
Resilience and Psychological Well-Being of Polish Women in the Perinatal Period during the COVID-19 Pandemic
 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Methods
2.2. Measures
2.2.1. Maternal Depression Symptoms
2.2.2. Maternal Anxiety Symptoms
2.2.3. Resilience
2.3. Data Analysis
3. Results
3.1. Sample Characteristics
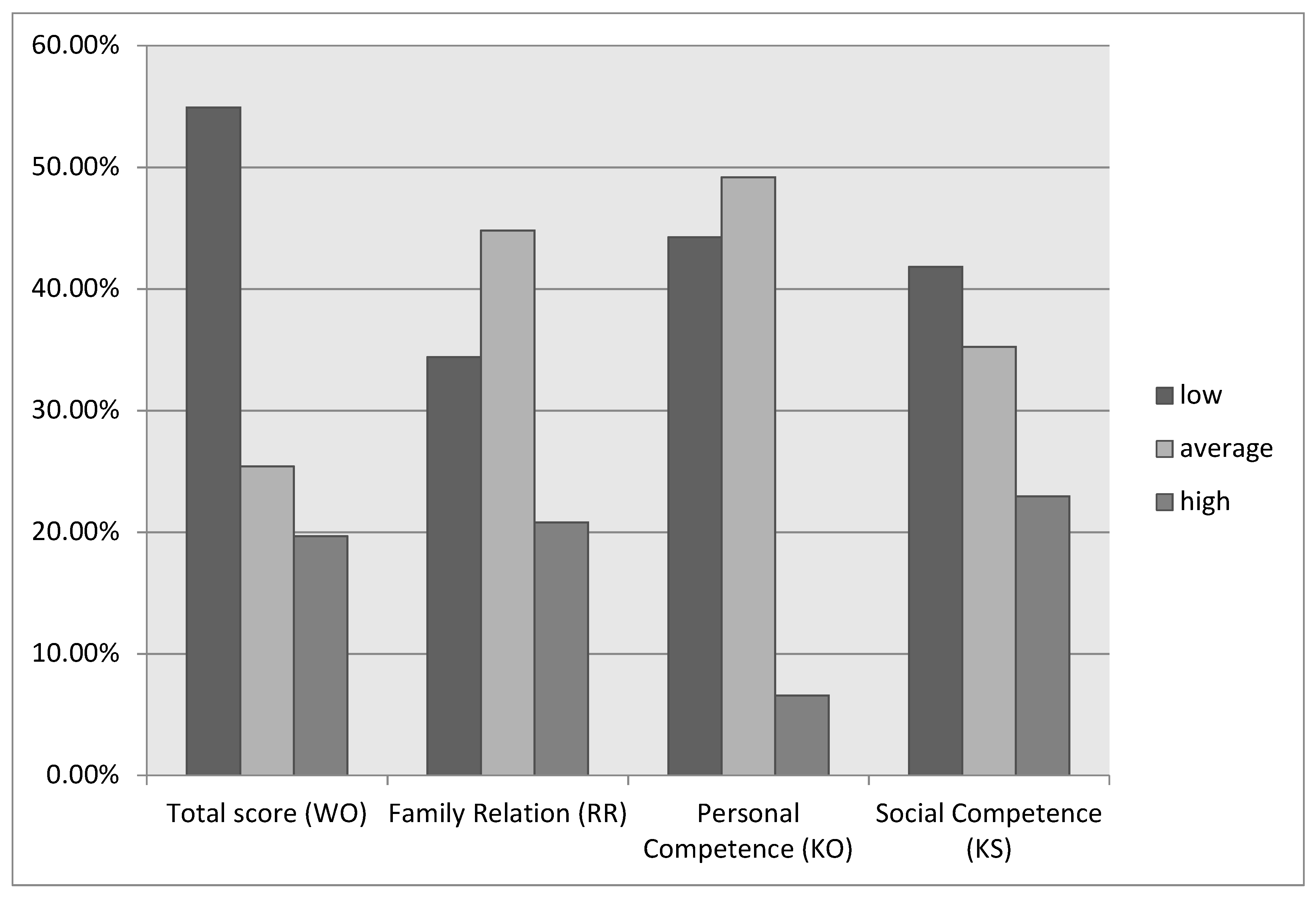
3.2. Resilience Level in the Study Sample
3.3. Level of Depressiveness and Anxiety in the Study Sample
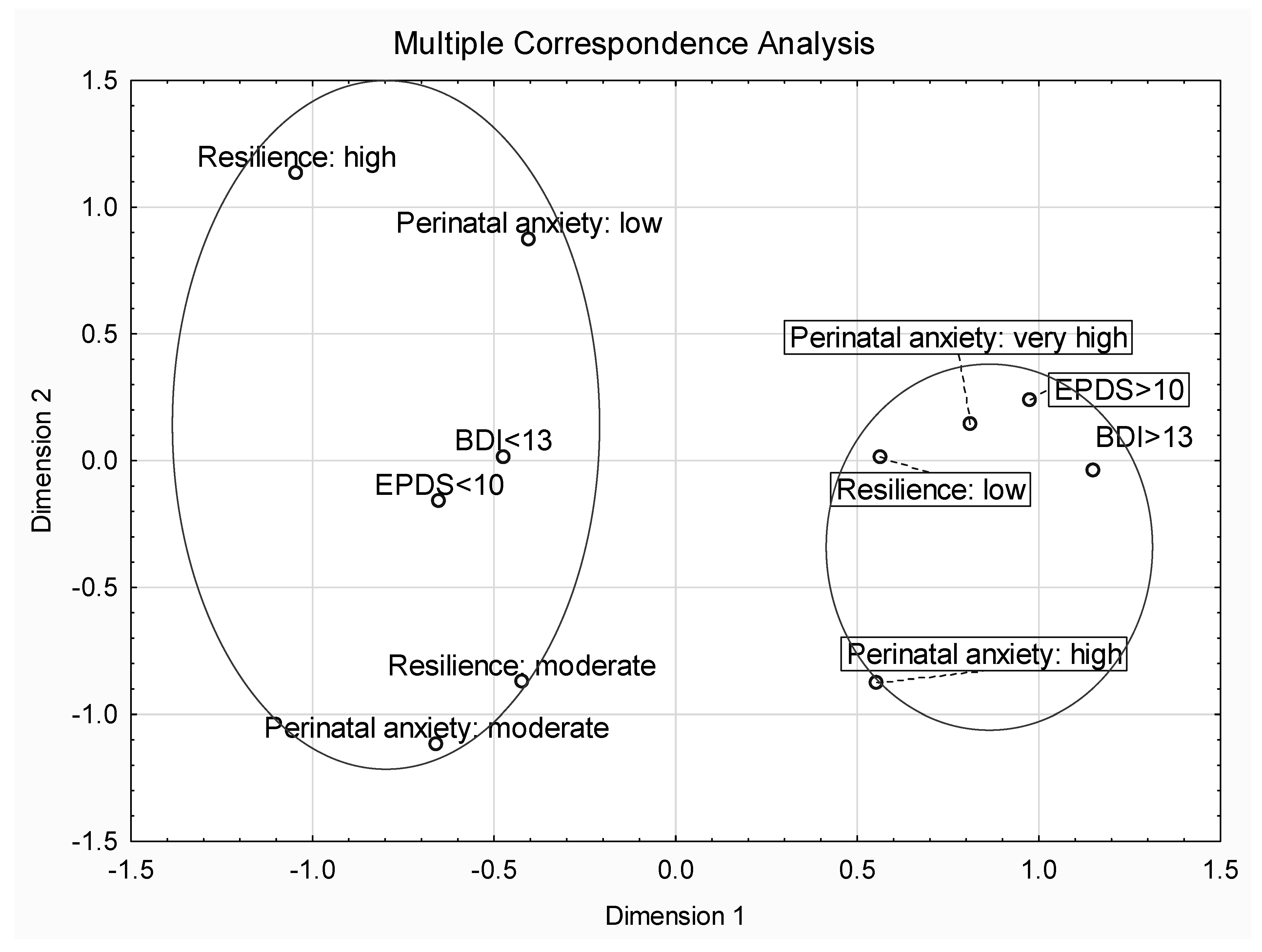
3.4. Relationship between Depressiveness, Labour Anxiety, COVID-Related Anxiety and Resilience
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Apter, G.; Devouche, E.; Gratier, M. Perinatal Mental Health. J. Nerv. Ment. Dis. 2011, 199, 575–577. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, M.W.; Wisner, K.L. Perinatal Mental Illness: Definition, Description and Aetiology. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Accortt, E.E.; Wong, M.S. It Is Time for Routine Screening for Perinatal Mood and Anxiety Disorders in Obstetrics and Gynecology Settings. Obstet. Gynecol. Surv. 2017, 72, 553–568. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, B.; Conde, A. Anxiety and Depression Symptoms in Women and Men from Early Pregnancy to 3-Months Postpartum: Parity Differences and Effects. J. Affect. Disord. 2011, 132, 146–157. [Google Scholar] [CrossRef]
- Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C.M. Identifying the Women at Risk of Antenatal Anxiety and Depression: A Systematic Review. J. Affect. Disord. 2016, 191, 62–77. [Google Scholar] [CrossRef]
- Howard, L.M.; Molyneaux, E.; Dennis, C.-L.; Rochat, T.; Stein, A.; Milgrom, J. Non-Psychotic Mental Disorders in the Perinatal Period. Lancet 2014, 384, 1775–1788. [Google Scholar] [CrossRef]
