Impact of Hyperbaric Oxygen Therapy on Subsequent Neurological Sequelae Following Carbon Monoxide Poisoning

 , ,
, ,
Abstract
:
1. Introduction
2. Experimental Section
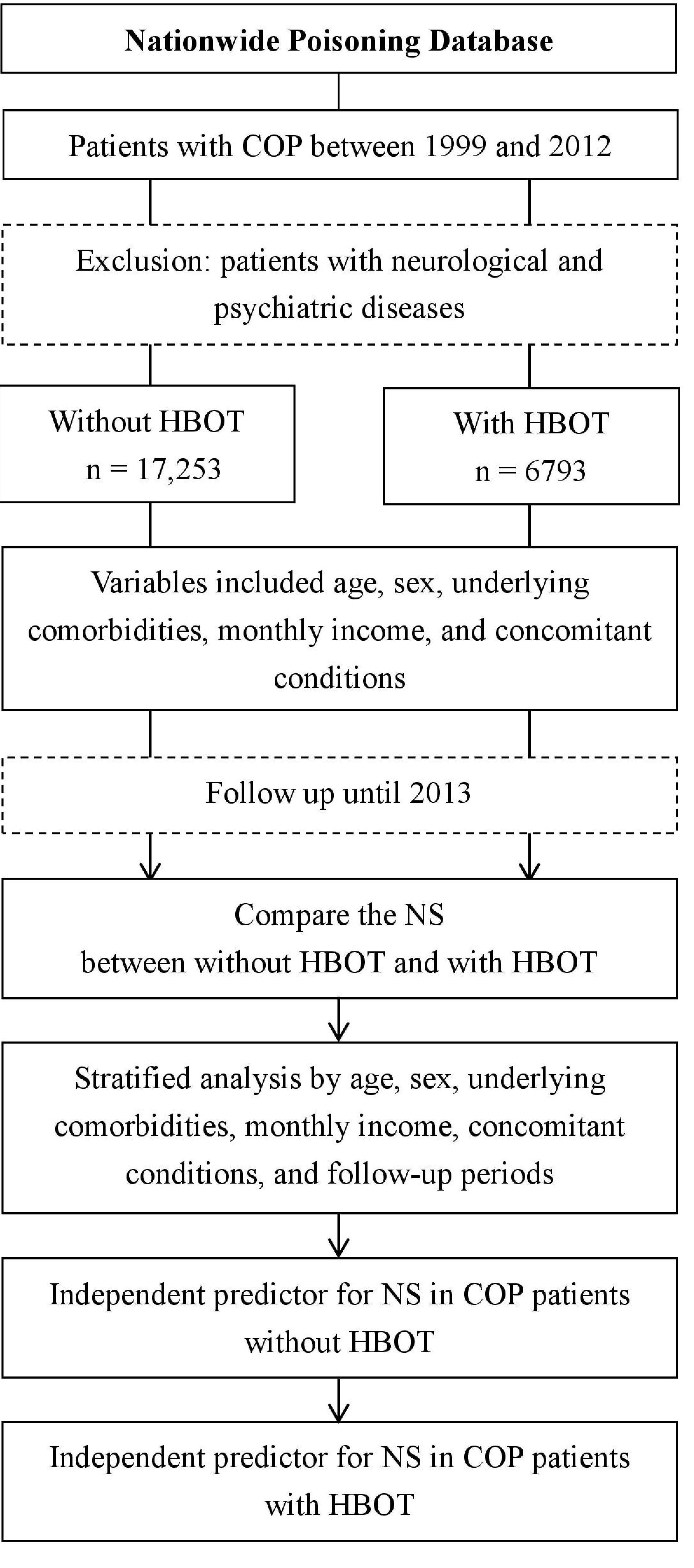
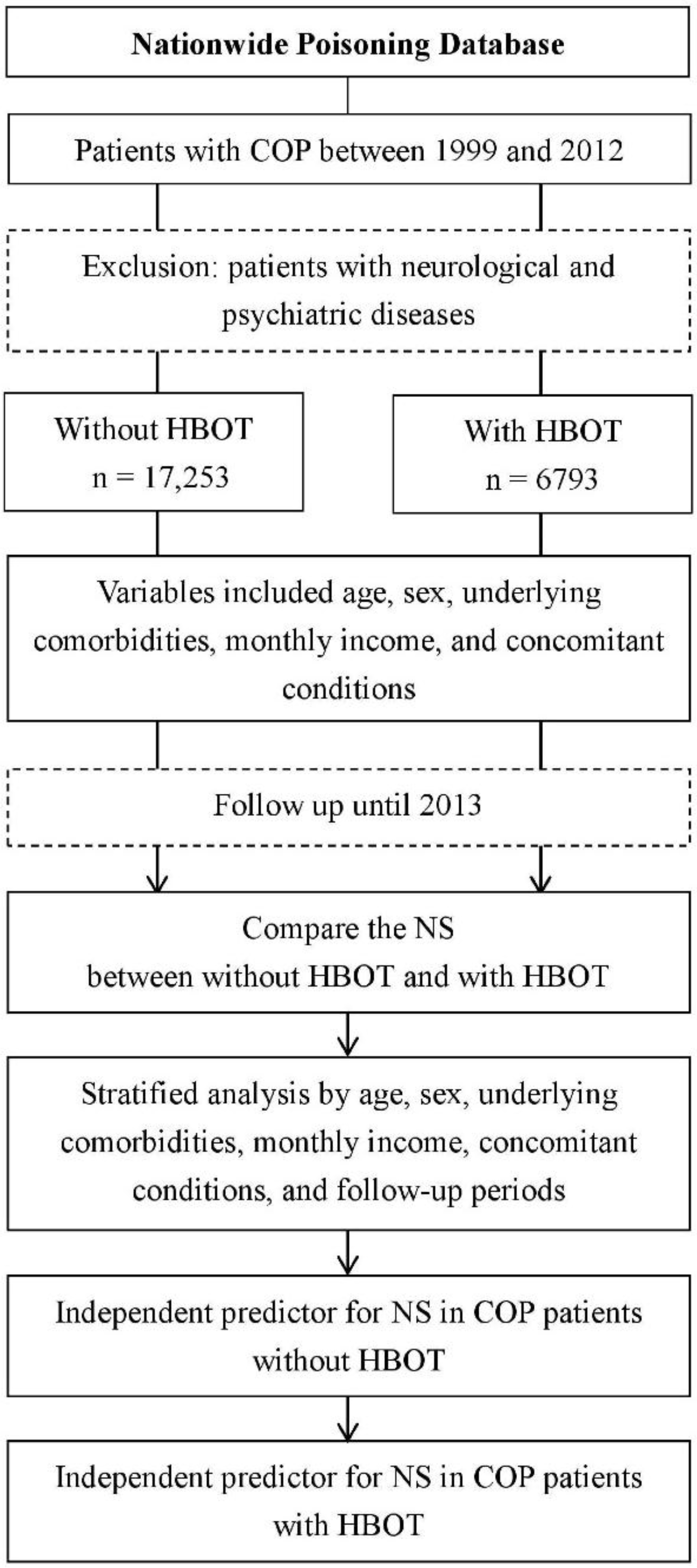
2.1. Data Source
2.2. Identification of Patients with COP
2.3. Definitions of Variables
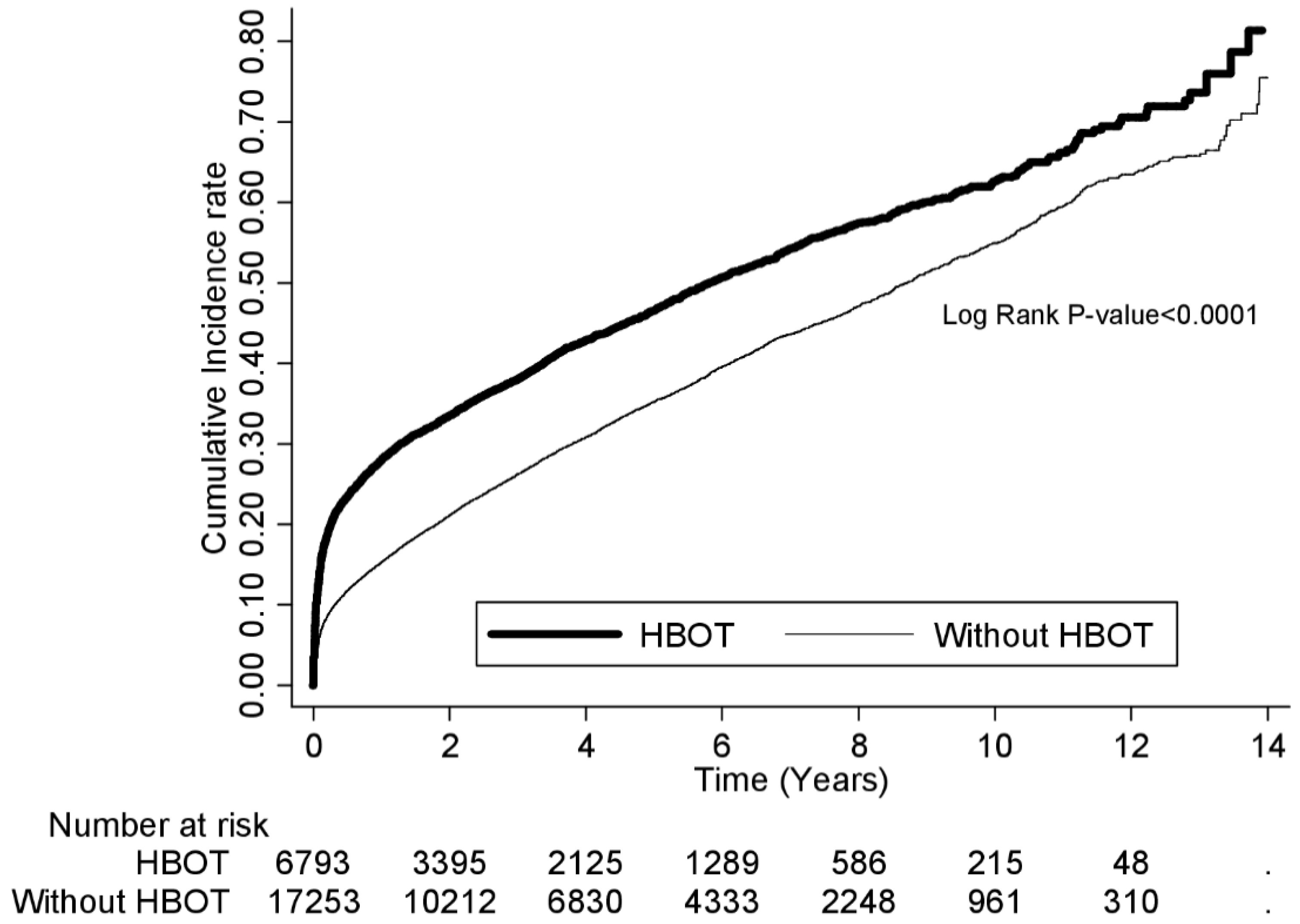
2.4. Comparison of the Risk for NS Between the Two Cohorts and Independent Predictors for NS
2.5. Ethics Statement
2.6. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| HBOT | hyperbaric oxygen therapy |
| NS | neurological sequelae |
| COP | carbon monoxide poisoning |
| NBO | normobaricoxygen |
| COPD | chronic pulmonary obstructive disease |
| HIV | Human Immunodeficiency Virus |
| AHR | adjusted hazard ratio |
| CI | confidence interval |
| CO | carbon monoxide |
| NPD | Nationwide Poisoning Database |
| NHIRD | National Health Insurance Research Database |
| ICD-9-CM | International Classification of Diseases, Ninth Revision, Clinical Modification |
| COHb | carboxyhemoglobin |
| IRR | incidence rate ratio |
| ATA | atmosphere absolute |
References
- United States Environmental Protection Agency. An Introduction to Indoor Air Quality (IAQ). Carbon Monoxide (CO). Available online: http://www.epa.gov/iaq/co.html (accessed on 22 March 2016).
