Systemic Sclerosis Is Linked to Psoriasis and May Impact on Patients’ Survival: A Large Cohort Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Ethical Clearance
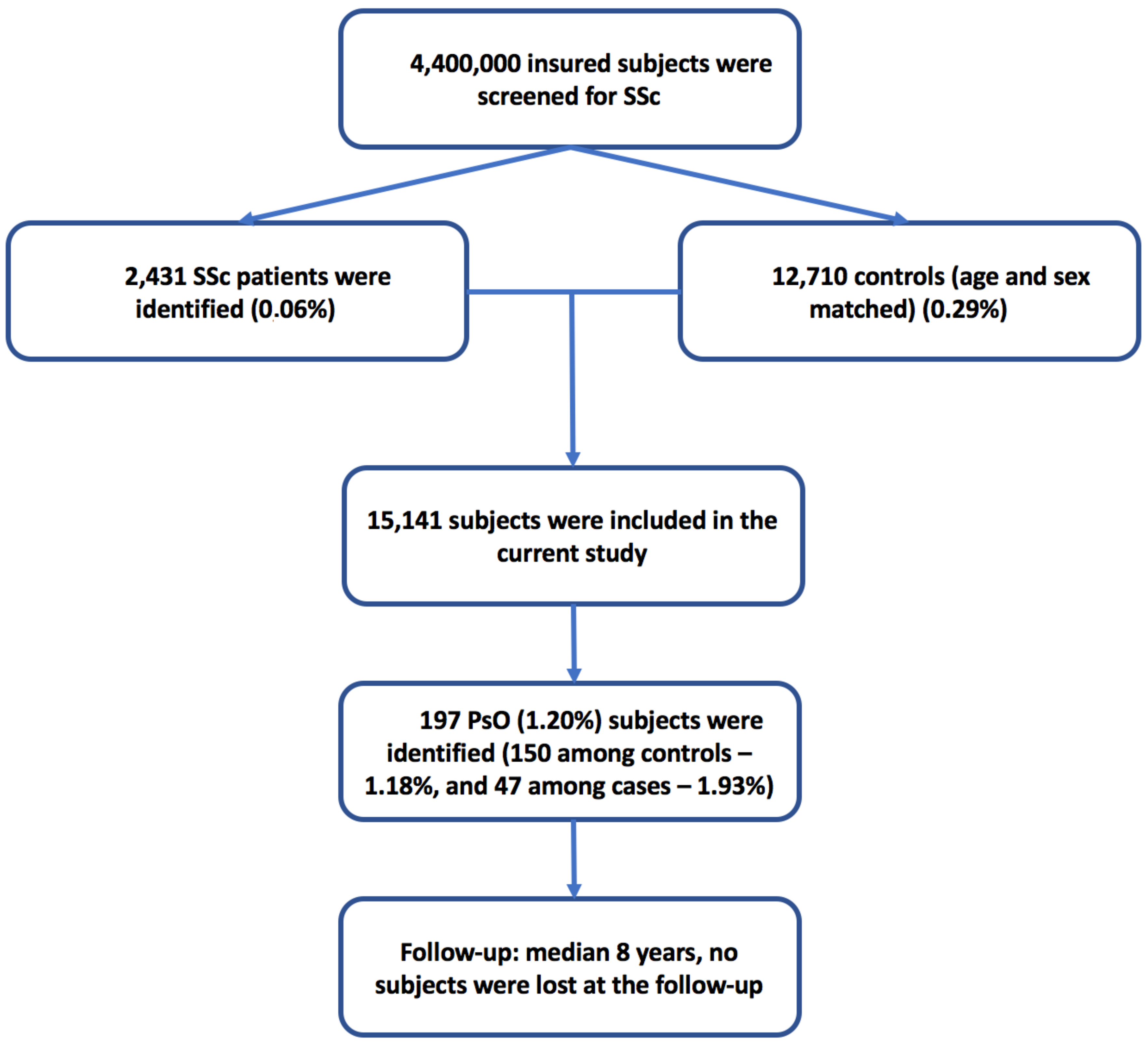
2.2. Design, Sample and Procedures
2.3. Measures
2.4. Statistical Analyses
3. Results
3.1. Basic Characteristics of the Study Population
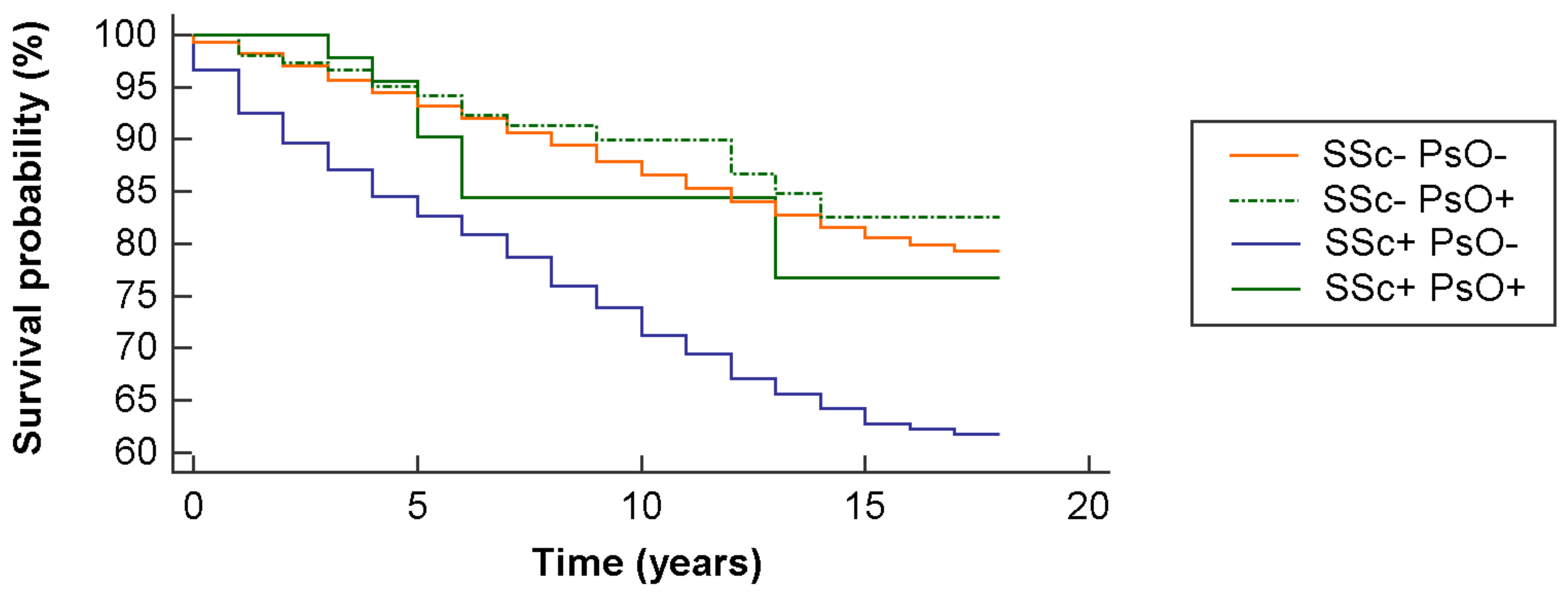
3.2. Mortality Rates and Survival Analysis
3.3. Independent Predictors of Psoriasis
3.4. Independent Predictors of All-Cause Mortality
3.5. Role of SSc-Linked Autoantibodies in the Co-Existence of SSc and PsO
3.6. The Temporal Relationship between SSc and PsO Diagnoses
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Denton, C.P.; Khanna, D. Systemic sclerosis. Lancet 2017, 390, 1685–1699. [Google Scholar] [CrossRef]
- The Lancet. Systemic sclerosis: Advances and prospects. Lancet 2017, 390, 1624. [Google Scholar] [CrossRef]
- Rongioletti, F.; Kaiser, F.; Cinotti, E.; Metze, D.; Battistella, M.; Calzavara-Pinton, P.G.; Damevska, K.; Girolomoni, G.; André, J.; Perrot, J.L.; et al. Scleredema. A multicentre study of characteristics, comorbidities, course and therapy in 44 patients. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 2399–2404. [Google Scholar] [CrossRef]
- Valentini, G.; Cuomo, G. Skin Manifestations of Systemic Sclerosis. In Skin Manifestations in Rheumatic Disease; Matucci-Cerinic, M., Furst, D., Fiorentino, D., Eds.; Springer: New York, NY, USA, 2014; pp. 191–200. [Google Scholar]
- Czirjak, L.; Foeldvari, I.; Muller-Ladner, U. Skin involvement in systemic sclerosis. Rheumatology (Oxf. Engl.) 2008, 47 (Suppl. 5), v44–v45. [Google Scholar] [CrossRef] [PubMed]
- Gabrielli, A.; Avvedimento, E.V.; Krieg, T. Scleroderma. NEJM 2009, 360, 1989–2003. [Google Scholar] [CrossRef]
- Arnett, F.C.; Gourh, P.; Shete, S.; Ahn, C.W.; Honey, R.E.; Agarwal, S.K.; Tan, F.K.; McNearney, T.; Fischbach, M.; Fritzler, M.J.; et al. Major histocompatibility complex (MHC) class II alleles, haplotypes and epitopes which confer susceptibility or protection in systemic sclerosis: Analyses in 1300 Caucasian, African-American and Hispanic cases and 1000 controls. Ann. Rheum. Dis. 2010, 69, 822–827. [Google Scholar] [CrossRef] [PubMed]
