
Predicting Potentially Fatal COVID-19 Disease in Pregnant Patients Using the Neutrophil-to-Lymphocyte Ratio (NLR)
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Patient Selection
2.2. Data Collection
2.3. Statistical Methods
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 54, 536–544. [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 3828, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 39510223, 507–513. [Google Scholar] [CrossRef]
- Rahman, S.; Montero, M.T.V.; Rowe, K.; Kirton, R.; Frank, K., Jr. Epidemiology, pathogenesis, clinical presentations, diagnosis and treatment of COVID-19: A review of current evidence. Expert. Rev. Clin. Pharmacol. 2021, 145, 601–621. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Wang, Y. The Clinical Characteristics and Risk Factors of Severe COVID-19. Gerontology 2021, 673, 255–266. [Google Scholar] [CrossRef]
- Wei, S.Q.; Bilodeau-Bertrand, M.; Liu, S.; Auger, N. The impact of COVID-19 on pregnancy outcomes: A systematic review and meta-analysis. CMAJ 2021, 19316, E540–E548. [Google Scholar] [CrossRef]
- Majumder, J.; Minko, T. Recent Developments on Therapeutic and Diagnostic Approaches for COVID-19. AAPS J. 2021, 231, 14. [Google Scholar] [CrossRef] [PubMed]
- Tarbiah, N.I.; Alkhattabi, N.A.; Alsahafi, A.J.; Aljahdali, H.S.; Joharjy, H.M.; Sabban, A.M.; Alghamdi, R.A.; Balgoon, M.J.; Khalifa, R.A. T Cells Immunophenotyping and CD38 Overexpres-sion as Hallmarks of the Severity of COVID-19 and Predictors of Patients' Outcomes. J. Clin. Med. 2023, 122, 710. [Google Scholar] [CrossRef]
- Sharma, J.; Rajput, R.; Bhatia, M.; Arora, P.; Sood, V. Clinical Predictors of COVID-19 Severity and Mor-tality: A Perspective. Front. Cell Infect. Microbiol. 2021, 11, 674277. [Google Scholar] [CrossRef]
- Jimeno, S.; Ventura, P.S.; Castellano, J.M.; García-Adasme, S.I.; Miranda, M.; Touza, P.; Lllana, I.; López-Escobar, A. Prognostic implications of neutrophil-lymphocyte ratio in COVID-19. Eur. J. Clin. Investig. 2021, 511, e13404. [Google Scholar] [CrossRef]
- Liu, Y.; Du, X.; Chen, J.; Jin, Y.; Peng, L.; Wang, H.H.X.; Luo, M.; Chen, L.; Zhao, Y. Neutrophil-to-lymphocyte ratio as an independent risk factor for mortality in hospitalized patients with COVID-19. J. Infect. 2020, 811, e6–e12. [Google Scholar] [CrossRef] [PubMed]
- Carranza Lira, S.; García Espinosa, M. Differences in the neutrophil/lymphocyte ratio and the plate-let/lymphocyte ratio in pregnant women with and without COVID-19. Int. J. Gynaecol. Obstet. 2022, 1572, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Aslan, M.M.; Yeler, M.T.; Yuvacı, H.U.; Cerci, I.A.; Cevrioğlu, A.S.; Ozden, S. Can the neutrophil-to-lymphocyte ratio (NLR) predicts fetal loss in preeclampsia with severe features? Pregnancy Hypertens. 2020, 22, 14–16. [Google Scholar] [CrossRef] [PubMed]
- Sahin, M.; Oguz, A.; Tüzün, D.; Okay, I.; Songül, I.; Cansu, Ü.; Hatice, Ş.; Kamile, G. A new marker predicting gestational diabetes mellitus: First tri-mester neutrophil/lymphocyte ratio. Medicine 2022, 10136, e30514. [Google Scholar] [CrossRef]
- Liu, D.; Huang, X.; Xu, Z.; Chen, M.; Wu, M. Predictive value of NLR and PLR in missed miscarriage. J. Clin. Lab. Anal. 2022, 363, e24250. [Google Scholar] [CrossRef]
- Zahorec, R. Neutrophil-to-lymphocyte ratio, past, present and future perspectives. Bratisl. Lek. Listy 2021, 122, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Qin, B.; Ma, N.; Tang, Q.; Wei, T.; Yang, M.; Fu, H.; Hu, Z.; Liang, Y.; Yang, Z.; Zhong, R. Neutrophil to lymphocyte ratio (NLR) and platelet to lymphocyte ratio (PLR) were useful markers in assessment of inflammatory response and disease activity in SLE patients. Mod. Rheumatol. 2016, 263, 372–376. [Google Scholar] [CrossRef]
- Ren, Z.; Yang, J.; Liang, J.; Xu, Y.; Lu, G.; Han, Y.; Zhu, J.; Tan, H.; Xu, T.; Ren, M. Monitoring of postoperative neutrophil-to-lymphocyte ratio, D-dimer, and CA153 in: Diagnostic value for recurrent and metastatic breast cancer. Front. Surg. 2023, 9, 927491. [Google Scholar] [CrossRef]
- Justesen, M.M.; Jakobsen, K.K.; Bendtsen, S.K.; Garset-Zamani, M.; Mordhorst, C.; Carlander, A.-L.F.; Gothelf, A.B.; Grønhøj, C.; von Buchwald, C. Pretreatment Neutrophil-to-Lymphocyte Ratio as a Prognostic Marker for the Outcome of HPV-Positive and HPV-Negative Oropharyngeal Squamous Cell Carcinoma. Viruses 2023, 151, 198. [Google Scholar] [CrossRef]
- Langley, B.O.; Guedry, S.E.; Goldenberg, J.Z.; Hanes, D.A.; Beardsley, J.A.; Ryan, J.J. Inflammatory Bowel Disease and Neutrophil-Lymphocyte Ratio: A Systematic Scoping Review. J. Clin. Med. 2021, 10, 4219. [Google Scholar] [CrossRef]
- Buicu, A.L.; Cernea, S.; Benedek, I.; Buicu, C.F.; Benedek, T. Systemic Inflammation and COVID-19 Mortality in Patients with Major Noncommunicable Diseases: Chronic Coronary Syndromes, Diabetes and Obesity. J. Clin. Med. 2021, 10, 1545. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zeng, J.; Zhang, L.; Yu, X.; Guo, J.; Li, Z. The Utility of Peripheral Blood Leucocyte Ratios as Biomarkers in Neonatal Sepsis: A Systematic Review and Meta-Analysis. Front. Pediatr. 2022, 10, 908362. [Google Scholar] [CrossRef] [PubMed]
- Holm, S. A Simple Sequentially Rejective Multiple Test Procedure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- Damar Çakırca, T.; Torun, A.; Çakırca, G.; Portakal, R.D. Role of NLR, PLR, ELR and CLR in differentiating COVID-19 patients with and without pneumonia. Int. J. Clin. Pract. 2021, 75, e14781. [Google Scholar] [CrossRef] [PubMed]
- Zhu, K.; Ma, S.; Chen, H.; Xie, J.; Huang, D.; Fu, C.; Ma, G.; Huang, Y. Value of Laboratory Indicators in Predicting Pneumonia in Symptomatic COVID-19 Patients Infected with the SARS-CoV-2 Omicron Variant. Infect. Drug Resist. 2023, 16, 1159–1170. [Google Scholar] [CrossRef] [PubMed]
- Abeid, S.T.; Mezedawee, A.A.S.; Alam, Y.S.J. Exploring the Influence of Neutrophil-Lymphocyte Ratio on Outcome Prediction of Severely-Ill Patients with COVID-19. Wiad. Lek. 2022, 7512, 2926–2932. [Google Scholar] [CrossRef]
- Bai, Y.Y.; Xi, Y.; Yin, B.B.; Zhang, J.H.; Chen, F.; Zhu, B. Reference intervals of systemic immune-inflammation index, neutrophil-to-lymphocyte ratio, lymphocyte-to-monocyte ratio, and platelet-to-lymphocyte ratio during normal pregnancy in China. Eur. Rev. Med. Pharmacol. Sci. 2023, 273, 1033–1044. [Google Scholar] [CrossRef]
- Oylumlu, M.; Ozler, A.; Yildiz, A.; Oylumlu, M.; Acet, H.; Polat, N.; Soydinc, H.E.; Ertas, F. New inflammatory markers in pre-eclampsia: Echocardiograph-ic epicardial fat thickness and neutrophil to lymphocyte ratio. Clin. Exp. Hypertens. 2014, 367, 503–507. [Google Scholar] [CrossRef]
- Thombare, D.; Bhalerao, A.; Dixit, P.; Joshi, S.; Dapkekar, P. Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio in Antenatal Women With Pre-eclampsia: A Case-Control Study. Cureus 2023, 15, e40338. [Google Scholar] [CrossRef]
- Cui, H.X.; Chen, C.; Jung, Y.M.; Guo, Z.Y.; Dong, C.Y.; Lee, S.M.; Zhang, Y.H. Neutrophil-to-lymphocyte ratio (NLR) as a predictive index for liver and coagulation dysfunction in preeclampsia patients. BMC Pregnancy Childbirth 2023, 23, 4. [Google Scholar] [CrossRef]
- Pace, N.P.; Vassallo, J. Association Between Neutrophil-Lymphocyte Ratio and Gestational Diabetes-A Systematic Review and Meta-Analysis. J. Endocr. Soc. 2021, 57, bvab051. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Mei, H.; Xiao, H.; Zhang, Y.; Gao, W.; Qi, H.; Zhang, J. Association between neutrophil-lymphocyte ratio and perinatal de-pressive symptoms among Chinese women. J. Psychosom. Res. 2023, 166, 111101. [Google Scholar] [CrossRef] [PubMed]
- Ozkan, D.; Ibanoglu, M.C.; Adar, K.; Ozkan, M.; Lutfi Tapisiz, O.; Engin-Ustun, Y.; Iskender, C.T. Efficacy of blood parameters in predicting the severity of gestational hypertension and preeclampsia. J. Obstet. Gynaecol. 2023, 43, 2144175. [Google Scholar] [CrossRef]
- Supák, D.; Mészáros, B.; Nagy, M.; Gáspár, D.; Wagner, L.J.; Kukor, Z.; Valent, S. Case report: COVID-19 infection in a pregnant 33-year-old kidney transplant recipient. Front. Med. 2022, 9, 948025. [Google Scholar] [CrossRef] [PubMed]
- Rehman, S.U.; Yoo, H.H. COVID-19 challenges and its therapeutics. Biomed. Pharmacother. 2021, 142, 112015. [Google Scholar] [CrossRef]
- Fesu, D.; Bohacs, A.; Hidvegi, E.; Matics, Z.; Polivka, L.; Horvath, P.; Czaller, I.; Sutto, Z.; Eszes, N.; Vincze, K.; et al. Remdesivir in Solid Organ Recipients for COVID-19 Pneumonia. Transplant. Proc. 2022, 549, 2567–2569. [Google Scholar] [CrossRef]
