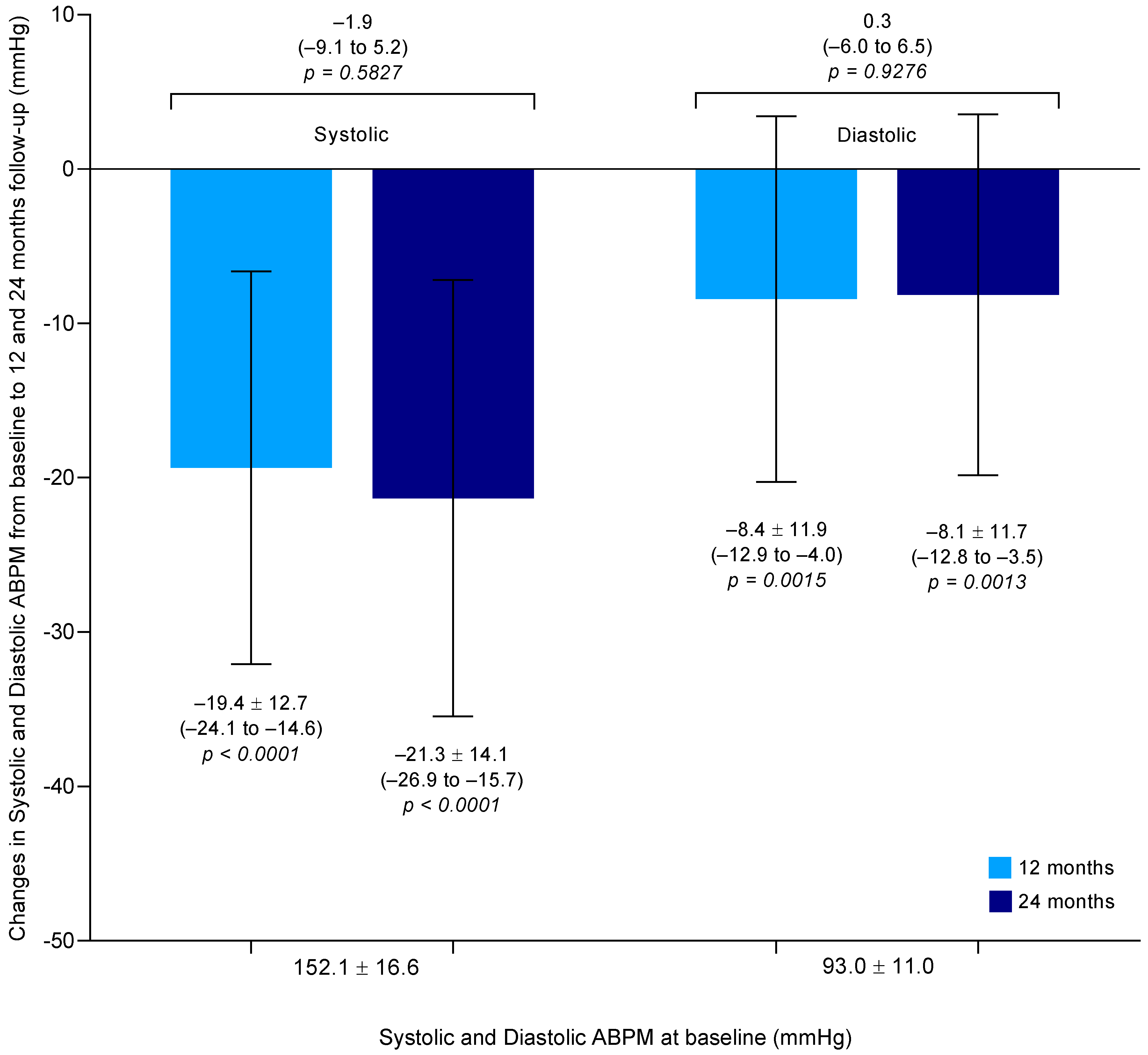
3.3. Systolic and Diastolic ABPM-Lowering Effect
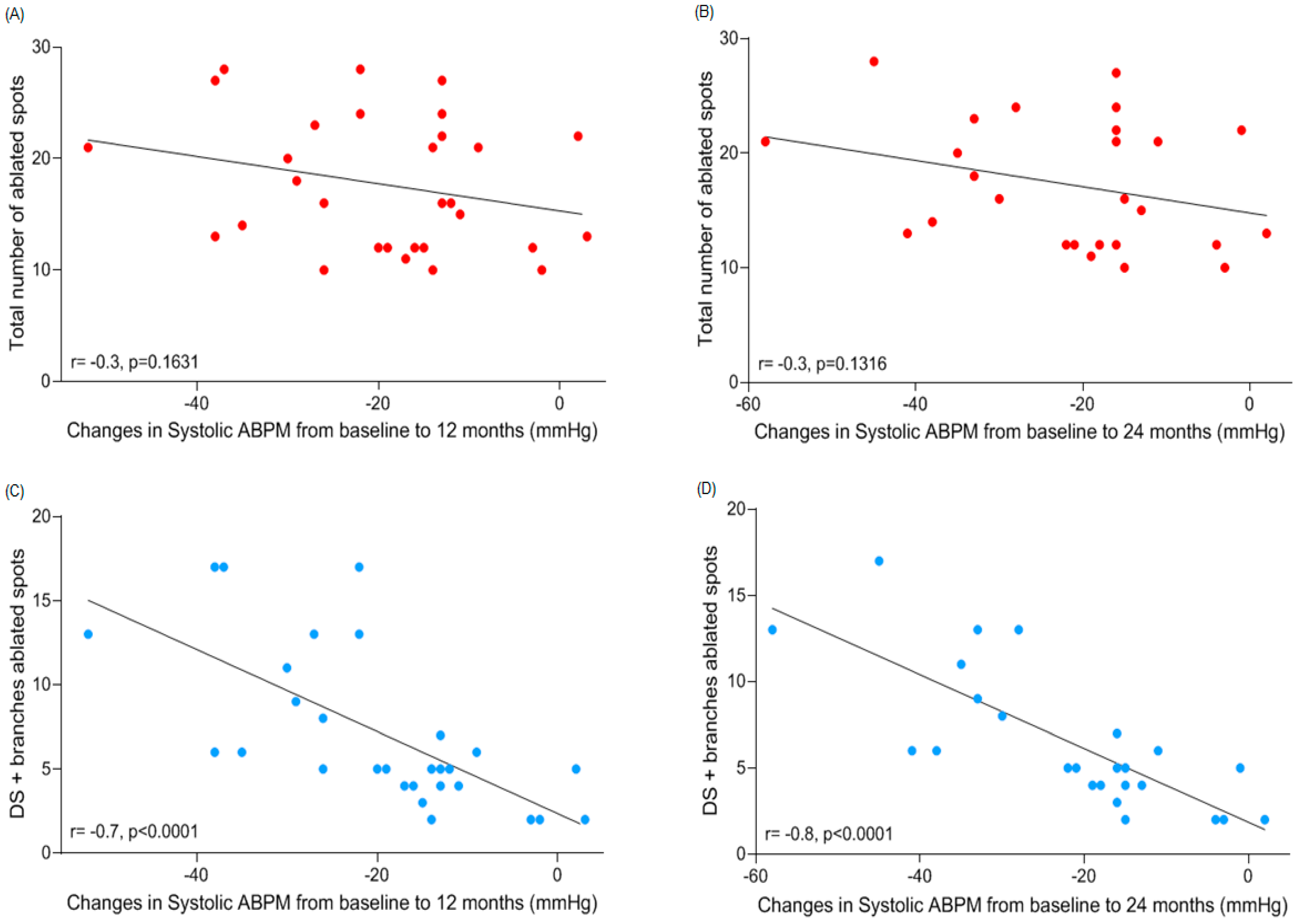
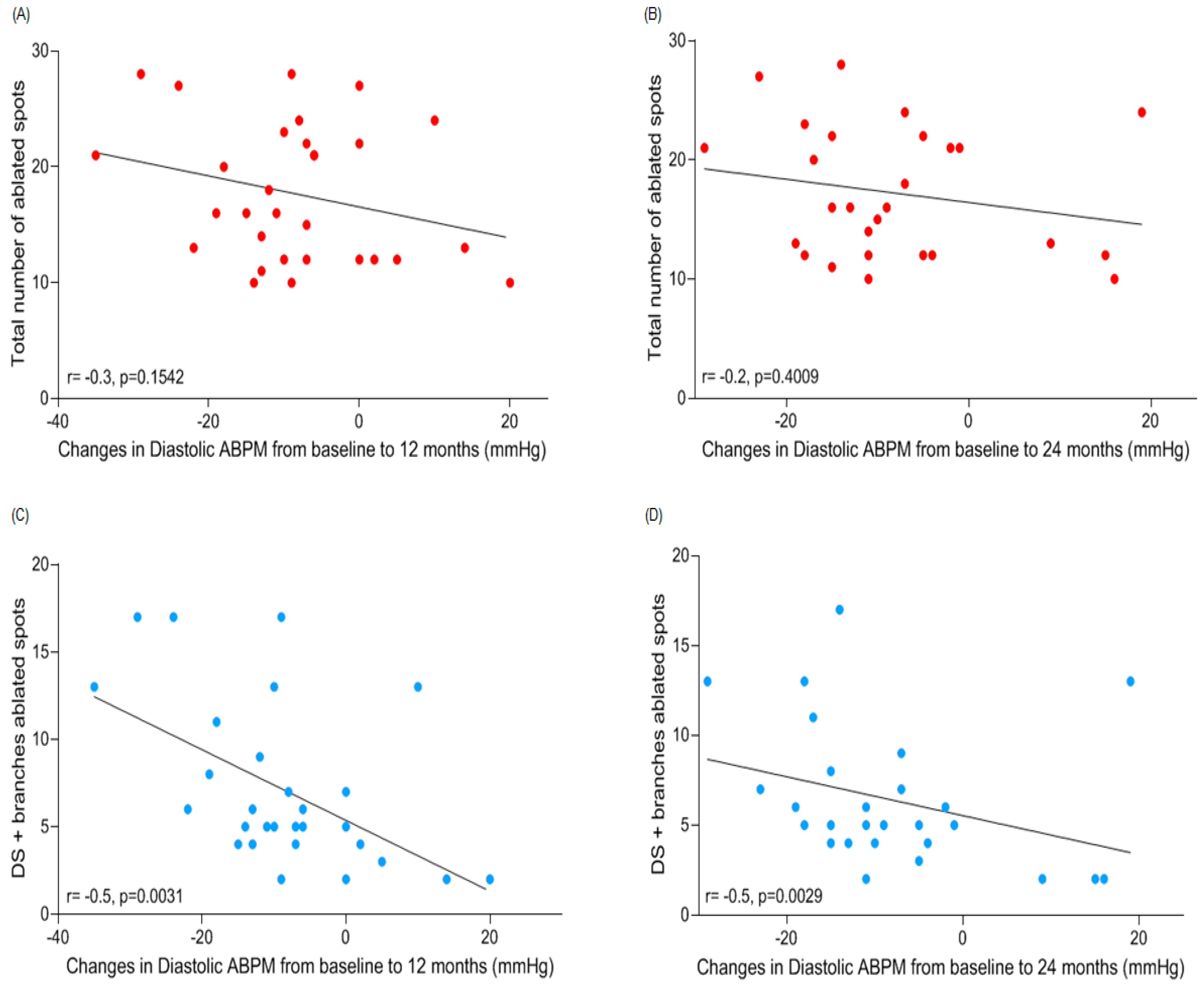
3.4. Correlations between Number of Ablated Spots per Segment and Changes in ABPM
4. Discussion
5. Study Limitations
6. Conclusions
7. Impact on Daily Practce
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Bohm, M.; Linz, D.; Ukena, C.; Esler, M.; Mahfoud, F. Renal denervation for the treatment of cardiovascular high risk-hypertension or beyond? Circ. Res. 2014, 115, 400–409. [Google Scholar] [CrossRef]
- Mahfoud, F.; Luscher, T.F.; Andersson, B.; Baumgartner, I.; Cifkova, R.; Dimario, C.; Doevendans, P.; Fagard, R.; Fajadet, J.; Komajda, M.; et al. Expert consensus document from the European Society of Cardiology on catheter-based renal denervation. Eur. Heart J. 2013, 34, 2149–2157. [Google Scholar] [CrossRef] [PubMed]
- Krum, H.; Schlaich, M.P.; Sobotka, P.A.; Bohm, M.; Mahfoud, F.; Rocha-Singh, K.; Katholi, R.; Esler, M.D. Percutaneous renal denervation in patients with treatment-resistant hypertension: Final 3-year report of the Symplicity HTN-1 study. Lancet 2014, 383, 622–629. [Google Scholar] [PubMed]
- Esler, M.D.; Bohm, M.; Sievert, H.; Rump, C.L.; Schmieder, R.E.; Krum, H.; Mahfoud, F.; Schlaich, M.P. Catheter-based renal denervation for treatment of patients with treatment-resistant hypertension: 36 month results from the SYMPLICITY HTN-2 randomized clinical trial. Eur. Heart J. 2014, 35, 1752–1759. [Google Scholar] [CrossRef] [PubMed]
- Azizi, M.; Sapoval, M.; Gosse, P.; Monge, M.; Bobrie, G.; Delsart, P.; Midulla, M.; Mounier-Véhier, C.; Courand, P.Y.; Lantelme, P.; et al. Optimum and stepped care standardised antihypertensive treatment with or without renal denervation for resistant hypertension (DENERHTN): A multicentre, open-label, randomised controlled trial. Lancet 2015, 385, 1957–1965. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Kandzari, D.E.; O’Neill, W.W.; D’Agostino, R.; Flack, J.M.; Katzen, B.T.; Leon, M.B.; Liu, M.; Mauri, L.; Negoita, M.; et al. A controlled trial of renal denervation for resistant hypertension. N. Engl. J. Med. 2014, 370, 1393–1401. [Google Scholar] [CrossRef]
- Rosa, J.; Widimsky, P.; Tousek, P.; Petrak, O.; Curila, K.; Waldauf, P.; Bednář, F.; Zelinka, T.; Holaj, R.; Štrauch, B.; et al. Randomized comparison of renal denervation versus intensified pharmacotherapy including spironolactone in true-resistant hypertension: Six-month results from the Prague-15 study. Hypertension 2015, 65, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Mahfoud, F.; Ukena, C.; Schmieder, R.E.; Cremers, B.; Rump, L.C.; Vonend, O.; Weil, J.; Schmidt, M.; Hoppe, U.C.; Zeller, T.; et al. Ambulatory blood pressure changes after renal sympathetic denervation in patients with resistant hypertension. Circulation 2013, 128, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Kindermann, I.; Wedegartner, S.M.; Mahfoud, F.; Weil, J.; Brilakis, N.; Ukena, J.; Ewen, S.; Linz, D.; Fahy, M.; Mancia, G.; et al. Improvement in health-related quality of life after renal sympathetic denervation in real-world hypertensive patients: 12-month outcomes in the Global SYMPLICITY Registry. J. Clin. Hypertens. 2017, 19, 833–839. [Google Scholar]
- Mahfoud, F.; Tunev, S.; Ewen, S.; Cremers, B.; Ruwart, J.; Schulz-Jander, D.; Linz, D.; Davies, J.; Kandzari, D.E.; Whitbourn, R.; et al. Impact of Lesion Placement on Efficacy and Safety of Catheter-Based Radiofrequency Renal Denervation. J. Am. Coll. Cardiol. 2015, 66, 1766–1775. [Google Scholar] [CrossRef] [PubMed]
