
Calculating Tumor Volume Using Three-Dimensional Models in Preoperative Soft-Tissue Sarcoma Surgical Planning: Does Size Matter?
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
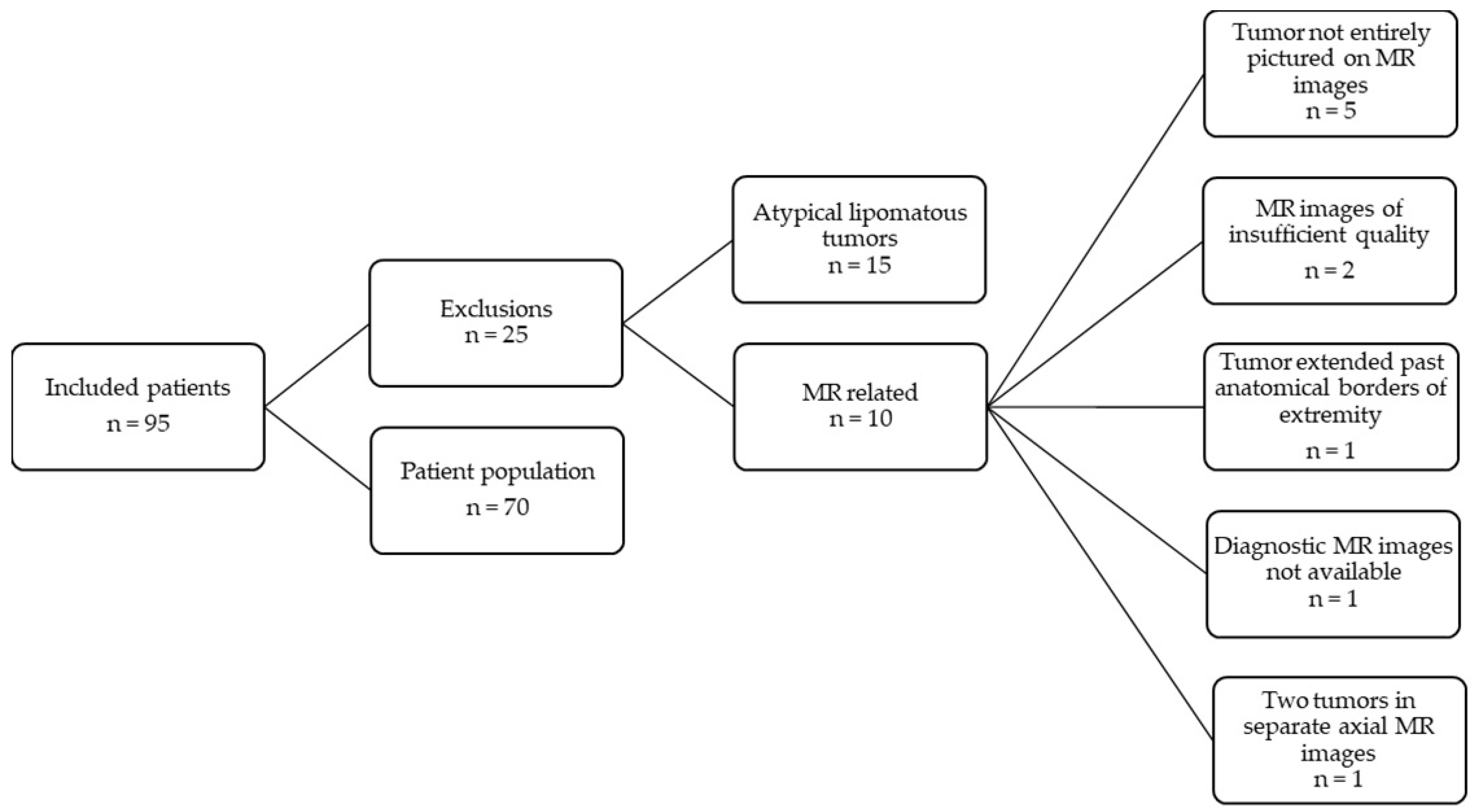
3.1. Population
3.2. Patient, Tumor and Treatment Characteristics
3.3. Three-Dimensional Virtual Surgical Planning: Tumor Volume
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gronchi, A.; Miah, A.B.; Dei Tos, A.P.; Abecassis, N.; Bajpai, J.; Bauer, S.; Biagini, R.; Bielack, S.; Blay, J.Y.; Bolle, S.; et al. Soft Tissue and Visceral Sarcomas: ESMO–EURACAN–GENTURIS Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up☆. Ann. Oncol. 2021, 32, 1348–1365. [Google Scholar] [CrossRef]
- Vilanova, J.C. WHO Classification of Soft Tissue Tumors. In WHO Classification of Soft Tissue Tumors; Springer: Berlin/Heidelberg, Germany, 2017; pp. 187–196. ISBN 9783319466798. [Google Scholar]
- Dutch Cancer Registration Incidence of Sarcomas. Available online: https://iknl.nl/kankersoorten/bot-en-wekedelenkanker/registratie/incidentie (accessed on 10 June 2021).
