Effects of Mind–Body Exercises (Tai Chi/Yoga) on Heart Rate Variability Parameters and Perceived Stress: A Systematic Review with Meta-Analysis of Randomized Controlled Trials

 , , ,
, , , 
Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Inclusion Criteria and Study Selection
2.3. Methodological Quality Assessment of Randomized Controlled Trials
2.4. Data Extraction and Analysis
3. Results
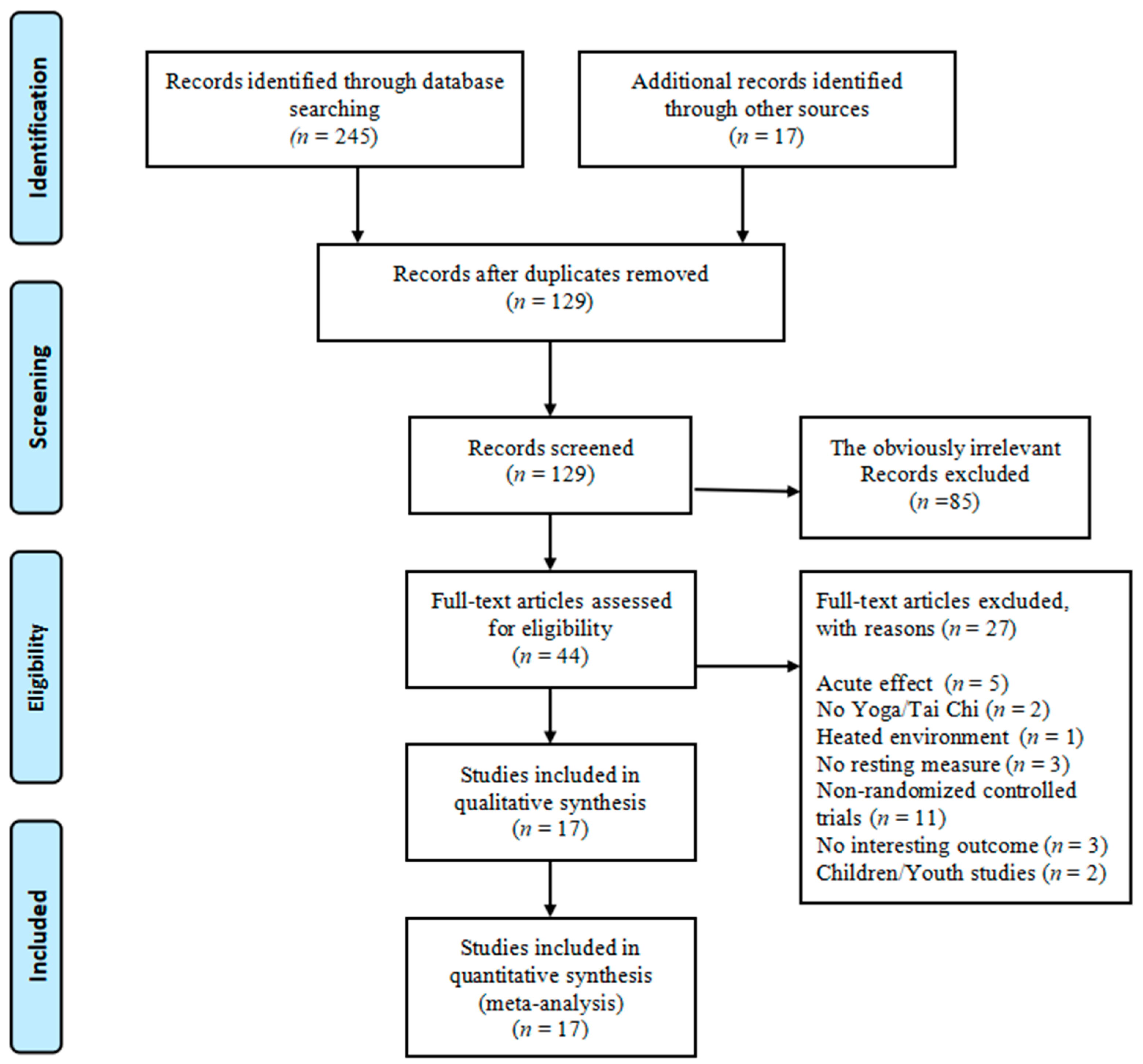
3.1. Eligible Study Selection
3.2. Study Characteristics
3.3. Methodological Quality of Randomized Controlled Trials
3.4. Effects of Mind–Body Exercises on Psycho-Physiological Parameters
4. Discussion
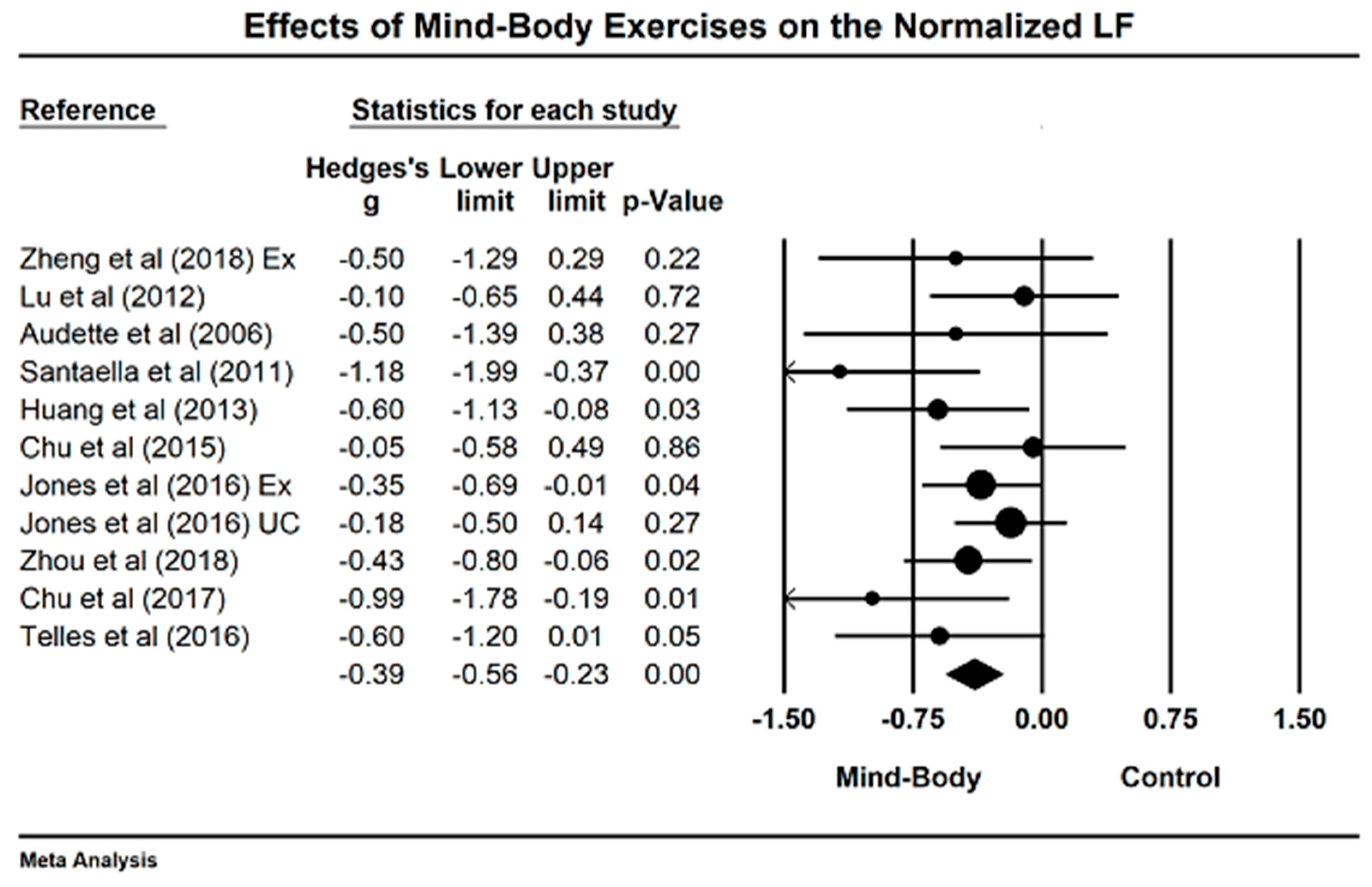
4.1. Effects of Mind–Body Exercises on Normalized Low-Frequency Power
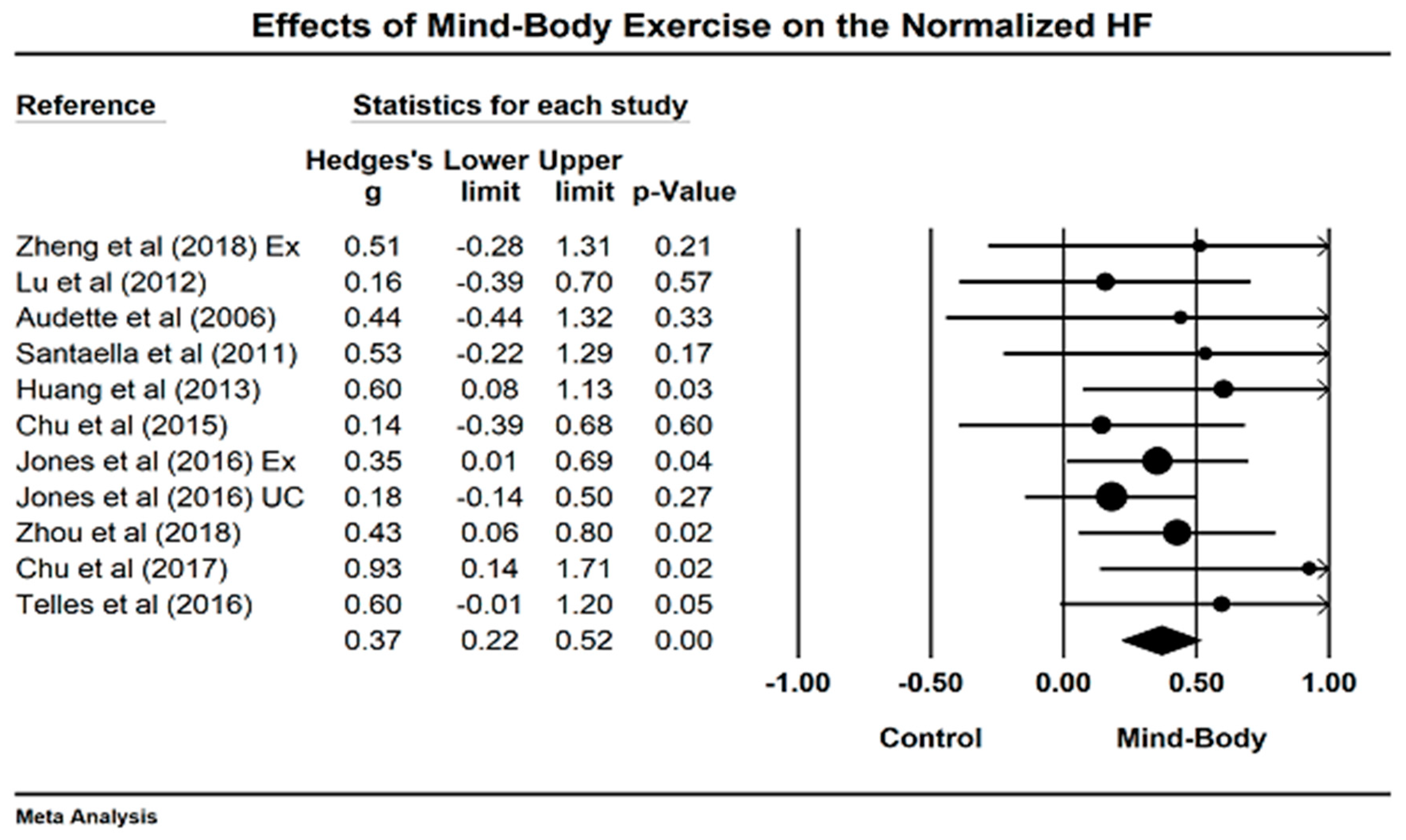
4.2. Effects of Mind–Body Exercises on Normalized High-Frequency Power
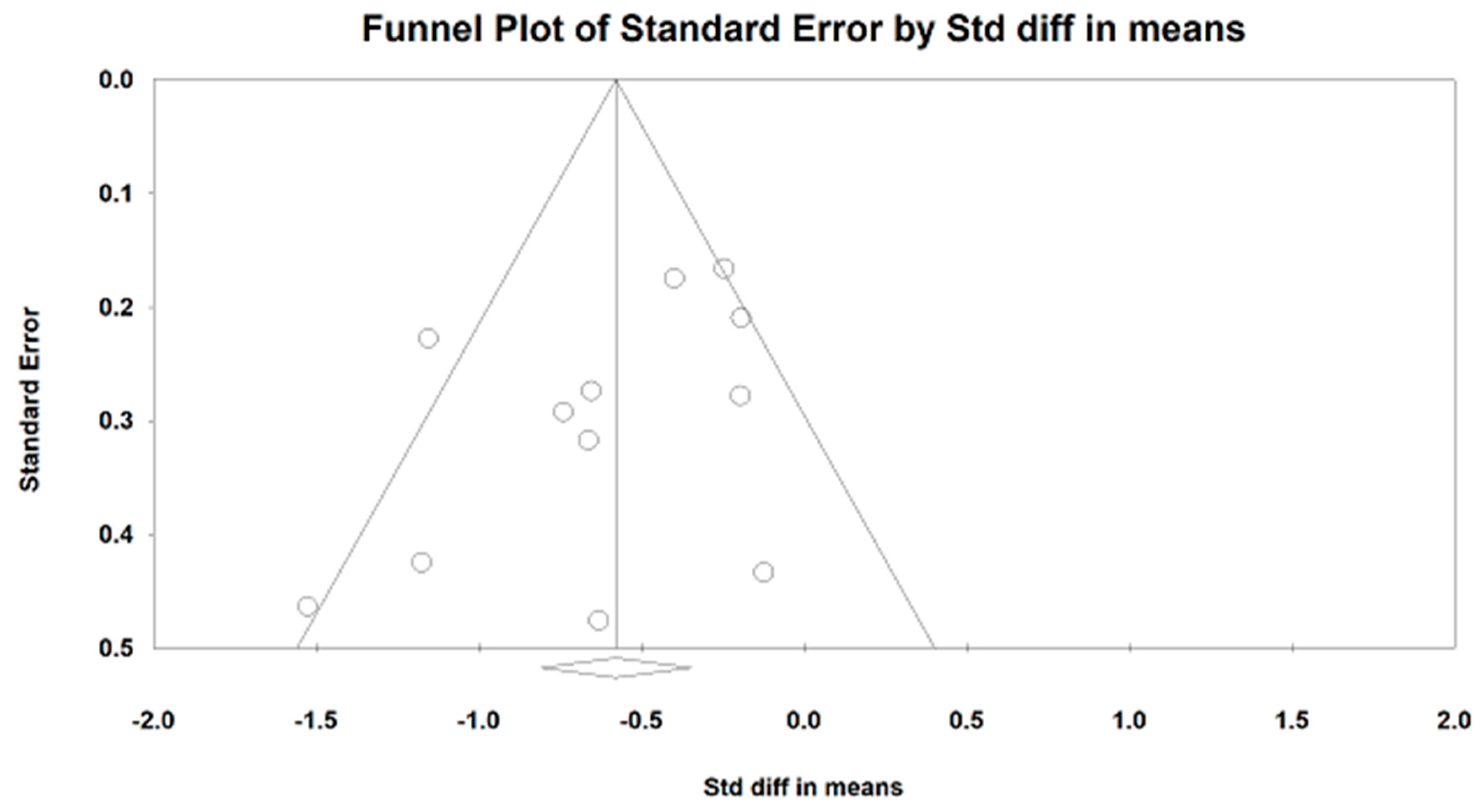
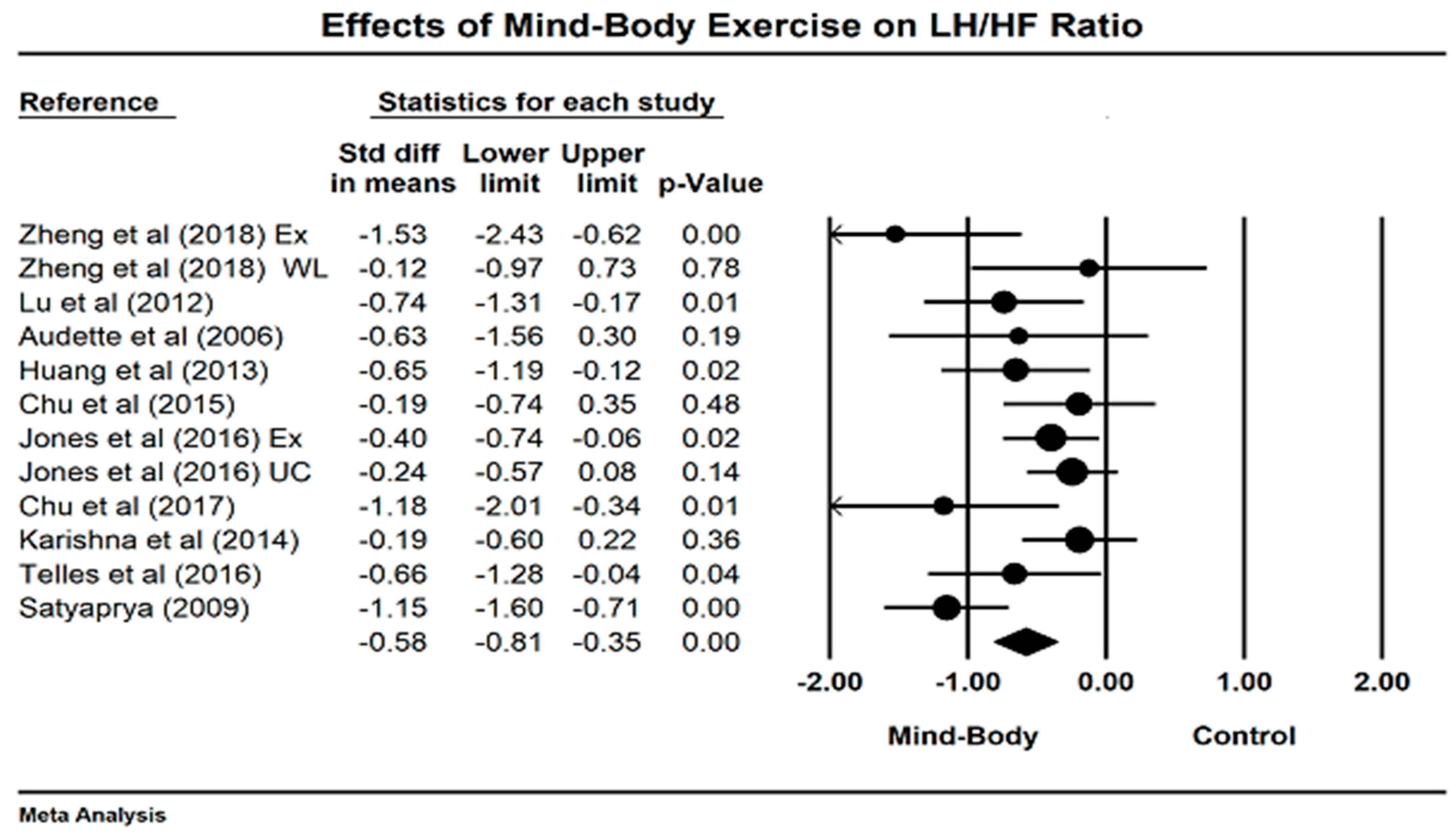
4.3. Effects of Mind–Body Exercises on LF/HF Ratio
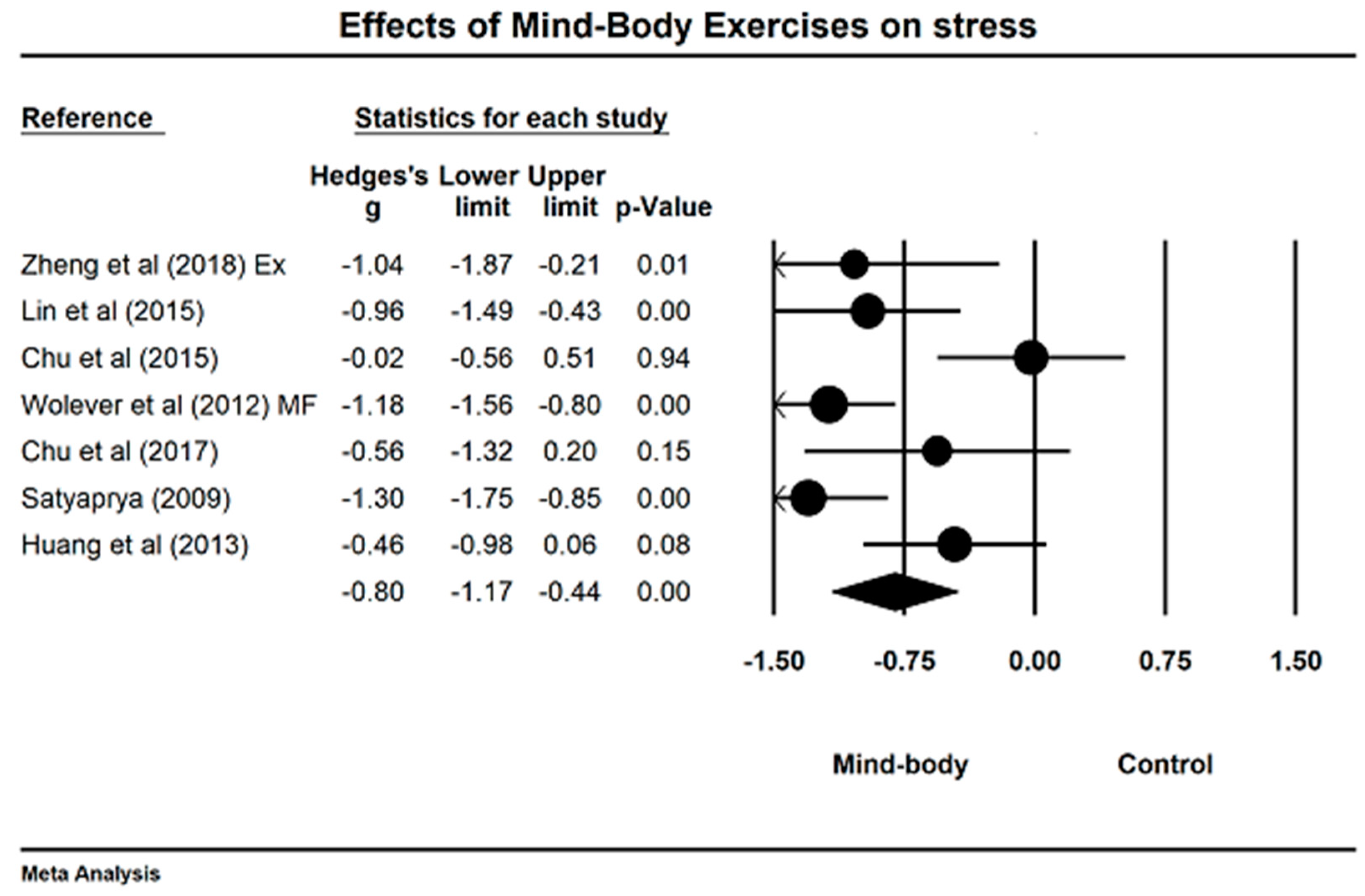
4.4. Effects of Mind–Body Exercises on Perceived Stress
4.5. Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tyagi, A.; Cohen, M. Yoga and heart rate variability: A comprehensive review of the literature. Int. J. Yoga 2016, 9, 97–113. [Google Scholar] [CrossRef] [PubMed]
- Sessa, F.; Anna, V.; Messina, G.; Cibelli, G.; Monda, V.; Marsala, G.; Ruberto, M.; Biondi, A.; Cascio, O.; Bertozzi, G.; et al. Heart rate variability as predictive factor for sudden cardiac death. Aging 2018, 10, 166–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Cheon, E.; Bai, D.; Lee, Y.; Koo, B. Stress and heart rate variability: A meta-analysis and review of literature. Psychiatry Investig. 2018, 15, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Jarczok, M.N.; Jarczok, M.; Mauss, D.; Koenig, J.; Li, J.; Herr, R.M.; Thayer, J.F. Autonomic nervous system activity and workplace stressors—A systematic review. Neurosci. Biobehav. Rev. 2013, 37, 1810–1823. [Google Scholar] [CrossRef] [PubMed]
- Oldehinkel, A.J.; Verhulst, F.C.; Ormel, J. Low heart rate: A marker of stress resilience. The TRAILS study. Biol. Psychiatry 2008, 63, 1141–1146. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.A.; Quitana, D.S.; Abbott, M.; Kemp, A. Anxiety disorders are associated with reduced heart rate variability: A meta-analaysis. Front. Psychiatry 2014, 4, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Negrão, C.E.; Moreira, E.D.; Santos, M.C.; Farah, V.M.; Krieger, E.M. Vagal function impairment after exercise training. J. Appl. Physiol. 1992, 72, 1749–1753. [Google Scholar] [CrossRef] [PubMed]
