
The Effectiveness of Rehabilitation after Open Surgical Release for Trigger Finger: A Prospective, Randomized, Controlled Study

Abstract
:1. Introduction
2. Materials and Methods
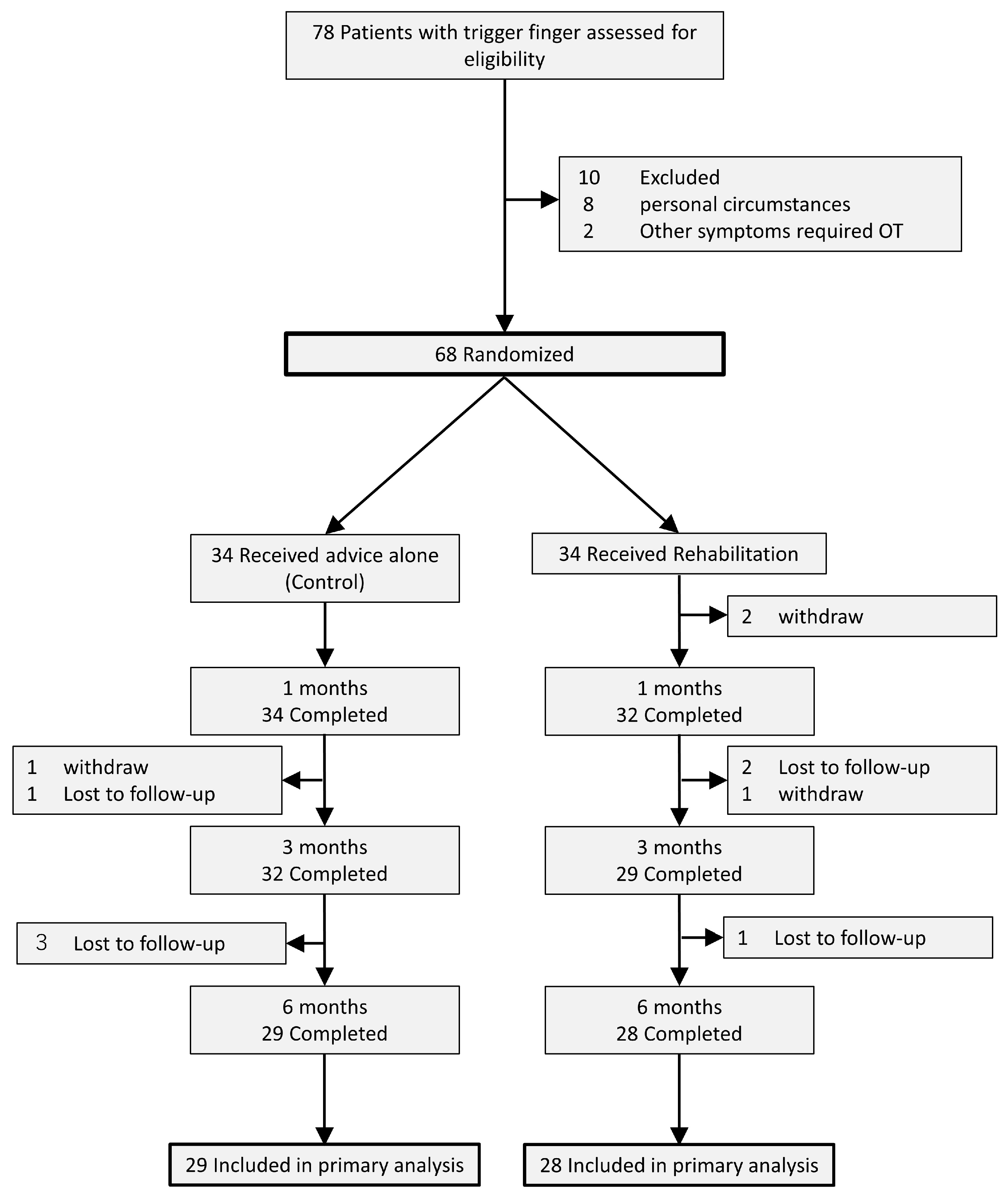
2.1. Design
2.2. Randomization
2.3. Treatments
2.4. Intervention
2.5. Follow-Up
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
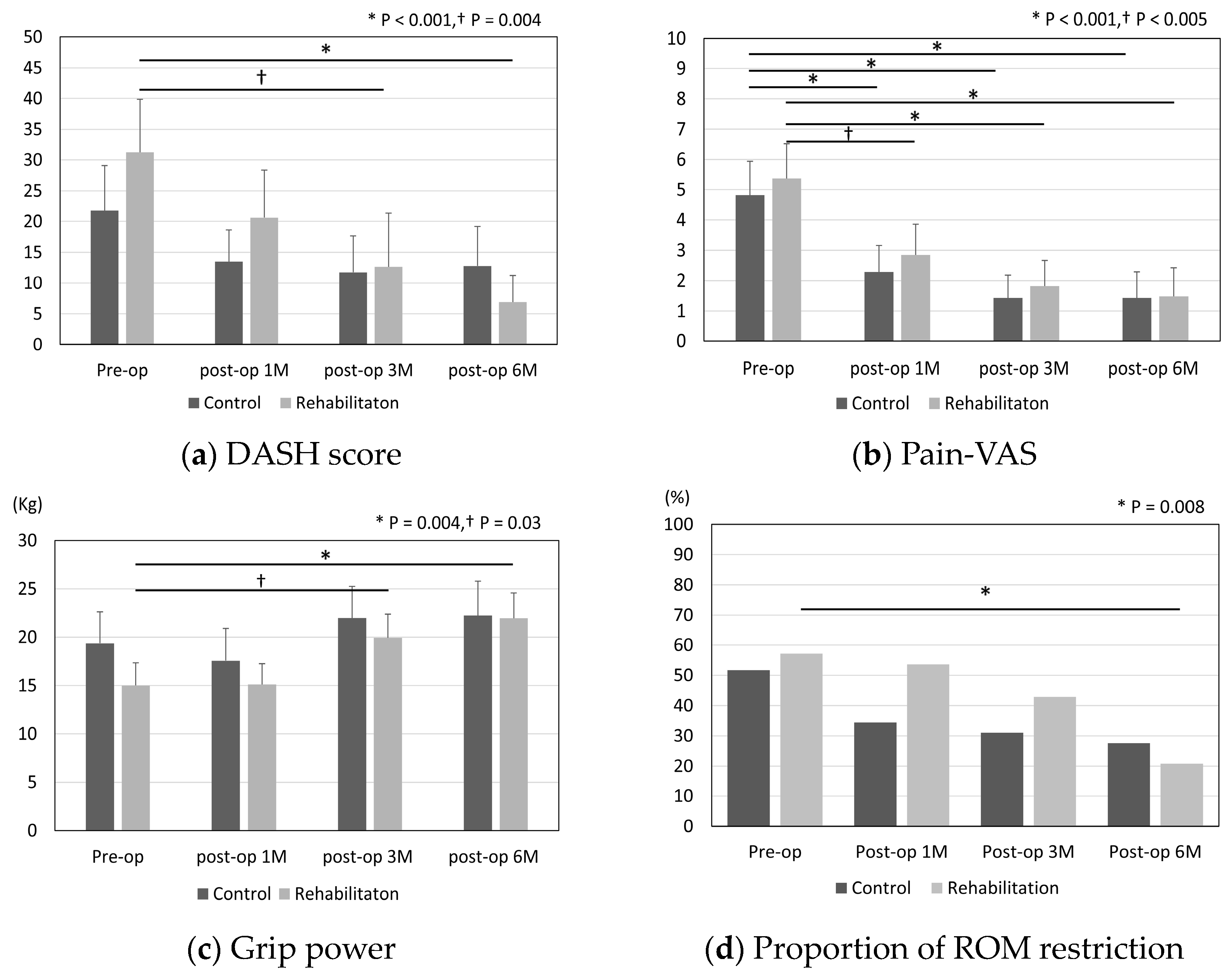
3.2. Effect of Postoperative Rehabilitation
3.3. Subanalysis
3.4. Complications
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Strom, L. Trigger finger in diabetes. J. Med. Soc. N. J. 1977, 74, 951–954. [Google Scholar]
- Ryzewicz, M.; Wolf, J.M. Trigger digits: Principles, management, and complications. J. Hand Surg. Am. 2006, 31, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Amirfeyz, R.; McNinch, R.; Watts, A.; Rodrigues, J.; Davis, T.R.C.; Glassey, N.; Bullock, J. Evidence-based management of adult trigger digits. J. Hand Surg. Eur. Vol. 2017, 42, 473–480. [Google Scholar] [CrossRef]
- Leow, M.Q.H.; Hay, A.S.R.; Ng, S.L.; Choudhury, M.M.; Li, H.; McGrouther, D.A.; Tay, S.C. A randomized controlled trial comparing ketorolac and triamcinolone injections in adults with trigger digits. J. Hand Surg. Eur. Vol. 2018, 43, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Everding, N.G.; Bishop, G.B.; Belyea, C.M.; Soong, M.C. Risk factors for complications of open trigger finger release. Hand 2015, 10, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Bruijnzeel, H.; Neuhaus, V.; Fostvedt, S.; Jupiter, J.B.; Mudgal, C.S.; Ring, D.C. Adverse events of open A1 pulley release for idiopathic trigger finger. J. Hand Surg. Am. 2012, 37, 1650–1656. [Google Scholar] [CrossRef]
- Dehghan, N.; Mitchell, S.M.; Schemitsch, E.H. Rehabilitation after plate fixation of upper and lower extremity fractures. Injury 2018, 49, S72–S77. [Google Scholar] [CrossRef]
- Tedesco, D.; Gibertoni, D.; Rucci, P.; Hernandez-Boussard, T.; Rosa, S.; Bianciardi, L.; Rolli, M.; Fantini, M.P. Impact of rehabilitation on mortality and readmissions after surgery for hip fracture. BMC Health Serv. Res. 2018, 18, 701. [Google Scholar] [CrossRef]