- Dennis, C.-L.; Falah-Hassani, K.; Shiri, R. Prevalence of Antenatal and Postnatal Anxiety: Systematic Review and Meta-Analysis. Br. J. Psychiatry 2017, 210, 315–323. [Google Scholar] [CrossRef]
- Stein, A.; Pearson, R.M.; Goodman, S.H.; Rapa, E.; Rahman, A.; McCallum, M.; Howard, L.M.; Pariante, C.M. Effects of Perinatal Mental Disorders on the Fetus and Child. Lancet 2014, 384, 1800–1819. [Google Scholar] [CrossRef]
- Marc, I.; Toureche, N.; Ernst, E.; Hodnett, E.D.; Blanchet, C.; Dodin, S.; Njoya, M.M. Mind-body Interventions during Pregnancy for Preventing or Treating Women’s Anxiety. Cochrane Database Syst. Rev. 2011, 2011, CD007559. [Google Scholar] [CrossRef]
- Fekadu Dadi, A.; Miller, E.R.; Mwanri, L. Antenatal Depression and Its Association with Adverse Birth Outcomes in Low and Middle-Income Countries: A Systematic Review and Meta-Analysis. PLoS ONE 2020, 15, e0227323. [Google Scholar] [CrossRef]
- Li, J.; Yin, J.; Waqas, A.; Huang, Z.; Zhang, H.; Chen, M.; Guo, Y.; Rahman, A.; Yang, L.; Li, X. Quality of Life in Mothers with Perinatal Depression: A Systematic Review and Meta-Analysis. Front. Psychiatry 2022, 13, 734836. [Google Scholar] [CrossRef] [PubMed]
- Acheampong, K.; Pan, X.; Kaminga, A.C.; Wen, S.W.; Liu, A. Risk of Adverse Maternal Outcomes Associated with Prenatal Exposure to Moderate-Severe Depression Compared with Mild Depression: A Fellow-up Study. J. Psychiatr. Res. 2021, 136, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Alvik, A.; Heyerdahl, S.; Haldorsen, T.; Lindemann, R. Alcohol Use before and during Pregnancy: A Population-Based Study. Acta Obstet. Gynecol. Scand. 2006, 85, 1292–1298. [Google Scholar] [CrossRef] [PubMed]
- Andersson, L.; Sundström-Poromaa, I.; Wulff, M.; Aström, M.; Bixo, M. Implications of Antenatal Depression and Anxiety for Obstetric Outcome. Obstet. Gynecol. 2004, 104, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Rollè, L.; Giordano, M.; Santoniccolo, F.; Trombetta, T. Prenatal Attachment and Perinatal Depression: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 2644. [Google Scholar] [CrossRef] [PubMed]