- ChuDuc, H.; NgyyenPhan, K.; Nguyen, V. A review of heart rate variability and its applications. APCBEE Procedia 2017, 7, 80–85. [Google Scholar] [CrossRef]
- Zou, L.; Wang, C.; Yeung, A.; Liu, Y.; Pan, Z. A Review Study on the beneficial effects of Baduanjin. J. Altern. Complement. Med. 2018, 24, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Li, T.; Lu, L. Effect of traditional Chinese mind-body exercise on disease activity, spinal mobility, and quality of life in patients with ankylosing spondylitis. Trav. Hum. 2017, 80, 1585–1597. [Google Scholar]
- Zou, L.; Wang, C.; Chen, X.; Wang, H. Baduanjin Exercise for Stroke Rehabilitation: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2018, 15, 600. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Sasaki, J.; Zeng, N.; Wang, C.; Sun, L. A Systematic Review with Meta-Analysis of Mindful Exercises on Rehabilitative Outcomes among post-stroke patients. Arch. Phys. Med. Rehabil. 2018, 99, 2355–2364. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Li, C.; Chiou, S.; Zeng, N.; Tzeng, H. Effects of mind-body movement on balance function in stroke survivors: A meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 2018, 15, 1292. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Chen, K.; Shu, Y.; Chen, X.; Luo, L.; Zhao, X. The Effect of Taichi Practice on Attenuating Bone Mineral Density Loss: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2017, 14, 1000. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Yu, D. Effect of a long-term modified Tai Chi-based intervention in attenuating bone mineral density in postmenopausal women in southeast China: Study protocol for a randomized controlled trial. Clin. Trials Degener. Dis. 2017, 2, 46–52. [Google Scholar]
- Zou, L.; Wang, C.; Tian, Z.; Wang, H.; Shu, Y. Effect of Yang-Style Tai Chi on Gait Parameters and Musculoskeletal Flexibility in Healthy Chinese Older Women. Sports 2017, 5, 52. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M.; Li, T.; Du, G.; Liu, Y. Tai chi for health benefits in patients with multiple sclerosis: A systematic review. PLoS ONE 2017, 12, e0170212. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; SasaKi, J.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M. A Systematic Review and Meta-Analysis Baduanjin Qigong for Health Benefits: Randomized Controlled Trials. Evid.-Based Complement. Altern. Med. 2017, 2017, 4548706. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Quan, X.; Wang, H. A Systematic review and Meta-analysis of Mindfulness-based (Baduanjin) exercise for alleviating musculoskeletal pain and improving sleep quality in people with chronic diseases. Int. J. Environ. Res. Public Health 2018, 15, 206. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Zeng, N.; Wang, C.; Sun, L.; Thomas, G.; Wang, H. Effects of Mind-Body Exercises for Mood and Functional Capabilities in Post-Stroke Patients: An Analytical Review of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2018, 15, 721. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Li, C.; Wei, G.X.; Chen, K.W.; Kinser, P.A.; Chan, J.S.; Ren, Z. Effects of Meditative Movements on Major Depressive Disorder: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2018, 7, 195. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Quan, X.; Hui, S.S.C.; Hu, X.; Chan, J.S.; Wang, C.; Boyden, S.D.; Sun, L.; Wang, H. Mindfulness-based Baduanjin exercise for depression and anxiety in people with physical or mental illnesses: A Systematic Review and Meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 2018, 15, 321. [Google Scholar] [CrossRef] [PubMed]
- Väänänen, J.; Xu, S.S.; Wang, S.; Laitinen, T.; Pekkarinen, H.; Länsimies, E. Taichiquan acutely increases heart rate variability. Clin. Physiol. Funct. Imaging 2002, 5, 2–3. [Google Scholar] [CrossRef]
- Lu, W.A.; Kuo, C.D. Breathing frequency-independent effect of Tai Chi Chuan on autonomic modulation. Clin. Auton. Res. 2014, 24, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.A.; Kuo, C.D. Comparison of the effects of Tai Chi Chuan and Wai Tan Kung exercises on autonomic nervous system modulation and on hemodynamics in elder adults. Am. J. Chin. Med. 2006, 34, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.A.; Kuo, C.D. The effect of Tai Chi Chuan on the autonomic nervous modulation in older persons. Med. Sci. Sports Exerc. 2003, 35, 1972–1976. [Google Scholar] [CrossRef] [PubMed]
- Kalsaria, P.; Li, H.; Waite, G.N.; Moga, M.M.; Kingsley, D.J.; Geib, R.W. Acute effects of tai chi exercise on cardiac autonomic function in healthy adults with tai chi experience. Biomed. Sci. Instrum. 2012, 48, 226–231. [Google Scholar] [PubMed]
- Chang, R.; Koo, M.; Yu, Z.; Kan, C.; Chu, I.; Hsu, C.; Chen, C. The effect of Tai Chi on autonomic nervous function of patients with coronary artery disease. J. Altern. Complement. Med. 2008, 14, 1107–1113. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Makita, S.; Uchida, R.; Ishihara, S.; Masuda, M. Effect of Tai Chi training on baroreflex sensitivity and heart rate variability in patients with coronary heart disease. Int. Heart J. 2010, 51, 238–241. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.; Lee, E.; Lee, M. Effects of Tai Chi on symptoms and quality of life in women with overactive bladder symptoms: A non-randomized clinical trials. Eur. J. Integr. Med. 2017, 12, 189–195. [Google Scholar] [CrossRef]