- Hoekstra, H.J.; Haas, R.L.M.; Verhoef, C.; Suurmeijer, A.J.H.; van Rijswijk, C.S.P.; Bongers, B.G.H.; van der Graaf, W.T.; Ho, V.K.Y. Adherence to Guidelines for Adult (Non-GIST) Soft Tissue Sarcoma in the Netherlands: A Plea for Dedicated Sarcoma Centers. Ann. Surg. Oncol. 2017, 24, 3279–3288. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, N.F.; Cannon, C.P.; Lin, P.P.; Lewis, V.O. Soft-Tissue Sarcoma. J. Am. Acad. Orthop. Surg. 2009, 17, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Holzapfel, K.; Regler, J.; Baum, T.; Rechl, H.; Specht, K.; Haller, B.; Von Eisenhart-Rothe, R.; Gradinger, R.; Rummeny, E.J.; Woertler, K. Local Staging of Soft-Tissue Sarcoma: Emphasis on Assessment of Neurovascular Encasement-Value of MR Imaging in 174 Confirmed Cases. Radiology 2015, 275, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Casali, P.G.; Abecassis, N.; Aro, H.T.; Bauer, S.; Biagini, R.; Bielack, S.; Bonvalot, S.; Boukovinas, I.; Bovee, J.V.M.G.; Brodowicz, T.; et al. Soft Tissue and Visceral Sarcomas: ESMO-EURACAN Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2018, 29, iv268–iv269. [Google Scholar] [CrossRef] [PubMed]
- Lupton, K.; Salins, M.; Pass, B.; Negi, R.; Gupta, H. Imaging Recommendations for Diagnosis, Staging, and Management of Soft Tissue Sarcomas. Indian J. Med. Paediatr. Oncol. 2023, 44, 261–267. [Google Scholar] [CrossRef]
- Noebauer-Huhmann, I.M.; Weber, M.A.; Lalam, R.K.; Trattnig, S.; Bohndorf, K.; Vanhoenacker, F.; Tagliafico, A.; Van Rijswijk, C.; Vilanova, J.C.; Afonso, P.D.; et al. Erratum: Soft Tissue Tumors in Adults: ESSR-Approved Guidelines for Diagnostic Imaging. Semin. Musculoskelet. Radiol. 2015, 19, 475–482. [Google Scholar] [CrossRef]
- Crombé, A.; Kind, M.; Fadli, D.; Miceli, M.; Linck, P.A.; Bianchi, G.; Sambri, A.; Spinnato, P. Soft-Tissue Sarcoma in Adults: Imaging Appearances, Pitfalls and Diagnostic Algorithms. Diagn. Interv. Imaging 2023, 104, 207–220. [Google Scholar] [CrossRef]
- Sedaghat, S.; Ravesh, M.S.; Sedaghat, M.; Both, M.; Jansen, O. Configuration of Soft-Tissue Sarcoma on MRI Correlates with Grade of Malignancy. Radiol. Oncol. 2021, 55, 158–163. [Google Scholar] [CrossRef]
- Sedaghat, S.; Sedaghat, M.; Meschede, J.; Jansen, O.; Both, M. Diagnostic Value of MRI for Detecting Recurrent Soft-Tissue Sarcoma in a Long-Term Analysis at a Multidisciplinary Sarcoma Center. BMC Cancer 2021, 21, 398. [Google Scholar] [CrossRef]