- Townsend, R.R.; Mahfoud, F.; Kandzari, D.E.; Kario, K.; Pocock, S.; Weber, M.A.; Ewen, S.; Tsioufis, K.; Tousoulis, D.; Sharp, A.S.P.; et al. Catheter-based renal denervation in patients with uncontrolled hypertension in the absence of antihypertensive medications (SPYRAL HTN-OFF MED): A randomised, sham-controlled, proof-of-concept trial. Lancet 2017, 390, 2160–2170. [Google Scholar] [CrossRef]
- Kandzari, D.E.; Bohm, M.; Mahfoud, F.; Townsend, R.R.; Weber, M.A.; Pocock, S.; Tsioufis, K.; Tousoulis, D.; Choi, J.W.; East, C.; et al. Effect of renal denervation on blood pressure in the presence of antihypertensive drugs: 6-month efficacy and safety results from the SPYRAL HTN-ON MED proof-of-concept randomised trial. Lancet 2018, 391, 2346–2355. [Google Scholar] [CrossRef]
- Schlaich, M.P.; Kiuchi, M.G.; Esler, M.D. Renal Denervation-Ready for Prime Time!? The Steep SPYRAL Stairs to RADIANCE in Hypertension Treatment. Hypertension 2018, 72, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Kiuchi, M.G.; Maia, G.L.M.; Carreira, M.A.M.D.; Kiuchi, T.; Chen, S.C.; Andrea, B.R.; Graciano, M.L.; Lugon, J.R. Effects of renal denervation with a standard irrigated cardiac ablation catheter on blood pressure and renal function in patients with chronic kidney disease and resistant hypertension. Eur. Heart J. 2013, 34, 2114–2121. [Google Scholar] [CrossRef] [PubMed]
- Kiuchi, M.G.; Graciano, M.L.; Carreira, M.A.M.D.; Kiuchi, T.; Chen, S.J.; Lugon, J.R. Long-Term Effects of Renal Sympathetic Denervation on Hypertensive Patients With Mild to Moderate Chronic Kidney Disease. J. Clin. Hypertens. 2016, 18, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Sociedade Brasileira de, C.; Sociedade Brasileira de, H.; Sociedade Brasileira de, N. VI Brazilian Guidelines on Hypertension. Arq Bras. Cardiol. 2010, 95, 1–51. [Google Scholar]
