
Diagnostic Accuracy of Cone Beam Computed Tomography and Periapical Radiography for Detecting Apical Root Resorption in Retention Phase of Orthodontic Patients: A Cross-Sectional Study
 ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Radiographic Technique
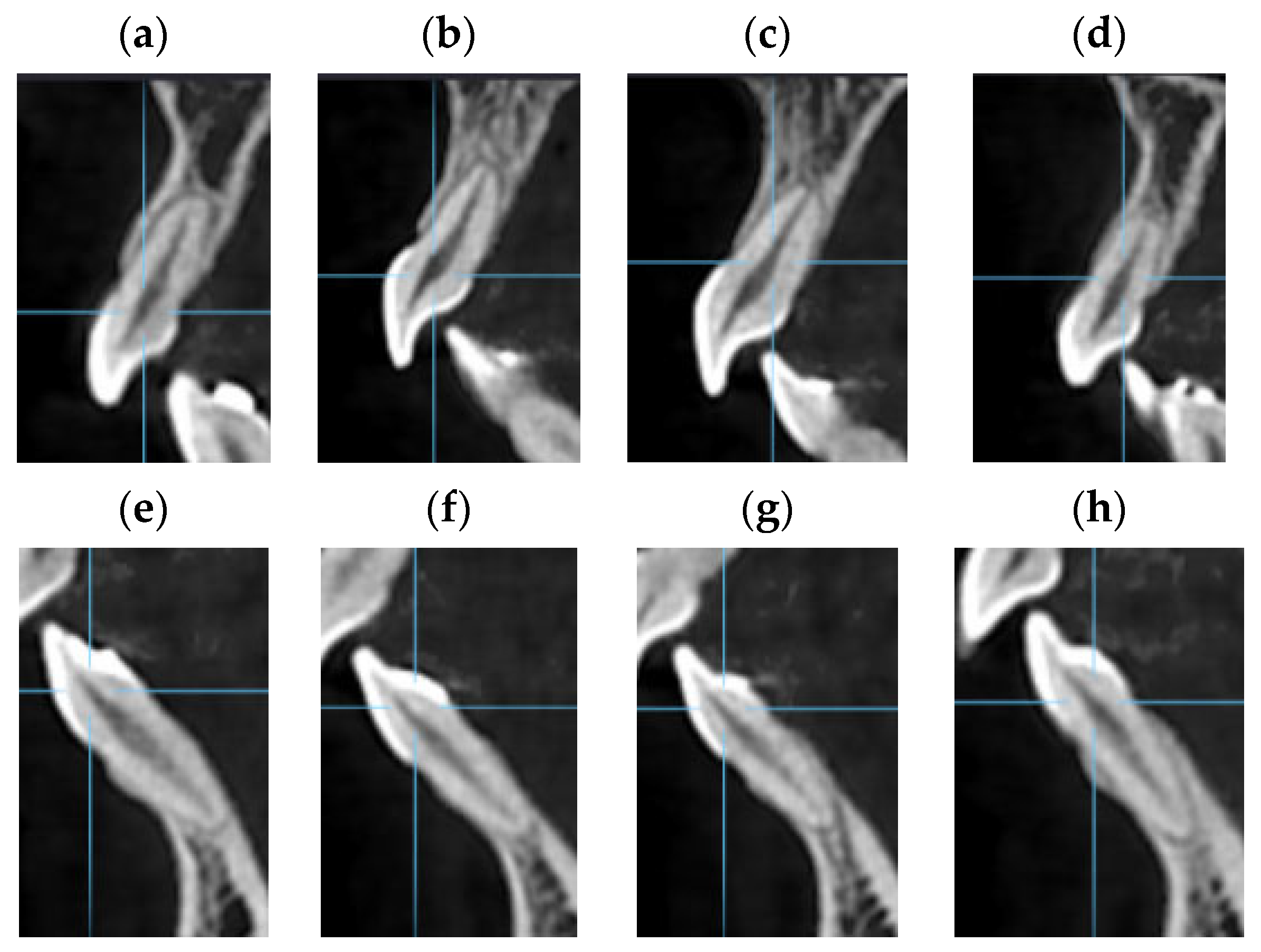
2.3. CBCT Technique
2.4. Radiological Assessment
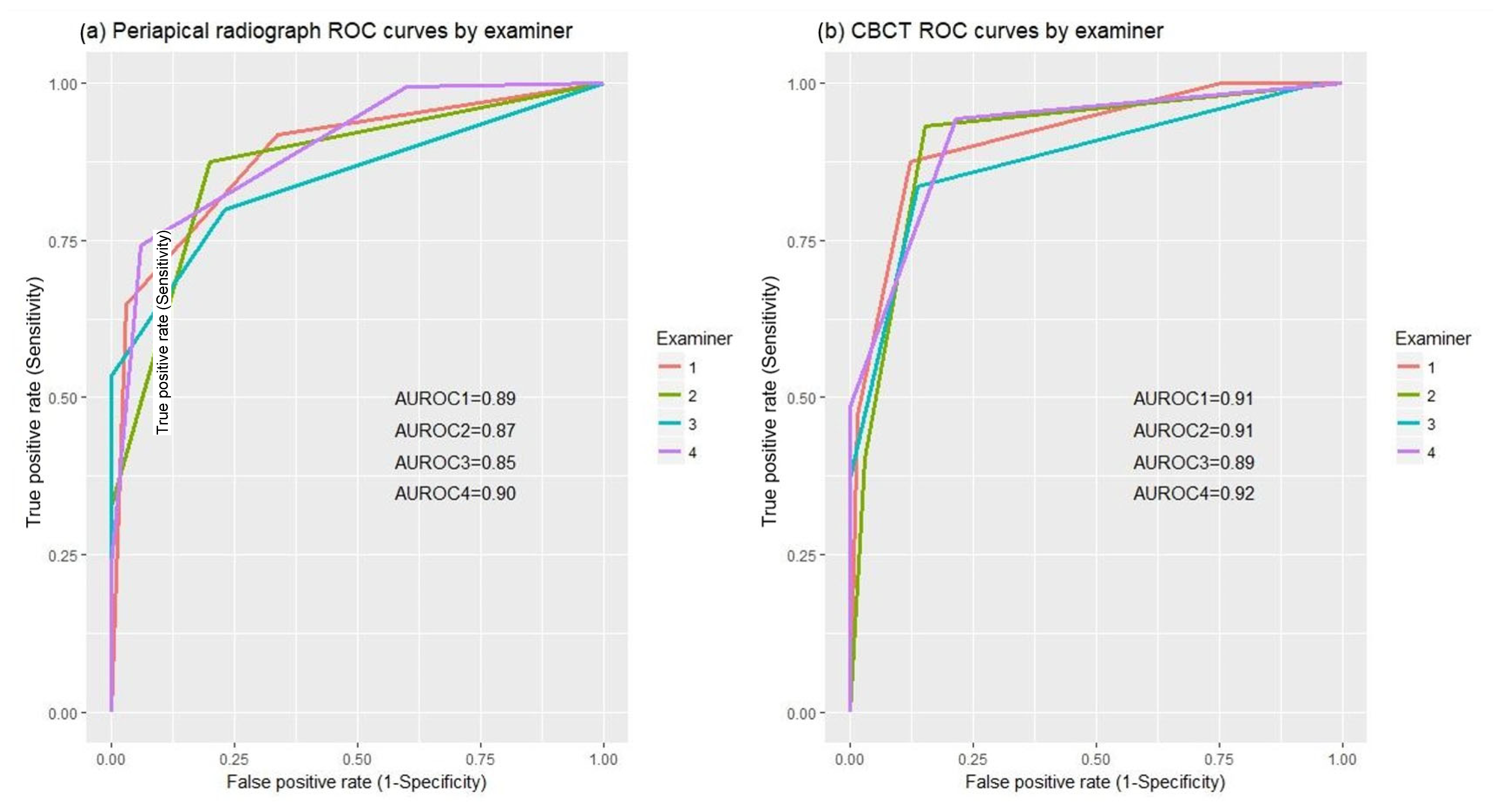
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yi, J.; Sun, Y.; Li, Y.; Li, C.; Li, X.; Zhao, Z. Cone-beam computed tomography versus periapical radiograph for diagnosing external root resorption: A systematic review and meta-analysis. Angle Orthod. 2017, 87, 328–337. [Google Scholar] [CrossRef]
- Ren, H.; Chen, J.; Deng, F.; Zheng, L.; Liu, X.; Dong, Y. Comparison of cone-beam computed tomography and periapical radiography for detecting simulated apical root resorption. Angle Orthod. 2013, 83, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Feller, L.; Khammissa, R.A.G.; Thomadakis, G.; Fourie, J.; Lemmer, J. Apical External Root Resorption and Repair in Orthodontic Tooth Movement: Biological Events. Biomed. Res. Int. 2016, 2016, 4864195. [Google Scholar] [CrossRef] [PubMed]
- Shokri, A.; Mortazavi, H.; Salemi, F.; Javadian, A.; Bakhtiari, H.; Matlabi, H. Diagnosis of simulated external root resorption using conventional intraoral film radiography, ccd, psp, and cbct: A comparison study. Biomed. J. 2013, 36, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Dawood, A.; Wilson, R.; Horner, K.; Mannocci, F. The detection and management of root resorption lesions using intraoral radiography and cone beam computed tomography—An in vivo investigation. Int. Endod. J. 2009, 42, 831–838. [Google Scholar] [CrossRef] [PubMed]
- Durack, C.; Patel, S.; Davies, J.; Wilson, R.; Mannocci, F. Diagnostic accuracy of small volume cone beam computed tomography and intraoral periapical radiography for the detection of simulated external inflammatory root resorption. Int. Endod. J. 2011, 44, 136–147. [Google Scholar] [CrossRef] [PubMed]
- Aidos, H.; Diogo, P.; Santos, J.M. Root resorption classifications: A narrative review and a clinical aid proposal for routine assessment. Eur. Endod. J. 2018, 3, 134–145. [Google Scholar] [CrossRef]