- O’Dea, G.A.; Youssef, G.J.; Hagg, L.J.; Francis, L.M.; Spry, E.A.; Rossen, L.; Smith, I.; Teague, S.J.; Mansour, K.; Booth, A.; et al. Associations between Maternal Psychological Distress and Mother-Infant Bonding: A Systematic Review and Meta-Analysis. Arch. Womens Ment. Health 2023, 26, 441–452. [Google Scholar] [CrossRef]
- Grigoriadis, S.; VonderPorten, E.H.; Mamisashvili, L.; Tomlinson, G.; Dennis, C.-L.; Koren, G.; Steiner, M.; Mousmanis, P.; Cheung, A.; Radford, K.; et al. The Impact of Maternal Depression during Pregnancy on Perinatal Outcomes: A Systematic Review and Meta-Analysis. J. Clin. Psychiatry 2013, 74, 8615. [Google Scholar] [CrossRef]
- Staneva, A.; Bogossian, F.; Pritchard, M.; Wittkowski, A. The Effects of Maternal Depression, Anxiety, and Perceived Stress during Pregnancy on Preterm Birth: A Systematic Review. Women Birth 2015, 28, 179–193. [Google Scholar] [CrossRef]
- Goodman, J.H. Perinatal Depression and Infant Mental Health. Arch. Psychiatr. Nurs. 2019, 33, 217–224. [Google Scholar] [CrossRef]
- Wu, Y.; Lu, Y.-C.; Jacobs, M.; Pradhan, S.; Kapse, K.; Zhao, L.; Niforatos-Andescavage, N.; Vezina, G.; du Plessis, A.J.; Limperopoulos, C. Association of Prenatal Maternal Psychological Distress with Fetal Brain Growth, Metabolism, and Cortical Maturation. JAMA Netw. Open 2020, 3, e1919940. [Google Scholar] [CrossRef]
- Rogers, A.; Obst, S.; Teague, S.J.; Rossen, L.; Spry, E.A.; Macdonald, J.A.; Sunderland, M.; Olsson, C.A.; Youssef, G.; Hutchinson, D. Association Between Maternal Perinatal Depression and Anxiety and Child and Adolescent Development: A Meta-Analysis. JAMA Pediatr. 2020, 174, 1082–1092. [Google Scholar] [CrossRef] [PubMed]