- Mancia, G.; De Backer, G.; Dominiczak, A.; Cifkova, R.; Fagard, R.; Germano, G.; Grassi, G.; Heagerty, A.M.; Kjeldsen, S.E.; Laurent, S.; et al. 2007 Guidelines for the management of arterial hypertension—The task force for the management of arterial hypertension of the European society of hypertension (ESH) and of the European society of cardiology (ESC). Eur. Heart J. 2007, 28, 1462–1536. [Google Scholar]
- Krum, H.; Schlaich, M.; Whitbourn, R.; Sobotka, P.A.; Sadowski, J.; Bartus, K.; Kapelak, B.; Walton, A.; Sievert, H.; Thambar, S.; et al. Catheter-based renal sympathetic denervation for resistant hypertension: A multicentre safety and proof-of-principle cohort study. Lancet 2009, 373, 1275–1281. [Google Scholar] [CrossRef]
- Esler, M. Illusions of truths in the Symplicity HTN-3 trial: Generic design strengths but neuroscience failings. J. Am. Soc. Hypertens. 2014, 8, 593–598. [Google Scholar] [CrossRef]
- Nakagawa, H.; Yamanashi, W.S.; Pitha, J.V.; Arruda, M.; Wang, X.; Ohtomo, K.; Beckman, K.J.; McClelland, J.H.; Lazzara, R.; Jackman, W.M. Comparison of in vivo tissue temperature profile and lesion geometry for radiofrequency ablation with a saline-irrigated electrode versus temperature control in a canine thigh muscle preparation. Circulation 1995, 91, 2264–2273. [Google Scholar] [CrossRef]
- Mahfoud, F.; Luscher, T.F. Renal denervation: Symply trapped by complexity? Eur. Heart J. 2015, 36, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Vink, E.E.; Goldschmeding, R.; Vink, A.; Weggemans, C.; Bleijs, R.L.; Blankestijn, P.J. Limited destruction of renal nerves after catheter-based renal denervation: Results of a human case study. Nephrol Dial. Transplant. 2014, 29, 1608–1610. [Google Scholar] [CrossRef]
- Atherton, D.S.; Deep, N.L.; Mendelsohn, F.O. Micro-anatomy of the renal sympathetic nervous system: A human postmortem histologic study. Clin. Anat. 2012, 25, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Foss, J.D.; Wainford, R.D.; Engeland, W.C.; Fink, G.D.; Osborn, J.W. A novel method of selective ablation of afferent renal nerves by periaxonal application of capsaicin. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2015, 308, R112–R122. [Google Scholar] [CrossRef] [PubMed]