- Kumar, V.; Gossett, L.; Blattner, A.; Iwasaki, L.R.; Williams, K.; Nickel, J.C. Comparison between cone-beam computed tomography and intraoral digital radiography for assessment of tooth root lesions. Am. J. Orthod. Dentofac. Orthop. 2011, 139, e533–e541. [Google Scholar] [CrossRef]
- Mohandesan, H.; Ravanmehr, H.; Valaei, N. A radiographic analysis of external apical root resorption of maxillary incisors during active orthodontic treatment. Eur. J. Orthod. 2007, 29, 134–139. [Google Scholar] [CrossRef]
- Pereira, S.; Lavado, N.; Nogueira, L.; Lopez, M.; Abreu, J.; Silva, H. Polymorphisms of genes encoding P2X7R, IL-1B, OPG and RANK in orthodontic-induced apical root resorption. Oral Dis. 2014, 20, 659–667. [Google Scholar] [CrossRef]
- Deng, Y.; Sun, Y.; Xu, T. Evaluation of root resorption after comprehensive orthodontic treatment using cone beam computed tomography (CBCT): A meta-analysis. BMC Oral Health 2018, 18, 116. [Google Scholar] [CrossRef]
- Weltman, B.; Vig, K.W.L.; Fields, H.W.; Shanker, S.; Kaizar, E.E. Root resorption associated with orthodontic tooth movement: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 462–476. [Google Scholar] [CrossRef] [PubMed]
- Årtun, J.; Van ’t Hullenaar, R.; Doppel, D.; Kuijpers-Jagtman, A.M. Identification of orthodontic patients at risk of severe apical root resorption. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Aman, C.; Azevedo, B.; Bednar, E.; Chandiramami, S.; German, D.; Nicholson, E.; Nicholson, K.; Scarfe, W.C. Apical root resorption during orthodontic treatment with clear aligners: A retrospective study using cone-beam computed tomography. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 842–851. [Google Scholar] [CrossRef] [PubMed]
- Ponder, S.N.; Benavides, E.; Kapila, S.; Hatch, N.E. Quantification of external root resorption by low- vs high-resolution cone-beam computed tomography and periapical radiography: A volumetric and linear analysis. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 77–91. [Google Scholar] [CrossRef] [PubMed]
- Roscoe, M.G.; Meira, J.B.C.; Cattaneo, P.M. Association of orthodontic force system and root resorption: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 610–626. [Google Scholar] [CrossRef] [PubMed]