- Snell, D.L.; Hipango, J.; Sinnott, K.A.; Dunn, J.A.; Rothwell, A.; Hsieh, C.J.; DeJong, G.; Hooper, G. Rehabilitation after total joint replacement: A scoping study. Disabil. Rehabil. 2018, 40, 1718–1731. [Google Scholar] [CrossRef]
- Sultana, S.S.; MacDermid, J.C.; Grewal, R.; Rath, S. The effectiveness of early mobilization after tendon transfers in the hand: A systematic review. J. Hand Ther. 2013, 26, 1–20. [Google Scholar] [CrossRef]
- Provinciali, L.; Giattini, A.; Splendiani, G.; Logullo, F. Usefulness of hand rehabilitation after carpal tunnel surgery. Muscle Nerve 2000, 23, 211–216. [Google Scholar] [CrossRef]
- Yoshida, A.; Yamamoto, M.; Li-Tsang, C.W.P.; Iwatsuki, K.; Hirata, H. A systematic review assessing the effectiveness of hand therapy programmes in adults with burns using the International Classification of Functioning, Disability and Health framework. Nagoya J. Med. Sci. 2022, 84, 689–704. [Google Scholar] [PubMed]
- Deskur, A.; Deskur, Z. Surgical Treatment and Rehabilitation of Trigger Thumb and Finger. Cent. Eur. J. Sport Sci. Med. 2017, 17, 61–66. [Google Scholar] [CrossRef]
- Sato, E.S.; Gomes Dos Santos, J.B.; Belloti, J.C.; Albertoni, W.M.; Faloppa, F. Treatment of trigger finger: Randomized clinical trial comparing the methods of corticosteroid injection, percutaneous release and open surgery. Rheumatology 2012, 51, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Zyluk, A.; Jagielski, G. Percutaneous A1 pulley release vs steroid injection for trigger digit: The results of a prospective, randomized trial. J. Hand Surg. Eur. Vol. 2011, 36, 53–56. [Google Scholar] [CrossRef]
- Quinnell, R.C. Conservative management of trigger finger. Practitioner 1980, 224, 187–190. [Google Scholar]
- Czerniecki, J.M.; Turner, A.P.; Williams, R.M.; Hakimi, K.N.; Norvell, D.C. The effect of rehabilitation in a comprehensive inpatient rehabilitation unit on mobility outcome after dysvascular lower extremity amputation. Arch. Phys. Med. Rehabil. 2012, 93, 1384–1391. [Google Scholar] [CrossRef]
