
Early-Onset Colorectal Cancer: Are Neuroendocrine Tumors or Adenocarcinomas the Culprit? Analysis of the Largest U.S. Cancer Incidence Database, 2001–2020
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Early-Onset CRC Incidence Stratified by Histopathology
3.2. Early-Onset CRC Incidence Stratified by Histopathology and Sex
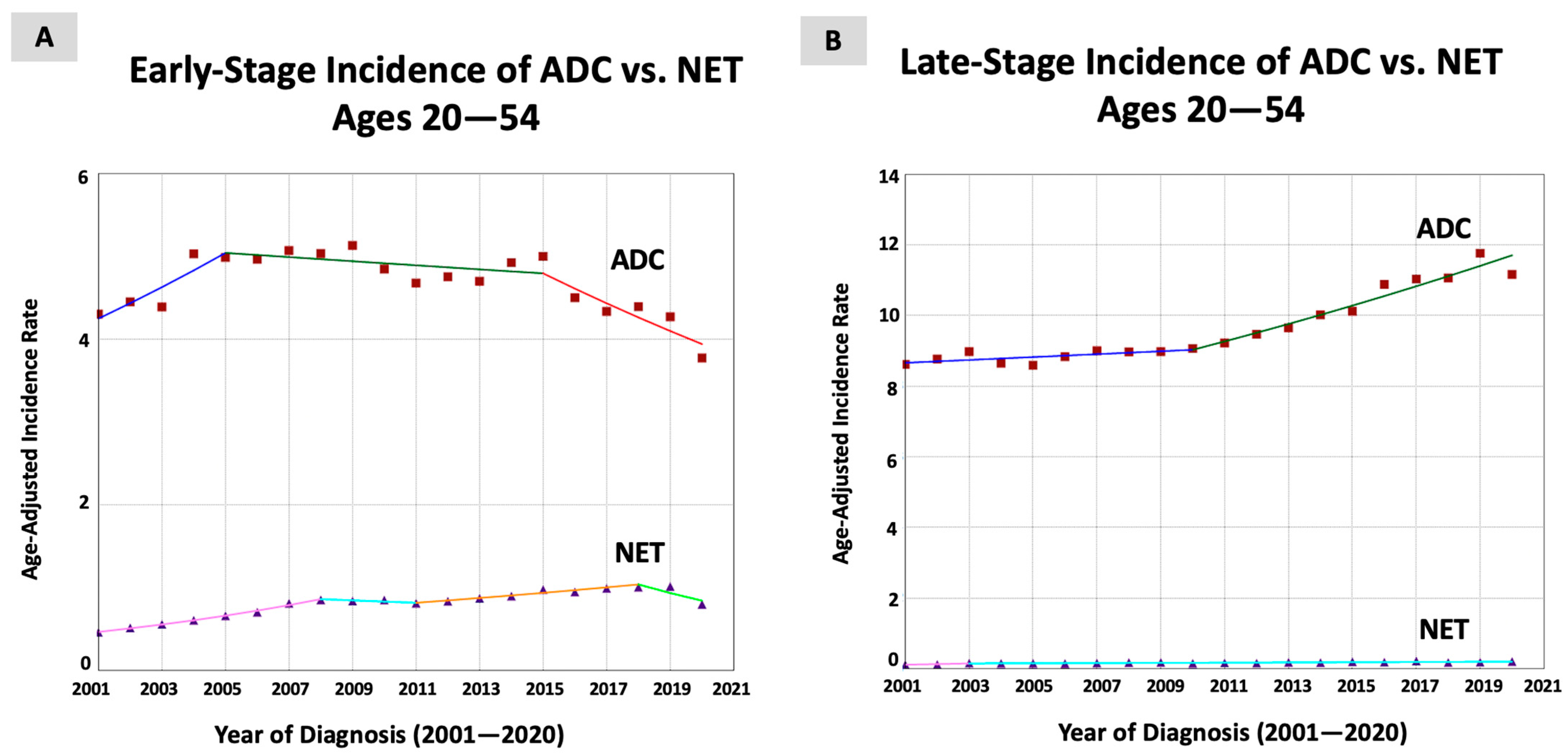
3.3. Early-Onset CRC Incidence Stratified by Histopathology and Stage at Diagnosis
3.4. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 2 January 2024).