- Deliga Schröder, Â.G.; Westphalen, F.H.; Schröder, J.C.; Fernandes, Â.; Westphalen, V.P.D. Accuracy of Digital Periapical Radiography and Cone-beam Computed Tomography for Diagnosis of Natural and Simulated External Root Resorption. J. Endod. 2018, 44, 1151–1158. [Google Scholar] [CrossRef] [PubMed]
- Fuss, Z.; Tsesis, I.; Lin, S. Root resorption—Diagnosis, classification and treatment choices based on stimulation factors. Dent. Traumatol. 2003, 19, 175–182. [Google Scholar] [CrossRef]
- Sondeijker, C.F.W.; Lamberts, A.A.; Beckmann, S.H.; Kuitert, R.B.; van Westing, K.; Persoon, S.; Kuijpers-Jagtman, A.M. Development of a clinical practice guideline for orthodontically induced external apical root resorption. Eur. J. Orthod. 2020, 42, 115–124. [Google Scholar] [CrossRef]
- NVVO. Wortelresorptie in de Orthodontie. 2018. Available online: https://www.orthodontist.nl/files/wortelresorptie-in-de-orthodontie.pdf (accessed on 20 April 2020).
- NVVO. Richtlijn Orthodontische Radiologie. 2018, pp. 1–122. Available online: https://orthodontist.nl/ (accessed on 20 April 2020).
- Parrales-Bravo, C.; Friedrichsdorf, S.P.; Costa, C.; Paiva, J.B.; Iglesias-Linares, A. Does endodontics influence radiological detection of external root resorption? An in vitro study. BMC Oral Health 2023, 23, 221. [Google Scholar] [CrossRef]
- Alamadi, E.; Alhazmi, H.; Hansen, K.; Lundgren, T.; Naoumova, J. A comparative study of cone beam computed tomography and conventional radiography in diagnosing the extent of root resorptions. Prog. Orthod. 2017, 18, 37. [Google Scholar] [CrossRef] [PubMed]
- Whaites, E. Princípios de Radiologia Odontológica, 4th ed.; Elsevier: Rio de Janeiro, Brazil, 2009. [Google Scholar]
- Samandara, A.; Papageorgiou, S.N.; Ioannidou-Marathiotou, I.; Kavvadia-Tsatala, S.; Papadopoulos, M.A. Evaluation of orthodontically induced external root resorption following orthodontic treatment using cone beam computed tomography (CBCT): A systematic review and meta-analysis. Eur. J. Orthod. 2019, 41, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Lima, T.F.R.; Gamba, T.D.O.; Zaia, A.A.; Soares, A.D.J. Evaluation of cone beam computed tomography and periapical radiography in the diagnosis of root resorption. Aust. Dent. J. 2016, 61, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Da Silva Campos, M.J.; Silva, K.S.; Gravina, M.A.; Fraga, M.R.; Vitral, R.W.F. Apical root resorption: The dark side of the root. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 492–498. [Google Scholar] [CrossRef]
