
Development of Notch-Free, Pre-Bent Rod Applicable for Posterior Corrective Surgery of Thoracolumbar/Lumbar Adolescent Idiopathic Scoliosis

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Radiographic Parameters
2.3. Rod Angle
2.4. Surgical Techniques
2.5. Algorithm for Analyzing and Identifying the Optimal Rod Shapes
- Step 1: Generation of a center point cloud for existing rod shapes
- Step 2: Hierarchical cluster analysis for length-based grouping of the existing rods
- Step 3: Evaluation of geometric difference among rods using a modified iterative closest point (ICP) method
- Step 4: Evaluation of rod shape difference
- Step 5: Hierarchical cluster analysis among rod shapes
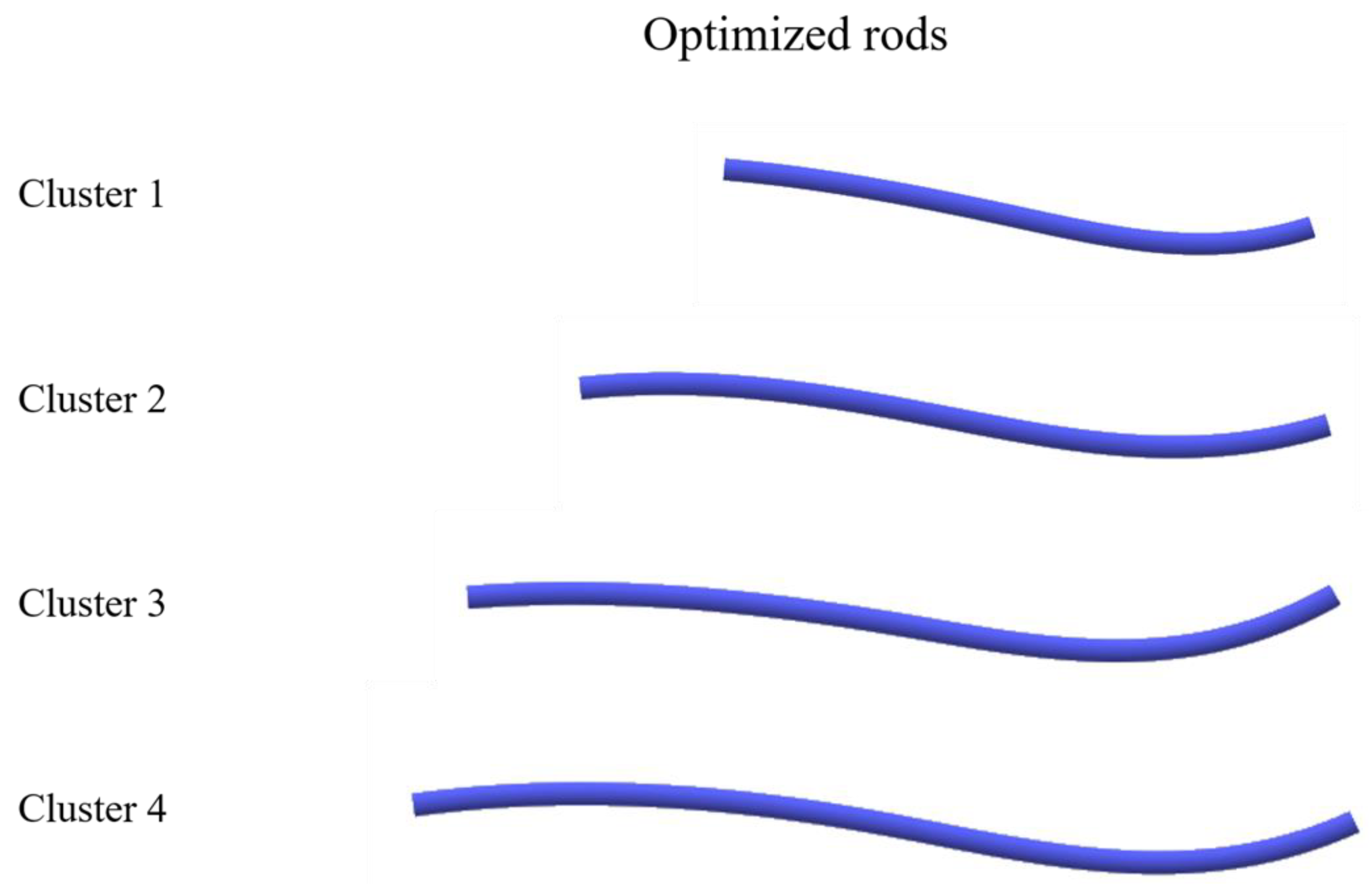
- Step 6: Derivation of a pre-bent and pre-cut rod shape from the representative curve in rod subgroups
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Altaf, F.; Gibson, A.; Dannawi, Z.; Noordeen, H. Adolescent idiopathic scoliosis. BMJ 2013, 346, f2508. [Google Scholar] [CrossRef] [PubMed]
- Addai, D.; Zarkos, J.; Bowey, A.J. Current concepts in the diagnosis and management of adolescent idiopathic scoliosis. Child’s Nerv. Syst. 2020, 36, 1111–1119. [Google Scholar] [CrossRef] [PubMed]
- Lenke, L.G.; Betz, R.R.; Harms, J.; Bridwell, K.H.; Clements, D.H.; Lowe, T.G.; Blanke, K. Adolescent idiopathic scoliosis: A new classification to determine extent of spinal arthrodesis. J. Bone Joint Surg. Am. 2001, 83, 1169–1181. [Google Scholar] [CrossRef] [PubMed]
- Hosseinpour-Feizi, H.; Soleimanpour, J.; Sales, J.G.; Arzroumchilar, A. Lenke and King classification systems for adolescent idiopathic scoliosis: Interobserver agreement and postoperative results. Int. J. Gen. Med. 2011, 4, 821–825. [Google Scholar] [CrossRef]
- Ovadia, D. Classification of adolescent idiopathic scoliosis (AIS). J. Child. Orthop. 2013, 7, 25–28. [Google Scholar] [CrossRef]
- Lenke, L.G.; Betz, R.R.; Clements, D.; Merola, A.; Haher, T.; Lowe, T.; Newton, P.; Bridwell, K.H.; Blanke, K. Curve prevalence of a new classification of operative adolescent idiopathic scoliosis: Does classification correlate with treatment? Spine 2002, 27, 604–611. [Google Scholar] [CrossRef]
- Helenius, I. Anterior surgery for adolescent idiopathic scoliosis. J. Child. Orthop 2013, 7, 63–68. [Google Scholar] [CrossRef]
- Chen, Z.; Rong, L. Comparison of combined anterior-posterior approach versus posterior-only approach in treating adolescent idiopathic scoliosis: A meta-analysis. Eur. Spine J. 2016, 25, 363–371. [Google Scholar] [CrossRef]