- Radstake, T.R.; Gorlova, O.; Rueda, B.; Martin, J.E.; Alizadeh, B.Z.; Palomino-Morales, R.; Coenen, M.J.; Vonk, M.C.; Voskuyl, A.E.; Schuerwegh, A.J.; et al. Genome-wide association study of systemic sclerosis identifies CD247 as a novel susceptibility locus. Nat. Genet. 2010, 42, 426–429. [Google Scholar] [CrossRef]
- Damiani, G.; Radaeli, A.; Olivini, A.; Calvara-Pinton, P.; Malerba, M. Increased airway inflammation in patients with psoriasis. Br. J. Dermatol. 2016, 175, 797–799. [Google Scholar] [CrossRef]
- Fiore, M.; Leone, S.; Maraolo, A.E.; Berti, E.; Damiani, G. Liver Illness and Psoriatic Patients. BioMed. Res. Int. 2018, 2018, 3140983. [Google Scholar] [CrossRef]
- Sticherling, M. Psoriasis and autoimmunity. Autoimmun Rev. 2016, 15, 1167–1170. [Google Scholar] [CrossRef]
- Christophers, E. Psoriasis—Epidemiology and clinical spectrum. Clin. Exp. Dermatol. 2002, 26, 314–320. [Google Scholar] [CrossRef]
- Schön, M.P.; Boehncke, W.H. Psoriasis. NEJM 2005, 352, 1899–1912. [Google Scholar] [CrossRef] [PubMed]
- Christophers, E. The Immunopathology of Psoriasis. Int. Arch. Allergy Immunol. 1996, 110, 199–206. [Google Scholar] [CrossRef]
- Di Meglio, P.; Duarte, J.H. CD8 T Cells and IFN-gamma emerge as critical players for psoriasis in a novel model of mouse psoriasiform skin inflammation. J. Investig. Dermatol. 2013, 133, 871–874. [Google Scholar] [CrossRef]
- Kim, J.; Krueger, J.G. The immunopathogenesis of psoriasis. Dermatol. Clin. 2015, 33, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Lande, R.; Botti, E.; Jandus, C.; Dojcinovic, D.; Fanelli, G.; Conrad, C.; Chamilos, G.; Feldmeyer, L.; Marinari, B.; Chon, S.; et al. The antimicrobial peptide LL37 is a T-cell autoantigen in psoriasis. Nat. Commun. 2014, 5, 5621. [Google Scholar] [CrossRef]
- Prinz, J.C. Melanocytes: Target Cells of an HLA-C*06:02-Restricted Autoimmune Response in Psoriasis. J. Investig. Dermatol. 2017, 137, 2053–2058. [Google Scholar] [CrossRef]
- Harrison, B.; Herrick, A.; Griffiths, C. Psoriasis and diffuse systemic sclerosis: A report of three patients. Rheumatol (Oxf. Engl.) 2000, 39, 213–215. [Google Scholar] [CrossRef]