- Andreasen, F.M.; Sewerin, I.; Mandel, U.; Andreasen, J.O. Radiographic assessment of simulated root resorption cavities. Dent. Traumatol. 1987, 3, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, F.; De Siivio, A.; Dreyer, C. Radiographie assessment of simulated external root résorption cavities in maxillary incisors. Endod. Dent. Traumatol. 1998, 14, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; He, S.; Gu, T.; Liu, Y.; Chen, S. Genetic and clinical risk factors of root resorption associated with orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 283–289. [Google Scholar] [CrossRef]
- Kapila, S.D.; Nervina, J.M. CBCT in orthodontics: Assessment of treatment outcomes and indications for its use. Dentomaxillofac. Radiol. 2015, 44, 20140282. [Google Scholar] [CrossRef]
- Ludlow, J.B.; Timothy, R.; Walker, C.; Hunter, R.; Benavides, E.; Samuelson, D.B.; Scheske, M.J. Ffective dose of dental CBCT—A meta analysis of published data and additional data for nine CBCT units. Dentomaxillofac. Radiol. 2015, 44, 20140197. [Google Scholar] [CrossRef]
- de Freitas, J.C.; Lyra, O.C.P.; de Alencar, A.H.G.; Estrela, C. Long-term evaluation of apical root resorption after orthodontic treatment using periapical radiography and cone beam computed tomography. Dent. Press J. Orthod. 2013, 18, 104–112. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef]
- Gamer Matthias, L.J.; SIFP. irr: Various Coefficients of Interrater Reliability and Agreement, R Package Version 084; R Foundation for Statistical Computing: Vienna, Austria, 2012. [Google Scholar]
- Dudic, A.; Giannopoulou, C.; Leuzinger, M.; Kiliaridis, S. Detection of apical root resorption after orthodontic treatment by using panoramic radiography and cone-beam computed tomography of super-high resolution. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 434–437. [Google Scholar] [CrossRef] [PubMed]