- Fernandes, Q.; Inchakalody, V.P.; Merhi, M.; Mestiri, S.; Taib, N.; El-Ella, D.M.A.; Bedhiafi, T.; Raza, A.; Al-Zaidan, L.; Mohsen, M.O.; et al. Emerging COVID-19 variants and their impact on SARS-CoV-2 diagnosis, therapeutics and vaccines. Ann. Med. 2022, 541, 524–540. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristic | Group 1 (n = 10) | Group 2 (n = 15) | Group 3 (n = 20) |
|---|---|---|---|
| Age (years) | 34.60 ± 5.04 | 31.87 ± 4.90 | 33.20 ± 7.05 |
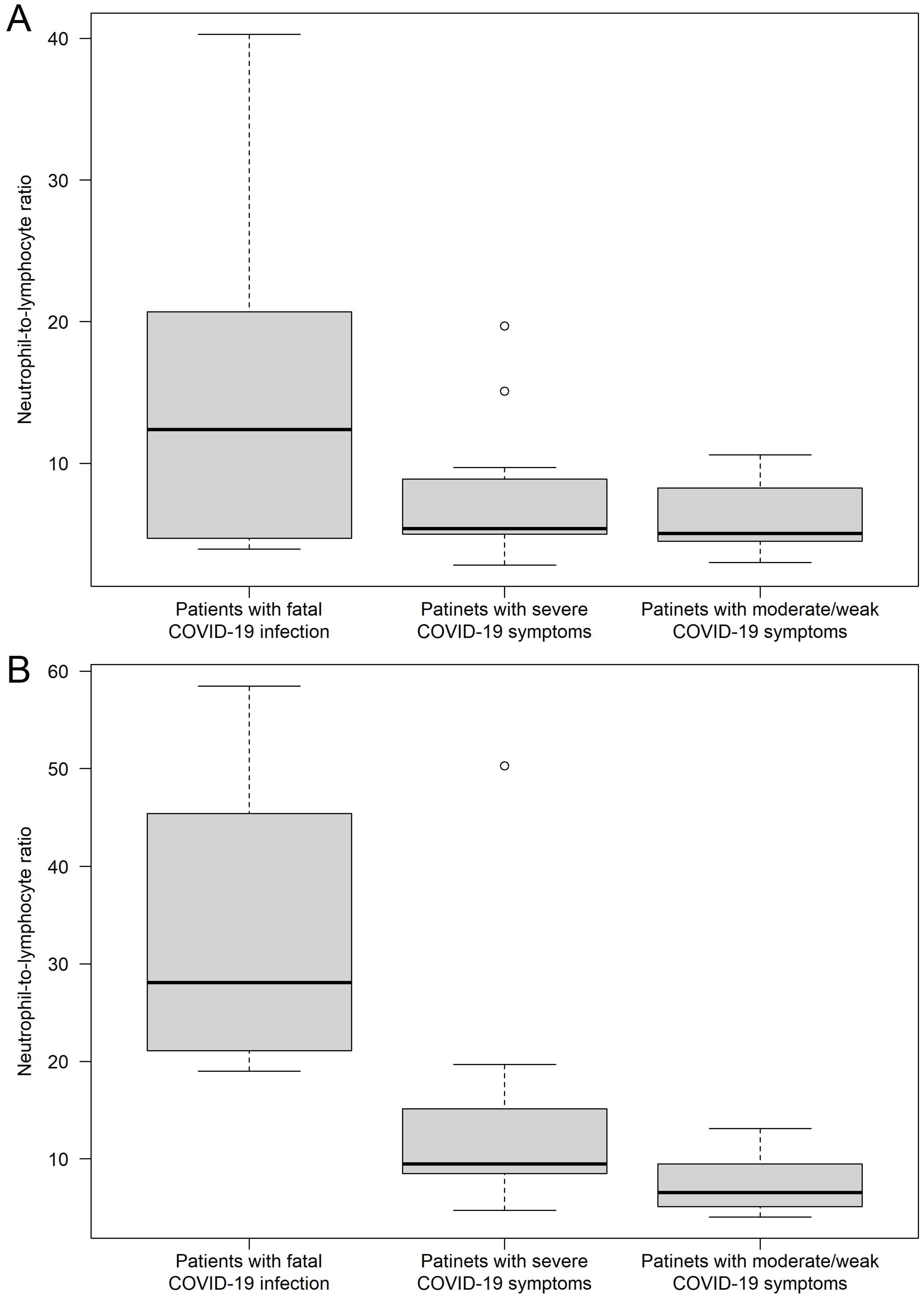
| First-day NLR value | 14.56 ± 11.34 | 7.66 ± 4.62 | 5.97 ± 2.23 |
| Peak NLR during the infection | 33.77 ± 14.03 | 13.35 ± 11.43 | 7.54 ± 2.86 |
| Gestational age when the infection started (weeks) | 31.30 ± 3.09 | 30.27 ± 5.46 | 31.05 ± 4.74 |
| Clinical Characteristic | Groups 1 vs. 2 | Groups 1 vs. 3 | Groups 2 vs. 3 |
|---|---|---|---|
| age (years) | p = 0.5447 | p = 1.0000 | p = 1.0000 |
| first-day NLR value | p = 0.3926 | p = 0.1288 | p = 0.3926 |
| peak NLR during the infection | p = 0.0006 | p < 0.0001 | p = 0.0143 |
| gestational age when the infection started (weeks) | p = 1.0000 | p = 1.0000 | p = 1.0000 |
| Groups | Patients with 0 Comorbidity in Medical History | Patients with 1 Comorbidity in Medical History | Patients with 2 Comorbidities in Medical History |
|---|---|---|---|
| Group 1 (n = 10) | 5 | 4 | 1 |
| Group 2 (n = 15) | 8 | 5 | 2 |
| Group 3 (n = 20) | 15 | 5 | 0 |
| Clinical Characteristic | Model Investigating D1 NLR | Model Investigating Peak NLR |
|---|---|---|
| Age (years) | 0.5198 | 0.8520 |
| Gestational week | 0.9482 | 0.4850 |
| Number of comorbidities | ||
| 0 vs. 1 | 0.0776 | 0.5020 |
| 0 vs. 2 | 0.4077 | 0.6700 |
| 0 vs. 3 | 0.9138 | 0.4760 |
| Clinical Characteristic | Model Investigating D1 NLR | Model Investigating Peak NLR |
|---|---|---|
| p-Values | ||
| Age (years) | 0.6681 | 0.3448 |
| Gestational week | 0.9742 | 0.2054 |
| Number of comorbidities | ||
| 0 vs. 1 | 0.1864 | 0.8583 |
| 0 vs. 2 | 0.6462 | 0.1610 |
| 0 vs. 3 | 0.7542 | 0.1649 |
| Random effect | ||
| Random effect of NLR values | 0.0006 | 0.0006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Supák, D.; Mészáros, B.; Turi, B.; Herold, Z.; Kukor, Z.; Valent, S. Predicting Potentially Fatal COVID-19 Disease in Pregnant Patients Using the Neutrophil-to-Lymphocyte Ratio (NLR). J. Clin. Med. 2023, 12, 6896. https://doi.org/10.3390/jcm12216896
Supák D, Mészáros B, Turi B, Herold Z, Kukor Z, Valent S. Predicting Potentially Fatal COVID-19 Disease in Pregnant Patients Using the Neutrophil-to-Lymphocyte Ratio (NLR). Journal of Clinical Medicine. 2023; 12(21):6896. https://doi.org/10.3390/jcm12216896
Chicago/Turabian StyleSupák, Dorina, Balázs Mészáros, Balázs Turi, Zoltán Herold, Zoltán Kukor, and Sándor Valent. 2023. "Predicting Potentially Fatal COVID-19 Disease in Pregnant Patients Using the Neutrophil-to-Lymphocyte Ratio (NLR)" Journal of Clinical Medicine 12, no. 21: 6896. https://doi.org/10.3390/jcm12216896