Risk Factors for Same Pathogen Sepsis Readmission Following Hospitalization for Septic Shock


Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Study Population
2.2. Data collection and Definition
2.3. Statistical Analyses
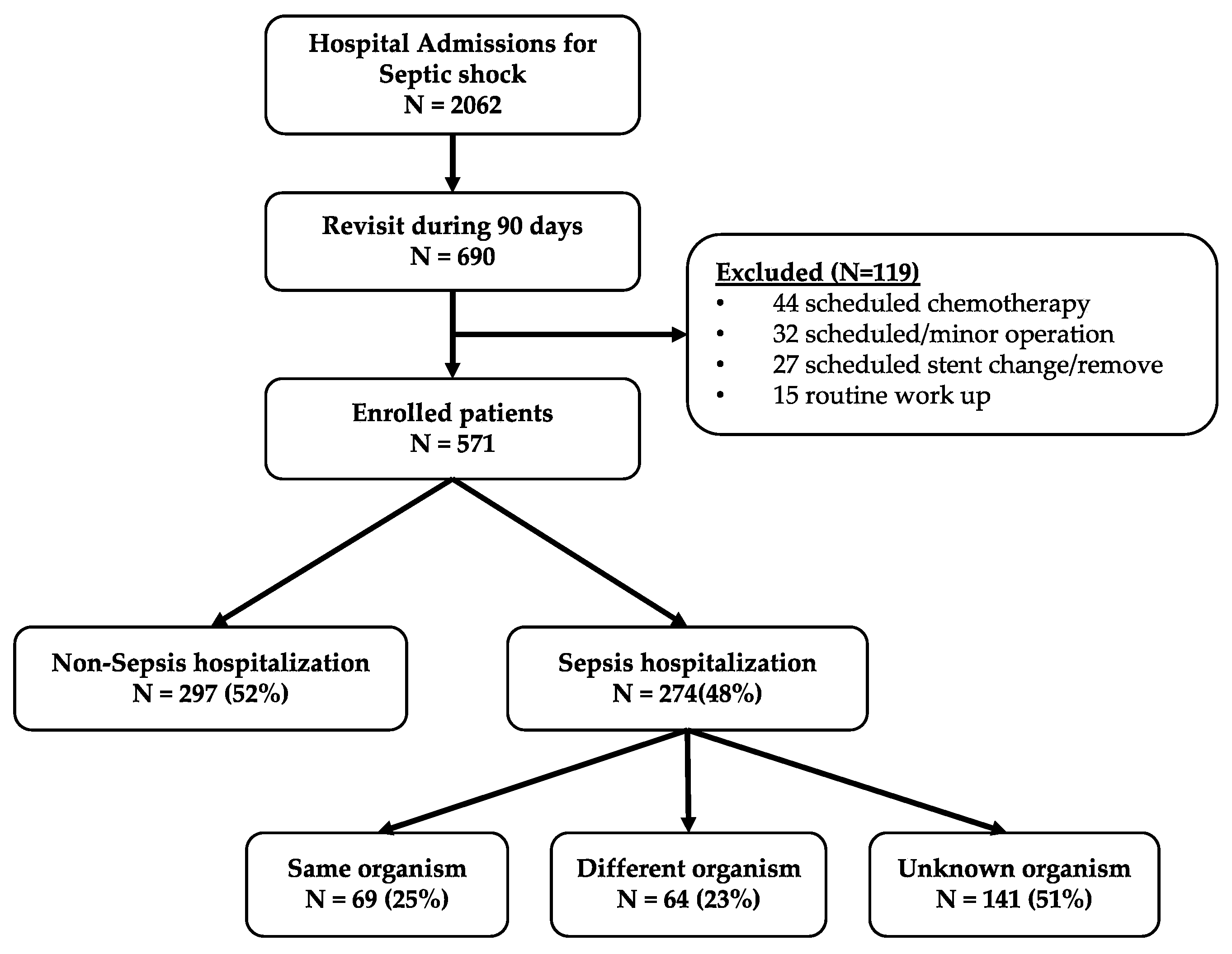
3. Results
3.1. Baseline Characteristics
3.2. Etiology of Recurrent Sepsis
3.3. Risk Factors Independently Associated with Sepsis due to the Same Organism
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Lagu, T.; Rothberg, M.B.; Shieh, M.-S.; Pekow, P.S.; Steingrub, J.S.; Lindenauer, P.K. Hospitalizations, costs and outcomes of severe sepsis in the United States 2003 to 2007. Criti. Care Med. 2012, 40, 754–761. [Google Scholar] [CrossRef] [PubMed]
- Meyer, N.; Harhay, M.O.; Small, D.S.; Prescott, H.C.; Bowles, K.H.; Gaieski, D.F.; Mikkelsen, M.E. Temporal trends in incidence, sepsis-related mortality and hospital-based acute care after sepsis. Criti. Care Med. 2018, 46, 354–360. [Google Scholar]
- Fujishima, S. Organ dysfunction as a new standard for defining sepsis. Inflamm. Regen. 2016, 36, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kaukonen, K.-M.; Bailey, M.; Suzuki, S.; Pilcher, D.; Bellomo, R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000–2012. JAMA 2014, 311, 1308–1309. [Google Scholar] [CrossRef]
- Wang, T.; Derhovanessian, A.; de Cruz, S.; Belperio, J.A.; Deng, J.C.; Hoo, G.S. Subsequent infections in survivors of sepsis. J. Intensive Care Med. 2012, 29, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.Y.; Kumar, A. Empiric antimicrobial therapy in severe sepsis and septic shock: Optimizing pathogen clearance. Curr. Infect. Dis. Rep. 2015, 17, 1123–1167. [Google Scholar] [CrossRef]
- Alsina, L.; Basteiro, M.G.; de Paz, H.D.; Iñigo, M.; de Sevilla, M.F.; Triviño, M.; Juan, M.; Muñoz-Almagro, C. Recurrent invasive pneumococcal disease in children: Underlying clinical conditions and immunological and microbiological characteristics. PLoS ONE 2015, 10, e0118848. [Google Scholar] [CrossRef] [PubMed]
- Yum, H.-K.; Park, I.-N.; Shin, B.-M.; Choi, S.-J. Recurrent pseudomonas aeruginosaInfection in chronic lung diseases: Relapse or reinfection? Tuberc. Respir. Dis. 2014, 77, 172–176. [Google Scholar] [CrossRef]
- Kethireddy, S.; Bilgili, B.; Sees, A.; Kirchner, H.L.; Ofoma, U.R.; Light, R.B.; Mirzanejad, Y.; Maki, D.; Kumar, A.; Layon, A.J.; et al. Culture-negative septic shock compared with culture-positive septic shock. Crit. Care Med. 2018, 46, 506–512. [Google Scholar]