- O’Sullivan, B.; Davis, A.M.; Turcotte, R.; Bell, R.; Catton, C.; Chabot, P.; Wunder, J.; Kandel, R.; Goddard, K.; Sadura, A.; et al. Preoperative versus Postoperative Radiotherapy in Soft-Tissue Sarcoma of the Limbs: A Randomised Trial. Lancet 2002, 359, 2235–2241. [Google Scholar] [CrossRef]
- Albertsmeier, M.; Rauch, A.; Roeder, F.; Hasenhütl, S.; Pratschke, S.; Kirschneck, M.; Gronchi, A.; Jebsen, N.L.; Cassier, P.A.; Sargos, P.; et al. External Beam Radiation Therapy for Resectable Soft Tissue Sarcoma: A Systematic Review and Meta-Analysis. Ann. Surg. Oncol. 2018, 25, 754–767. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, M.G.; Seinen, J.M.; Pras, E.; Brouwers, A.H.; van Ginkel, R.J.; van Leeuwen, B.L.; Suurmeijer, A.J.H.; Been, L.B.; Hoekstra, H.J. Hyperthermic Isolated Limb Perfusion, Preoperative Radiotherapy, and Surgery (PRS) a New Limb Saving Treatment Strategy for Locally Advanced Sarcomas. J. Surg. Oncol. 2018, 117, 1447–1454. [Google Scholar] [CrossRef]
- Stevenson, M.G.; Ubbels, J.F.; Slump, J.; Huijing, M.A.; Bastiaannet, E.; Pras, E.; Hoekstra, H.J.; Been, L.B. Identification of Predictors for Wound Complications Following Preoperative or Postoperative Radiotherapy in Extremity Soft Tissue Sarcoma. Eur. J. Surg. Oncol. 2018, 44, 816–822. [Google Scholar] [CrossRef]
- Felderhof, J.M.; Creutzberg, C.L.; Putter, H.; Nout, R.A.; Bovée, J.V.M.G.; Dijkstra, P.D.S.; Hartgrink, H.H.; Marijnen, C.A.M. Long-Term Clinical Outcome of Patients with Soft Tissue Sarcomas Treated with Limb-Sparing Surgery and Postoperative Radiotherapy. Acta Oncol. 2013, 52, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Slump, J.; Bastiaannet, E.; Halka, A.; Hoekstra, H.J.; Ferguson, P.C.; Wunder, J.S.; Hofer, S.O.P.; O’Neill, A.C. Risk Factors for Postoperative Wound Complications after Extremity Soft Tissue Sarcoma Resection: A Systematic Review and Meta-Analyses. J. Plast. Reconstr. Aesthetic Surg. 2019, 72, 1449–1464. [Google Scholar] [CrossRef] [PubMed]
- Dutch Cancer Registration: Survival of Extremity Soft-Tissue Sarcomas in the Netherlands from 1989–2015. Available online: http://iknl.nhttps://iknl.nl/kankersoorten/bot-en-wekedelenkanker/registratie/overlevingl (accessed on 18 October 2023).