- Bellissimo, S.; Iannone, F.; Musio, A.; Covelli, M.; Lapadula, G. Association of systemic sclerosis and psoriatic arthritis: A case report. Reumatismo 2001, 53, 232–234. [Google Scholar] [CrossRef]
- Wu, M.; Assassi, S. The Role of Type 1 Interferon in Systemic Sclerosis. Front. Immunol. 2013, 4, 266. [Google Scholar] [CrossRef]
- Strange, A.; Capon, F.; Spencer, C.C.; Knight, J.; Weale, M.E.; Allen, M.H.; Barton, A.; Band, G.; Bellenguez, C.; Bergboer, J.G.; Blackwell, J.M.; et al. A genome-wide association study identifies new psoriasis susceptibility loci and an interaction between HLA-C and ERAP1. Genetic Analysis of Psoriasis Consortium and the Wellcome Trust Case Control Consortium 2. Nat. Genet. 2010, 42, 985–990. [Google Scholar] [CrossRef] [PubMed]
- Bragazzi, N.L.; Watad, A.; Gizunterman, A.; McGonagle, D.; Mahagna, H.; Comaneshter, D.; Amital, H.; Cohen, A.D.; Amital, D. The burden of depression in systemic sclerosis patients: A nationwide population-based study. J. Affect. Dis. 2018, 243, 427–431. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; Abu Much, A.; Bracco, D.; Mahroum, N.; Comaneshter, D.; Cohen, A.D.; Amital, H. Association between ischemic heart disease and systemic lupus erythematosus-a large case-control study. Immunol. Res. 2017, 65, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; Tiosano, S.; Azrielant, S.; Whitby, A.; Comaneshter, D.; Cohen, A.D.; Shoenfeld, Y.; Amital, H. Low levels of calcium or vitamin D-which is more important in systemic lupus erythematosus patients? An extensive data analysis. Clin. Exp. Rheumatol. 2017, 35, 108–112. [Google Scholar] [PubMed]
- Watad, A.; Tiosano, S.; Yahav, D.; Comaneshter, D.; Shoenfeld, Y.; Cohen, A.D.; Amital, H. Behcet’s disease and familial Mediterranean fever: Two sides of the same coin or just an association? A cross-sectional study. Eur. J. Int. Med. 2017, 39, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; Bragazzi, N.L.; Tiosano, S.; Yavne, Y.; Comaneshter, D.; Cohen, A.D.; Amital, H. Alzheimer’s Disease in Systemic Sclerosis Patients: A Nationwide Population-Based Cohort Study. J. Alzheimers Dis. 2018, 65, 117–124. [Google Scholar] [CrossRef]