- Zelkowitz, P.; Papageorgiou, A. Maternal Anxiety: An Emerging Prognostic Factor in Neonatology. Acta Paediatr. 2005, 94, 1704–1705. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.-H.; Cai, L.; Cheng, Z.-S.; Cheng, H.; Deng, T.; Fan, Y.-P.; Fang, C.; Huang, D.; Huang, L.-Q.; Huang, Q.; et al. A Rapid Advice Guideline for the Diagnosis and Treatment of 2019 Novel Coronavirus (2019-nCoV) Infected Pneumonia (Standard Version). Mil. Med. Res. 2020, 7, 4. [Google Scholar] [CrossRef] [PubMed]
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The Psychological Impact of Quarantine and How to Reduce It: Rapid Review of the Evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [PubMed]
- Leung, C.M.C.; Ho, M.K.; Bharwani, A.A.; Cogo-Moreira, H.; Wang, Y.; Chow, M.S.C.; Fan, X.; Galea, S.; Leung, G.M.; Ni, M.Y. Mental Disorders Following COVID-19 and Other Epidemics: A Systematic Review and Meta-Analysis. Transl. Psychiatry 2022, 12, 205. [Google Scholar] [CrossRef]
- World Health Organization Guide for Integration of Perinatal Mental Health in Maternal and Child Health Services. Available online: https://www.who.int/publications-detail-redirect/9789240057142 (accessed on 3 January 2023).
- Thibaut, F.; ELNahas, G. Women’s Mental Health and Lessons Learnt from the COVID-19 Pandemic. Psychiatr. Clin. N. Am. 2023, 46, 415–426. [Google Scholar] [CrossRef]
- Bohren, M.A.; Berger, B.O.; Munthe-Kaas, H.; Tunçalp, Ö. Perceptions and Experiences of Labour Companionship: A Qualitative Evidence Synthesis. Cochrane Database Syst. Rev. 2019, 3, CD012449. [Google Scholar] [CrossRef]
- Opieka Okołoporodowa Podczas Pandemii COVID-19 w Świetle Doświadczeń Kobiet; Fundacja Rodzić po Ludzku: Warszawa, Poland, 2021.
- Wytyczne dla Poszczególnych Zakresów i Rodzajów Świadczeń—Ministerstwo Zdrowia—Portal Gov.pl. Available online: https://www.gov.pl/web/zdrowie/wytyczne-dla-poszczegolnych-zakresow-i-rodzajow-swiadczen (accessed on 14 September 2023).