- CDC (Centers for Disease Control and Prevention). Unintentional, non-fire-related, carbon monoxide exposures―United States, 2001–2003. MMWR Morb. Morta.l Wkly. Rep. 2005, 54, 36–39. [Google Scholar]
- Prockop, L.D.; Chichkova, R.I. Carbon monoxide intoxication: An updated review. J. Neurol. Sci. 2007, 262, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Ernst, A.; Zibrak, J.D. Carbon monoxide poisoning. N. Engl. J. Med. 1998, 339, 1603–1608. [Google Scholar] [CrossRef] [PubMed]
- Hampson, N.B.; Weaver, L.K. Carbon monoxide poisoning: A new incidence for an old disease. Undersea Hyperb. Med. 2007, 34, 163–168. [Google Scholar] [PubMed]
- Hampson, N.B.; Piantadosi, C.A.; Thom, S.R.; Weaver, L.K. Practice recommendations in the diagnosis, management, and prevention of carbon monoxide poisoning. Am. J. Respir. Crit. Care 2012, 186, 1095–1101. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.J.; Liao, S.C.; Lee, M.B. Suicide by charcoal burning in Taiwan, 1995–2006. J. Affect. Disord. 2010, 120, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.J.; Lavonas, E.J.; Sloan, E.P.; Jagoda, A.S. Clinical policy: Critical issues in the management of adult patients presenting to the emergency department with acute carbon monoxide poisoning. Ann. Emerg. Med. 2008, 51, 138–152. [Google Scholar] [CrossRef] [PubMed]