- Bidwell, A.; Yazel, B.; Davin, D.; Fairchild, T.; Kanaley, J. Yoga training improves quality of life in women with asthma. J. Altern. Complement. Med. 2012, 18, 749–755. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.C.; Harvey, D.J.; Shields, R.H.; Shields, G.S.; Rashedi, R.N.; Tancredi, D.J. Effects of Yoga on attention, impulsivity, and hyperactivity in preschool-aged children with attention-deficit hyperactivity disorder symptoms. J. Dev. Behav. Pediatr. 2018, 39, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Markil, N.; Whitehurst, M.; Jacobs, P.; Zoeller, R. Yoga Nidra relaxation increases heart rate variability and is unaffected by a prior bout of Hatha Yoga. J. Altern. Complement. Med. 2012, 18, 953–958. [Google Scholar] [CrossRef] [PubMed]
- Hewett, Z.; Pumpa, K.; Smith, C.; Fahey, P.; Cheema, B. Effect of a 16-week Bikram Yoga program on heart rate variability and associated cardiovascular disease risk factors in stressed and sedentary adults: A randomized controlled trials. BMC Complement. Altern. Med. 2017, 17, 226. [Google Scholar] [CrossRef] [PubMed]
- Cole, A.; Wijarnpreecha, K.; Chattipakorn, S.; Chattipakorn, N. Effects of Tai Chi exercise on heart rate variability. Complement. Ther. Clin. Pract. 2016, 23, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Posadzki, P.; Kuzdzal, A.; Lee, M.S.; Ernst, E. Yoga for Heart Rate Variability: A Systematic Review and Meta-analysis of Randomized Clinical Trials. Appl. Psychophys. Biofeedback 2015, 40, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.; Figueroa, A.; Sanchez-Gonzalez, M.A.; Son, W.M.; Chernykh, O.; Park, S.Y. Effectiveness of Tai Chi on Cardiac Autonomic Function and Symptomatology in Women with Fibromyalgia: A Randomized Controlled Trial. J. Aging Phys. Act. 2018, 26, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Michael, B.; Larry, V.H.; Julian, H.; Hannah, R.W. Introduction to Meta-Analysis; A John Wiley and Sons Ltd.: Chichester, UK, 2009. [Google Scholar]
- Zheng, S.; Kim, C.; Lal, S.; Meier, P.; Sibbritt, D.; Zaslawski, C. The Effects of Twelve Weeks of Tai Chi Practice on Anxiety in Stressed but Healthy People Compared to Exercise and Wait-List Groups-A Randomized Controlled Trial. J. Clin. Psychol. 2018, 74, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.A.; Kuo, C.D. Effect of 3-month Tai Chi Chuan on heart rate variability, blood lipid and cytokine profiles in middle-aged and elderly individuals. Int. J. Gerontol. 2012, 6, 267–272. [Google Scholar] [CrossRef]
