
First-in-Human Drug-Eluting Balloon Treatment of Vulnerable Lipid-Rich Plaques: Rationale and Design of the DEBuT-LRP Study

 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
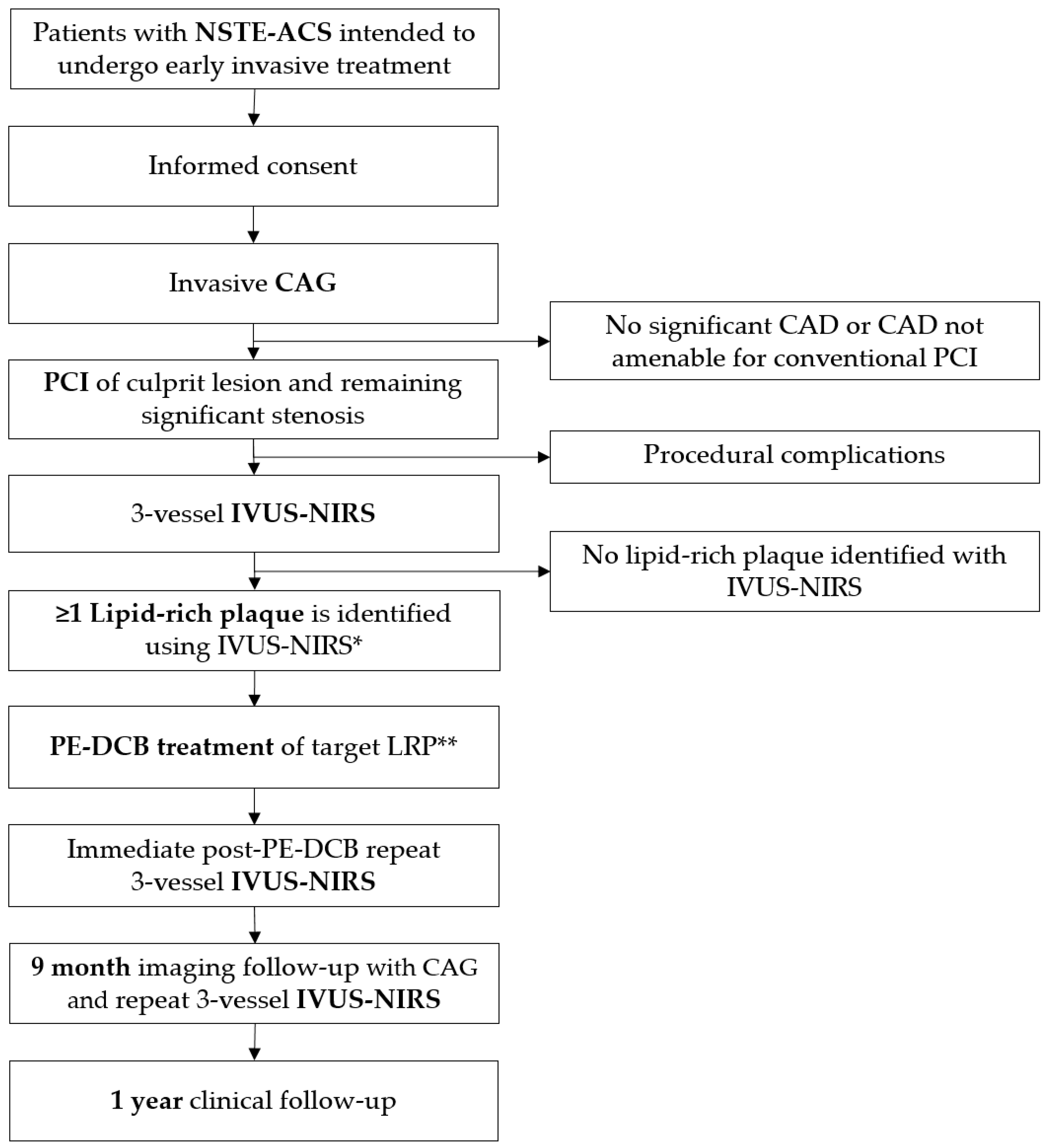
2.1. Overview
2.2. Patient Selection
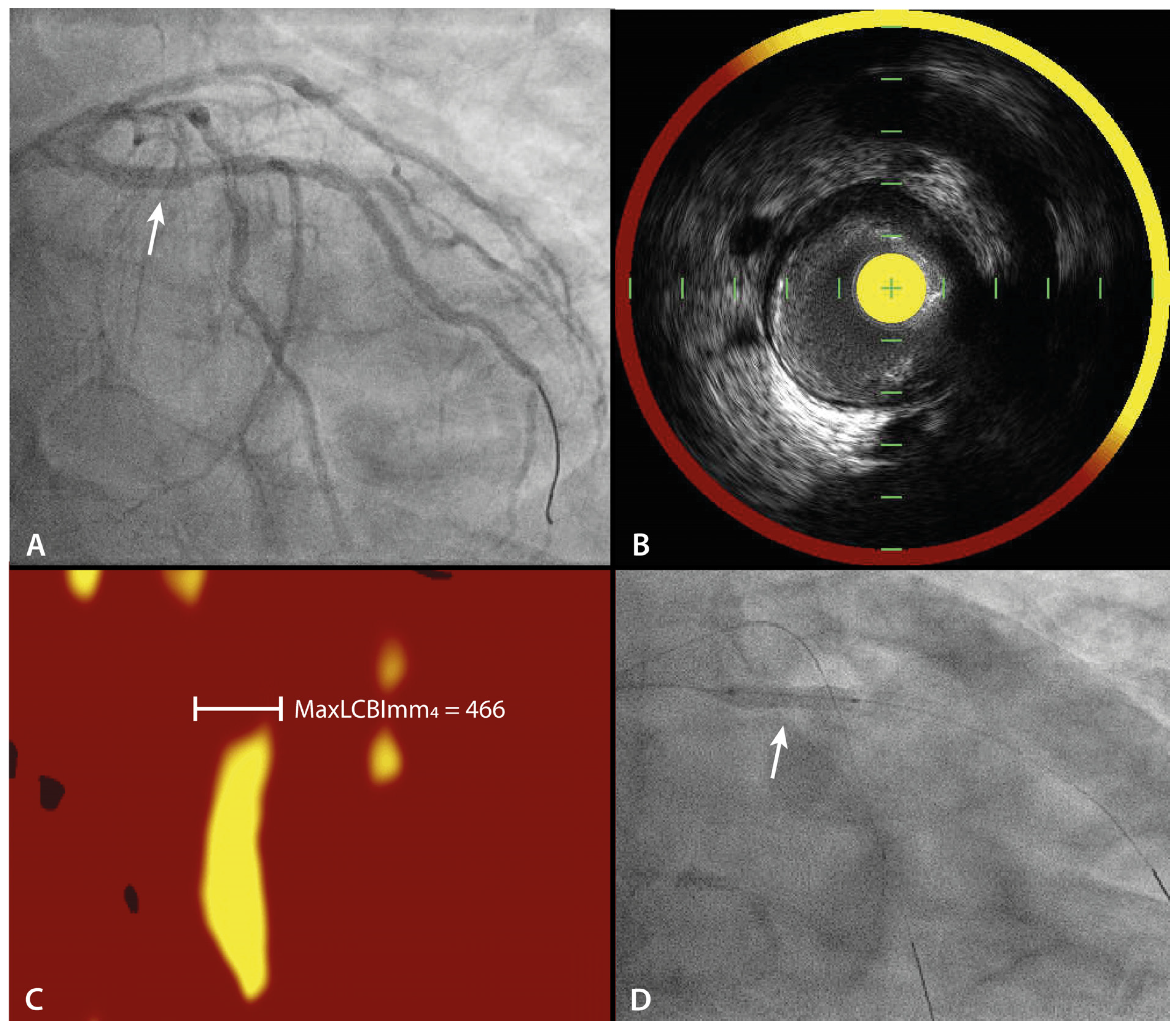
2.3. Imaging
2.4. Investigational Treatment
2.5. Imaging Analysis
2.6. Study Endpoints
2.7. Follow-Up
2.8. Statistical Considerations
2.9. Safety
3. Current Status
4. Discussion
4.1. Prognostic Impact of a Lipid-Rich Plaque
4.2. Systemic Treatment vs. Local Treatment
4.3. Drug-Eluting Stent vs. Drug-Eluting Balloon
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sanchis-Gomar, F.; Perez-Quilis, C.; Leischik, R.; Lucia, A. Epidemiology of coronary heart disease and acute coronary syndrome. Ann. Transl. Med. 2016, 4, 256. [Google Scholar] [CrossRef] [PubMed]
- Cutlip, D.; Chhabra, A.; Baim, D. Beyond restenosis: Five-year clinical outcomes from second-generation coronary stent trials. Circulation 2004, 110, 1226–1230. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Maehara, A.; Lansky, A.J.; De Bruyne, B.; Cristea, E.; Mintz, G.S.; Mehran, R.; McPherson, J.; Farhat, N.; Marso, S.P.; et al. A prospective natural-history study of coronary atherosclerosis. N. Engl. J. Med. 2011, 364, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Waksman, R.; Di Mario, C.; Torguson, R.; Ali, Z.A.; Singh, V.; Skinner, W.H.; Artis, A.K.; Cate, T.T.; Powers, E.; Kim, C.; et al. Identification of patients and plaques vulnerable to future coronary events with near-infrared spectroscopy intravascular ultrasound imaging: A prospective, cohort study. Lancet 2019, 394, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- van Veelen, A.; van der Sangen, N.M.R.; Delewi, R.; Beijk, M.A.M.; Henriques, J.P.S.; Claessen, B.E.P.M. Detection of Vulnerable Coronary Plaques Using Invasive and Non-Invasive Imaging Modalities. J. Clin. Med. 2022, 11, 1361. [Google Scholar] [CrossRef]
- Erlinge, D.; Maehara, A.; Ben-Yehuda, O.; Bøtker, H.E.; Maeng, M.; Kjøller-Hansen, L.; Engstrøm, T.; Matsumura, M.; Crowley, A.; Dressler, O.; et al. Identification of vulnerable plaques and patients by intracoronary near-infrared spectroscopy and ultrasound (PROSPECT II): A prospective natural history study. Lancet 2021, 397, 985–995. [Google Scholar] [CrossRef]