- Abel, M.F.; Singla, A.; Feger, M.A.; Sauer, L.D.; Novicoff, W. Surgical treatment of Lenke 5 adolescent idiopathic scoliosis: Comparison of anterior vs posterior approach. World J. Orthop. 2016, 7, 553–560. [Google Scholar] [CrossRef]
- O’Donnell, C.; Michael, N.; Pan, X.; Emans, J.; Garg, S.; Erickson, M. Anterior Spinal Fusion and Posterior Spinal Fusion Both Effectively Treat Lenke Type 5 Curves in Adolescent Idiopathic Scoliosis: A Multicenter Study. Spine Deform. 2018, 6, 231–240. [Google Scholar] [CrossRef]
- Hirase, T.; Ling, J.F.; Haghshenas, V.; Thirumavalavan, J.; Dong, D.; Hanson, D.S.; Marco, R.A.W. Anterior versus posterior spinal fusion for Lenke type 5 adolescent idiopathic scoliosis: A systematic review and meta-analysis of comparative studies. Spine Deform. 2022, 10, 267–281. [Google Scholar] [CrossRef]
- Wang, Z.W.; Shen, Y.Q.; Wu, Y.; Li, J.; Liu, Z.; Xu, J.K.; Chen, Q.X.; Chen, W.S.; Chen, L.W.; Zhang, N.; et al. Anterior Selective Lumbar Fusion Saving More Distal Fusion Segments Compared with Posterior Approach in the Treatment of Adolescent Idiopathic Scoliosis with Lenke Type 5: A Cohort Study with More Than 8-Year Follow-up. Orthop. Surg. 2021, 13, 2327–2334. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Wang, W.; Shen, M.; Xia, L. Anterior versus posterior approach in Lenke 5C adolescent idiopathic scoliosis: A meta-analysis of fusion segments and radiological outcomes. J. Orthop. Surg. Res. 2016, 11, 77. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Han, B.; Sun, D.; Hai, Y.; Yin, P.; Liu, Y.; Yang, J. Surgical Treatment of Scoliosis Lenke Type 5, Anterior Versus Posterior, Which Approach is Better?: A Systematic Review and Meta-Analysis. Spine 2023, 48, E223–E234. [Google Scholar] [CrossRef] [PubMed]
- Yoshihara, H. Surgical Treatment of Lenke Type 5 Adolescent Idiopathic Scoliosis: A Systematic Review. Spine 2019, 44, E788–E799. [Google Scholar] [CrossRef]
- Kokabu, T.; Kanai, S.; Abe, Y.; Iwasaki, N.; Sudo, H. Identification of optimized rod shapes to guide anatomical spinal reconstruction for adolescent thoracic idiopathic scoliosis. J. Orthop. Res. 2018, 36, 3219–3224. [Google Scholar] [CrossRef]
- Lindsey, C.; Deviren, V.; Xu, Z.; Yeh, R.F.; Puttlitz, C.M. The effects of rod contouring on spinal construct fatigue strength. Spine 2006, 31, 1680–1687. [Google Scholar] [CrossRef]