- Audette, J.F.; Jin, Y.S.; Newcomer, R.; Stein, L.; Duncan, G.; Frontera, W.R. Tai Chi versus brisk walking in elderly women. Age Ageing 2006, 35, 388–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, S.L.; Huang, C.Y.; Shiu, S.P.; Yeh, S.H. Effects of yoga on stress, stress adaption, and heart rate variability among mental health professionals—A randomized controlled trial. World. Evid.-Based Nurs. 2015, 12, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Santaella, D.F.; Devesa, C.R.; Rojo, M.R.; Amato, M.B.; Drager, L.F.; Casali, K.R.; Montano, N. Yoga respiratory training improves respiratory function and cardiac sympathovagal balance in elderly subjects: A randomised controlled trial. BMJ Open 2011, 1, e000085. [Google Scholar] [CrossRef] [PubMed]
- Cheema, B.S.; Houridis, A.; Busch, L.; Raschke-Cheema, V.; Melville, G.W.; Marshall, P.W.; Chang, D.; Machliss, B.; Lonsdale, C.; Bowman, J.; et al. Effect of an office worksite-based yoga program on heart rate variability: Outcomes of a randomized controlled trial. BMC Complement. Altern. Med. 2013, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Chien, D.; Chung, U. Effects of Hatha Yoga on stress in middle-aged women. J. Nurs. Res. 2013, 21, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Chu, I.; Lin, Y.; Wu, W.; Chang, Y.; Lin, I. Effects of Yoga on heart rate variability and mood in women: A randomized controlled trial. J. Altern. Complement. Med. 2015, 21, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.M.; Guthrie, K.A.; Reed, S.D.; Landis, C.A.; Sternfeld, B.; LaCroix, A.Z. A yoga & exercise randomized controlled trial for vasomotor symptoms: Effects on heart ratevariability. Complement. Ther. Med. 2016, 26, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Wolever, R.Q.; Bobinet, K.J.; McCabe, K.; Mackenzie, E.R.; Fekete, E.; Kusnick, C.A.; Baime, M. Effective and viable mind-body stress reduction in the workplace: A randomized controlled trial. J. Occup. Health Psychol. 2012, 17, 246–258. [Google Scholar] [CrossRef] [PubMed]
- Satyapriya, M.; Nagendra, H.; Nagarathna, R.; Padmalatha, V. Effect of integrated yoga on stress and heart rate variability in pregnant women. Int. J. Cynecol. Obstet. 2009, 104, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Bowman, A.; Clayton, R.; Reed, A.; Subhan, M.; Ford, G. Effects of aerobic exercise training and yoga on the baroreflex in healthy elderly persons. Eur. J. Clin. Investig. 1997, 27, 443–449. [Google Scholar] [CrossRef]
- Zhou, W.; Wan, Y.H.; Chen, Q.; Qiu, Y.R.; Luo, X.M. Effects of Tai Chi Exercise on Cancer-Related Fatigue in Patients with Nasopharyngeal Carcinoma Undergoing Chemoradiotherapy: A Randomized Controlled Trial. J. Pain Symptom Manag. 2018, 55, 737–744. [Google Scholar] [CrossRef] [PubMed]