- Kolodgie, F.D.; Virmani, R.; Burke, A.P.; Farb, A.; Weber, D.K.; Kutys, R.; Finn, A.V.; Gold, H.K. Pathologic assessment of the vulnerable human coronary plaque. Heart (Br. Card. Soc.) 2004, 90, 1385–1391. [Google Scholar] [CrossRef]
- Gardner, C.M.; Tan, H.; Hull, E.L.; Lisauskas, J.B.; Sum, S.T.; Meese, T.M.; Jiang, C.; Madden, S.P.; Caplan, J.D.; Burke, A.P.; et al. Detection of lipid core coronary plaques in autopsy specimens with a novel catheter-based near-infrared spectroscopy system. JACC Cardiovasc. Imaging 2008, 1, 638–648. [Google Scholar] [CrossRef]
- Stone, G.W.; Maehara, A.; Ali, Z.A.; Held, C.; Matsumura, M.; Kjøller-Hansen, L.; Bøtker, H.E.; Maeng, M.; Engstrøm, T.; Wiseth, R.; et al. Percutaneous Coronary Intervention for Vulnerable Coronary Atherosclerotic Plaque. J. Am. Coll. Cardiol. 2020, 76, 2289–2301. [Google Scholar] [CrossRef]
- Baan, J.; Claessen, B.E.; Dijk, K.B.V.; Vendrik, J.; van der Schaaf, R.J.; Meuwissen, M.; van Royen, N.; Marcel Gosselink, A.T.; van Wely, M.H.; Dirkali, A.; et al. A Randomized Comparison of Paclitaxel-Eluting Balloon Versus Everolimus-Eluting Stent for the Treatment of Any In-Stent Restenosis: The DARE Trial. JACC Cardiovasc. Interv. 2018, 11, 275–283. [Google Scholar] [CrossRef]
- Jeger, R.V.; Farah, A.; Ohlow, M.-A.; Mangner, N.; Möbius-Winkler, S.; Leibundgut, G.; Weilenmann, D.; Wöhrle, J.; Richter, S.; Schreiber, M.; et al. Drug-coated balloons for small coronary artery disease (BASKET-SMALL 2): An open-label randomised non-inferiority trial. Lancet 2018, 392, 849–856. [Google Scholar] [CrossRef]
- Liu, L.; Liu, B.; Ren, J.; Hui, G.; Qi, C.; Wang, J. Comparison of drug-eluting balloon versus drug-eluting stent for treatment of coronary artery disease: A meta-analysis of randomized controlled trials. BMC Cardiovasc. Disord 2018, 18, 46. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, M.M.; Singh, K.; Albaghdadi, M.S.; Khraishah, H.; Mauskapf, A.; Kessinger, C.W.; Osborn, E.A.; Kellnberger, S.; Piao, Z.; Cardenas, C.L.L.; et al. Paclitaxel Drug-Coated Balloon Angioplasty Suppresses Progression and Inflammation of Experimental Atherosclerosis in Rabbits. JACC Basic Transl. Sci. 2020, 5, 685–695. [Google Scholar] [CrossRef] [PubMed]
- Ann, S.H.; Balbir Singh, G.; Lim, K.H.; Koo, B.K.; Shin, E.S. Anatomical and Physiological Changes after Paclitaxel-Coated Balloon for Atherosclerotic De Novo Coronary Lesions: Serial IVUS-VH and FFR Study. PLoS ONE 2016, 11, e0147057. [Google Scholar] [CrossRef]