- Buckley, N.A.; Juurlink, D.N.; Isbister, G.; Bennett, M.H.; Lavonas, E.J. Hyperbaric oxygen for carbon monoxide poisoning. Cochrane Database Syst. Rev. 2011, 4. [Google Scholar] [CrossRef] [PubMed]
- Buckley, N.A.; Juurlink, D.N. Carbon monoxide treatment guidelines must acknowledge the limitations of the existing evidence. Am. J. Respir. Crit. Care 2013, 187, 1390. [Google Scholar] [CrossRef] [PubMed]
- Hampson, N.B.; Piantadosi, C.A.; Thom, S.R.; Weaver, L.K. Reply: Carbon monoxide treatment guidelines must acknowledge the limitations of the existing evidence. Am. J. Respir. Crit. Care 2013, 187, 1390–1391. [Google Scholar] [CrossRef] [PubMed]
- Weaver, L.K.; Hopkins, R.O.; Chan, K.J.; Churchill, S.; Elliott, C.G.; Clemmer, T.P.; Orme, J.F.; Thomas, F.O.; Morris, A.H. Hyperbaric oxygen for acute carbon monoxide poisoning. N. Engl. J. Med. 2002, 347, 1057–1067. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.C.; Ho, C.H.; Chen, Y.C.; Lin, H.J.; Hsu, C.C.; Wang, J.J.; Su, S.B.; Guo, H.R. Hyperbaric oxygen therapy is associated with lower short- and long-term mortality in patients with carbon monoxide poisoning. Chest 2017, 152, 943–953. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance Research Database. Available online: http://nhird.nhri.org.tw/en/index.html (accessed on 22 April 2017).