- Chu, I.H.; Wu, W.L.; Lin, I.M.; Chang, Y.K.; Lin, Y.J.; Yang, P.C. Effects of Yoga on Heart Rate Variability and Depressive Symptoms in Women: A Randomized Controlled Trial. J. Altern. Complement. Med. 2017, 23, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Krishna, B.H.; Pal, P.; Pal, G.K.; Balachander, J.; Jayasettiaseelon, E.; Seekanth, Y.; Sridhar, M.G.; Gaur, G.S. Effect of Yoga Therapy on Heart Rate, Blood Pressure and Cardiac Autonomic Function in Heart Failure. J. Clin. Diagn. Res. 2014, 8, 14–16. [Google Scholar] [CrossRef] [PubMed]
- Telles, S.; ShaRma, S.; Gupta, R.; Bhardwaj, A.; Balkrishna, A. Heart rate variability in chronic low back pain patients randomized to yoga or standard care. BMC Complement. Altern. Med. 2016, 16, 279. [Google Scholar] [CrossRef] [PubMed]
- Stauss, H.M. Heart rate variability. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2003, 285, 927–931. [Google Scholar] [CrossRef] [PubMed]
- Billman, G.E. The LF/HF Ratio does not accurately measure cardiac sympatho-vagal balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Participants | Duration (Weeks) | Intervention Protocol | Outcome Measured | Safety | |||
|---|---|---|---|---|---|---|---|---|
| Experiment | Control | Time-Domain or Frequency Domain | Detection Method (Position) | Period Length | AE | |||
| Zheng et al. (2018) [38] | Healthy but stressed people, Mean age: 33.9 N = 55(27.5%), 11 M; 49 F | 12 Weeks | 5 × 60 min/week, Tai Chi | C1: 5 × 60 min/week, Other Gym exercise; C2: waitlist | LF, HF, LF/HF ratio, nLF, nHF; stress (PSS) | ECG (siting) | 10 min | No |
| Lu et al. (2012) [39] | Middle-aged/elderly people, Mean age: 55 N = 50 (0%), 20 M; 30 F | 12 weeks | 7 × 40 min/week, Tai Chi | Unaltered lifestyle | LF, HF, LF/HF ratio, nLF, nHF | ECG (supine) | 10 min | No |
| Audette et al. (2006) [40] | Elderly women, Mean age: 71.4 N = 34 (20.5%), 0 M; 34 F | 12 weeks | 3 × 60 min/week, Tai Chi | 3 × 60 min/week, brisk walking | LF/HF ratio, nLF, nHF | ECG (NR) | 5 min | No |
| Wong et al. (2018) [41] | Women with fibromyalgia, Mean age: 51 N = 37 (16.2%), 0 M; 37 F | 12 weeks | 3 × 55 min/week, Tai Chi | Unaltered lifestyle | nLF, nHF | The SA-200E model (supine), 12 breaths/min | 5 min | No |
| Lin et al. (2015) [37] | Mental health professionals, Mean age: 30.92 N = 60 (0%), 12 M; 48 F | 12 weeks | 1 × 60 min/week, Yoga | Watching TV during a free tea time | LH, HF, LF/HF ratio, stress (the Chinese Version of Work-related Stress Scale) | HRV Monitor (NR) | NR | No |
| Santaella et al. (2011) [42] | Healthy elderly people, Mean age: 68 N = 30 (3.3%), 10 M; 19 F | 16 weeks | 2 × 30 min/week, Yoga | 2 × 30 min/week, Stretching | LF, HF, nLF, nHF | ECG (sitting) | 20 min | No |