- Kuchroo, V.K.; Ohashi, P.S.; Sartor, R.B.; Vinuesa, C.G. Dysregulation of immune homeostasis in autoimmune diseases. Nat. Med. 2012, 18, 42–47. [Google Scholar] [CrossRef]
- Vojdani, A. A Potential Link between Environmental Triggers and Autoimmunity. Autoimmune Dis. 2014, 2014, 437231. [Google Scholar] [CrossRef]
- Watad, A.; Azrielant, S.; Bragazzi, N.L.; Sharif, K.; David, P.; Katz, I.; Aljadeff, G.; Quaresma, M.; Tanay, G.; Adawi, M.; et al. Seasonality and autoimmune diseases: The contribution of the four seasons to the mosaic of autoimmunity. J. Autoimmun. 2017, 82, 13–30. [Google Scholar] [CrossRef]
- Marson, A.; Housley, W.J.; Hafler, D.A. Genetic basis of autoimmunity. J. Clin. Investig. 2015, 125, 2234–2241. [Google Scholar] [CrossRef]
- Gudjonsson, J.E.; Johnston, A.; Sigmundsdottir, H.; Valdimarsson, H. Immunopathogenic mechanisms in psoriasis. Clin. Exp. Immunol. 2004, 135, 1–8. [Google Scholar] [CrossRef]
- Sakkas, L.I.; Bogdanos, D.P. Systemic sclerosis: New evidence re-enforces the role of B cells. Autoimmun. Rev. 2016, 15, 155–161. [Google Scholar] [CrossRef]
- Schauber, J.; Dombrowski, Y.; Besch, R. Pathogenic DNA: Cytosolic DNA promotes inflammation in psoriasis. Cell Cycle (Georget. Tex.) 2011, 10, 3038–3039. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.F.; Luo, S.F.; Yu, K.H.; See, L.C.; Zhang, W.; Doherty, M. Familial risk of systemic sclerosis and co-aggregation of autoimmune diseases in affected families. Arthritis Res. Ther. 2016, 18, 231. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Reyna, T.S.; Mercado-Velázquez, P.; Yu, N.; Alosco, S.; Ohashi, M.; Lebedeva, T.; Cruz-Lagunas, A.; Núñez-Álvarez, C.; Cabiedes-Contreras, J.; Vargas-Alarcón, G.; et al. HLA Class I and II Blocks Are Associated to Susceptibility, Clinical Subtypes and Autoantibodies in Mexican Systemic Sclerosis (SSc) Patients. PLoS ONE 2015, 10, e0126727. [Google Scholar] [CrossRef]
- FitzGerald, O.; Haroon, M.; Giles, J.T.; Winchester, R. Concepts of pathogenesis in psoriatic arthritis: Genotype determines clinical phenotype. Arthritis Res. Ther. 2015, 17, 115. [Google Scholar] [CrossRef] [PubMed]
- Prinz, J.C. The role of T cells in psoriasis. J. Eur. Acad. Dermatol. Venereol. 2003, 17, 257–270. [Google Scholar] [CrossRef] [PubMed]