- Creanga, A.G.; Geha, H.; Sankar, V.; Teixeira, F.B.; McMahan, C.A.; Noujeim, M. Accuracy of digital periapical radiography and cone-beam computed tomography in detecting external root resorption. Imaging Sci. Dent. 2015, 45, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Metz, C. Some practical issues of experimental design and data analysis in radiological ROC studies. Investig. Radiol. 1989, 24, 234–245. [Google Scholar] [CrossRef]
- Alfailany, D.T.; Shaweesh, A.I.; Hajeer, M.Y.; Brad, B.; Alhaffar, J.B. The diagnostic accuracy of cone-beam computed tomography and two-dimensional imaging methods in the 3D localization and assessment of maxillary impacted canines compared to the gold standard in-vivo readings: A cross-sectional study. Int. Orthod. 2023, 21, 100780. [Google Scholar] [CrossRef] [PubMed]
- Moreira-Souza, L.; Butini Oliveira, L.; Gaêta-Araujo, H.; Almeida-Marques, M.; Asprino, L.; Oenning, A.C. Comparison of CBCT and panoramic radiography for the assessment of bone loss and root resorption on the second molar associated with third molar impaction: A systematic review. Dentomaxillofac. Radiol. 2022, 51, 20210217. [Google Scholar] [CrossRef] [PubMed]
- Keerthana, G.; Singh, N.; Yadav, R.; Duhan, J.; Tewari, S.; Gupta, A.; Sangwan, P.; Mittal, S. Comparative analysis of the accuracy of periapical radiography and cone-beam computed tomography for diagnosing complex endodontic pathoses using a gold standard reference—A prospective clinical study. Int. Endod. J. 2021, 54, 1448–1461. [Google Scholar] [CrossRef]
- Kamburoǧlu, K.; Kurşun, Ş.; Yüksel, S.; Öztaş, B. Observer ability to detect ex vivo simulated internal or external cervical root resorption. J. Endod. 2011, 37, 168–175. [Google Scholar] [CrossRef]
- Li, Y.; Deng, S.; Mei, L.; Li, Z.; Zhang, X.; Yang, C.; Li, Y. Prevalence and severity of apical root resorption during orthodontic treatment with clear aligners and fixed appliances: A cone beam computed tomography study. Prog. Orthod. 2020, 21, 1. [Google Scholar] [CrossRef]
- Aras, I.; Unal, I.; Huniler, G.; Aras, A. Root resorption due to orthodontic treatment using self-ligating and conventional brackets: A cone-beam computed tomography study. J. Orofac. Orthop. 2018, 79, 181–190. [Google Scholar] [CrossRef]