- Wall, S.; Dempsey, M. The Effect of COVID-19 Lockdowns on Women’s Perinatal Mental Health: A Systematic Review. Women Birth 2022, 36, 47–55. [Google Scholar] [CrossRef]
- Hessami, K.; Romanelli, C.; Chiurazzi, M.; Cozzolino, M. COVID-19 Pandemic and Maternal Mental Health: A Systematic Review and Meta-Analysis. J. Matern. Fetal Neonatal Med. 2022, 35, 4014–4021. [Google Scholar] [CrossRef]
- Sisto, A.; Vicinanza, F.; Campanozzi, L.L.; Ricci, G.; Tartaglini, D.; Tambone, V. Towards a Transversal Definition of Psychological Resilience: A Literature Review. Medicina 2019, 55, 745. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, S.K.; Kunzler, A.M.; Kalisch, R.; Tüscher, O.; Lieb, K. Trajectories of Resilience and Mental Distress to Global Major Disruptions. Trends Cogn. Sci. 2022, 26, 1171–1189. [Google Scholar] [CrossRef] [PubMed]
- Kornfield, S.L.; White, L.K.; Waller, R.; Njoroge, W.; Barzilay, R.; Chaiyachati, B.H.; Himes, M.; Rodriguez, Y.; Riis, V.; Simonette, K.; et al. Risk and Resilience Factors Underlying Postpartum Depression and Impaired Mother-Infant Bonding during COVID-19. Health Aff. 2021, 40, 1566–1574. [Google Scholar] [CrossRef] [PubMed]
- Walker, A.L.; Witteveen, A.B.; Otten, R.H.J.; Verhoeven, C.J.; Henrichs, J.; de Jonge, A. Resilience-Enhancing Interventions for Antepartum Depressive Symptoms: Systematic Review. BJPsych Open 2022, 8, e89. [Google Scholar] [CrossRef]
- Bhamani, S.S.; Arthur, D.; Van Parys, A.-S.; Letourneau, N.; Wagnild, G.; Premji, S.S.; Asad, N.; Degomme, O. Resilience and Prenatal Mental Health in Pakistan: A Qualitative Inquiry. BMC Pregnancy Childbirth 2022, 22, 839. [Google Scholar] [CrossRef] [PubMed]
- Kishore, M.T.; Satyanarayana, V.; Ananthanpillai, S.T.; Desai, G.; Bhaskarapillai, B.; Thippeswamy, H.; Chandra, P.S. Life Events and Depressive Symptoms among Pregnant Women in India: Moderating Role of Resilience and Social Support. Int. J. Soc. Psychiatry 2018, 64, 570–577. [Google Scholar] [CrossRef]
- Ma, X.; Wang, Y.; Hu, H.; Tao, X.G.; Zhang, Y.; Shi, H. The Impact of Resilience on Prenatal Anxiety and Depression among Pregnant Women in Shanghai. J. Affect. Disord. 2019, 250, 57–64. [Google Scholar] [CrossRef]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of Postnatal Depression. Development of the 10-Item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G. Beck Depression Inventory–II 2011; APA PsycTests: Lawrence, KS, USA, 1996. [Google Scholar]
- National Collaborating Centre for Mental Health (UK). Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance: Updated Edition; National Institute for Health and Clinical Excellence: Guidance; British Psychological Society: Leicester, UK, 2014. [Google Scholar]
- Levis, B.; Negeri, Z.; Sun, Y.; Benedetti, A.; Thombs, B.D.; DEPRESsion Screening Data (DEPRESSD) EPDS Group. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for Screening to Detect Major Depression among Pregnant and Postpartum Women: Systematic Review and Meta-Analysis of Individual Participant Data. BMJ 2020, 371, m4022. [Google Scholar] [CrossRef]
- Sambrook Smith, M.; Cairns, L.; Pullen, L.S.W.; Opondo, C.; Fellmeth, G.; Alderdice, F. Validated Tools to Identify Common Mental Disorders in the Perinatal Period: A Systematic Review of Systematic Reviews. J. Affect. Disord. 2022, 298, 634–643. [Google Scholar] [CrossRef]
- Putyński, L.; Paciorek, M. Kwestionariusz Lęku Porodowego (KLP II) Wersja Zrewidowana—Konstrukcja i Właściwości Psychometryczne. Acta Univ. Lodz. Folia Psychol. 2008, 12. [Google Scholar] [CrossRef]