- Di Meglio, P.; Villanova, F.; Navarini, A.A.; Mylonas, A.; Tosi, I.; Nestle, F.O.; Conrad, C. Targeting CD8(+) T cells prevents psoriasis development. J. Allergy Clin. Immunol. 2016, 138, 274–276.e6. [Google Scholar] [CrossRef]
- O’Reilly, S.; Hugle, T.; van Laar, J.M. T cells in systemic sclerosis: A reappraisal. Rheumatology (Oxf. Engl.) 2012, 51, 1540–1549. [Google Scholar] [CrossRef]
- Coelho, L.F.; de Oliveira, J.G.; Kroon, E.G. Interferons and scleroderma-a new clue to understanding the pathogenesis of scleroderma? Immunol. Lett. 2008, 118, 110–115. [Google Scholar] [CrossRef]
- Afshar, M.; Martinez, A.D.; Gallo, R.L.; Hata, T.R. Induction and exacerbation of psoriasis with Interferon-alpha therapy for hepatitis C: A review and analysis of 36 cases. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Rosen, A.; Casciola-Rosen, L. Autoantigens as substrates for apoptotic proteases: Implications for the pathogenesis of systemic autoimmune disease. Cell Death Differ. 1999, 6, 6–12. [Google Scholar] [CrossRef]
- Casciola-Rosen, L.; Rosen, A. Ultraviolet light-induced keratinocyte apoptosis: A potential mechanism for the induction of skin lesions and autoantibody production in LE. Lupus 1997, 6, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.A. Skin resident T cells: The ups and downs of on site immunity. J. Investig. Dermatol. 2010, 130, 362–370. [Google Scholar] [CrossRef] [PubMed]
- McGonagle, D.; Aydin, S.Z.; Gul, A.; Mahr, A.; Direskeneli, H. ‘MHC-I-opathy’-unified concept for spondyloarthritis and Behcet disease. Nat. Rev. Rheumatol. 2015, 11, 731–740. [Google Scholar] [CrossRef] [PubMed]
- Caricchio, R.; McPhie, L.; Cohen, P.L. Ultraviolet B radiation-induced cell death: Critical role of ultraviolet dose in inflammation and lupus autoantigen redistribution. J. Immunol. (Baltim. Md. 1950) 2003, 171, 5778–5786. [Google Scholar] [CrossRef]
- Shalom, G.; Zisman, D.; Babaev, M.; Horev, A.; Tiosano, S.; Schonmann, Y.; Comaneshter, D.; Cohen, A.D. Psoriasis in Israel: Demographic, epidemiology, and healthcare services utilization. Int. J. Dermatol. 2018, 57, 1068–1074. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | All Population (n = 15,141) | Controls without SSc (n = 12,710) | SSc Patients (n = 2431) | Statistical Significance (p-Value) |