- Weaver, L.K. Carbon monoxide poisoning. N. Engl. J. Med. 2009, 360, 1217–1225. [Google Scholar] [CrossRef] [PubMed]
- Buckley, N.A.; Isbister, G.K.; Stokes, B.; Juurlink, D.N. Hyperbaric oxygen for carbon monoxide poisoning: A systematic review and critical analysis of the evidence. Toxicol. Rev. 2005, 24, 75–92. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-N.; Lin, C.-L.; Lin, M.-C.; Lai, C.-H.; Lin, H.-H.; Yang, C.-H.; Sung, F.-C.; Kao, C.-H. Risk of leukaemia in children infected with enterovirus: A nationwide, retrospective, population-based, Taiwanese-registry, cohort study. Lancet Oncol. 2015, 16, 1335–1343. [Google Scholar] [CrossRef]
- Lee, C.-C.; Lee, M.-T.; Chen, Y.-S.; Lee, S.-H.; Chen, Y.-S.; Chen, S.-C.; Chang, S.-C. Risk of Aortic Dissection and Aortic Aneurysm in Patients Taking Oral Fluoroquinolone. JAMA Intern. Med. 2015, 175, 1839–1847. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance Administration, Ministry of Health and Welfare. Items for Medical Payments. Available online: http://www.nhi.gov.tw/query/query2.aspx (accessed on 23 April 2017).
- National Health Insurance Administration, Ministry of Health and Welfare. Classification of Diseases. Available online: http://www.nhi.gov.tw/webdata/webdata.aspx?menu=18&menu_id=703&webdata_id=1008 (accessed on 23 April 2017).
- Annane, D.; Chadda, K.; Gajdos, P.; Jars-Guincestre, M.C.; Chevret, S.; Raphael, J.C. Hyperbaric oxygen therapy for acute domestic carbon monoxide poisoning: Two randomized controlled trials. Intens. Care Med. 2011, 37, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Scheinkestel, C.D.; Bailey, M.; Myles, P.S.; Jones, K.; Cooper, D.J.; Millar, I.L.; Tuxen, D.V. Hyperbaric or normobaric oxygen for acute carbon monoxide poisoning: A randomised controlled clinical trial. Med. J. Aust. 1999, 170, 203–210. [Google Scholar] [PubMed]
- Huang, C.-C.; Chung, M.-H.; Weng, S.-F.; Chien, C.-C.; Lin, S.-J.; Lin, H.-J.; Guo, H.-R.; Su, S.-B.; Hsu, C.-C.; Juan, C.-W. Long-term prognosis of patients with carbon monoxide poisoning: A nationwide cohort study. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Thom, S.R.; Taber, R.L.; Mendiguren, I.I.; Clark, J.M.; Hardy, H.M.; Fisher, A.B. Delayed neuropsychologic sequelae after carbon monoxide poisoning: Prevention by treatment with hyperbaric oxygen. Ann. Emerg. Med. 1995, 25, 474–480. [Google Scholar] [CrossRef]
- Thom, S.R. Hyperbaric-oxygen therapy for acute carbon monoxide poisoning. N. Engl. J. Med. 2002, 347, 1105–1106. [Google Scholar] [CrossRef] [PubMed]