- Bernardes, R.A.; de Paulo, R.S.; Pereira, L.O.; Duarte, M.A.H.; Ordinola-Zapata, R.; de Azevedo, J.R. Comparative study of cone beam computed tomography and intraoral periapical radiographs in diagnosis of lingual-simulated external root resorptions. Dent. Traumatol. 2012, 28, 268–272. [Google Scholar] [CrossRef]
- Ahangari, Z.; Nasser, M.; Mahdian, M.; Fedorowicz, Z.; Marchesan, M.A. Interventions for the management of external root resorption. Cochrane Database Syst. Rev. 2015, 2015, CD008003. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Present | Absent | |||
|---|---|---|---|---|
| Committee | ||||
| EARR | Definitely Present | Probably Present | Probably Absent | Definitely Absent |
| Examiners | ||||
| Teeth Groups | EARR Present n (%) | EARR not Present n (%) | n |
|---|---|---|---|
| maxillary and mandibular incisors | 159 (71%) | 65 (29%) | 224 |
| maxillary incisors only | 89 (74%) | 31 (26%) | 120 |
| mandibular incisors only | 70 (67%) | 34 (33%) | 104 |
| central incisors | 72 (67%) | 36 (33%) | 108 |
| lateral incisors | 87 (75%) | 29 (25%) | 116 |
| (A) | ||||||
| Teeth groups | Accuracy | Sensitivity | Specificity | PPV | NPV | |
| maxillary and mandibular incisors | PR | 0.60 (0.13) | 0.43 (0.19) | 0.99 (0.02) | 0.99 (0.09) | 0.43 (0.08) |
| CBCT | 0.59 (0.04) | 0.43 (0.05) | 0.99 (0.01) | 0.99 (0.01) | 0.42 (0.02) | |
| maxillary incisors only | PR | 0.69 (0.14) | 0.59 (0.20) | 0.98 (0.03) | 0.99 (0.01) | 0.48 (0.12) |
| CBCT | 0.67 (0.06) | 0.56 (0.07) | 0.98 (0.03) | 0.99 (0.02) | 0.44 (0.05) | |
| mandibular incisors only | PR | 0.49 (0.13) | 0.24 (0.19) | 1 (0.00) | 1 (0.00) | 0.40 (0.07) |
| CBCT | 0.50 (0.05) | 0.26 (0.08) | 0.99 (0.01) | 0.99 (0.03) | 0.49 (0.03) | |
| central incisors | PR | 0.63 (0.14) | 0.45 (0.22) | 0.99 (0.03) | 0.99 (0.02) | 0.49 (0.1) |
| CBCT | 0.64 (0.03) | 0.47 (0.04) | 0.99 (0.03) | 0.99 (0.03) | 0.48 (0.02) | |
| lateral incisors | PR | 0.56 (0.13) | 0.42 (0.17) | 1 (0.00) | 1 (0.00) | 0.37 (0.07) |
| CBCT | 0.55 (0.05) | 0.40 (0.07) | 0.99 (0.02) | 0.99 (0.01) | 0.36 (0.03) | |
| (B) | ||||||
| Teeth groups | Accuracy | Sensitivity | Specificity | PPV | NPV | |
| maxillary and mandibular incisors | PR | 0.82 (0.03) | 0.83 (0.08) | 0.79 (0.11) | 0.91 (0.04) | 0.67 (0.08) |
| CBCT | 0.88 (0.03) | 0.89 (0.05) | 0.84 (0.04) | 0.93 (0.01) | 0.78 (0.08) | |