- Morgan, E.; Arnold, M.; Gini, A.; Lorenzoni, V.; Cabasag, C.J.; Laversanne, M.; Vignat, J.; Ferlay, J.; Murphy, N.; Bray, F. Global burden of colorectal cancer in 2020 and 2040: Incidence and mortality estimates from GLOBOCAN. Gut 2023, 72, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.L.; Wike, J.M.; Kato, I.; Lewis, D.R.; Michaud, F. A population-based study of colorectal cancer histology in the United States, 1998–2001. Cancer 2006, 107, 1128–1141. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.S.; Huang, J.; Lok, V.; Wang, J.; Fung, F.; Ding, H.; Zheng, Z.J. Differences in Incidence and Mortality Trends of Colorectal Cancer Worldwide Based on Sex, Age, and Anatomic Location. Clin. Gastroenterol. Hepatol. 2021, 19, 955–966.e61. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, T.; Ruszkowska, M.; Danielewicz, A.; Niedźwiedzka, E.; Arłukowicz, T.; Przybyłowicz, K.E. A Review of Colorectal Cancer in Terms of Epidemiology, Risk Factors, Development, Symptoms and Diagnosis. Cancers 2021, 13, 2025. [Google Scholar] [CrossRef] [PubMed]
- Douaiher, J.; Ravipati, A.; Grams, B.; Chowdhury, S.; Alatise, O.; Are, C. Colorectal cancer-global burden, trends, and geographical variations. J. Surg. Oncol. 2017, 115, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Fedewa, S.A.; Anderson, W.F.; Miller, K.D.; Ma, J.; Rosenberg, P.S.; Jemal, A. Colorectal Cancer Incidence Patterns in the United States, 1974–2013. J. Natl. Cancer Inst. 2017, 109, djw322. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, A.B.; Rutter, C.M.; Peterse, E.F.P.; Lietz, A.P.; Seguin, C.L.; Meester, R.G.S.; Perdue, L.A.; Lin, J.S.; Siegel, R.L.; Doria-Rose, V.P.; et al. U.S. Preventive Services Task Force Evidence Syntheses, formerly Systematic Evidence Reviews. In Colorectal Cancer Screening: An Updated Decision Analysis for the U.S. Preventive Services Task Force; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2021. [Google Scholar]
- Montminy, E.M.; Zhou, M.; Maniscalco, L.; Abualkhair, W.; Kim, M.K.; Siegel, R.L.; Wu, X.C.; Itzkowitz, S.H.; Karlitz, J.J. Contributions of Adenocarcinoma and Carcinoid Tumors to Early-Onset Colorectal Cancer Incidence Rates in the United States. Ann. Intern. Med. 2021, 174, 157–166. [Google Scholar] [CrossRef]
- Zaborowski, A.M.; Abdile, A.; Adamina, M.; Aigner, F.; d’Allens, L.; Allmer, C.; Álvarez, A.; Anula, R.; Andric, M.; Atallah, S.; et al. Characteristics of Early-Onset vs Late-Onset Colorectal Cancer: A Review. JAMA Surg. 2021, 156, 865–874. [Google Scholar] [CrossRef]
- Sinicrope, F.A. Increasing Incidence of Early-Onset Colorectal Cancer. N. Engl. J. Med. 2022, 386, 1547–1558. [Google Scholar] [CrossRef]
- Mauri, G.; Sartore-Bianchi, A.; Russo, A.G.; Marsoni, S.; Bardelli, A.; Siena, S. Early-onset colorectal cancer in young individuals. Mol. Oncol. 2019, 13, 109–131. [Google Scholar] [CrossRef]
- Saraiva, M.R.; Rosa, I.; Claro, I. Early-onset colorectal cancer: A review of current knowledge. World J. Gastroenterol. 2023, 29, 1289–1303. [Google Scholar] [CrossRef] [PubMed]
- Ullah, F.; Pillai, A.B.; Omar, N.; Dima, D.; Harichand, S. Early-Onset Colorectal Cancer: Current Insights. Cancers 2023, 15, 3202. [Google Scholar] [CrossRef] [PubMed]