- Weaver, L.K.; Valentine, K.J.; Hopkins, R.O. Carbon monoxide poisoning: Risk factors for cognitive sequelae and the role of hyperbaric oxygen. Am. J. Respir. Crit. Care 2007, 176, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Zou, J.-F.; Guo, Q.; Shao, H.; Li, B.; Du, Y.X.; Liu, M.-F.; Liu, F.-L.; Dai, L.-X.; Lin, H.-J.; Su, S.-B.; et al. Lack of pupil reflex and loss of consciousness predict 30-day neurological sequelae in patients with carbon monoxide poisoning. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Zou, J.-F.; Guo, Q.; Shao, H.; Li, B.; Du, Y.-X.; Liu, M.-F.; Liu, F.-L.; Dai, L.-X.; Chung, M.-H.; Lin, H.-J. A positive Babinski reflex predicts delayed neuropsychiatric sequelae in Chinese patients with carbon monoxide poisoning. Biomed. Res. Int. 2014, 2014, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Pan, X.; Wan, Y.; Zhang, Q.; Liang, W. Factors affecting the prognosis of patients with delayed encephalopathy after acute carbon monoxide poisoning. Am. J. Emerg. Med. 2011, 29, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.-H.; Lin, J.-Y.; Pan, K.-T.; Chou, Y.-C.; Peng, C.-K.; Huang, K.-L. Predicting poor outcome in patients with intentional carbon monoxide poisoning and acute respiratory failure: A retrospective study. J. Med. Sci. 2015, 35, 105–110. [Google Scholar] [CrossRef]
- Liu, K.Y.; Beautrais, A.; Caine, E.; Chan, K.; Chao, A.; Conwell, Y.; Law, C.; Lee, D.; Li, P.; Yip, P. Charcoal burning suicides in Hong Kong and urban Taiwan: An illustration of the impact of a novel suicide method on overall regional rates. J. Epidemiol. Commun. Health 2007, 61, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Runyan, C.W.; Johnson, R.M.; Yang, J.; Waller, A.E.; Perkis, D.; Marshall, S.W.; Coyne-Beasley, T.; MSPH, K.S.M. Risk and protective factors for fires, burns, and carbon monoxide poisoning in U.S. households. Am. J. Prev. Med. 2005, 28, 102–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson-Arbor, K.; Liebman, D.L.; Carter, E.M. A survey of residential carbon monoxide detector utilization among Connecticut Emergency Department patients. Clin. Toxicol. 2012, 50, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Lemstra, M.; Rogers, M.; Moraros, J. Income and heart disease: Neglected risk factor. Can. Fam. Physician 2015, 61, 698–704. [Google Scholar] [PubMed]
- Behera, S.K.; Winkleby, M.A.; Collins, R. Low awareness of cardiovascular disease risk among low-income African-American women. Am. J. Health Promot. 2000, 14, 301–305. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Variable | Total Patients n = 24,046 (100.0) | Without HBOT n = 17,253 (71.8) | With HBOT n = 6793 (28.2) | p-Value * |
|---|---|---|---|---|
| Age (years) | 35.7 ± 16.6 | 36.1 ± 17.2 | 34.8 ± 14.8 | <0.001 |
| Age subgroup (years) | ||||
| <20 | 3382 (14.1) | 2509 (14.5) | 873 (12.9) | <0.001 |
| 20−34 | 8987 (37.4) | 6221 (36.1) | 2766 (40.7) | |
| 35−50 | 7293 (30.3) | 5148 (29.8) | 2145 (31.6) | |
| 51−64 | 2996 (12.5) | 2223 (12.9) | 773 (11.4) | |
| ≥65 | 1388 (5.8) | 1152 (6.7) | 236 (3.5) | |
| Sex | ||||
| Female | 12,062 (50.2) | 8653 (50.2) | 3409 (50.2) | 0.966 |
| Male | 11,984 (49.8) | 8600 (49.9) | 3384 (49.8) | |
| Underlying comorbidity | ||||
| Hypertension | 2815 (11.7) | 2216 (12.8) | 599 (8.8) | <0.001 |
| Diabetes | 1499 (6.2) | 1137 (6.6) | 362 (5.3) | <0.001 |