- Restini, C.B.A.; Ismail, A.; Kumar, R.K.; Burnett, R.; Garver, H.; Fink, G.D.; Watts, S.W. Renal perivascular adipose tissue: Form and function. Vasc. Pharmacol. 2018, 106, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Mahfoud, F.; Edelman, E.R.; Bohm, M. Catheter-based renal denervation is no simple matter: Lessons to be learned from our anatomy? J. Am. Coll. Cardiol. 2014, 64, 644–646. [Google Scholar] [CrossRef]
- Sakakura, K.; Ladich, E.; Cheng, Q.; Otsuka, F.; Yahagi, K.; Fowler, D.R.; Kolodgie, F.D.; Virmani, R.; Joner, M. Anatomic assessment of sympathetic peri-arterial renal nerves in man. J. Am. Coll. Cardiol. 2014, 64, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Grassi, G. Sympathetic neural activity in hypertension and related diseases. Am. J. Hypertens. 2010, 23, 1052–1060. [Google Scholar] [CrossRef]
- Grassi, G. Assessment of sympathetic cardiovascular drive in human hypertension: Achievements and perspectives. Hypertension 2009, 54, 690–697. [Google Scholar] [CrossRef]
- Schlaich, M.P.; Socratous, F.; Hennebry, S.; Eikelis, N.; Lambert, E.A.; Straznicky, N.; Esler, M.D.; Lambert, G.W. Sympathetic activation in chronic renal failure. J. Am. Soc. Nephrol. 2009, 20, 933–939. [Google Scholar] [CrossRef]
- Neumann, J.; Ligtenberg, G.; Klein, I.I.; Koomans, H.A.; Blankestijn, P.J. Sympathetic hyperactivity in chronic kidney disease: Pathogenesis, clinical relevance, and treatment. Kidney Int. 2004, 65, 1568–1576. [Google Scholar] [CrossRef] [PubMed]
- Grassi, G.; Bertoli, S.; Seravalle, G. Sympathetic nervous system: Role in hypertension and in chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2012, 21, 46–51. [Google Scholar] [CrossRef] [PubMed]