- Silla, I.O.; Rueda, D.; Rodríguez, Y.; García, J.L.; de la Cruz Vigo, F.; Perea, J. Early-onset colorectal cancer: A separate subset of colorectal cancer. World J. Gastroenterol. 2014, 20, 17288–17296. [Google Scholar] [CrossRef]
- Stigliano, V.; Sanchez-Mete, L.; Martayan, A.; Anti, M. Early-onset colorectal cancer: A sporadic or inherited disease? World J. Gastroenterol. 2014, 20, 12420–12430. [Google Scholar] [CrossRef]
- Tsikitis, V.L.; Wertheim, B.C.; Guerrero, M.A. Trends of incidence and survival of gastrointestinal neuroendocrine tumors in the United States: A seer analysis. J. Cancer 2012, 3, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Kooyker, A.I.; Verbeek, W.H.; van den Berg, J.G.; Tesselaar, M.E.; van Leerdam, M.E. Change in incidence, characteristics and management of colorectal neuroendocrine tumours in the Netherlands in the last decade. United Eur. Gastroenterol. J. 2020, 8, 59–67. [Google Scholar] [CrossRef]
- Warsinggih; Liliyanto; Prihantono; Ariani, G.D.W.; Faruk, M. Colorectal neuroendocrine tumors: A case series. Int. J. Surg. Case Rep. 2020, 72, 411–417. [Google Scholar] [CrossRef]
- Maione, F.; Chini, A.; Milone, M.; Gennarelli, N.; Manigrasso, M.; Maione, R.; Cassese, G.; Pagano, G.; Tropeano, F.P.; Luglio, G.; et al. Diagnosis and Management of Rectal Neuroendocrine Tumors (NETs). Diagnostics 2021, 11, 771. [Google Scholar] [CrossRef]
- National Program of Cancer Registries and Surveillance EaERPSSDNaSI-USCSPURD, 2022 Submission (2001–2020). United States Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute. Released June 2023. Available online: www.cdc.gov/cancer/uscs/public-use (accessed on 2 January 2024).
- Software and Tools for Cancer Registries and Surveillance. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/cancer/npcr/tools/index.htm (accessed on 2 January 2024).
- Siegel, R.L.; Miller, K.D.; Jemal, A. Colorectal Cancer Mortality Rates in Adults Aged 20 to 54 Years in the United States, 1970–2014. Jama 2017, 318, 572–574. [Google Scholar] [CrossRef]
- Kim, H.J.; Yu, B.; Feuer, E.J. Selecting the number of change-points in segmented line regression. Stat. Sin. 2009, 19, 597–609. [Google Scholar]
- Kim, J.; Kim, H.J. Consistent Model Selection in Segmented Line Regression. J. Stat. Plan. Inference 2016, 170, 106–116. [Google Scholar] [CrossRef]
- Statistical Research and Applications Branch NCI. Joinpoint Regression Program, VM. 2021. Available online: https://surveillance.cancer.gov/joinpoint/ (accessed on 2 January 2024).
- Kim, H.J.; Fay, M.P.; Yu, B.; Barrett, M.J.; Feuer, E.J. Comparability of segmented line regression models. Biometrics 2004, 60, 1005–1014. [Google Scholar] [CrossRef]
- Lumsdaine, C.T.; Liu-Smith, F.; Li, X.; Zell, J.A.; Lu, Y. Increased incidence of early onset colorectal adenocarcinoma is accompanied by an increased incidence of rectal neuroendocrine tumors. Am. J. Cancer Res. 2020, 10, 1888–1899. [Google Scholar] [PubMed]
- Shafqat, H.; Ali, S.; Salhab, M.; Olszewski, A.J. Survival of patients with neuroendocrine carcinoma of the colon and rectum: A population-based analysis. Dis. Colon Rectum 2015, 58, 294–303. [Google Scholar] [CrossRef] [PubMed]