- Akeson, W.H.; Amiel, D.; Abel, M.F.; Garfin, S.R.; Woo, S.L. Effects of immobilization on joints. Clin. Orthop. Relat. Res. 1987, 219, 28–37. [Google Scholar] [CrossRef]
- Namba, R.S.; Kabo, J.M.; Dorey, F.J.; Meals, R.A. Continuous passive motion versus immobilization. The effect on posttraumatic joint stiffness. Clin. Orthop. Relat. Res. 1991, 267, 218–223. [Google Scholar] [CrossRef]
- Salter, R.B. The Biological Concept of Continuous Passive Motion of Synovial Joints—The 1st 18 Years of Basic Research and Its Clinical-Application; Bristol Myers Squibb: New York, NY, USA, 1990; pp. 335–353. [Google Scholar]
- Kearney, L.M.; Brown, K.K. The therapist’s management of intra-articular fractures. Hand Clin. 1994, 10, 199–209. [Google Scholar] [CrossRef]
- Li, S.; Sun, H.; Luo, X.; Wang, K.; Wu, G.; Zhou, J.; Wang, P.; Sun, X. The clinical effect of rehabilitation following arthroscopic rotator cuff repair: A meta-analysis of early versus delayed passive motion. Medicine 2018, 97, e9625. [Google Scholar] [CrossRef] [PubMed]
- DeStefano, F.; Nordstrom, D.L.; Vierkant, R.A. Long-term symptom outcomes of carpal tunnel syndrome and its treatment. J. Hand Surg. Am. 1997, 22, 200–210. [Google Scholar] [CrossRef]
- Nygaard, O.P.; Kloster, R.; Solberg, T. Duration of leg pain as a predictor of outcome after surgery for lumbar disc herniation: A prospective cohort study with 1-year follow up. J. Neurosurg. 2000, 92, 131–134. [Google Scholar] [CrossRef]
- Inderhaug, E.; Kollevold, K.H.; Kalsvik, M.; Hegna, J.; Solheim, E. Preoperative NSAIDs, non-acute onset and long-standing symptoms predict inferior outcome at long-term follow-up after rotator cuff repair. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 2067–2072. [Google Scholar] [CrossRef]
- Le Viet, D.; Tsionos, I.; Boulouednine, M.; Hannouche, D. Trigger finger treatment by ulnar superficialis slip resection (U.S.S.R.). J. Hand Surg. Br. 2004, 29, 368–373. [Google Scholar] [CrossRef]
- Kuczmarski, A.S.; Harris, A.P.; Gil, J.A.; Weiss, A.C. Management of Diabetic Trigger Finger. J. Hand Surg. Am. 2019, 44, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Wiwanitkit, S.; Wiwanitkit, V. Trigger digits and diabetes mellitus. N. Am. J. Med. Sci. 2012, 4, 117–119. [Google Scholar] [CrossRef] [PubMed]