- Zagars, G.K.; Ballo, M.T.; Pisters, P.W.T.; Pollock, R.E.; Patel, S.R.; Benjamin, R.S.; Evans, H.L. Prognostic Factors for Patients with Localized Soft-Tissue Sarcoma Treated with Conservation Surgery and Radiation Therapy: An Analysis of 1225 Patients. Cancer 2003, 97, 2530–2543. [Google Scholar] [CrossRef] [PubMed]
- Slump, J.; Hofer, S.O.P.; Ferguson, P.C.; Wunder, J.S.; Griffin, A.M.; Hoekstra, H.J.; Bastiaannet, E.; O’Neill, A.C. Flap Reconstruction Does Not Increase Complication Rates Following Surgical Resection of Extremity Soft Tissue Sarcoma. Eur. J. Surg. Oncol. 2018, 44, 251–259. [Google Scholar] [CrossRef]
- Lohman, R.F.; Nabawi, A.S.; Reece, G.P.; Pollock, R.E.; Evans, G.R.D. Soft Tissue Sarcoma of the Upper Extremity: A 5-Year Experience at Two Institutions Emphasizing the Role of Soft Tissue Flap Reconstruction. Cancer 2002, 94, 2256–2264. [Google Scholar] [CrossRef]
- Elswick, S.M.; Wu, P.; Arkhavan, A.A.; Molinar, V.E.; Mohan, A.T.; Sim, F.H.; Martinez-Jorge, J.; Saint-Cyr, M. A Reconstructive Algorithm after Thigh Soft Tissue Sarcoma Resection Including Predictors of Free Flap Reconstruction✰. J. Plast. Reconstr. Aesthetic Surg. 2019, 72, 1304–1315. [Google Scholar] [CrossRef] [PubMed]
- Heller, L.; Kronowitz, S.J. Lower Extremity Reconstruction. J. Surg. Oncol. 2006, 94, 479–489. [Google Scholar] [CrossRef]
- Slump, J.; Ferguson, P.C.; Wunder, J.S.; Griffin, A.M.; Hoekstra, H.J.; Liu, X.; Hofer, S.O.P.; O’Neill, A.C. Patient, Tumour and Treatment Factors Affect Complication Rates in Soft Tissue Sarcoma Flap Reconstruction in a Synergistic Manner. Eur. J. Surg. Oncol. 2017, 43, 1126–1133. [Google Scholar] [CrossRef]
- Abouarab, M.H.; Salem, I.L.; Degheidy, M.M.; Henn, D.; Hirche, C.; Eweida, A.; Uhl, M.; Kneser, U.; Kremer, T. Therapeutic Options and Postoperative Wound Complications after Extremity Soft Tissue Sarcoma Resection and Postoperative External Beam Radiotherapy. Int. Wound J. 2018, 15, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, N.; Wan, D.; Bryan, Z.; Boehmler, J.; Miller, M.; Tiwari, P. Outcomes Analysis of the Role of Plastic Surgery in Extremity Sarcoma Treatment. J. Reconstr. Microsurg. 2013, 29, 107–112. [Google Scholar] [CrossRef]
- Slump, J.; Hofer, S.O.P.; Ferguson, P.C.; Wunder, J.S.; Griffin, A.M.; Hoekstra, H.J.; Bastiaannet, E.; O’Neill, A.C. Flap Choice Does Not Affect Complication Rates or Functional Outcomes Following Extremity Soft Tissue Sarcoma Reconstruction. J. Plast. Reconstr. Aesthetic Surg. 2018, 71, 989–996. [Google Scholar] [CrossRef]
- Bolliger, M.; Kroehnert, J.A.; Molineus, F.; Kandioler, D.; Schindl, M.; Riss, P. Experiences with the Standardized Classification of Surgical Complications (Clavien-Dindo) in General Surgery Patients. Eur. Surg. 2018, 50, 256–261. [Google Scholar] [CrossRef]
- Suresh, V.; Gao, J.; Jung, S.-H.; Brigman, B.; Eward, W.; Erdmann, D. The Role of Reconstructive Surgery After Skeletal and Soft Tissue Sarcoma Resection. Ann. Plast. Surg. 2018, 80, S372–S376. [Google Scholar] [CrossRef] [PubMed]
- Braza, M.E.; Fahrenkopf, M.P. Split-Thickness Skin Grafts; StatPearls Publishing: St. Petersburg, FL, USA, 2022. [Google Scholar]
