Daylight Saving Time and Acute Myocardial Infarction: A Meta-Analysis

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
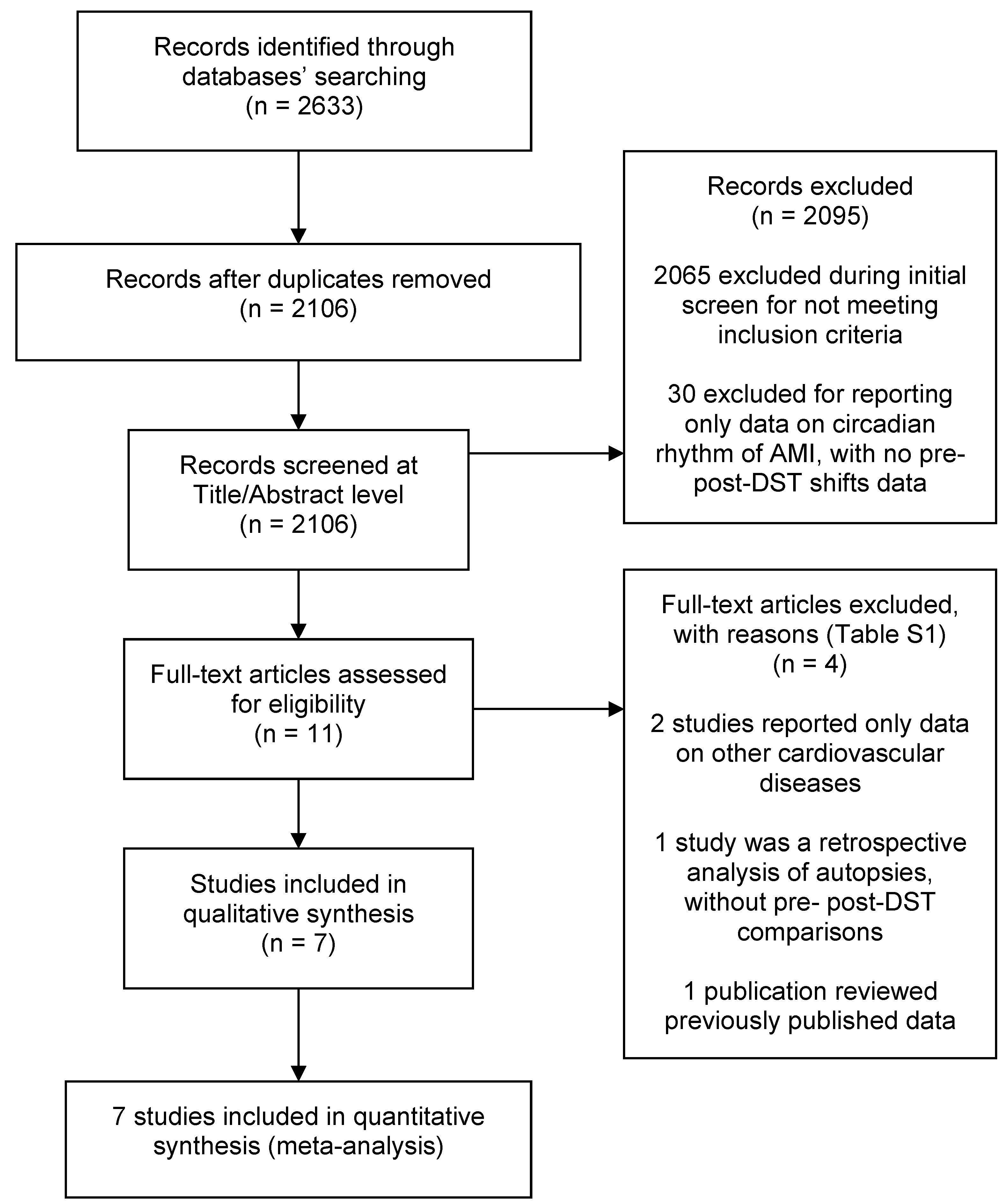
2.1. Bibliographic Search, Study Selection Criteria and Quality Assessment
2.2. Data Analysis
3. Results
3.1. Characteristics of the Included Studies and Methodological Quality
3.2. Overall Meta-Analysis: One Week after Both Spring and Autumn DST Transitions versus Control Weeks
3.3. One-Week Post-Spring Shift to DST versus Control Weeks
3.4. One-Week Post Autumn Shift from DST versus Control Weeks
3.5. Small Study Effects (Publication Bias)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dibner, C.; Schibler, U. Body clocks: Time for the Nobel Prize. Acta Physiol. 2018, 222. [Google Scholar] [CrossRef] [PubMed]
- Vinciguerra, M.; Tevy, M.F.; Mazzoccoli, G. A ticking clock links metabolic pathways and organ systems function in health and disease. Clin. Exp. Med. 2014, 14, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Meira, E.C.M.; Acuna-Castroviejo, D. Cardiometabolic impact of changing internal time during daylight saving time: A window for a deleterious role within sleep-related breathing disorders. Intern. Emerg. Med. 2018, 13, 1345–1346. [Google Scholar] [CrossRef] [PubMed]
- Herzig, K.H. Circadian rhythms-Daylight saving time, health and body clocks. Acta Physiol. 2019, 225, e13221. [Google Scholar] [CrossRef]