| Cheema et al. (2013) [43] | university-based office employees Mean age: 38 N = 37 (8.1%), 7 M; 30 F | 10 weeks | 3 × 50 min/week, Hatha Yoga | Unaltered lifestyle | LnLF, LnHF, LnLH/LnHF ratio, Log RMSS, Log SDNN, PNN50 | The Sphygmocor system (supine) | 10 min | No |
| Huang et al. (2013) [44] | Female community residents Mean age: 45.8 N = 63 (1.6%), 0 M; 63 F | 8 weeks | 1 × 90 min/week, Yoga | Unaltered lifestyle | LF/HF ratio, nLF, nHF, Stress (PSS) | ECG (sitting) | 5 min | No |
| Chu et al. (2015) [45] | Healthy women, Mean age: 26.21 N = 52 (11.5%), 0 M; 52 F | 8 weeks | 2 × 60min/week, Yoga | Unaltered level of physical activity | LF/HF ratio, nLF, nHF, SDNN, stress (PSS) | ECG (supine) | 20 min | No |
| Jones et al. (2006) [46] | menopausal women Mean age:54.7 N = 355 (5.6%) 0M; 355 F | 12 weeks | 2 × 90 min/week + 20 min daily home practice, Yoga | C1: 3 × 40 min/week, other exercise C2: usual care | LH, HF, LF/HF ratio, nLF, nHF | ECG (sitting) | 15 min | No |
| Wolever et al. (2012) [47] | highly stressed employees Mean age:42.9 N = 239(9.5%), 56 M; 183F | 12 weeks | 1 × 60 min/week, Yoga | C1: 14-h training in total, mindfulness C2: unaltered lifestyle | HRV Coherence ratio, RR interval stress (PSS) | emWave Ear Sensor (sitting) | 10 min | No |
| Satyapriya et al. (2009) [48] | Pregnant women Mean age: 25.85 N = 122 (27.8%) 0 M; 122 F | 16 weeks | 3 × 120 min/week for Week 1 + 60min daily home practice for other 15 weeks (Yoga) | standard prenatal exercise | LF, HF, LF/HF ratio; stress (PSS) | ECG (NR) | 5 min | No |
| Bowman et al. (1997) [49] | Healthy sedentary elderly subjects Mean age: 68 N = 40 (35%), 23 M; 17 F | 6 weeks | 2 × 45 min/week, Yoga | 2 × 45 min/week, bicycle-base, aerobic training | HF | ECG (supine) | 20 min | No |
| Zhou et al. (2018) [50] | Patients with NPC, Age range: 18–70 N = 114 (27.2%), 83 M; 31 F | 19 weeks | 5 × 60 min/week, Tai Chi during chemordiotherapy | Usual care during chemordiotherapy | nLF, nHF, nLF/nHF ratio | ECG (supine) | 5 min | No |
| Chu et al. (2017) [51] | Sedentary women with depressive symptoms, Mean age: 32.7 N = 26 (23%), 0 M; 26 F | 12 weeks | 2 × 60 min/week, Yoga | Wait-list | nLF, nHF, LH/HF ratio, SDNN; stress (PPS) | ECG (supine) | 20 min | No |
| Karishna et al. (2014) [52] | Patients with CHF Mean age:49.8 N = 130 (29.2%), 64 M; 28 F | 12 weeks | 3 × 60 min/week, Yoga during standard medical therapy | Standard medical therapy | LF/HF ratio, nLF, nHF | ECG (supine) | 10 min | No |
| Telles et al. (2016) [53] | Patients with chronic low back Mean age: 35.6 N = 62 (46.8%), 32 M; 30 F | 12 weeks | 3 × 60 min/week for 2 weeks + daily home practice (10 weeks), Yoga | Standard care | LF/HF ratio, nLF, nHF, RMSSD | ECG (sitting) | 5 min | No |