|---|---|---|---|---|
| Age (mean ± SD; median) | 63.32 ± 18.06; 66 | 63.44 ± 18.08; 66 | 62.69 ± 17.90; 66 | NS |
| Age at diagnosis/beginning of the follow-up (mean ± SD; median) | 54.57 ± 18.64; 57 | 54.54 ± 18.63; 57 | 54.77 ± 18.67; 57 | NS |
| Gender (female; %) | 12,377 (81.7%) | 10,390 (81.7%) | 1987 (81.7%) | NS |
| BMI (n; %) a | <0.001 | |||
| <20 kg/m2 | 1283 (9.2%) | 1098 (8.6%) | 185 (15.6%) | |
| 20–25 kg/m2 | 4189 (30.1%) | 3803 (29.9%) | 386 (32.5%) | |
| 25–30 kg/m2 | 4380 (31.5%) | 4055 (31.9%) | 325 (27.4%) | |
| >30 kg/m2 | 4045 (29.1%) | 3754 (29.5%) | 291 (24.5%) | |
| SES (n; %) b | <0.001 | |||
| Low | 5763 (40.4%) | 4769 (39.7%) | 994 (44.4%) | |
| Medium | 5364 (37.6%) | 4543 (37.8%) | 821 (36.7%) | |
| High | 3122 (22.0%) | 2699 (22.5%) | 423 (18.9%) | |
| Smoking (n; %) | 4332 (28.6%) | 3628 (28.5%) | 704 (29.0%) | NS |
| Psoriasis (n; %) | 197 (1.3%) | 150 (1.2%) | 47 (1.9%) | 0.0027 |
| All-cause mortality (n; %) | 2226 (14.7%) | 1589 (12.5%) | 637 (26.2%) | <0.001 |
| Parameter | SSc- PsO- | SSc- PsO+ | SSc+ PsO- | SSc+ PsO+ | Statistical Significance (p-Value) |
|---|---|---|---|---|---|
| (n = 12,560) | (n = 150) | (n = 2384) | (n = 47) | ||
| Age | 63.39 ± 18.12 | 67.76 ± 14.11 | 62.65 ± 17.96 | 64.47 ± 14.57 | 0.0109 |
| Gender (female) | 10,268 (81.8%) | 122 (81.3%) | 1949 (81.8%) | 38 (80.9%) | 0.9977 |
| BMI | p < 0.0001 | ||||
| BMI <20 kg/m2 | 1091 (8.7%) | 7 (4.7%) | 182 (15.7%) | 3 (11.1%) | |
| BMI 20–25 kg/m2 | 3772 (30.0%) | 31 (20.7%) | 376 (32.4%) | 10 (37.0%) | |
| BMI 25–30 kg/m2 | 4005 (31.9%) | 50 (33.3%) | 321 (27.7%) | 4 (14.8%) | |
| BMI >30 kg/m2 | 3692 (29.4%) | 62 (41.3%) | 281 (24.2%) | 10 (37.0%) | |
| SES | p < 0.0001 | ||||
| Low | 4731 (39.9%) | 38 (27.1%) | 978 (44.5%) | 16 (39.0%) | |
| Medium | 4478 (37.7%) | 65 (46.4%) | 807 (36.7%) | 14 (34.1%) | |
| High | 2662 (22.4%) | 37 (26.4%) | 412 (18.8%) | 11 (26.8%) | |
| Smoking status | 3573 (28.4%) | 55 (36.7%) | 680 (28.5%) | 24 (51.1%) | 0.0009 |
| Mean age at psoriasis onset/beginning of the follow-up | 54.48 ± 18.67 | 58.90 ± 14.39 | 54.74 ± 18.71 | 56.09 ± 16.25 | 0.0740 |