- Manfredini, R.; Manfredini, F.; Fersini, C.; Conconi, F. Circadian rhythms, athletic performance and jet lag. Br. J. Sports Med. 1998, 32, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Vitale, J.; Manfredini, R.; Gallerani, M.; Mumoli, N.; Eagle, K.A.; Ageno, W.; Dentali, F. Chronobiology of acute aortic rupture or dissection: A systematic review and a meta-analysis of the literature. Chronobiol. Int. 2015, 32, 385–394. [Google Scholar] [CrossRef]
- Elliott, W.J. Circadian variation in the timing of stroke onset: A meta-analysis. Stroke 1998, 29, 992–996. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.C.; Rohtla, K.M.; Lavery, C.E.; Muller, J.E.; Mittleman, M.A. Meta-analysis of the morning excess of acute myocardial infarction and sudden cardiac death. Am. J. Cardiol. 1997, 79, 1512–1516. [Google Scholar] [CrossRef]
- Dentali, F.; Ageno, W.; Rancan, E.; Donati, A.V.; Galli, L.; Squizzato, A.; Venco, A.; Mannucci, P.M.; Manfredini, R. Seasonal and monthly variability in the incidence of venous thromboembolism. A systematic review and a meta-analysis of the literature. Thromb. Haemost. 2011, 106, 439–447. [Google Scholar]
- Meira, E.C.M.; Miyazawa, M.; Manfredini, R.; Cardinali, D.; Madrid, J.A.; Reiter, R.; Araujo, J.F.; Agostinho, R.; Acuna-Castroviejo, D. Impact of Daylight Saving Time on circadian timing system: An expert statement. Eur. J. Intern. Med. 2019, 60, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Lindenberger, L.M.; Ackermann, H.; Parzeller, M. The controversial debate about daylight saving time (DST)-results of a retrospective forensic autopsy study in Frankfurt/Main (Germany) over 10 years (2006–2015). Int. J. Legal Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 31 December 2018).