- Ferrero, E.; Mazda, K.; Simon, A.L.; Ilharreborde, B. Preliminary experience with SpineEOS, a new software for 3D planning in AIS surgery. Eur. Spine J. 2018, 27, 2165–2174. [Google Scholar] [CrossRef]
- Sudo, H.; Tachi, H.; Kokabu, T.; Yamada, K.; Iwata, A.; Endo, T.; Takahata, M.; Abe, Y.; Iwasaki, N. In vivo deformation of anatomically pre-bent rods in thoracic adolescent idiopathic scoliosis. Sci. Rep. 2021, 11, 12622. [Google Scholar] [CrossRef]
- Seki, S.; Newton, P.O.; Yahara, Y.; Makino, H.; Nakano, M.; Hirano, N.; Kawaguchi, Y.; Kimura, T. Differential Rod Contouring is Essential for Improving Vertebral Rotation in Patients with Adolescent Idiopathic Scoliosis: Thoracic Curves Assessed with Intraoperative CT. Spine 2018, 43, E585–E591. [Google Scholar] [CrossRef]
- Cidambi, K.R.; Glaser, D.A.; Bastrom, T.P.; Nunn, T.N.; Ono, T.; Newton, P.O. Postoperative changes in spinal rod contour in adolescent idiopathic scoliosis: An in vivo deformation study. Spine 2012, 37, 1566–1572. [Google Scholar] [CrossRef] [PubMed]
- Salmingo, R.; Tadano, S.; Fujisaki, K.; Abe, Y.; Ito, M. Corrective force analysis for scoliosis from implant rod deformation. Clin. Biomech. 2012, 27, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Soutome, A.; Kanai, S.; Date, H.; Kokabu, T.; Abe, Y.; Moridaira, H.; Taneichi, H.; Sudo, H. Preliminary Shape Similarity Analysis and Standardization for Pre-Bent Rod Design for Adult Spinal Deformity Correction. Comput. Aided Des. Appl. 2023, 20, 797–813. [Google Scholar] [CrossRef]
- Besl, P.J.; McKay, H.D. A method for registration of 3-D shapes. IEEE Trans. Pattern Anal. Mach. Intell. 1992, 1611, 586–606. [Google Scholar] [CrossRef]
- Bowden, D.; Michielli, A.; Merrill, M.; Will, S. Systematic review and meta-analysis for the impact of rod materials and sizes in the surgical treatment of adolescent idiopathic scoliosis. Spine Deform. 2022, 10, 1245–1263. [Google Scholar] [CrossRef]
- Lee, Y.; Welsch, G. Young’s modulus and damping of Ti 6Al 4 Valloy as a function of heat treatment and oxygen concentration. Mater. Sci. Eng. A Struct. Mater. 1990, 128, 77–89. [Google Scholar] [CrossRef]
- Fan, Z. On the young’s moduli of Ti 6Al 4V alloys. Scr. Metall. Mater. 1993, 29, 1427–1432. [Google Scholar] [CrossRef]
- Sabah, Y.; Clément, J.L.; Solla, F.; Rosello, O.; Rampal, V. Cobalt-chrome and titanium alloy rods provide similar coronal and sagittal correction in adolescent idiopathic scoliosis. Orthop. Traumatol. Surg. Res. 2018, 104, 1073–1077. [Google Scholar] [CrossRef]
- Staiger, M.P.; Pietak, A.M.; Huadmai, J.; Dias, G. