

COVID-19 versus Other Disease Etiologies as the Cause of ARDS in Patients Necessitating Venovenous Extracorporeal Membrane Oxygenation—A Comparison of Patients’ Data during the Three Years of the COVID-19 Pandemic
 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. VV ECMO Management
2.4. Outcome of the Study
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristic and Patients’ Condition before VV ECMO in Non-COVID-19 and COVID-19 ARDS Patients
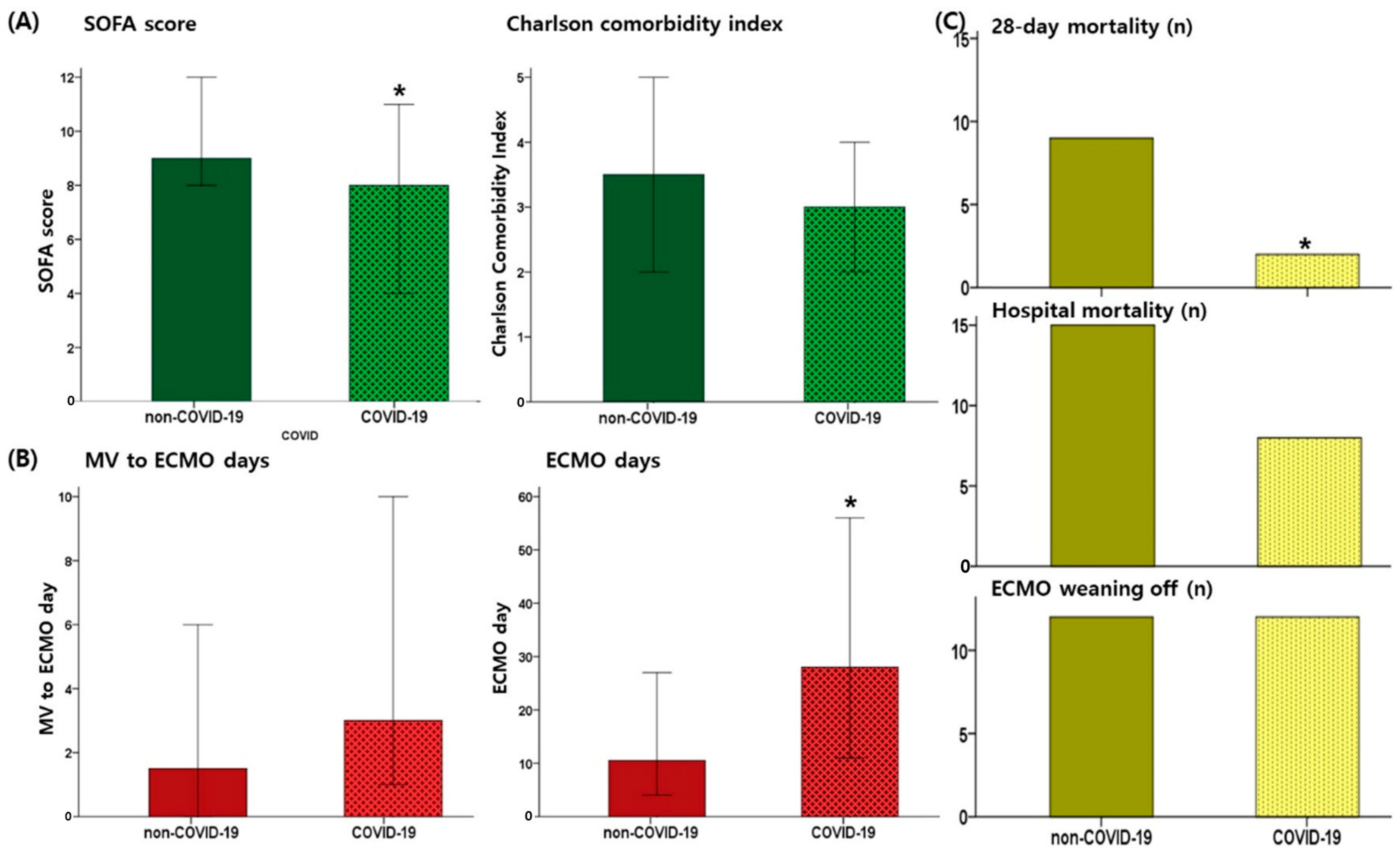
3.2. Disease Course and Prognosis of Non-COVID-19 and COVID-19 Patients
3.3. VV ECMO Weaning Off, Mortality, and COVID-19
3.4. Complications during VV ECMO
4. Discussion
4.1. Severe ARDS in COVID-19 and VV ECMO
4.2. COVID-19 and Other Etiologies as the Cause of Severe ARDS Requiring ECMO
4.3. Comparison of ARDS Due to COVID-19 and Other Etiologies in Our Study Patients
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Taubenberger, J.K.; Morens, D.M. 1918 Influenza: The mother of all pandemics. Emerg. Infect. Dis. 2006, 12, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Golicnik, A.; Zivanovic, I.; Gorjup, V.; Berden, J. Same but Different-ECMO in COVID-19 and ARDS of Other Etiologies. Comparison of Survival Outcomes and Management in Different ARDS Groups. J. Intensive Care Med. 2023, 38, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.J.; Heinsar, S.; Jeong, I.S.; Shekar, K.; Li Bassi, G.; Jung, J.S.; Suen, J.Y.; Fraser, J.F. ECMO use in COVID-19: Lessons from past respiratory virus outbreaks—A narrative review. Crit. Care 2020, 24, 301. [Google Scholar] [CrossRef] [PubMed]
- Ramanathan, K.; Antognini, D.; Combes, A.; Paden, M.; Zakhary, B.; Ogino, M.; MacLaren, G.; Brodie, D.; Shekar, K. Planning and provision of ECMO services for severe ARDS during the COVID-19 pandemic and other outbreaks of emerging infectious diseases. Lancet Respir. Med. 2020, 8, 518–526. [Google Scholar] [CrossRef]
- Davies, A.; Jones, D.; Bailey, M.; Beca, J.; Bellomo, R.; Blackwell, N.; Forrest, P.; Gattas, D.; Granger, E.; Herkes, R.; et al. Extracorporeal Membrane Oxygenation for 2009 Influenza A(H1N1) Acute Respiratory Distress Syndrome. JAMA 2009, 302, 1888–1895. [Google Scholar] [CrossRef] [PubMed]