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [Updated March 2011]; Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: Chichester, West Sussex, UK, 2011. [Google Scholar]
- Manzoli, L.; De Vito, C.; Marzuillo, C.; Boccia, A.; Villari, P. Oral contraceptives and venous thromboembolism: A systematic review and meta-analysis. Drug Saf. 2012, 35, 191–205. [Google Scholar] [CrossRef]
- Sterne, J.A.; Egger, M.; Smith, G.D. Systematic reviews in health care: Investigating and dealing with publication and other biases in meta-analysis. BMJ 2001, 323, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirchberger, I.; Wolf, K.; Heier, M.; Kuch, B.; von Scheidt, W.; Peters, A.; Meisinger, C. Are daylight saving time transitions associated with changes in myocardial infarction incidence? Results from the German MONICA/KORA Myocardial Infarction Registry. BMC Public Health 2015, 15, 778. [Google Scholar] [CrossRef]
- Sipila, J.O.; Rautava, P.; Kyto, V. Association of daylight saving time transitions with incidence and in-hospital mortality of myocardial infarction in Finland. Ann. Med. 2016, 48, 10–16. [Google Scholar] [CrossRef]
- Janszky, I.; Ahnve, S.; Ljung, R.; Mukamal, K.J.; Gautam, S.; Wallentin, L.; Stenestrand, U. Daylight saving time shifts and incidence of acute myocardial infarction—Swedish Register of Information and Knowledge About Swedish Heart Intensive Care Admissions (RIKS-HIA). Sleep Med. 2012, 13, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Culic, V. Daylight saving time transitions and acute myocardial infarction. Chronobiol. Int. 2013, 30, 662–668. [Google Scholar] [CrossRef]
- Sandhu, A.; Seth, M.; Gurm, H.S. Daylight savings time and myocardial infarction. Open Heart 2014, 1, e000019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiddou, M.R.; Pica, M.; Boura, J.; Qu, L.; Franklin, B.A. Incidence of myocardial infarction with shifts to and from daylight savings time. Am. J. Cardiol. 2013, 111, 631–635. [Google Scholar] [CrossRef]
- Janszky, I.; Ljung, R. Shifts to and from daylight saving time and incidence of myocardial infarction. N. Engl. J. Med. 2008, 359, 1966–1968. [Google Scholar] [CrossRef] [PubMed]
- Lahti, T.A.; Leppamaki, S.; Ojanen, S.M.; Haukka, J.; Tuulio-Henriksson, A.; Lonnqvist, J.; Partonen, T. Transition into daylight saving time influences the fragmentation of the rest-activity cycle. J. Circadian Rhythms 2006, 4, 1. [Google Scholar] [CrossRef]
- Spiegel, K.; Leproult, R.; Van Cauter, E. Impact of sleep debt on metabolic and endocrine function. Lancet 1999, 354, 1435–1439. [Google Scholar] [CrossRef]
- Cheng, T.O. Effect of sleep deprivation on cardiovascular health. Int. J. Cardiol. 2009, 134, 293–294. [Google Scholar] [CrossRef]
- Manfredini, R.; Fabbian, F.; De Giorgi, A.; Zucchi, B.; Cappadona, R.; Signani, F.; Katsiki, N.; Mikhailidis, D.P. Daylight saving time and myocardial infarction: Should we be worried? A review of the evidence. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 750–755. [Google Scholar] [PubMed]
- Manfredini, R.; Fabbian, F.; Cappadona, R.; Modesti, P.A. Daylight saving time, circadian rhythms and cardiovascular health. Intern. Emerg. Med. 2018, 13, 641–646. [Google Scholar] [CrossRef]
- Monk, T.H.; Folkard, S. Adjusting to the changes to and from Daylight Saving Time. Nature 1976, 261, 688–689. [Google Scholar] [CrossRef]
- Kantermann, T.; Juda, M.; Merrow, M.; Roenneberg, T. The human circadian clock’s seasonal adjustment is disrupted by daylight saving time. Curr. Biol. 2007, 17, 1996–2000. [Google Scholar] [CrossRef]
- Tonetti, L.; Erbacci, A.; Fabbri, M.; Martoni, M.; Natale, V. Effects of transitions into and out of daylight saving time on the quality of the sleep/wake cycle: An actigraphic study in healthy university students. Chronobiol. Int. 2013, 30, 1218–1222. [Google Scholar] [CrossRef] [PubMed]
- Lahti, T.A.; Leppamaki, S.; Lonnqvist, J.; Partonen, T. Transition to daylight saving time reduces sleep duration plus sleep efficiency of the deprived sleep. Neurosci. Lett. 2006, 406, 174–177. [Google Scholar] [CrossRef] [PubMed]
- Barnes, C.M.; Wagner, D.T. Changing to daylight saving time cuts into sleep and increases workplace injuries. J. Appl. Psychol. 2009, 94, 1305–1317. [Google Scholar] [CrossRef] [PubMed]
- Harrison, Y. The impact of daylight saving time on sleep and related behaviours. Sleep Med. Rev. 2013, 17, 285–292. [Google Scholar] [CrossRef]
- Miguel, M.; Oliveira, V.C.; Pereira, D.; Pedrazzoli, M. Detecting chronotype differences associated to latitude: A comparison between Horne–Ostberg and Munich Chronotype questionnaires. Ann. Hum. Biol. 2014, 41, 105–108. [Google Scholar] [CrossRef]
- Sipila, J.O.; Ruuskanen, J.O.; Rautava, P.; Kyto, V. Changes in ischemic stroke occurrence following daylight saving time transitions. Sleep Med. 2016, 27-28, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Havranek, T.; Herman, D.; Irsova, Z. Does Daylight Saving Save Energy? A Meta-Analysis; IES Working Paper 24/2016; Institute of Economic Studies, Faculty of Social Sciences Charles University: Prague, Czech Republic, 2016. [Google Scholar]
- Lahti, T.A.; Haukka, J.; Lonnqvist, J.; Partonen, T. Daylight saving time transitions and hospital treatments due to accidents or manic episodes. BMC Public Health 2008, 8, 74. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, C.M.; Blake, F.; Fossey, E.; Adams, B. Daylight saving time in psychiatric illness. J. Affect. Disord. 1990, 19, 177–181. [Google Scholar] [CrossRef]
- Laszlo, K.D.; Cnattingius, S.; Janszky, I. Transition into and out of daylight saving time and spontaneous delivery: A population-based study. BMJ Open 2016, 6, e010925. [Google Scholar] [CrossRef] [PubMed]
- Coren, S. Daylight savings time and traffic accidents. N. Engl. J. Med. 1996, 334, 924–925. [Google Scholar] [CrossRef]
- Ellis, D.A.; Luther, K.; Jenkins, R. Missed medical appointments during shifts to and from daylight saving time. Chronobiol. Int. 2018, 35, 584–588. [Google Scholar] [CrossRef]
- Pizzi, C.; Xhyheri, B.; Costa, G.M.; Faustino, M.; Flacco, M.E.; Gualano, M.R.; Fragassi, G.; Grigioni, F.; Manzoli, L. Nonobstructive Versus Obstructive Coronary Artery Disease in Acute Coronary Syndrome: A Meta-Analysis. J. Am. Heart Assoc. 2016, 5, e004185. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| First Author | Year | Country | Study Years | Data Source | Total Sample (Males) | Mean Age in Years (SD) |
|---|---|---|---|---|---|---|
| Janszky [23] | 2008 | Sweden | 1987–2006 | Swedish Registry of Acute Myocardial Infarction (no further detail provided) | >24,000 * (NR) | NR |
| Janszky [19] | 2012 | Sweden | 1995–2007 | Register of Information and Knowledge about Swedish Heart Intensive Care Admission (RIKS-HIA), including all patients with a diagnosis of AMI admitted to the Coronary care Units of 74 Swedish hospitals | >7300 * (>4650) | NR |
| Culic [20] | 2013 | Croatia | 1990–1996 | Hospital Discharge Abstracts of all patients with a primary diagnosis of AMI discharged from the Split University Hospital | 2412 (1666) | 64.1 (11.9) |