- Gąsior, K.; Chodkiewicz, J.; Cechowski, W. Kwestionariusz Oceny Prężności (KOP-26): Konstrukcja i Właściwości Psychometryczne Narzędzia. Pol. Psychol. Forum 2016, XXI, 76–92. [Google Scholar]
- Kaźmierczak, M.; Gebuza, G.; Gierszewska, M.; Bannach, M.; Mieczkowska, E.; Dombrowska-Pali, A.; Czubkowska, M. Screening for Detection of the Risk of Perinatal Mental Disorders among Women in Poland. Issues Ment. Health Nurs. 2020, 41, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Studniczek, A.; Kossakowska, K. Experiencing Pregnancy during the COVID-19 Lockdown in Poland: A Cross-Sectional Study of the Mediating Effect of Resiliency on Prenatal Depression Symptoms. Behav. Sci. 2022, 12, 371. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, M.A.; Leahy-Warren, P.; Khashan, A.S.; Kenny, L.C.; O’Neill, S.M. Worldwide Prevalence of Tocophobia in Pregnant Women: Systematic Review and Meta-Analysis. Acta Obstet. Gynecol. Scand. 2017, 96, 907–920. [Google Scholar] [CrossRef] [PubMed]
- Zilver, S.J.M.; Hendrix, Y.M.G.A.; Broekman, B.F.P.; de Leeuw, R.A.; de Groot, C.J.M.; van Pampus, M.G. Fear of Childbirth in Pregnancy Was Not Increased during the COVID-19 Pandemic in the Netherlands: A Cross-Sectional Study. Acta Obstet. Gynecol. Scand. 2022, 101, 1129–1134. [Google Scholar] [CrossRef]
- Han, L.; Bai, H.; Lun, B.; Li, Y.; Wang, Y.; Ni, Q. The Prevalence of Fear of Childbirth and Its Association with Intolerance of Uncertainty and Coping Styles Among Pregnant Chinese Women During the COVID-19 Pandemic. Front. Psychiatry 2022, 13, 935760. [Google Scholar] [CrossRef]
- Lyons, D.M.; Schatzberg, A.F. Chapter 3—Resilience as a Process Instead of a Trait. In Stress Resilience; Chen, A., Ed.; Academic Press: Cambridge, MA, USA, 2020; pp. 33–44. ISBN 978-0-12-813983-7. [Google Scholar]
- Ungar, M.; Theron, L. Resilience and Mental Health: How Multisystemic Processes Contribute to Positive Outcomes. Lancet Psychiatry 2020, 7, 441–448. [Google Scholar] [CrossRef]
- Ionio, C.; Gallese, M.; Fenaroli, V.; Smorti, M.; Greco, A.; Testa, I.; Zilioli, A.; Bonassi, L. COVID-19: What about Pregnant Women during First Lockdown in Italy? J. Reprod. Infant Psychol. 2022, 40, 577–589. [Google Scholar] [CrossRef]
- Kinser, P.A.; Jallo, N.; Amstadter, A.B.; Thacker, L.R.; Jones, E.; Moyer, S.; Rider, A.; Karjane, N.; Salisbury, A.L. Depression, Anxiety, Resilience, and Coping: The Experience of Pregnant and New Mothers During the First Few Months of the COVID-19 Pandemic. J. Womens Health 2021, 30, 654–664. [Google Scholar] [CrossRef]
- Lubián López, D.M.; Butrón Hinojo, C.A.; Arjona Bernal, J.E.; Fasero Laiz, M.; Alcolea Santiago, J.; Guerra Vilches, V.; Casaus Fernández, M.; Bueno Moral, A.; Olvera Perdigones, A.; Rodríguez Rodríguez, B.; et al. Resilience and Psychological Distress in Pregnant Women during Quarantine Due to the COVID-19 Outbreak in Spain: A Multicentre Cross-Sectional Online Survey. J. Psychosom. Obstet. Gynecol. 2021, 42, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Farewell, C.V.; Jewell, J.; Walls, J.; Leiferman, J.A. A Mixed-Methods Pilot Study of Perinatal Risk and Resilience During COVID-19. J. Prim. Care Community Health 2020, 11, 2150132720944074. [Google Scholar] [CrossRef]
- Bellomo, A.; Severo, M.; Petito, A.; Nappi, L.; Iuso, S.; Altamura, M.; Marconcini, A.; Giannaccari, E.; Maruotti, G.; Palma, G.L.; et al. Perinatal Depression Screening and Prevention: Descriptive Findings from a Multicentric Program in the South of Italy. Front. Psychiatry 2022, 13, 962948. [Google Scholar] [CrossRef] [PubMed]