| Chronic obstructive pulmonary disease | 385 (1.6) | 320 (1.9) | 65 (1.0) | <0.001 |
| Hyperlipidemia | 1967 (8.2) | 1486 (8.6) | 481 (7.1) | <0.001 |
| Malignancy | 643 (2.7) | 499 (2.9) | 144 (2.1) | <0.001 |
| Coronary artery disease | 1358 (5.7) | 1067 (6.2) | 291 (4.3) | <0.001 |
| Congestive heart failure | 392 (1.6) | 326 (1.9) | 66 (1.0) | <0.001 |
| Liver disease | 3307 (13.8) | 2428 (14.1) | 879 (12.9) | 0.022 |
| Renal disease | 2445 (10.2) | 1804 (10.5) | 641 (9.4) | 0.013 |
| Connective tissue disease | 208 (0.9) | 146 (0.9) | 62 (0.9) | 0.616 |
| HIV infection | 61 (0.3) | 46 (0.3) | 15 (0.2) | 0.525 |
| Alcoholism | 861 (3.6) | 668 (3.9) | 193 (2.8) | <0.001 |
| Monthly income (NTD) | ||||
| <19,999 | 17,622 (73.3) | 12,670 (73.4) | 4952 (72.9) | 0.156 |
| 20,000−39,999 | 5122 (21.3) | 3629 (21.0) | 1493 (22.0) | |
| ≥40,000 | 1302 (5.4) | 954 (5.5) | 348 (5.1) | |
| Concomitant condition | ||||
| Suicide | 4763 (19.8) | 2642 (15.3) | 2121 (31.2) | <0.001 |
| Drug poisoning | 245 (1.0) | 187 (1.1) | 58 (0.9) | 0.110 |
| Acute respiratory failure | 1737 (7.2) | 1077 (6.2) | 660 (9.7) | <0.001 |
| Acute myocardial injury | 54 (0.2) | 39 (0.2) | 15 (0.2) | 0.939 |
| Acute hepatitis | 52 (0.2) | 39 (0.2) | 13 (0.2) | 0.602 |
| Acute renal failure | 299 (1.2) | 167 (1.0) | 132 (1.9) | <0.001 |
| Variable | With HBOT | Without HBOT (reference) | Crude HR (95% CI) | AHR (95% CI) * | IRR (95% CI) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Case | PY | Rate | Case | PY | Rate | ||||
| Overall analysis | 3043 | 20,765.3 | 146.5 | 5992 | 64,832.7 | 92.4 | 1.5 (1.4–1.6) | 1.4 (1.4–1.5) | – |
| Stratified analysis | |||||||||
| NS subgroup | |||||||||
| Degenerative diseases of the central nervous system | 657 | 28,291.9 | 23.2 | 1197 | 80,595.3 | 14.9 | 1.5 (1.3–1.6) | 1.5 (1.3–1.6) | – |
| Psychiatric diseases | 2076 | 23,642.8 | 87.8 | 4145 | 69,828.3 | 59.3 | 1.4 (1.3–1.5) | 1.3 (1.2–1.4) | – |
| Other diseases of the nervous system | 1461 | 25,357.5 | 57.6 | 2619 | 75,099.8 | 34.9 | 1.6 (1.5–1.7) | 1.5 (1.4–1.6) | – |
| Age (years) | |||||||||
| <20 | 217 | 3851.3 | 56.3 | 465 | 12,736.9 | 36.5 | 1.5 (13–1.8) | 1.4 (1.2–1.7) | – |
| 20−34 | 1243 | 8449.4 | 147.1 | 2170 | 24,724.1 | 87.8 | 1.6 (1.5–1.7) | 1.4 (1.3–1.5) | – |
| 35−50 | 1060 | 6093.6 | 174.0 | 1999 | 18,418.8 | 108.5 | 1.5 (1.4–1.6) | 1.4 (1.3–1.5) | – |
| 51−64 | 393 | 1890.4 | 207.9 | 871 | 6226.9 | 139.9 | 1.5 (1.3–1.6) | 1.4 (1.3–1.6) | – |
| ≥65 | 130 | 480.6 | 270.5 | 487 | 2726.2 | 178.6 | 1.5 (1.2–1.8) | 1.4 (1.2–1.7) | – |
| Sex | |||||||||
| Female | 1566 | 10,574.5 | 148.1 | 3235 | 33,324.4 | 97.1 | 1.5 (1.4–1.6) | 1.6 (1.3–1.4) | – |
| Male | 1477 | 10,190.8 | 144.9 | 2757 | 31,508.3 | 87.5 | 1.6 (1.5–1.7) | 1.5 (1.4–1.6) | – |
| Underlying comorbidity | |||||||||
| Hypertension | 309 | 1374.7 | 224.8 | 925 | 5416.5 | 170.8 | 1.3 (1.1–1.5) | 1.3 (1.1–1.5) | – |
| Diabetes | 167 | 852.4 | 195.9 | 437 | 2676.5 | 163.3 | 1.2 (1.0–1.4) | 1.2 (1.0–1.4) | – |