- Levy, M.M.; Fink, M.P.; Marshall, J.C.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.M.; Vincent, J.-L.; Ramsay, G. 2001 SCCM/ESICM/ACCP/ATS/SIS International sepsis definitions conference. Crit. Care Med. 2003, 31, 1250–1256. [Google Scholar] [CrossRef]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Mirrett, S.; Reller, L.B.; Weinstein, M.P. Detection of bloodstream infections in adults: How many blood cultures are needed? J. Clin. Microbiol. 2007, 45, 3546–3548. [Google Scholar] [CrossRef] [PubMed]
- Prescott, H.C.; Langa, K.M.; Liu, V.; Escobar, G.J.; Iwashyna, T.J. Increased 1-year healthcare use in survivors of severe sepsis. Am. J. Respir. Crit. Care Med. 2014, 190, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Ortego, A.; Gaieski, D.F.; Fuchs, B.D.; Jones, T.; Halpern, S.D.; Small, D.S.; Sante, S.C.; Drumheller, B.; Christie, J.D.; Mikkelsen, M.E. Hospital-based acute care use in survivors of septic shock. Crit. Care Med. 2015, 43, 729–737. [Google Scholar] [CrossRef]
- Sun, A.; Netzer, G.; Small, D.S.; Hanish, A.; Fuchs, B.D.; Gaieski, D.F.; Mikkelsen, M.E. Association between index hospitalization and hospital readmission in sepsis survivors. Crit. Care Med. 2016, 44, 478–487. [Google Scholar] [CrossRef]
- DeMerle, K.M.; Royer, S.C.; Mikkelsen, M.E.; Prescott, H.C. Readmissions for recurrent sepsis. Crit. Care Med. 2017, 45, 1702–1708. [Google Scholar] [CrossRef] [PubMed]
- Hotchkiss, R.S.; Monneret, G.; Payen, D. Sepsis-induced immunosuppression: From cellular dysfunctions to immunotherapy. Nat. Rev. Immunol. 2013, 13, 862–874. [Google Scholar] [CrossRef]
- Delano, M.J.; Ward, P.A. Sepsis-induced immune dysfunction: Can immune therapies reduce mortality? J. Clin. Investig. 2016, 126, 23–31. [Google Scholar] [CrossRef]
- Franco, A.V.M. Recurrent urinary tract infections. Best Pract. Res. Clin. Obstet. Gynaecol. 2005, 19, 861–873. [Google Scholar] [CrossRef]
- Agarwal, M.; Shiau, S.; Larson, E.L. Repeat gram-negative hospital-acquired infections and antibiotic susceptibility: A systematic review. J. Infect. Public Health 2017, 11, 455–462. [Google Scholar] [CrossRef]
- Lupp, C.; Robertson, M.L.; Wickham, M.E.; Sekirov, I.; Champion, O.L.; Gaynor, E.C.; Finlay, B.B. Host-mediated inflammation disrupts the intestinal microbiota and promotes the overgrowth of Enterobacteriaceae. Cell Host Microbe. 2007, 2, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Honda, K.; Littman, D.R. The microbiome in infectious disease and inflammation. Annu. Rev. Immunol. 2012, 30, 759–795. [Google Scholar] [CrossRef] [PubMed]