- McGrath, B.P.; Ledingham, J.G.; Benedict, C.R. Catecholamines in peripheral venous plasma in patients on chronic haemodialysis. Clin. Sci. Mol. Med. 1978, 55, 89–96. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Values |
|---|---|
| n | 30 |
| Age (years) | 55 ± 10 |
| Female sex (%) | 17 (57%) |
| Ethnicity (non-white) (%) | 21 (70%) |
| Body mass index, kg/m2 | 30.8 ± 4.9 |
| Coronary artery disease (%) | 5 (17%) |
| Atrial fibrillation (%) | 2 (7%) |
| Stroke (%) | 6 (20%) |
| Type 2 diabetes (%) | 11 (37%) |
| LDL-cholesterol >130 mg/dL (%) | 19 (63%) |
| Smoking (%) | 3 (10%) |
| Mean office systolic/diastolic blood pressure, mmHg | 184.9 ± 18.4/106.9 ± 13.3 |
| Mean 24-h systolic/diastolic ABPM, mmHg | 152.1 ± 16.6/93.0 ± 11.0 |
| eGFR, mL/min/1.73 m2 (CKD-EPI) | 61.9 ± 23.9 |
| Stages of CKD 2/3/4 | 19 (63%)/6 (20%)/5 (17%) |
| Number of antihypertensive medications (%) | 4.6 ± 1.4 |
| ACE-I | 5 (17%) |
| ARB | 25 (83%) |
| Aliskiren | 3 (10%) |
| α-1 blocker | 1 (3%) |
| β-blocker | 24 (80%) |
| Clonidine or Moxonidine | 11 (37%) |
| Calcium channel blocker | 25 (83%) |
| Diuretic | 30 (100%) |
| Aldosterone antagonist | 3 (10%) |
| Vasodilator | 4 (13%) |
| Mean ± SD | Difference between Means (95% CI) | ||||
|---|---|---|---|---|---|
| Total | 17.7 ± 6.0 | - | - | - | - |
| PS vs. MS | PS vs. DS | PS vs. Br | PS vs. DS + Br | ||
| Proximal segment (PS) | 5.2 ± 1.8 | 0.2 (−04 to 0.8) p = 0.9039 | 0.0 (−1.5 to 1.5) p > 0.9999 | 3.3 (1.4 to 5.3) p = 0.0002 | 1.9 (−0.9 to 4.6) p = 0.3227 |
| MS vs. DS | MS vs. Br | MS vs. DS + Br | |||
| Middle segment (MS) | 5.4 ± 2.0 | - | 0.2 (−1.3 to 1.7) p = 0.9984 | 3.5 (1.5 to 5.5) p = 0.0001 | 1.7 (−1.1 to 4.4) p = 0.4626 |
| DS vs. Br | DS vs. DS + Br | ||||
| Distal segment (DS) | 5.2 ± 2.1 | - | - | 3.3 (2.2 to 4.5) p < 0.0001 | 1.9 (0.3 to 3.5) p = 0.0144 |
| Br vs. DS + Br | |||||