| Chronic obstructive pulmonary disease | 42 | 104.8 | 400.7 | 129 | 730.3 | 176.7 | 2.1 (1.4–2.9) | 2.1 (1.4–3.0) | – |
| Hyperlipidemia | 257 | 1008.0 | 255.0 | 577 | 3700.7 | 155.9 | 1.6 (1.4–1.8) | 1.5 (1.3–1.8) | – |
| Malignancy | 72 | 258.7 | 278.3 | 184 | 989.0 | 186.1 | 1.4 (1.1–1.9) | 1.4 (1.1–1.9) | – |
| Coronary artery disease | 148 | 621.3 | 238.2 | 452 | 2490.7 | 181.5 | 1.3 (1.1–1.6) | 1.3 (1.0–1.5) | – |
| Congestive heart failure | 33 | 130.6 | 252.7 | 122 | 616.9 | 197.8 | 1.3 (0.9–1.9) | 1.5 (1.0–2.3) | – |
| Liver disease | 446 | 2059.1 | 216.6 | 1037 | 6424.1 | 161.4 | 1.3 (1.2–1.5) | 1.3 (1.1–1.4) | – |
| Renal disease | 319 | 1490.7 | 214 | 707 | 4975.9 | 142.1 | 1.5 (1.3–1.7) | 1.4 (1.2–1.6) | – |
| Connective tissue disease | 38 | 121.9 | 311.7 | 55 | 345.1 | 159.4 | 1.9 (1.3–2.9) | 2.0 (1.2–3.2) | – |
| HIV infection | 9 | 29.2 | 308.3 | 13 | 118.5 | 109.7 | 2.5 (1.1–5.9) | 10.3 (2.3–45.8) | – |
| Alcoholism | 115 | 381.3 | 301.6 | 308 | 1574.3 | 195.7 | 1.5 (1.2–1.9) | 1.6 (1.2–1.9) | – |
| Monthly income (NTD) | |||||||||
| <19,999 | 2322 | 15,060.2 | 154.2 | 4573 | 47,295.3 | 96.7 | 1.5 (1.4–1.6) | 1.4 (1.4–1.5) | – |
| 20,000−39,999 | 586 | 4516.8 | 129.7 | 1142 | 13,501.0 | 84.6 | 1.5 (1.3–1.6) | 1.4 (1.2–1.5) | – |
| ≥40,000 | 135 | 1188.4 | 113.6 | 277 | 4036.4 | 68.6 | 1.6 (1.3–1.9) | 1.5 (1.2–1.9) | – |
| Suicide | |||||||||
| Yes | 1181 | 5664.8 | 208.5 | 1305 | 8639.4 | 151.1 | 1.3 (1.2–1.4) | 1.3 (1.2–1.4) | – |
| No | 1862 | 15,100.5 | 123.3 | 4687 | 56,193.3 | 83.4 | 1.4 (1.3–1.5) | 1.5 (1.4–1.5) | – |
| Drug poisoning | |||||||||
| Yes | 33 | 116.0 | 284.4 | 81 | 620.2 | 130.6 | 1.9 (1.2–2.8) | 1.6 (1.0–2.6) | – |
| No | 3010 | 20,649.3 | 145.8 | 5911 | 64,212.5 | 92.1 | 1.5 (1.4–1.6) | 1.4 (1.4–1.5) | – |
| Acute respiratory failure | |||||||||
| Yes | 429 | 1268.5 | 338.2 | 440 | 2281.6 | 192.9 | 1.6 (1.4–1.8) | 1.5 (1.3–1.8) | – |
| No | 2614 | 19,496.8 | 134.1 | 5552 | 62,551.1 | 88.8 | 1.4 (1.4–1.5) | 1.4 (1.3–1.5) | – |
| Follow-up period | |||||||||
| <2 weeks | 597 | 245.2 | 2434.7 | 579 | 620.5 | 933.1 | 2.6 (2.3–2.9) | 2.4 (2.1–2.7) | 2.6 (2.3–2.9) |
| 2–4 weeks | 283 | 290.6 | 973.8 | 308 | 733.9 | 419.7 | 1.7 (1.5–2.0) | 1.6 (1.4–1.9) | 2.3 (2.0–2.7) |
| 1−6 months | 682 | 2279.1 | 299.2 | 1010 | 6162.6 | 163.9 | 1.8 (1.6–2.0) | 1.6 (1.4–1.7) | 1.8 (1.7–2.0) |
| 6−12 months | 283 | 2871.4 | 98.6 | 537 | 7661.6 | 70.1 | 1.7 (0.9–1.2) | 1.0 (0.8–1.1) | 1.4 (1.2–1.6) |
| 1−2 years | 306 | 5422.4 | 56.4 | 816 | 15,028.2 | 54.3 | 1.0 (0.9–1.2) | 0.9 (0.8–1.1) | 1.0 (0.9–1.2) |
| 2−4 years | 416 | 10,066.8 | 41.3 | 1121 | 28,572.7 | 39.2 | 1.0 (0.9–1.1) | 0.9 (0.8–1.1) | 1.1 (0.9–1.2) |
| ≥4 years | 476 | 20,765.3 | 22.9 | 1621 | 64,832.7 | 25.0 | 1.1 (0.9–1.2) | 1.0 (0.9–1.2) | 0.9 (0.8–1.0) |
| Patients with COP Who Received HBOT | Patients with COP Who Did Not Receive HBOT | |||
|---|---|---|---|---|
| Variable | Crude HR (95% CI) | AHR (95% CI) * | Crude HR (95% CI) | AHR (95% CI) * |