- Di Paolo, A.-L.; King, S.; McLean, M.A.; Lequertier, B.; Elgbeili, G.; Kildea, S.; Dahlen, H.G. Prenatal Stress from the COVID-19 Pandemic Predicts Maternal Postpartum Anxiety as Moderated by Psychological Factors: The Australian BITTOC Study. J. Affect. Disord. 2022, 314, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Chi, N.-C.; Han, S.; Lin, S.-Y.; Fu, Y.-K.; Zhu, Z.; Nakad, L.; Demiris, G. Resilience-Enhancing Interventions for Family Caregivers: A Systematic Review. Chronic Illn. 2023, 0, 17423953231174928. [Google Scholar] [CrossRef]
- Norris, F.H.; Stevens, S.P.; Pfefferbaum, B.; Wyche, K.F.; Pfefferbaum, R.L. Community Resilience as a Metaphor, Theory, Set of Capacities, and Strategy for Disaster Readiness. Am. J. Community Psychol. 2008, 41, 127–150. [Google Scholar] [CrossRef]
- Ma, Y.; Deng, J.; Liu, Q.; Du, M.; Liu, M.; Liu, J. Long-Term Consequences of COVID-19 at 6 Months and Above: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6865. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and Mental Health: A Review of the Existing Literature. Asian J. Psychiatr. 2020, 52, 102066. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The Socio-Economic Implications of the Coronavirus Pandemic (COVID-19): A Review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Finstad, G.L.; Giorgi, G.; Lulli, L.G.; Pandolfi, C.; Foti, G.; León-Perez, J.M.; Cantero-Sánchez, F.J.; Mucci, N. Resilience, Coping Strategies and Posttraumatic Growth in the Workplace Following COVID-19: A Narrative Review on the Positive Aspects of Trauma. Int. J. Environ. Res. Public Health 2021, 18, 9453. [Google Scholar] [CrossRef]
- Yazdanimehr, R.; Omidi, A.; Sadat, Z.; Akbari, H. The Effect of Mindfulness-Integrated Cognitive Behavior Therapy on Depression and Anxiety among Pregnant Women: A Randomized Clinical Trial. J. Caring Sci. 2016, 5, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Jia, G.; Sun, S.; Ye, C.; Zhang, R.; Yu, X. Effects of an Online Mindfulness Intervention Focusing on Attention Monitoring and Acceptance in Pregnant Women: A Randomized Controlled Trial. J. Midwifery Womens Health 2019, 64, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Zemestani, M.; Fazeli Nikoo, Z. Effectiveness of Mindfulness-Based Cognitive Therapy for Comorbid Depression and Anxiety in Pregnancy: A Randomized Controlled Trial. Arch. Womens Ment. Health 2020, 23, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Aslami, E.; Alipour, A.; Najib, F.S.; Aghayosefi, A. A Comparative Study of Mindfulness Efficiency Based on Islamic-Spiritual Schemes and Group Cognitive Behavioral Therapy on Reduction of Anxiety and Depression in Pregnant Women. Int. J.Community Based Nurs. Midwifery 2017, 5, 144–152. [Google Scholar] [PubMed]
- Kozinszky, Z.; Dudas, R.B.; Devosa, I.; Csatordai, S.; Tóth, E.; Szabó, D.; Sikovanyecz, J.; Barabás, K.; Pál, A. Can a Brief Antepartum Preventive Group Intervention Help Reduce Postpartum Depressive Symptomatology? Psychother. Psychosom. 2012, 81, 98–107. [Google Scholar] [CrossRef]
- Lara, M.A.; Navarro, C.; Navarrete, L. Outcome Results of a Psycho-Educational Intervention in Pregnancy to Prevent PPD: A Randomized Control Trial. J. Affect. Disord. 2010, 122, 109–117. [Google Scholar] [CrossRef]
- Kumar, S.; Lee, N.K.; Pinkerton, E.; Wroblewski, K.E.; Lengyel, E.; Tobin, M. Resilience: A Mediator of the Negative Effects of Pandemic-Related Stress on Women’s Mental Health in the USA. Arch. Womens Ment. Health 2022, 25, 137–146. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| The Issue of Perinatal Care | Recommendations Resulting from the Pandemic |
|---|---|
| Family birth |
|