- Her, A.-Y.; Shin, E.-S.; Chung, J.-H.; Kim, Y.H.; Garg, S.; Lee, J.M.; Doh, J.-H.; Nam, C.-W.; Koo, B.-K. Plaque modification and stabilization after paclitaxel-coated balloon treatment for de novo coronary lesions. Heart Vessel. 2019, 34, 1113–1121. [Google Scholar] [CrossRef]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.-A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes: Developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC). Eur. Heart J. 2023. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Madder, R.D.; Goldstein, J.A.; Madden, S.P.; Puri, R.; Wolski, K.; Hendricks, M.; Sum, S.T.; Kini, A.; Sharma, S.; Rizik, D.; et al. Detection by near-infrared spectroscopy of large lipid core plaques at culprit sites in patients with acute ST-segment elevation myocardial infarction. JACC Cardiovasc. Interv. 2013, 6, 838–846. [Google Scholar] [CrossRef]
- Madder, R.D.; Husaini, M.; Davis, A.T.; Van Oosterhout, S.; Harnek, J.; Götberg, M.; Erlinge, D. Detection by near-infrared spectroscopy of large lipid cores at culprit sites in patients with non-ST-segment elevation myocardial infarction and unstable angina. Catheter. Cardiovasc. Interv. Off. J. Soc. Card. Angiogr. Interv. 2015, 86, 1014–1021. [Google Scholar] [CrossRef]
- Garcia-Garcia, H.M.; McFadden, E.P.; Farb, A.; Mehran, R.; Stone, G.W.; Spertus, J.; Onuma, Y.; Morel, M.-A.; van Es, G.-A.; Zuckerman, B.; et al. Standardized End Point Definitions for Coronary Intervention Trials: The Academic Research Consortium-2 Consensus Document. Circulation 2018, 137, 2635–2650. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.A. Fourth Universal Definition of Myocardial Infarction (2018). Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef] [PubMed]
- Campeau, L. Letter: Grading of angina pectoris. Circulation 1976, 54, 522–523. [Google Scholar] [CrossRef] [PubMed]
- The Criteria Committee of the New York Heart Association. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels, 9th ed.; Little, Brown & Co: Boston, MA, USA, 1994; pp. 253–256. [Google Scholar]