- Robert, P.D. The microbiome and critical illness. Lancet Respir. 2015, 4, 59–72. [Google Scholar]


{kind=link}
| Characteristics | Sepsis due to a Different Organism n = 64 | Sepsis due to Unknown Organism n = 141 | Sepsis due to the Same Organism n = 69 | p-Value |
|---|---|---|---|---|
| Age | 65 (59–72) | 54 (57–71) | 64 (68–72) | 0.215 |
| Male | 38 (59.3) | 92 (65.2) | 31 (44.9) | 0.027 |
| Hypertension | 22 (34.4) | 46 (32.6) | 31 (44.9) | 0.308 |
| Stroke | 7 (10.9) | 15 (10.6) | 2 (2.9) | 0.299 |
| Diabetes | 18 (28.1) | 39 (27.7) | 19 (27.5) | 1.000 |
| Coronary artery disease | 11 (17.2) | 19 (13.5) | 5 (7.2) | 0.478 |
| Chronic pulmonary disease | 13 (20.3) | 37 (26.2) | 13 (18.8) | 0.357 |
| Chronic renal failure | 4 (6.3) | 8 (5.7) | 7 (10.1) | 0.055 |
| Liver cirrhosis | 8 (12.5) | 25 (17.7) | 18 (26.1) | 0.738 |
| Malignancy | 49 (76.6) | 116 (82.3) | 58 (84.1) | 0.898 |
| 28 d mortality | 2 (3.1) | 3 (2.1) | 1 (1.4) | 1.000 |
| 90 d mortality | 3 (4.7) | 8 (5.7) | 5 (7.2) | 0.839 |
| Mechanical ventilation | 6 (9.4) | 6 (4.3) | 2 (2.9) | 0.299 |
| ICU stay | 0 (0–3) | 0 (0–2) | 0 (0–3) | 0.608 |
| Same site | 37 (57.8) | 98 (69.5) | 62 (89.9) | 0.001 |
| Characteristics | Total (%) n = 274 | Different Organism (%) n = 64 | Unknown Organism (%) n = 141 | Same Organism (%) n = 69 | p-Value |
|---|---|---|---|---|---|
| Organism | |||||
| Gram-positive | 34 (12.4) | 22 (34.3) | 10 (7.1) | 2 (2.9) | 0.001 |
| Gram-negative | 181 (65.8) | 46 (71.8) | 69 (48.9) | 66 (95.7) | <0.001 |
| Viral | 13 (4.7) | 3 (4.7) | 10 (7.1) | 0 (0.0) | 0.069 |
| Fungi | 4 (1.5) | 1 (1.6) | 2 (1.4) | 1 (1.4) | 1.000 |
| Site | |||||
| Urinary | 47 (17.1) | 13 (20.3) | 10 (7.1) | 24 (34.8) | <0.001 |
| Gastrointestinal | 43 (15.7) | 10 (15.6) | 17 (12.1) | 16 (23.2) | 0.153 |
| Hepatobiliary | 103 (37.6) | 22 (34.4) | 61 (43.3) | 20 (29.0) | 0.153 |
| Respiratory | 72 (26.3) | 25 (39.1) | 44 (31.2) | 3 (4.3) | 0.165 |
| Skin and soft tissue | 10 (3.6) | 4 (6.3) | 4 (2.8) | 2 (2.9) | 0.638 |
| Other | 29 (10.6) | 8 (12.5) | 15 (10.6) | 6 (8.7) | 0.061 |
| Type | Organisms | Frequency (%) |
|---|---|---|
| Blood | Staphylococcus aureus | 3 (8.1%) |
| Hemolytic streptococci | 1 (2.7%) | |
| Escherichia coli | 19 (51.4%) | |
| Klebsiella spp. | 6 (16.2%) | |
| Enterobacteriaceae | 2 (5.4%) | |
| Pseudomonas aeruginosa | 2 (5.4%) | |
| Other Gram-negatives | 2 (5.4%) | |
| Aspergillus spp. | 1 (2.7%) | |
| Candida albicans | 1 (2.7%) | |
| Urine | Staphylococcus aureus | 1 (2.7%) |