| Delivery of pregnant women infected with/suspected of COVID |
|
| Skin-to-skin contact after a cesarean section |
|
| Study Sample | [41] | |||
|---|---|---|---|---|
| KOP-26 | M | SD | M | SD |
| Family Relation (RR) | 44.36 | 8.79 | 46.46 | 7.26 |
| Personal Competence (KO) | 30.90 | 7.03 | 35.43 | 5.27 |
| Social Competence (KS) | 18.57 | 5.47 | 20.15 | 4.27 |
| Total score (WO) | 94.06 | 18.18 | 102.04 | 12.98 |
| Variable | Resilience Low | Resilience Average | Resilience High | X2 | p | |||
|---|---|---|---|---|---|---|---|---|
| Age | M = 30 | SD = 4.5 | M = 32 | SD = 3.2 | M = 31 | SD = 3.4 | ||
| Education | 0.964 | 0.618 | ||||||
| Higher education | N = 60 | 89.5% | N = 26 | 83.9% | N = 22 | 91.7% | ||
| Secondary education | N = 7 | 10.5% | N = 5 | 16.1% | N = 2 | 8.3% | ||
| Place of residence | 1.986 | 0.738 | ||||||
| Rural | N = 15 | 22.4% | N = 4 | 12.9% | N = 5 | 20.8% | ||
| City up to 100,000 residents | N = 11 | 16.4% | N = 8 | 25.8% | N = 5 | 20.8% | ||
| City with over 100,000 residents | N = 41 | 61.2% | N = 19 | 61.3% | N = 14 | 58.3% | ||
| Current pregnancy status | 0.855 | 0.652 | ||||||
| Healthy | N = 46 | 68.7% | N = 20 | 64.5% | N = 14 | 58.3% | ||
| Pregnancy Complications | N = 21 | 31.3% | N = 11 | 35.5% | N = 10 | 41.7% | ||
| Pregnancy | 3.801 | 0.434 | ||||||
| First | N = 30 | 44.8% | N = 11 | 35.5% | N = 10 | 41.7% | ||
| Second | N = 21 | 31.3% | N = 13 | 41.9% | N = 5 | 20.8% | ||
| Third and subsequent | N = 16 | 23.9% | N = 7 | 22.6 | N = 9 | 37.5 | ||
| Previous diagnosis of mental disorders | 1.096 | 0.578 | ||||||
| No | N = 52 | 77.6% | N = 25 | 80.6% | N = 21 | 87.5% | ||
| Yes | N = 15 | 22.4% | N = 6 | 19.4% | N = 3 | 12.5% | ||
| Previous COVID-19 infection | 0.030 | 0.985 | ||||||
| No | N = 52 | 77.6% | N = 24 | 77.4% | N = 19 | 79.2% | ||
| Yes | N = 15 | 22.4% | N = 7 | 22.6% | N = 5 | 20.8% | ||
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Perinatal depression BDI–II 1 | 1 | |||||||||
| 2. Perinatal depression EPDS 1 | 0.17 | 1 | ||||||||
| 3. Perinatal depression BDI–II 2 | −0.56 | 0.99 | 1 | |||||||
| 4. Perinatal depression EPDS 2 | 0.34 | 0.76 | 0.63 | 1 | ||||||
| 5. CRAQ | 0.01 | 0.19 | 0.30 | −0.26 | 1 | |||||
| 6. LA | 0.39 | −0.11 | 0.20 | −0.08 | 0.14 | 1 | ||||
| 7. Resilience Total score (WO) | −0.39 | −0.46 | −0.64 | −0.36 | −0.07 | −0.21 | 1 | |||
| 8. Resilience Social Competence (KS) | −0.34 | −0.29 | −0.38 | −0.31 | −0.04 | −0.18 | 0.66 | 1 | ||
| 9. Resilience Family Relations (RR) | −0.24 | −0.41 | −0.64 | −0.25 | −0.03 | −0.09 | 0.90 | 0.34 | 1 | |
| 10. Resilience Personal Competence (KO) | −0.43 | −0.47 | −0.80 | −0.37 | −0.11 | −0.29 | 0.93 | 0.50 | 0.81 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sójta, K.; Margulska, A.; Plewka, M.; Płeska, K.; Strzelecki, D.; Gawlik-Kotelnicka, O. Resilience and Psychological Well-Being of Polish Women in the Perinatal Period during the COVID-19 Pandemic. J. Clin. Med. 2023, 12, 6279. https://doi.org/10.3390/jcm12196279
Sójta K, Margulska A, Plewka M, Płeska K, Strzelecki D, Gawlik-Kotelnicka O. Resilience and Psychological Well-Being of Polish Women in the Perinatal Period during the COVID-19 Pandemic. Journal of Clinical Medicine. 2023; 12(19):6279. https://doi.org/10.3390/jcm12196279
Chicago/Turabian StyleSójta, Klaudia, Aleksandra Margulska, Maksymilian Plewka, Kacper Płeska, Dominik Strzelecki, and Oliwia Gawlik-Kotelnicka. 2023. "Resilience and Psychological Well-Being of Polish Women in the Perinatal Period during the COVID-19 Pandemic" Journal of Clinical Medicine 12, no. 19: 6279. https://doi.org/10.3390/jcm12196279