- Anthony, L.B.; Strosberg, J.R.; Klimstra, D.S.; Maples, W.J.; O’Dorisio, T.M.; Warner, R.R.; Wiseman, G.A.; Benson, A.B., 3rd; Pommier, R.F. The NANETS consensus guidelines for the diagnosis and management of gastrointestinal neuroendocrine tumors (nets): Well-differentiated nets of the distal colon and rectum. Pancreas 2010, 39, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Petrick, J.L.; Barber, L.E.; Warren Andersen, S.; Florio, A.A.; Palmer, J.R.; Rosenberg, L. Racial Disparities and Sex Differences in Early- and Late-Onset Colorectal Cancer Incidence, 2001–2018. Front. Oncol. 2021, 11, 734998. [Google Scholar] [CrossRef]
- Gausman, V.; Dornblaser, D.; Anand, S.; Hayes, R.B.; O’Connell, K.; Du, M.; Liang, P.S. Risk Factors Associated With Early-Onset Colorectal Cancer. Clin. Gastroenterol. Hepatol. 2020, 18, 2752–2759. [Google Scholar] [CrossRef]
- Porter, M.G.; Stoeger, S.M. Atypical Colorectal Neoplasms. Surg. Clin. N. Am. 2017, 97, 641–656. [Google Scholar] [CrossRef]
- Prabhakaran, S.; Kong, J.C.; Williams, E.; Bell, S.; Warrier, S.; Simpson, P.; Chin, M.; Skinner, S.; Carne, P. Comparison of colorectal cancer outcomes in young adults and octogenarians. Am. J. Surg. 2022, 223, 951–956. [Google Scholar] [CrossRef]
- Hassan, M.M.; Phan, A.; Li, D.; Dagohoy, C.G.; Leary, C.; Yao, J.C. Risk factors associated with neuroendocrine tumors: A U.S.-based case-control study. Int. J. Cancer 2008, 123, 867–873. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.S.; Yun, K.E.; Chang, Y.; Ryu, S.; Park, J.H.; Kim, H.J.; Cho, Y.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I.; et al. Risk factors associated with rectal neuroendocrine tumors: A cross-sectional study. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 1406–1413. [Google Scholar] [CrossRef]
- Giannakis, M.; Ng, K. A common cancer at an uncommon age. Science 2023, 379, 1088–1090. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Medhanie, G.A.; Fedewa, S.A.; Jemal, A. State Variation in Early-Onset Colorectal Cancer in the United States, 1995–2015. J. Natl. Cancer Inst. 2019, 111, 1104–1106. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.R.; Millien, V.O.; da Costa, W.L., Jr.; Oluyomi, A.O.; Gould Suarez, M.; Thrift, A.P. Trends in the incidence of early-onset colorectal cancer in all 50 United States from 2001 through 2017. Cancer 2022, 128, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Torre, L.A.; Soerjomataram, I.; Hayes, R.B.; Bray, F.; Weber, T.K.; Jemal, A. Global patterns and trends in colorectal cancer incidence in young adults. Gut 2019, 68, 2179–2185. [Google Scholar] [CrossRef] [PubMed]
- Cope, J.; Srirajaskanthan, R. Rectal Neuroendocrine Neoplasms: Why Is There a Global Variation? Curr. Oncol. Rep. 2022, 24, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Barthold, D.; Yeung, K.; Lieberman, D.; Fendrick, A.M. Comparison of Screening Colonoscopy Rates After Positive Noninvasive Testing for Colorectal Cancer in States with and without Cost-Sharing. JAMA Netw. Open 2022, 5, e2216910. [Google Scholar] [CrossRef] [PubMed]
- Gillis, D.; Edwards, B.P.M. The utility of joinpoint regression for estimating population parameters given changes in population structure. Heliyon 2019, 5, e02515. [Google Scholar] [CrossRef]