- Koh, S.; Nakamura, S.; Hattori, T.; Hirata, H. Trigger digits in diabetes: Their incidence and characteristics. J. Hand Surg. Eur. Vol. 2010, 35, 302–305. [Google Scholar] [CrossRef]
- Nimigan, A.S.; Ross, D.C.; Gan, B.S. Steroid injections in the management of trigger fingers. Am. J. Phys. Med. Rehabil. 2006, 85, 36–43. [Google Scholar] [CrossRef]
- Stahl, S.; Kanter, Y.; Karnielli, E. Outcome of trigger finger treatment in diabetes. J. Diabetes Complicat. 1997, 11, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Grigorios, K.; Pantouvaki, A.; Spyrantis, M.; Christoforidis, C.; Velivasakis, G. Percutaneous or Open Release is the Most Effective Surgical Technique in Diabetic Recurrent Trigger Finger in Short and Long Term Outcomes? A Clinical Review. Acta Sci. Orthop. 2020, 3, 33–38. [Google Scholar]
- Murphy, D.; Failla, J.M.; Koniuch, M.P. Steroid versus placebo injection for trigger finger. J. Hand Surg. Am. 1995, 20, 628–631. [Google Scholar] [CrossRef] [PubMed]
- Gilberts, E.C.; Beekman, W.H.; Stevens, H.J.; Wereldsma, J.C. Prospective randomized trial of open versus percutaneous surgery for trigger digits. J. Hand Surg. Am. 2001, 26, 497–500. [Google Scholar] [CrossRef] [PubMed]
- Dierks, U.; Hoffmann, R.; Meek, M.F. Open versus percutaneous release of the A1-pulley for stenosing tendovaginitis: A prospective randomized trial. Tech. Hand Up. Extrem. Surg. 2008, 12, 183–187. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Number | p-Value | ||
|---|---|---|---|---|
| Total (n = 57) | Control (n = 29) | Rehabilitation (n = 28) | ||
| Sex | 0.25 | |||
| Men | 17 | 11 | 6 | |
| Women | 40 | 18 | 22 | |
| Age | 66.5 | 67.8 | 65.1 | 0.41 |
| Duration of symptom (M) | 14.3 | 12.4 | 16.8 | 0.46 |
| Quinnell grading | 0.08 | |||
| I | 6 | 2 | 4 | |
| II | 32 | 20 | 12 | |
| III | 19 | 7 | 12 | |
| Dominant hand affected (%) | 63.2 | 62.0 | 64.2 | 1.00 |
| Involved digit | 0.89 | |||
| Thumb | 17 | 9 | 8 | |
| Index finger | 3 | 2 | 1 | |
| Long finger | 17 | 12 | 15 | |