| Age (years) | ||||
| <20 | 1 | 1 | 1 | 1 |
| 20−34 | 2.4 (2.1–2.6) | 2.3 (2.1–2.5) | 2.3 (2.0–2.7) | 2.2 (1.9–2.5) |
| 35−50 | 2.9 (2.6–3.2) | 2.6 (2.3–2.9) | 2.7 (2.3–3.1) | 2.4 (2.0–2.8) |
| 51−64 | 3.5 (3.1–3.9) | 2.8 (2.5–3.2) | 3.0 (2.5–3.5) | 2.6 (2.2–3.1) |
| ≥65 | 4.3 (3.8–4.9) | 3.4 (2.9–3.9) | 3.5 (2.8–4.3) | 2.9 (2.2–3.7) |
| Sex | ||||
| Female | 1 | 1 | 1 | 1 |
| Male | 0.9 (0.9–0.9) | 1.2 (1.2–1.3) | 1.0 (0.9–1.1) | 1.1 (1.0–1.2) |
| Monthly income (NTD) | ||||
| <19,999 | 1.4 (1.2–1.6) | 1.4 (1.3–1.6) | 1.3 (1.1–1.6) | 1.3 (1.1–1.6) |
| 20,000−39,999 | 1.2 (1.1–1.4) | 1.2 (1.0–1.3) | 1.1 (0.9–1.3) | 1.1 (0.9–1.3) |
| ≥40,000 | 1 | 1 | 1 | 1 |
| Underlying comorbidity | ||||
| Hypertension | 1.8 (1.7–1.9) | 1.2 (1.1–1.3) | 1.4 (1.2–1.6) | 1.0 (0.9–1.2) |
| Diabetes | 1.6 (1.5–1.8) | 1.0 (0.9–1.1) | 1.2 (1.0–1.4) | 0.7 (0.6–0.9) |
| Chronic obstructive pulmonary disease | 1.7 (1.4–2.0) | 1.0 (0.8–1.2) | 2.0 (1.5–2.7) | 1.5 (1.1–2.1) |
| Hyperlipidemia | 1.6 (1.5–1.7) | 1.0 (0.9–1.1) | 1.5 (1.3–1.7) | 1.3 (1.1–1.5) |
| Malignancy | 1.8 (1.5–2.0) | 1.2 (1.0–1.4) | 1.5 (1.2–1.9) | 1.1 (0.9–1.4) |
| Coronary artery disease | 1.8 (1.7–2.0) | 1.1 (1.0–1.2) | 1.4 (1.2–1.6) | 1.0 (0.8–1.2) |
| Congestive heart failure | 1.8 (1.5–2.1) | 1.0 (0.8–1.2) | 1.4 (1.0–2.0) | 0.9 (0.6–1.3) |
| Liver disease | 1.8 (1.6–1.9) | 1.3 (1.2–1.4) | 1.4 (1.2–1.5) | 1.1 (0.9–1.2) |
| Renal disease | 1.5 (1.4–1.6) | 1.1 (1.0–1.2) | 1.3 (1.2–1.5) | 1.1 (1.0–1.2) |
| Connective tissue disease | 1.6 (1.2–2.1) | 1.1 (0.9–1.5) | 1.7 (1.3–2.4) | 1.3 (1.0–1.8) |
| HIV infection | 1.1 (0.6–1.9) | 1.0 (0.6–1.7) | 1.7 (0.9–3.2) | 1.2 (0.6–2.3) |
| Alcoholism | 1.9 (1.7–2.2) | 1.4 (1.2–1.5) | 1.7 (1.4–2.0) | 1.3 (1.1–1.6) |
| Concomitant condition | ||||
| Suicide | 1.8 (1.7–1.9) | 1.5 (1.4–1.6) | 1.6 (1.5–1.7) | 1.4 (1.3–1.5) |
| Drug poisoning | 1.4 (1.1–1.7) | 1.2 (1.0–1.5) | 1.6 (1.2–2.3) | 1.5 (1.1–2.1) |
| Acute respiratory failure | 2.0 (1.8–2.2) | 1.6 (1.4–1.7) | 2.1 (1.9–2.3) | 1.7 (1.6–1.9) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.-C.; Ho, C.-H.; Chen, Y.-C.; Hsu, C.-C.; Wang, Y.-F.; Lin, H.-J.; Wang, J.-J.; Guo, H.-R. Impact of Hyperbaric Oxygen Therapy on Subsequent Neurological Sequelae Following Carbon Monoxide Poisoning. J. Clin. Med. 2018, 7, 349. https://doi.org/10.3390/jcm7100349
Huang C-C, Ho C-H, Chen Y-C, Hsu C-C, Wang Y-F, Lin H-J, Wang J-J, Guo H-R. Impact of Hyperbaric Oxygen Therapy on Subsequent Neurological Sequelae Following Carbon Monoxide Poisoning. Journal of Clinical Medicine. 2018; 7(10):349. https://doi.org/10.3390/jcm7100349
Chicago/Turabian StyleHuang, Chien-Cheng, Chung-Han Ho, Yi-Chen Chen, Chien-Chin Hsu, Yi-Fong Wang, Hung-Jung Lin, Jhi-Joung Wang, and How-Ran Guo. 2018. "Impact of Hyperbaric Oxygen Therapy on Subsequent Neurological Sequelae Following Carbon Monoxide Poisoning" Journal of Clinical Medicine 7, no. 10: 349. https://doi.org/10.3390/jcm7100349