- Prohaska, J.; Cook, C. Skin Grafting; StatPearls Publishing: St. Petersburg, FL, USA, 2022. [Google Scholar]
- Bridgham, K.M.; El Abiad, J.M.; Lu, Z.A.; Bhat, D.; Darrach, H.; Morris, C.D.; Levin, A.S.; Sacks, J.M. Reconstructive Limb-Salvage Surgery after Lower Extremity Soft Tissue Sarcoma Resection: A 20-Year Experience. J. Surg. Oncol. 2019, 119, 708–716. [Google Scholar] [CrossRef] [PubMed]
- Sedaghat, S.; Schmitz, F.; Grözinger, M.; Sedaghat, M. Malignant Peripheral Nerve Sheath Tumours in Magnetic Resonance Imaging: Primary and Recurrent Tumour Appearance, Post-Treatment Changes, and Metastases. Pol. J. Radiol. 2020, 85, e196–e201. [Google Scholar] [CrossRef]
- Banierink, H.; Meesters, A.M.L.; Ten Duis, K.; Doornberg, J.N.; El Moumni, M.; Heineman, E.; Reininga, I.H.F.; Ijpma, F.F.A. Does 3d-Assisted Operative Treatment of Pelvic Ring Injuries Improve Patient Outcome?—A Systematic Review of the Literature. J. Pers. Med. 2021, 11, 930. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Primary Closure n = 50 | Skin Graft n = 13 | Flap Reconstruction n = 7 | ||
|---|---|---|---|---|
| Age (years) | 68.9 (28) | 66.6 (15) | 71.6 (27) | |
| BMI 1 (kg/m2) | 26.4 (4.9) | 25.1 (5.3) | 28.5 (9.6) | |
| Tumor localization | Upper arm | 5 (10.0) | 2 (15.4) | 1 (14.3) |
| Lower arm | 3 (6.0) | 2 (15.4) | 2 (28.6) | |
| Upper leg | 36 (72.0) | 4 (30.8) | 2 (28.6) | |
| Lower leg | 6 (12.0) | 5 (38.5) | 2 (28.6) | |
| Tumor depth | Superficial | 9 (18.0) | 9 (69.2) | 3 (42.9) |
| Deep | 41 (82.0) | 4 (30.8) | 4 (57.1) | |
| Tumor grade | Borderline | 1 (2.0) | 1 (7.7) | 0 (0) |
| Low | 6 (12.0) | 0 (0) | 1 (14.3) | |
| High | 28 (56.0) | 11 (84.6) | 4 (57.1) | |
| Radiotherapy | None | 10 (20.0) | 4 (30.8) | 2 (28.6) |
| Preoperative RT 2 | 34 (68.0) | 8 (61.5) | 5 (71.4) | |
| Postoperative RT | 6 (12.0) | 1 (7.7) | 0 (0) | |
| PRS 3 | No | 46 (92.0) | 13 (100) | 4 (57.1) |
| Yes | 4 (8.0) | 0 (0) | 3 (42.9) | |
| Wound complications | None | 34 (68.0) | 9 (62.9) | 5 (71.4) |
| Grade I | 0 (0) | 1 (7.7) | 0 (0) | |
| Grade II | 11 (22.0) | 1 (7.7) | 1 (14.3) | |
| Grade IIIa | 3 (6.0) | 1 (7.7) | 0 (0) | |
| Grade IIIb | 2 (4.0) | 1 (7.7) | 1 (14.3) | |
| Grade IV and V | 0 (0) | 0 (0) | 0 (0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Generaal, J.D.; Glas, H.H.; Ubbels, J.F.; Stevenson, M.G.; Huijing, M.A.; van Leeuwen, B.L.; Been, L.B. Calculating Tumor Volume Using Three-Dimensional Models in Preoperative Soft-Tissue Sarcoma Surgical Planning: Does Size Matter? J. Clin. Med. 2023, 12, 7242. https://doi.org/10.3390/jcm12237242
Generaal JD, Glas HH, Ubbels JF, Stevenson MG, Huijing MA, van Leeuwen BL, Been LB. Calculating Tumor Volume Using Three-Dimensional Models in Preoperative Soft-Tissue Sarcoma Surgical Planning: Does Size Matter? Journal of Clinical Medicine. 2023; 12(23):7242. https://doi.org/10.3390/jcm12237242
Chicago/Turabian StyleGeneraal, Jasmijn D., Haye H. Glas, Jan F. Ubbels, Marc G. Stevenson, Marijn A. Huijing, Barbara L. van Leeuwen, and Lukas B. Been. 2023. "Calculating Tumor Volume Using Three-Dimensional Models in Preoperative Soft-Tissue Sarcoma Surgical Planning: Does Size Matter?" Journal of Clinical Medicine 12, no. 23: 7242. https://doi.org/10.3390/jcm12237242