| Ring finger | 8 | 5 | 3 | |
| Small finger | 2 | 1 | 1 | |
| Diabetes mellitus (%) | 15.8 | 20.7 | 10.3 | 0.47 |
| History of trigger finger in other digits (%) | 10.5 | 6.9 | 14.3 | 0.42 |
| Restricted range of motion (%) | 54.3 | 51.7 | 57.1 | 0.79 |
| Type of occupation | 0.39 | |||
| Housework | 17 | 11 | 6 | |
| Light work | 23 | 10 | 13 | |
| Heavy work | 17 | 8 | 9 | |
| Item | Number | p-Value | |
|---|---|---|---|
| Control (n = 29) | Rehabilitation (n = 28) | ||
| Grip strength (kg) | 3.8 (0.8–6.9) | 8.0 (4.8–11.1) | 0.04 * |
| DASH | 6.9 (−2.3–16.0) | 23.2 (13.3–33.1) | 0.03 * |
| Pain-VAS | 3.7 (2.3–5.1) | 3.5 (2.1–4.9) | 0.64 |
| Item | DASH (Post-op 6M) | p-Value | |
|---|---|---|---|
| House or light work | Control (n = 21) | 14.2 (5.3–23.0) | 0.04 * |
| Rehabilitation (n = 19) | 6.1 (1.6–10.7) | ||
| Heavy work | Control (n = 8) | 9.5 (1.7–17.2) | 0.50 |
| Rehabilitation (n = 9) | 8.6 (0–20.8) |
| Item | DASH (Post-op 6M) | p-Value | |
|---|---|---|---|
| Duration of symptom < 12 M | Control (n = 12) | 5.9 (2.3–9.4) | 0.38 |
| Rehabilitation (n = 15) | 9.2 (1.9–16.5) | ||
| Duration of symptom > 12 M | Control (n = 13) | 19.6 (7.7–31.5) | 0.005 * |
| Rehabilitation (n = 6) | 0.7 (0–2.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saito, T.; Nakamichi, R.; Nakahara, R.; Nishida, K.; Ozaki, T. The Effectiveness of Rehabilitation after Open Surgical Release for Trigger Finger: A Prospective, Randomized, Controlled Study. J. Clin. Med. 2023, 12, 7187. https://doi.org/10.3390/jcm12227187
Saito T, Nakamichi R, Nakahara R, Nishida K, Ozaki T. The Effectiveness of Rehabilitation after Open Surgical Release for Trigger Finger: A Prospective, Randomized, Controlled Study. Journal of Clinical Medicine. 2023; 12(22):7187. https://doi.org/10.3390/jcm12227187
Chicago/Turabian StyleSaito, Taichi, Ryo Nakamichi, Ryuichi Nakahara, Keiichiro Nishida, and Toshifumi Ozaki. 2023. "The Effectiveness of Rehabilitation after Open Surgical Release for Trigger Finger: A Prospective, Randomized, Controlled Study" Journal of Clinical Medicine 12, no. 22: 7187. https://doi.org/10.3390/jcm12227187