| maxillary incisors only | PR | 0.77 (0.17) | 0.79 (0.29) | 0.73 (0.23) | 0.91 (0.07) | 0.69 (0.25) |
| CBCT | 0.93 (0.01) | 0.96 (0.03) | 0.85 (0.09) | 0.95 (0.03) | 0.87 (0.06) | |
| mandibular incisors only | PR | 0.77 (0.05) | 0.73 (0.12) | 0.87 (0.10) | 0.93 (0.05) | 0.62 (0.08) |
| CBCT | 0.83 (0.07) | 0.82 (0.10) | 0.84 (0.09) | 0.91 (0.04) | 0.71 (0.11) | |
| central incisors | PR | 0.79 (0.02) | 0.84 (0.07) | 0.71 (0.13) | 0.86 (0.05) | 0.70 (0.07) |
| CBCT | 0.88 (0.02) | 0.92 (0.03) | 0.82 (0.03) | 0.91 (0.02) | 0.84 (0.05) | |
| lateral incisors | PR | 0.84 (0.04) | 0.83 (0.08) | 0.90 (0.10) | 0.96 (0.03) | 0.65 (0.10) |
| CBCT | 0.78 (0.17) | 0.74 (0.26) | 0.90 (0.10) | 0.96 (0.03) | 0.60 (0.20) | |
| Teeth Groups | PR | CBCT | p-Value a |
|---|---|---|---|
| maxillary and mandibular incisors | 0.87 (0.02) | 0.90 (0.01) | 0.294, 0.228, 0.199, 0.436 |
| maxillary incisors only | 0.91 (0.01) | 0.94 (0.03) | 0.072, 0.523, 0.131, 0.361 |
| mandibular incisors only | 0.83 (0.02) | 0.86 (0.05) | 0.747, 0.012, 0.671, 0.803 |
| central incisors | 0.85 (0.02) | 0.91 (0.02) | 0.074, 0.281, 0.151, 0.189 |
| lateral incisors | 0.91 (0.02) | 0.91 (0.02) | 0.745, 0.430, 0.729, 0.476 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, S.A.; Corte-Real, A.; Melo, A.; Magalhães, L.; Lavado, N.; Santos, J.M. Diagnostic Accuracy of Cone Beam Computed Tomography and Periapical Radiography for Detecting Apical Root Resorption in Retention Phase of Orthodontic Patients: A Cross-Sectional Study. J. Clin. Med. 2024, 13, 1248. https://doi.org/10.3390/jcm13051248
Pereira SA, Corte-Real A, Melo A, Magalhães L, Lavado N, Santos JM. Diagnostic Accuracy of Cone Beam Computed Tomography and Periapical Radiography for Detecting Apical Root Resorption in Retention Phase of Orthodontic Patients: A Cross-Sectional Study. Journal of Clinical Medicine. 2024; 13(5):1248. https://doi.org/10.3390/jcm13051248
Chicago/Turabian StylePereira, Sónia A., Ana Corte-Real, Ana Melo, Linda Magalhães, Nuno Lavado, and João Miguel Santos. 2024. "Diagnostic Accuracy of Cone Beam Computed Tomography and Periapical Radiography for Detecting Apical Root Resorption in Retention Phase of Orthodontic Patients: A Cross-Sectional Study" Journal of Clinical Medicine 13, no. 5: 1248. https://doi.org/10.3390/jcm13051248