- Park, H.S.; Lloyd, S.; Decker, R.H.; Wilson, L.D.; Yu, J.B. Limitations and biases of the Surveillance, Epidemiology, and End Results database. Curr. Probl. Cancer 2012, 36, 216–224. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Histopathological Subtype | Early-Onset CRC Cases (N = 514,875) a | Trends b | Sex-Specific AAPC Difference (95% CI) c | Pairwise Comparison p-Values | ||||
|---|---|---|---|---|---|---|---|---|
| Time Period | APC (95% CI) | AAPC (95% CI) | Sex-Specific AAPC Difference | Coincidence d | Parallelism e | |||
| Both Sexes | ||||||||
| ADC | 448,670 (87.1%) | 2001–2020 | 0.91 * (0.73 to 1.10) | 0.91 * (0.73 to 1.10) | −1.73 * (−2.99 to −0.48) | 0.01 | <0.001 | <0.001 |
| NET | 36,205 (7.0%) | 2001–2008 | 7.32 * (6.19 to 8.47) | 2.65 * (1.41 to 3.90) | ||||
| 2008–2011 | −1.98 (−8.38 to 4.88) | |||||||
| 2011–2018 | 3.85 * (2.72 to 4.99) | |||||||
| 2018–2020 | −9.62 * (−15.50 to −3.32) | |||||||
| Males | ||||||||
| ADC | 247,526 (48.1%) | 2001–2012 | 0.61 * (0.34 to 0.89) | 0.85 * (0.39 to 1.32) | −1.81 * (−3.49 to −0.13) | 0.03 | <0.001 | <0.001 |
| 2012–2018 | 2.19 * (1.31 to 3.07) | |||||||
| 2018–2020 | −1.78 (−5.47 to 2.05) | |||||||
| NET | 17,452 (3.4%) | 2001–2008 | 7.32 * (5.85 to 8.81) | 2.67 * (1.06 to 4.29) | ||||
| 2008–2011 | −2.23 (−10.46 to 6.76) | |||||||
| 2011–2018 | 4.21 * (2.75 to 5.70) | |||||||
| 2018–2020 | −10.23 * (−17.70 to −2.81) | |||||||
| Females | ||||||||
| ADC | 201,144 (39.1%) | 2001–2020 | 0.71 * (0.52 to 0.90) | 0.71 * (0.52 to 0.90) | −2.03 (−4.20 to 0.14) | 0.06 | <0.001 | <0.001 |
| NET | 18,753 (3.6%) | 2001–2008 | 7.37 * (5.32 to 9.45) | 2.74 * (0.60 to 4.93) | ||||
| 2008–2011 | −2.26 (−13.52 to 10.47) | |||||||
| 2011–2017 | 4.31 * (1.55 to 7.14) | |||||||
| 2017–2020 | −5.45 (−11.08 to 0.54) | |||||||
| Histopathological Subtype | Early-Onset CRC Cases (N = 514,875) a | Trends b | Sex-Specific AAPC Difference (95% CI) c | Pairwise Comparison p-Values | ||||
|---|---|---|---|---|---|---|---|---|
| Time Period | APC (95% CI) | AAPC (95% CI) | Sex-Specific AAPC Difference | Coincidence d | Parallelism e | |||
| Early Stage | ||||||||
| ADC | 144,130 (28.0%) | 2001–2005 | 4.37 * (0.78 to 8.10) | −0.39 (−1.40 to 0.62) | −3.56 * (−5.20 to −1.92) | <0.001 | <0.001 | <0.001 |
| 2005–2015 | −0.50 (−1.45 to 0.45) | |||||||
| 2015–2020 | −3.84 * (−6.31 to −1.31) | |||||||
| NET | 24,845 (4.8%) | 2001–2008 | 9.18 * (7.95 to 10.41) | 3.17 * (1.88 to 4.47) | ||||
| 2008–2011 | −1.74 (−8.32 to 5.32) | |||||||
| 2011–2018 | 3.48 * (2.31 to 4.67) | |||||||
| 2018–2020 | −9.92 * (−16.01 to −3.40) | |||||||
| Late Stage | ||||||||
| ADC | 289,826 (56.3%) | 2001–2010 | 0.46 (−1.17 to 1.10) | 1.60 * (1.23 to 1.97) | −1.43 (−4.14 to 1.29) | 0.30 | <0.001 | 0.41 |
| 2010–2020 | 2.63 * (2.12 to 3.14) | |||||||
| NET | 5140 (1.0%) | 2001–2003 | 15.15 (−11.38 to 49.63) | 3.02 * (0.37 to 5.75) | ||||
| 2003–2020 | 1.68 * (0.93 to 2.45) | |||||||
| Histopathological Subtype | Early-Onset CRC Cases (N = 514,875) a | Trends b | Sex-Specific AAPC Difference (95% CI) c | Pairwise Comparison p-Values | ||||
|---|---|---|---|---|---|---|---|---|
| Time Period | APC (95% CI) | AAPC (95% CI) | Sex-Specific AAPC Difference | Coincidence d | Parallelism e | |||
| Microscopically Confirmed Cases | ||||||||