| Branches (Br) | 1.9 ± 2.9 | - | - | - | 5.2 (4.0 to 6.4) p < 0.0001 |
| Distal segment (DS) + branches (Br) | 7.1 ± 4.6 | - | - | - | - |
| Our Findings a | SYMPLICITY HTN-3 b | ||||||
|---|---|---|---|---|---|---|---|
| 12 Months | 24 Months | 12 Months | |||||
| n | 30 | 27 | 31 | 31 | 32 | 32 | 24 |
| Number of ablations | average 18 | ≤9 | 10 | 11 | 12 or 13 | ≥14 | |
| Changes in systolic ABPM from baseline, mmHg | −19.4 ± 12.7 p < 0.0001 | −21.3 ± 14.1 p < 0.0001 | −2.8 ± 10.8 p = 0.02 | −6.9 ± 15.5 p = 0.78 | −0.4 ± 18.2 p = 0.77 | −9.3 ± 9.6 p = 0.002 | −12.2 ± 19.1 p = 0.16 |
| Difference between means, mmHg (95% CI) | −16.6 (−26.1 to −7.1) p < 0.0001 | −12.5 (−22.0 to −3.0) p = 0.0046 | −19.0 (−28.4 to −9.6) p < 0.0001 | −10.1 (−19.5 to −0.7) p = 0.0299 | −7.2 (−17.3 to 2.9) p = 0.2526 | ||
| Our findings at 12 months vs. SYMPLICITY HTN-3 | |||||||
| Difference between means, mmHg (95% CI) | −18.5 (−28.3 to −8.7) p < 0.0001 | −14.4 (−24.3 to −4.6) p = 0.0014 | −20.9 (−30.7 to −11.1) p < 0.0001 | −12.0 (−21.8 to −2.2) p = 0.0098 | −9.1 (−19.6 to 1.4) p = 0.1116 | ||
| Our findings at 24 months vs. SYMPLICITY HTN-3 | |||||||
| SPYRAL HTN | ||||
|---|---|---|---|---|
| Our Findings a | OFF MED b | ON MED b | ||
| 12 Months | 24 Months | 3 Months | 6 Months | |
| n | 30 | 27 | 37 | 36 |
| Changes in systolic ABPM from baseline, mmHg | −19.4 ± 12.7 (−24.1 to −14.6) p < 0.0001 | −21.3 ± 14.1 (−26.9 to −15.7) p < 0.0001 | −5.5 ± 13.9 * (−9.1 to −2.0) p = 0.0031 | −9.0 ± 11.0 (−12.7 to −5.3) p < 0.0001 |
| Difference between means, mmHg (95% CI) | −13.9 (−22.2 to −5.6) p = 0.0001 | −10.4 (−18.7 to −2.1) p = 0.0078 | ||
| Our findings at 12 months vs. SPYRAL HTN | ||||
| Difference between means, mmHg (95% CI) | −15.8 (−24.3 to −7.3) p < 0.0001 | −12.3 (−20.9 to −3.7) p = 0.0016 | ||
| Our findings at 24 months vs. SPYRAL HTN | ||||
| SPYRAL HTN | |||