- Mol, J.Q.; Bom, M.J.; Damman, P.; Knaapen, P.; van Royen, N. Pre-Emptive OCT-Guided Angioplasty of Vulnerable Intermediate Coronary Lesions: Results from the Prematurely Halted PECTUS-Trial. J. Interv. Cardiol. 2020, 2020, 8821525. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.G.; Steg, P.G.; Szarek, M.; Bhatt, D.L.; Bittner, V.A.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; Hanotin, C.; Harrington, R.A.; et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N. Engl. J. Med. 2018, 379, 2097–2107. [Google Scholar] [CrossRef] [PubMed]
- Ferri, N.; Ruscica, M.; Lupo, M.G.; Vicenzi, M.; Sirtori, C.R.; Corsini, A. Pharmacological rationale for the very early treatment of acute coronary syndrome with monoclonal antibodies anti-PCSK9. Pharmacol. Res. 2022, 184, 106439. [Google Scholar] [CrossRef]
- Nicholls, S.J.; Kataoka, Y.; Nissen, S.E.; Prati, F.; Windecker, S.; Puri, R.; Hucko, T.; Aradi, D.; Herrman, J.-P.R.; Hermanides, R.S.; et al. Effect of Evolocumab on Coronary Plaque Phenotype and Burden in Statin-Treated Patients Following Myocardial Infarction. JACC Cardiovasc. Imaging 2022, 15, 1308–1321. [Google Scholar] [CrossRef]
- Nicholls, S.J.; Puri, R.; Anderson, T.; Ballantyne, C.M.; Cho, L.; Kastelein, J.J.; Koenig, W.; Somaratne, R.; Kassahun, H.; Yang, J.; et al. Effect of Evolocumab on Progression of Coronary Disease in Statin-Treated Patients: The GLAGOV Randomized Clinical Trial. Jama 2016, 316, 2373–2384. [Google Scholar] [CrossRef]
- Räber, L.; Ueki, Y.; Otsuka, T.; Losdat, S.; Häner, J.D.; Lonborg, J.; Fahrni, G.; Iglesias, J.F.; van Geuns, R.-J.; Ondracek, A.S.; et al. Effect of Alirocumab Added to High-Intensity Statin Therapy on Coronary Atherosclerosis in Patients With Acute Myocardial Infarction: The PACMAN-AMI Randomized Clinical Trial. Jama 2022, 327, 1771–1781. [Google Scholar] [CrossRef]
- Nidorf, S.M.; Fiolet, A.T.; Mosterd, A.; Eikelboom, J.W.; Schut, A.; Opstal, T.S.; The, S.H.K.; Xu, X.-F.; Ireland, M.A.; Lenderink, T.; et al. Colchicine in Patients with Chronic Coronary Disease. N. Engl. J. Med. 2020, 383, 1838–1847. [Google Scholar] [CrossRef]
- Vaidya, K.; Arnott, C.; Martínez, G.J.; Ng, B.; McCormack, S.; Sullivan, D.R.; Celermajer, D.S.; Patel, S. Colchicine Therapy and Plaque Stabilization in Patients With Acute Coronary Syndrome: A CT Coronary Angiography Study. JACC Cardiovasc. Imaging 2018, 11, 305–316. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion Criteria |
|---|
|
|
| Exclusion Criteria |
| Angiographic exclusion criteria |
|
|
|
|
| Clinical exclusion criteria |
|
|