| Mortality rate | 1573 (12.5%) | 16 (10.7%) | 630 (26.4%) | 7 (14.9%) | p < 0.0001 |
| Variable | Coefficient | Standard Error | Wald | p-Value | OR | 95% CI |
|---|---|---|---|---|---|---|
| Age | 0.01 | 0.01 | 2.47 | 0.1162 | 1.01 | 1.00 to 1.02 |
| BMI 20–25 kg/m2 | 0.21 | 0.37 | 0.31 | 0.5794 | 1.23 | 0.59 to 2.56 |
| BMI 25–30 kg/m2 | 0.49 | 0.37 | 1.78 | 0.1823 | 1.63 | 0.79 to 3.35 |
| BMI >30 kg/m2 | 0.84 | 0.36 | 5.40 | 0.0202 | 2.32 | 1.14 to 4.73 |
| Sex (female) | 0.15 | 0.22 | 0.50 | 0.4785 | 1.17 | 0.76 to 1.79 |
| SSc | 0.77 | 0.23 | 11.19 | 0.0008 | 2.16 | 1.38 to 3.39 |
| SES (medium) | 0.50 | 0.19 | 6.90 | 0.0086 | 1.65 | 1.14 to 2.41 |
| SES (high) | 0.64 | 0.21 | 8.90 | 0.0029 | 1.90 | 1.25 to 2.89 |
| Smoking | 0.40 | 0.17 | 5.86 | 0.0155 | 1.50 | 1.08 to 2.08 |
| Variable | Coefficient | Standard Error | Wald | p-Value | OR | 95% CI |
|---|---|---|---|---|---|---|
| ANA | −0.84 | 0.37 | 5.10 | 0.0239 | 0.43 | 0.21 to 0.89 |
| Anti-centromere | 0.000 | 0.35 | 0.00 | 0.9992 | 1.00 | 0.50 to 2.00 |
| Anti-SCL-70 | 0.48 | 0.39 | 1.47 | 0.2258 | 1.61 | 0.75 to 3.47 |
| Anti-RNA polymerase III | 0.72 | 0.59 | 1.50 | 0.2210 | 2.06 | 0.65 to 6.59 |
| Anti-RNP | −0.26 | 1.04 | 0.06 | 0.8022 | 0.77 | 0.10 to 5.95 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watad, A.; Bragazzi, N.L.; McGonagle, D.; Damiani, G.; Comaneshter, D.; Cohen, A.; Amital, H. Systemic Sclerosis Is Linked to Psoriasis and May Impact on Patients’ Survival: A Large Cohort Study. J. Clin. Med. 2019, 8, 521. https://doi.org/10.3390/jcm8040521
Watad A, Bragazzi NL, McGonagle D, Damiani G, Comaneshter D, Cohen A, Amital H. Systemic Sclerosis Is Linked to Psoriasis and May Impact on Patients’ Survival: A Large Cohort Study. Journal of Clinical Medicine. 2019; 8(4):521. https://doi.org/10.3390/jcm8040521
Chicago/Turabian StyleWatad, Abdulla, Nicola Luigi Bragazzi, Dennis McGonagle, Giovanni Damiani, Doron Comaneshter, Arnon Cohen, and Howard Amital. 2019. "Systemic Sclerosis Is Linked to Psoriasis and May Impact on Patients’ Survival: A Large Cohort Study" Journal of Clinical Medicine 8, no. 4: 521. https://doi.org/10.3390/jcm8040521