- Urner, M.; Barnett, A.G.; Bassi, G.L.; Brodie, D.; Dalton, H.J.; Ferguson, N.D.; Heinsar, S.; Hodgson, C.L.; Peek, G.; Shekar, K.; et al. Venovenous extracorporeal membrane oxygenation in patients with acute COVID-19 associated respiratory failure: Comparative effectiveness study. BMJ 2022, 377, e068723. [Google Scholar] [CrossRef] [PubMed]
- Ramanathan, K.; Shekar, K.; Ling, R.R.; Barbaro, R.P.; Wong, S.N.; Tan, C.S.; Rochwerg, B.; Fernando, S.M.; Takeda, S.; MacLaren, G.; et al. Extracorporeal membrane oxygenation for COVID-19: A systematic review and meta-analysis. Crit. Care 2021, 25, 211. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Slutsky, A.S.; Bein, T.; Windisch, W.; Weber-Carstens, S.; Brodie, D. Complete countrywide mortality in COVID patients receiving ECMO in Germany throughout the first three waves of the pandemic. Crit. Care 2021, 25, 413. [Google Scholar] [CrossRef]
- Wendisch, D.; Dietrich, O.; Mari, T.; von Stillfried, S.; Ibarra, I.L.; Mittermaier, M.; Mache, C.; Chua, R.L.; Knoll, R.; Timm, S.; et al. SARS-CoV-2 infection triggers profibrotic macrophage responses and lung fibrosis. Cell 2021, 184, 6243–6261.e6227. [Google Scholar] [CrossRef]
- George, P.M.; Wells, A.U.; Jenkins, R.G. Pulmonary fibrosis and COVID-19: The potential role for antifibrotic therapy. Lancet Respir. Med. 2020, 8, 807–815. [Google Scholar] [CrossRef]
- Russ, M.; Menk, M.; Graw, J.A.; Skrypnikov, V.; Hunsicker, O.; Rudat, K.; Weber-Carstens, S.; Francis, R.C.E.; Pickerodt, P.A. COVID-19 Patients Require Prolonged Extracorporeal Membrane Oxygenation Support for Survival Compared with Non-COVID-19 Patients. Crit. Care Explor. 2022, 4, e0671. [Google Scholar] [CrossRef] [PubMed]
- Yaqoob, H.; Greenberg, D.; Huang, L.; Henson, T.; Pitaktong, A.; Peneyra, D.; Spencer, P.J.; Malekan, R.; Goldberg, J.B.; Kai, M.; et al. Extracorporeal membrane oxygenation in COVID-19 compared to other etiologies of acute respiratory failure: A single-center experience. Heart Lung 2023, 57, 243–249. [Google Scholar] [CrossRef]
- The ARDS Definition Task Force. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Ling, R.R.; Ramanathan, K.; Sim, J.J.L.; Wong, S.N.; Chen, Y.; Amin, F.; Fernando, S.M.; Rochwerg, B.; Fan, E.; Barbaro, R.P.; et al. Evolving outcomes of extracorporeal membrane oxygenation during the first 2 years of the COVID-19 pandemic: A systematic review and meta-analysis. Crit. Care 2022, 26, 147. [Google Scholar] [CrossRef] [PubMed]
- Barbaro, R.P.; MacLaren, G.; Boonstra, P.S.; Combes, A.; Agerstrand, C.; Annich, G.; Diaz, R.; Fan, E.; Hryniewicz, K.; Lorusso, R.; et al. Extracorporeal membrane oxygenation for COVID-19: Evolving outcomes from the international Extracorporeal Life Support Organization Registry. Lancet 2021, 398, 1230–1238. [Google Scholar] [CrossRef] [PubMed]
- Riera, J.; Alcántara, S.; Bonilla, C.; Fortuna, P.; Ortiz, A.B.; Vaz, A.; Albacete, C.; Millán, P.; Ricart, P.; Boado, M.V.; et al. Risk factors for mortality in patients with COVID-19 needing extracorporeal respiratory support. Eur. Respir. J. 2022, 59, 2102463. [Google Scholar] [CrossRef] [PubMed]
- Friedrichson, B.; Kloka, J.A.; Neef, V.; Mutlak, H.; Old, O.; Zacharowski, K.; Piekarski, F. Extracorporeal membrane oxygenation in coronavirus disease 2019: A nationwide cohort analysis of 4279 runs from Germany. Eur. J. Anaesthesiol. 2022, 39, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Massart, N.; Guervilly, C.; Mansour, A.; Porto, A.; Flécher, E.; Esvan, M.; Fougerou, C.; Fillâtre, P.; Duburcq, T.; Lebreton, G.; et al. Impact of Prone Position in COVID-19 Patients on Extracorporeal Membrane Oxygenation. Crit. Care Med. 2023, 51, 36–46. [Google Scholar] [CrossRef]
- Xu, Y.; Chou, Y.T.; Wei, X.G.; Zhang, S.F.; Jiang, F.; Liu, Y. ECMO combined with prone positioning strategies in COVID-19 respiratory distress syndrome. Perfusion 2022, 37, 417–421. [Google Scholar] [CrossRef]
- Papazian, L.; Schmidt, M.; Hajage, D.; Combes, A.; Petit, M.; Lebreton, G.; Rilinger, J.; Giani, M.; Le Breton, C.; Duburcq, T.; et al. Effect of prone positioning on survival in adult patients receiving venovenous extracorporeal membrane oxygenation for acute respiratory distress syndrome: A systematic review and meta-analysis. Intensive Care Med. 2022, 48, 270–280. [Google Scholar] [CrossRef]
- Peek, G.J.; Mugford, M.; Tiruvoipati, R.; Wilson, A.; Allen, E.; Thalanany, M.M.; Hibbert, C.L.; Truesdale, A.; Clemens, F.; Cooper, N.; et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): A multicentre randomised controlled trial. Lancet 2009, 374, 1351–1363. [Google Scholar] [CrossRef] [PubMed]
- Fanelli, V.; Giani, M.; Grasselli, G.; Mojoli, F.; Martucci, G.; Grazioli, L.; Alessandri, F.; Mongodi, S.; Sales, G.; Montrucchio, G.; et al. Extracorporeal membrane oxygenation for COVID-19 and influenza H1N1 associated acute respiratory distress syndrome: A multicenter retrospective cohort study. Crit. Care 2022, 26, 34. [Google Scholar] [CrossRef] [PubMed]
- Dreier, E.; Malfertheiner, M.V.; Dienemann, T.; Fisser, C.; Foltan, M.; Geismann, F.; Graf, B.; Lunz, D.; Maier, L.S.; Müller, T.; et al. ECMO in COVID-19-prolonged therapy needed? A retrospective analysis of outcome and prognostic factors. Perfusion 2021, 36, 582–591. [Google Scholar] [CrossRef] [PubMed]
- Dave, S.B.; Rabinowitz, R.; Shah, A.; Tabatabai, A.; Galvagno, S.M.; Mazzeffi, M.A.; Rector, R.; Kaczorowski, D.J.; Scalea, T.M.; Menaker, J. COVID-19 outcomes of venovenous extracorporeal membrane oxygenation for acute respiratory failure vs historical cohort of non-COVID-19 viral infections. Perfusion 2022, 38, 1165–1173. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wu, J.; Wang, S.; Li, X.; Zhou, J.; Huang, B.; Luo, D.; Cao, Q.; Chen, Y.; Chen, S.; et al. Progression to fibrosing diffuse alveolar damage in a series of 30 minimally invasive autopsies with COVID-19 pneumonia in Wuhan, China. Histopathology 2021, 78, 542–555. [Google Scholar] [CrossRef] [PubMed]
- Gill, J.R.; Sheng, Z.M.; Ely, S.F.; Guinee, D.G.; Beasley, M.B.; Suh, J.; Deshpande, C.; Mollura, D.J.; Morens, D.M.; Bray, M.; et al. Pulmonary pathologic findings of fatal 2009 pandemic influenza A/H1N1 viral infections. Arch. Pathol. Lab. Med. 2010, 134, 235–243. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total (N = 45) | Non-COVID-19 (N = 24) | COVID-19 (N = 21) | p Value | |
|---|---|---|---|---|
| Age | 61 (54.00–67.00) | 57 (53.25–65.75) | 63 (54.50–67.50) | 0.255 |
| Sex, male | 27 (60) | 15 (62.5) | 12 (57.1) | 0.767 |
| Body mass index (kg/m2) | 22.7 (20.53–25.93) | 23.71 (21.91–26.89) | 21.74 (19.66–24.69) | 0.144 |
| Diabetes mellitus | 22 (48.9) | 10 (41.7) | 12 (57.1) | 0.376 |
| Hypertension | 20 (44.4) | 10 (41.7) | 10 (47.6) | 0.769 |
| Cardiovascular | 7 (15.6) | 5 (20.8) | 2 (9.5) | 0.422 |
| COPD | 7 (15.6) | 5 (20.8) | 2 (9.5) | 0.422 |
| Chronic kidney disease stage V | 3 (6.7) | 1 (4.2) | 2 (9.5) | 0.592 |
| Malignancy or immunocompromised host | 15 (33.3) | 12 (50) | 3 (14.3) | 0.026 |
| APACHE II score | 18 (14–22.50) | 19.5 (15.25–24.00) | 15 (13–20) | 0.121 |
| SOFA score | 9 (7.00–12.00) | 9 (8.00–12.75) | 8 (4.00–11.50) | 0.033 |
| Vasopressor-inotropic score | 3.50 (0.00–21.25) | 23.71 (21.91–26.89) | 3.0 (0.00–10.00) | 0.551 |
| Charlson comorbidity index | 3 (2.0–5.0) | 3.5 (2.0–5.0) | 3 (2.0–4.0) | 0.256 |
| Etiology of ECMO | - | |||
| COVID-19 | 21 (46.7) | 0 | 21 (100) | |
| Bacterial/other pneumonia | 11/4 (24.4/8.9) | 11/4 (45.8/16.7) | - | |
| Aspiration pneumonitis | 4 (8.9) | 4 (16.7) | - | |
| Interstitial lung disease | 3 (6.7) | 3 (12.5) | - | |
| Other | 3 (6.7) | 3 (12.5) | - | |
| Mechanical ventilator setting before ECMO | ||||
| PEEP (cmH2O) | 10 (7.75–10.00) | 8.5 (6.00–10.00) | 10 (8.00–12.00) | 0.069 |
| Volume control/pressure control | 27/14 | 14/8 | 13/6 | 1.00 |
| VT/PBW (mL/kg) | 6.78 (6.15–7.83) | 7.25 (6.15–8.03) | 6.49 (6.17–7.61) | 0.481 |
| Blood gas analysis before ECMO | ||||
| PF ratio (mmHg) | 59.50 (48.25–78.90) | 58.9 (44.50–76.60) | 61 (50.70–87.95) | 0.488 |
| pH | 7.37 (7.21–7.42) | 7.32 (7.17–7.38) | 7.40 (7.31–7.45) | 0.034 |
| PO2 (mmHg) | 60.70 (46.9–77.0) | 57.1 (43.2–73.7) | 62.0 (53.0–87.3) | 0.120 |
| PCO2 (mmHg) | 51 (42–66) | 63.2 (43.4–71.3) | 44.0 (37.3–52.6) | 0.006 |
| HCO3− (mmol/L) | 25.9 (21.8–32.7) | 25.9 (20.93–34.68) | 25.5 (21.8–31.3) | 0.903 |
| SaO2 (%) | 88.55 (79.47–94.28) | 84.3 (64.9–93.1) | 91.0 (85.3–96.4) | 0.049 |
| Total (N = 45) | Non-COVID-19 (N = 24) | COVID-19 (N = 21) | p Value | |
|---|---|---|---|---|
| Days from Diagnosis of COVID-19 to ECMO | 11.00 (5.50–19.50) | - | 11.00 (6.00–20.00) | - |
| Days from ICU admission to MV | 0.00 (0.00–1.00) | 0.00 (0.00–1.75) | 0.00 (0.00–0.50) | 0.132 |
| Days from ICU admission to ECMO | 3.00 (1.00–9.50) | 2 (1.00–8.75) | 4.0 (1.0–10.5) | 0.492 |
| Days from MV to ECMO | 2.00 (0.00–7.00) | 1.50 (0.00–6.00) | 3.0 (1.00–10.50) | 0.196 |
| Mechanical ventilation day | 30.00 (12.00–57.00) | 18.50 (7.00–50.75) | 38 (16.50–58.00) | 0.219 |
| ECMO day | 15 (8.00–45.00) | 10.5 (3.25–29.25) | 28.0 (10.50–70.50) | 0.018 |
| Hospital day | 47.00 (27.00–92.50) | 41 (18.25–71.75) | 59.0 (33.0–121.5) | 0.082 |
| Mechanical ventilator weaning off at discharge | 18/22 (81.8) | 8/9 (88.9) | 10/13 (76.9) | 1.0 |
| ECMO weaning | 24 (52.1) | 12 (50.0) | 12 (57.1) | 0.767 |
| 28-day mortality | 11 (24.4) | 9 (37.5) | 2 (9.5) | 0.040 |
| Hospital mortality | 23 (51.1) | 15 (62.5) | 8 (38.1) | 0.139 |
| CRRT | 20 (44.4) | 13 (54.2) | 7 (33.3) | 0.231 |
| CNS bleeding | 1 (2.2) | 1 (4.2) | 0 (0) | 1.00 |
| UGI bleeding | 9 (20.0) | 3 (12.5) | 6 (28.6) | 0.267 |
| pneumothorax | 9 (20.0) | 6 (25) | 3 (14.3) | 0.469 |
| ECMO cannula related infection | 2 (4.4) | 1 (4.2) | 1 (4.8) | 1.000 |
| Thrombosis of ECMO cannula | 4 (8.9) | 1 (4.2) | 3 (14.3) | 0.326 |
| Unadjusted Hazrd Ratio | 95% Confidence Interval | p-Value | Adjusted Hazard Ratio | 95% Confidence Interval | p-Value | |
|---|---|---|---|---|---|---|
| Age | 1.046 | 0.995–1.099 | 0.075 | 1.068 | 1.010–1.130 | 0.022 |
| Sex | 0.885 | 0.363–2.101 | 0.782 | 1.374 | 0.472–4.004 | 0.560 |
| CCI | 1.429 | 1.138–1.794 | 0.002 | 1.405 | 1.041–1.896 | 0.026 |
| SOFA | 1.148 | 1.027–1.282 | 0.015 | 1.213 | 1.044–1.410 | 0.012 |
| APACHE II | 1.063 | 1.017–1.111 | 0.007 | |||
| PaO2/FiO2 ratio | 0.998 | 0.985–1.011 | 0.742 | |||
| PEEP | 0.880 | 0.782–0.992 | 0.036 | 1.014 | 0.879–1.170 | 0.847 |
| VT/PBW | 0.892 | 0.558–1.427 | 0.634 | |||
| COVID-19 | 0.325 | 0.124–0.849 | 0.022 | 0.350 | 0.110–1.115 | 0.076 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.; Seok, H.; Kim, B.K.; Hwang, J.; Park, D.W.; Shin, J.S.; Kim, J.H. COVID-19 versus Other Disease Etiologies as the Cause of ARDS in Patients Necessitating Venovenous Extracorporeal Membrane Oxygenation—A Comparison of Patients’ Data during the Three Years of the COVID-19 Pandemic. J. Clin. Med. 2023, 12, 6752. https://doi.org/10.3390/jcm12216752
Kim S, Seok H, Kim BK, Hwang J, Park DW, Shin JS, Kim JH. COVID-19 versus Other Disease Etiologies as the Cause of ARDS in Patients Necessitating Venovenous Extracorporeal Membrane Oxygenation—A Comparison of Patients’ Data during the Three Years of the COVID-19 Pandemic. Journal of Clinical Medicine. 2023; 12(21):6752. https://doi.org/10.3390/jcm12216752
Chicago/Turabian StyleKim, Sua, Hyeri Seok, Beong Ki Kim, Jinwook Hwang, Dae Won Park, Jae Seung Shin, and Je Hyeong Kim. 2023. "COVID-19 versus Other Disease Etiologies as the Cause of ARDS in Patients Necessitating Venovenous Extracorporeal Membrane Oxygenation—A Comparison of Patients’ Data during the Three Years of the COVID-19 Pandemic" Journal of Clinical Medicine 12, no. 21: 6752. https://doi.org/10.3390/jcm12216752