|
|
|
|
|
|
|
| Primary Endpoint |
|---|
| Change in maxLCBImm4 between baseline and 9 months follow-upin PE-DCB treated LRPs. |
| Secondary Endpoints |
|
| PE-DCB (n = 20) | |
|---|---|
| Age, (years) | 66 (55–73) |
| Male | 18 (90%) |
| Body mass index, (kg/m2) | 26.4 (23.3–36.4) * |
| Current tobacco use | 3 (15%) ** |
| Chronic obstructive pulmonary disease | 1 (5%) |
| Diabetes mellitus | 1 (5%) |
| Hypertension | 11 (55%) |
| Hypercholesterolemia | 12 (60%) |
| Family history of coronary artery disease | 5 (39%) *** |
| Prior myocardial infarction | 3 (15%) |
| Prior percutaneous coronary intervention | 3 (15%) |
| Prior bypass graft surgery | 0 (0%) |
| Prior stroke | 1 (5%) |
| Laboratory measures | |
| Total cholesterol, (mmol/L) | 5.0 (4.2–6.4) **** |
| High-density lipoprotein, (mmol/L) | 1.1 (1.0–1.3) ***** |
| Low-density lipoprotein, (mmol/L) | 2.8 (2.2–4.0) ***** |
| Triglycerides, (mmol/L) | 1.9 (1.2–2.6) ***** |
| Hemoglobin, (mmol/L) | 9.3 (8.7–10.1) |
| Leucocytes, (×109/L) | 7.7 (6.2–11.4) ****** |
| Thrombocytes, (×109/L) | 204 (188–221) |
| Lipid-lowering medication prior to admission | 9 (45%) |
| Statin | 9 (45%) |
| Ezetimibe | 0 (0%) |
| PCSK9 inhibitor | 0 (0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Veelen, A.; Küçük, I.T.; Fuentes, F.H.; Kahsay, Y.; Garcia-Garcia, H.M.; Delewi, R.; Beijk, M.A.M.; den Hartog, A.W.; Grundeken, M.J.; Vis, M.M.; et al. First-in-Human Drug-Eluting Balloon Treatment of Vulnerable Lipid-Rich Plaques: Rationale and Design of the DEBuT-LRP Study. J. Clin. Med. 2023, 12, 5807. https://doi.org/10.3390/jcm12185807
van Veelen A, Küçük IT, Fuentes FH, Kahsay Y, Garcia-Garcia HM, Delewi R, Beijk MAM, den Hartog AW, Grundeken MJ, Vis MM, et al. First-in-Human Drug-Eluting Balloon Treatment of Vulnerable Lipid-Rich Plaques: Rationale and Design of the DEBuT-LRP Study. Journal of Clinical Medicine. 2023; 12(18):5807. https://doi.org/10.3390/jcm12185807
Chicago/Turabian Stylevan Veelen, Anna, I. Tarik Küçük, Federico H. Fuentes, Yirga Kahsay, Hector M. Garcia-Garcia, Ronak Delewi, Marcel A. M. Beijk, Alexander W. den Hartog, Maik J. Grundeken, M. Marije Vis, and et al. 2023. "First-in-Human Drug-Eluting Balloon Treatment of Vulnerable Lipid-Rich Plaques: Rationale and Design of the DEBuT-LRP Study" Journal of Clinical Medicine 12, no. 18: 5807. https://doi.org/10.3390/jcm12185807