| Reference | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Sum Scores |
|---|---|---|---|---|---|---|---|---|---|---|
| Zheng et al. (2018) [38] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 7 |
| Lu et al. (2012) [39] | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 6 |
| Audette et al. (2006) [40] | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 5 |
| Wong et al. (2018) [41] | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 6 |
| Lin et al. (2015) [37] | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Santaella et al. (2011) [42] | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 6 |
| Cheema et al. (2013) [43] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Huang et al. (2013) [44] | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 6 |
| Chu et al. (2015) [45] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Jones et al. (2016) [46] | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 7 |
| Wolever et al. (2012) [47] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| Satyaprya (2009) [48] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 7 |
| Bowman et al. (1997) [49] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 5 |
| Zhou et al. (2018) [50] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 7 |
| Chu et al. (2017) [51] | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 7 |
| Karishna et al. (2014) [52] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 5 |
| Telles et al. (2016) [53] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 8 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zou, L.; Sasaki, J.E.; Wei, G.-X.; Huang, T.; Yeung, A.S.; Neto, O.B.; Chen, K.W.; Hui, S.S.-c. Effects of Mind–Body Exercises (Tai Chi/Yoga) on Heart Rate Variability Parameters and Perceived Stress: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2018, 7, 404. https://doi.org/10.3390/jcm7110404
Zou L, Sasaki JE, Wei G-X, Huang T, Yeung AS, Neto OB, Chen KW, Hui SS-c. Effects of Mind–Body Exercises (Tai Chi/Yoga) on Heart Rate Variability Parameters and Perceived Stress: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2018; 7(11):404. https://doi.org/10.3390/jcm7110404
Chicago/Turabian StyleZou, Liye, Jeffer Eidi Sasaki, Gao-Xia Wei, Tao Huang, Albert S. Yeung, Octávio Barbosa Neto, Kevin W. Chen, and Stanley Sai-chuen Hui. 2018. "Effects of Mind–Body Exercises (Tai Chi/Yoga) on Heart Rate Variability Parameters and Perceived Stress: A Systematic Review with Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 7, no. 11: 404. https://doi.org/10.3390/jcm7110404