|---|---|---|---|
| Our Findings a | OFF MED b | ON MED b | |
| Total | 17.7 ± 6.0 | 43.8 ± 11.1 | 45.9 ± 13.7 |
| Difference between means (95% CI) Our findings vs. SPYRAL HTN | - | −26.1 (−32.5 to −19.7) p < 0.0001 | −28.2 (−34.7 to −21.7) p < 0.0001 |
| Ablations in the main artery (proximal, middle and distal segments) | 5.3 ± 2.0 | 17.9 ± 10.5 | 19.3 ± 8.9 |
| Difference between means (95% CI) Our findings vs. SPYRAL HTN | - | −12.7 (−17.5 to −7.9) p < 0.0001 | −14.1 (−19.0 to −9.2) p < 0.0001 |
| Ablations in branches | 1.9 ± 2.9 | 25.9 ± 12.8 | 26.6 ± 11.7 |
| Difference between means (95% CI) Our findings vs. SPYRAL HTN | - | −24.0 (−30.1 to −17.9) p < 0.0001 | −24.7 (−30.9 to −18.6) p < 0.0001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiuchi, M.G.; Schlaich, M.P.; Chen, S.; Villacorta, H.; Ho, J.K.; Carnagarin, R.; Matthews, V.B.; Lugon, J.R. Relevance of Targeting the Distal Renal Artery and Branches with Radiofrequency Renal Denervation Approaches—A Secondary Analysis from a Hypertensive CKD Patient Cohort. J. Clin. Med. 2019, 8, 581. https://doi.org/10.3390/jcm8050581
Kiuchi MG, Schlaich MP, Chen S, Villacorta H, Ho JK, Carnagarin R, Matthews VB, Lugon JR. Relevance of Targeting the Distal Renal Artery and Branches with Radiofrequency Renal Denervation Approaches—A Secondary Analysis from a Hypertensive CKD Patient Cohort. Journal of Clinical Medicine. 2019; 8(5):581. https://doi.org/10.3390/jcm8050581
Chicago/Turabian StyleKiuchi, Márcio Galindo, Markus P. Schlaich, Shaojie Chen, Humberto Villacorta, Jan K. Ho, Revathy Carnagarin, Vance B. Matthews, and Jocemir Ronaldo Lugon. 2019. "Relevance of Targeting the Distal Renal Artery and Branches with Radiofrequency Renal Denervation Approaches—A Secondary Analysis from a Hypertensive CKD Patient Cohort" Journal of Clinical Medicine 8, no. 5: 581. https://doi.org/10.3390/jcm8050581