| Other Gram-positives | 1 (2.7%) | |
| Escherichia coli | 8 (21.6%) | |
| Enterobacteriaceae. | 2 (5.4%) | |
| Pneumococci urine Ag | 1 (2.7%) | |
| Sputum | β-hemolytic Streptococcus | 1 (2.7%) |
| Enterobacteriaceae | 1 (2.7%) | |
| Pseudomonas aeruginosa | 1 (2.7%) | |
| Acinetobacter baumannii | 2 (5.4%) | |
| Pus | Staphylococcus aureus | 1 (2.7%) |
| Escherichia coli | 4 (10.8%) | |
| Klebsiella spp. | 1 (2.7%) | |
| Stool | Enterococcus spp. | 1 (2.7%) |
| Enterobacteriaceae | 1 (2.7%) |
| Variables | Multivariate Analysis | ||
|---|---|---|---|
| OR | 95% CI | p-value | |
| Male | 0.589 | 0.295–1.176 | 0.133 |
| Same site | 6.894 | 2.390–19.886 | <0.001 |
| Gram-positive | 0.194 | 0.037–1.016 | 0.052 |
| Gram-negative | 9.902 | 2.843–34.489 | <0.001 |
| UTI | 4.331 | 1.723–10.882 | 0.002 |
| Respiratory | 0.312 | 0.086–1.133 | 0.077 |
| Variables | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | PLR | NLR |
|---|---|---|---|---|---|---|
| Same site | 89.86 (80.21–100.00) | 33.50 (30.00–40.00) | 31.16 (28.54–33.90) | 90.79 (82.64–95.33) | 1.35 (1.19–1.53) | 0.30 (0.15–0.63) |
| Gram-negative | 95.65 (87.82–100.00) | 44.17 (40.00–50.00) | 36.46 (33.48–39.56) | 96.81 (90.85–98.93) | 1.71 (1.50–1.95) | 0.10 (0.03–0.30) |
| UTI | 34.78 (23.71–40.00) | 88.83 (80.00–90.00) | 51.06 (38.69–63.30) | 80.26 (77.27–82.95) | 3.12 (1.88–5.15) | 0.73 (0.61–0.88) |
| Any of two factors | 24.64 (15.05–30.00) | 96.60 (80.00–100.00) | 70.83 (51.26–84.87) | 79.28 (76.94–81.45) | 7.25 (3.14–16.74) | 0.78 (0.68–0.89) |
| All three factors | 95.65 (87.82–100.00) | 55.34 (0.00–100.00) | 41.77 (37.94–45.71) | 97.44 (92.58–99.14) | 2.14 (1.82–2.51) | 0.08 (0.03–0.24) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-s.; Kim, Y.-J.; Ryoo, S.M.; Sohn, C.H.; Ahn, S.; Seo, D.W.; Lim, K.S.; Kim, W.Y. Risk Factors for Same Pathogen Sepsis Readmission Following Hospitalization for Septic Shock. J. Clin. Med. 2019, 8, 181. https://doi.org/10.3390/jcm8020181
Kim J-s, Kim Y-J, Ryoo SM, Sohn CH, Ahn S, Seo DW, Lim KS, Kim WY. Risk Factors for Same Pathogen Sepsis Readmission Following Hospitalization for Septic Shock. Journal of Clinical Medicine. 2019; 8(2):181. https://doi.org/10.3390/jcm8020181
Chicago/Turabian StyleKim, June-sung, Youn-Jung Kim, Seung Mok Ryoo, Chang Hwan Sohn, Shin Ahn, Dong Woo Seo, Kyoung Soo Lim, and Won Young Kim. 2019. "Risk Factors for Same Pathogen Sepsis Readmission Following Hospitalization for Septic Shock" Journal of Clinical Medicine 8, no. 2: 181. https://doi.org/10.3390/jcm8020181