| ADC | 447,664 (86.9%) | 2001–2020 | 0.91 * (0.73 to 1.09) | 0.91 * (0.73 to 1.09) | −1.72 * (−2.98 to −0.46) | 0.007 | <0.001 | <0.001 |
| NET | 36,089 (7.0%) | 2001–2008 | 7.31 * (6.17 to 8.46) | 2.63 * (1.39 to 3.89) | ||||
| 2008–2011 | −1.94 (−8.39 to 4.95) | |||||||
| 2011–2018 | 3.84 * (2.71 to 4.99) | |||||||
| 2018–2020 | −9.77 * (−15.68 to −3.44) | |||||||
| Study | Current Study | Montminy et al. [9] | Lumsdaine et al. [28] | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Database | USCS (covers ~98% of U.S. population) | SEER 18 (covers ~27.8% of U.S. population) | SEER 13 (covers ~13.4% of U.S. population) | ||||||
| Time period | 2001–2020 | 2000–2016 | 1992–2015 | ||||||
| Sample size | 514,875 | 119,624 | 426,262 | ||||||
| APC: ADC (95% CI) | Ages 20–54 | 2001–2020 | 0.91 * (0.73–1.09) | Ages 20–29 | 2000–2005 | 5.6 * (0.5–11.1) | Ages 20–44 # | 1992–2015 | 2.4 * (1.9–2.8) |
| 2005–2016 | −0.30 (−1.7–1.1) | ||||||||
| Ages 30–39 | 2000–2016 | 1.6 * (1.2–2.0) | |||||||
| Ages 40–49 | 0.9 * (0.7–1.2) | Ages 45–54 # | 1.0 * (0.7–1.3) | ||||||
| Ages 50–54 | 0.2 (−0.1–0.5) | ||||||||
| APC: NET (95% CI) | Ages 20–54 | 2001–2008 | 7.31 * (6.17–8.46) | Ages 20–29 | 2000–2016 | 4.3 * (1.9–6.8) | Ages 20–44 # | 1992–1995 | −13 (−26.9–3.6) |
| 2008–2011 | −1.94 (−8.39–4.95) | Ages 30–39 | 2.4 * (1.0–4.0) | 2001–2015 | 2.2 * (0.5–2.8) | ||||
| 2011–2018 | 3.84 * (2.71–4.99) | Ages 40–49 | 2.5 * (1.4–3.6) | Ages 45–54 # | 1992–1994 | −6.1 (−25.7–18.7) | |||
| 2018–2020 | −9.77 * (−15.68–−3.44) | Ages 50–54 | 2000–2007 | 2.4 * (0.4–4.4) | 1994–2007 | 10.6 * (9.1–12.2) | |||
| 2007–2016 | 10.6 * (6.2–15.2) | 2007–2015 | 2.2 (−0.3–4.8) | ||||||
| AAPC: ADC (95% CI) | Ages 20–54 | 2001–2020 | 0.91 * (0.73–1.09) | Ages 20–29 | 2000–2016 | Not calculated/provided | Ages 20–44 # | 1992–2015 | 2.4 * (1.9–2.8) |
| Ages 30–39 | 1.6 * (1.2–2.0) | ||||||||
| Ages 40–49 | 0.9 * (0.7–1.2) | Ages 45–54 # | 1.0 * (0.7–1.3) | ||||||
| Ages 50–54 | 0.2 (−0.1–0.5) | ||||||||
| AAPC: NET (95% CI) | Ages 20–54 | 2001–2020 | 2.63 * (1.39–3.89) | Ages 20–29 | 2000–2016 | 4.3 * (1.9–6.8) | Ages 20–44 # | 1992–2015 | 2.9 (−0.1–6.0) |
| Ages 30–39 | 2.4 * (1.0–4.0) | ||||||||
| Ages 40–49 | 2.5 * (1.4–3.6) | Ages 45–54 # | 6.1 * (3.8–8.4) | ||||||
| Ages 50–54 | Not calculated/provided | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abboud, Y.; Fraser, M.; Qureshi, I.; Hajifathalian, K. Early-Onset Colorectal Cancer: Are Neuroendocrine Tumors or Adenocarcinomas the Culprit? Analysis of the Largest U.S. Cancer Incidence Database, 2001–2020. J. Clin. Med. 2024, 13, 1098. https://doi.org/10.3390/jcm13041098
Abboud Y, Fraser M, Qureshi I, Hajifathalian K. Early-Onset Colorectal Cancer: Are Neuroendocrine Tumors or Adenocarcinomas the Culprit? Analysis of the Largest U.S. Cancer Incidence Database, 2001–2020. Journal of Clinical Medicine. 2024; 13(4):1098. https://doi.org/10.3390/jcm13041098
Chicago/Turabian StyleAbboud, Yazan, Madison Fraser, Imran Qureshi, and Kaveh Hajifathalian. 2024. "Early-Onset Colorectal Cancer: Are Neuroendocrine Tumors or Adenocarcinomas the Culprit? Analysis of the Largest U.S. Cancer Incidence Database, 2001–2020" Journal of Clinical Medicine 13, no. 4: 1098. https://doi.org/10.3390/jcm13041098