| Jiddou [22] | 2013 | USA | 2006–2012 | Hospital Discharge Abstracts of all patients with a primary diagnosis of AMI discharged from the Royal Oak and Troy Campuses of Beaumont Hospitals (Michigan) | 935 (551) | 70.0 (14.8) |
| Sandhu [21] | 2014 | USA | 2010–2013 | Blue Cross Blue Shield of Michigan Cardiovascular Consortium (BMC2) Database, including all Michigan residents with a diagnosis of AMI undergoing a PCI | 42,060 (NR) | NR |
| Kirchberger [17] | 2015 | Germany | 1985–2010 | MONICA-KORA Myocardial Infarction Registry, including all residents in the County of Augsburg with a diagnosis of AMI, discharged from the Klinikum Augsburg Hospital (80%) or from minor County hospitals | 25,499 (18,524) | 62.6 (9.2) |
| Sipilä [18] | 2015 | Finland | 2001–2009 | Hospital Discharge Abstracts of all patients with a primary diagnosis of AMI (ICD-10 code 121x), discharged from one of the 22 Finnish hospitals with a coronary catheterization lab and treating emergency cardiac patients | 14,459 (8748) | 71.2 (12.8) |
| Selection (Max Score 4) | Comparability (Max Score 2) | Outcome (Max Score 3) | |
|---|---|---|---|
| Janszky [23] | 4 | 0 | 3 |
| Janszky [19] | 4 | 0 | 3 |
| Culic [20] | 4 | 0 | 3 |
| Jiddou [22] | 4 | 1 | 3 |
| Sandhu [21] | 4 | 1 | 3 |
| Kirchberger [17] | 4 | 2 | 3 |
| Sipilä [18] | 4 | 1 | 3 |
| Variables | N. of Datasets ** (Sample) ϕ | AMI Risk OR (95% CI) | p-Value | I2, % |
|---|---|---|---|---|
| 1-week post-spring and autumn DST transitions vs. control weeks | ||||
| Overall [17,18,19,20,21,22,23] | 14 (116,675) | 1.03 (1.01–1.06) | 0.01 | 67 |
| Females only [17,19,20] | 6 (10,382) | 1.02 (0.95–1.09) | 0.6 | 41 |
| Males only [17,18,19,20] | 8 (33,587) | 1.02 (0.98–1.06) | 0.3 | 25 |
| Age < 65 years only [17,19] | 4 (15,525) | 1.01 (0.97–1.05) | 0.6 | 0 |
| Age ≥ 65 years only [17,19] | 4 (17,284) | 1.03 (0.97–1.08) | 0.3 | 64 |
| Spring shift—1-week post-transition to DST vs. control weeks | ||||
| Overall [17,18,19,20,21,22,23] | 7 | 1.05 (1.02–1.07) | <0.001 | 24 |
| Females only [17,19,20] | 3 | 1.02 (0.88–1.18) | 0.8 | 46 |
| Males only [17,18,19,20] | 4 | 1.06 (0.97–1.15) | 0.2 | 49 |
| Age < 65 years only [17,19] | 2 | 1.01 (0.96–1.07) | 0.9 | 68 |
| Age ≥ 65 years only [17,19] | 2 | 1.07 (1.00–1.14) | 0.06 | 25 |
| Autumn shift—1-week post-transition from DST vs. control weeks | ||||
| Overall | 7 | 1.01 (0.98–1.04) | 0.7 | 49 |
| Females only [17,19,20] | 3 | 0.99 (0.94–1.04) | 0.8 | 0 |
| Males only [17,18,19,20] | 4 | 1.00 (0.97–1.04) | 0.9 | 0 |
| Age < 65 years only [17,19] | 2 | 1.01 (0.96–1.06) | 0.7 | 0 |
| Age ≥ 65 years only [17,19] | 2 | 0.99 (0.96–1.02) | 0.5 | 0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manfredini, R.; Fabbian, F.; Cappadona, R.; De Giorgi, A.; Bravi, F.; Carradori, T.; Flacco, M.E.; Manzoli, L. Daylight Saving Time and Acute Myocardial Infarction: A Meta-Analysis. J. Clin. Med. 2019, 8, 404. https://doi.org/10.3390/jcm8030404
Manfredini R, Fabbian F, Cappadona R, De Giorgi A, Bravi F, Carradori T, Flacco ME, Manzoli L. Daylight Saving Time and Acute Myocardial Infarction: A Meta-Analysis. Journal of Clinical Medicine. 2019; 8(3):404. https://doi.org/10.3390/jcm8030404
Chicago/Turabian StyleManfredini, Roberto, Fabio Fabbian, Rosaria Cappadona, Alfredo De Giorgi, Francesca Bravi, Tiziano Carradori, Maria Elena Flacco, and Lamberto Manzoli. 2019. "Daylight Saving Time and Acute Myocardial Infarction: A Meta-Analysis" Journal of Clinical Medicine 8, no. 3: 404. https://doi.org/10.3390/jcm8030404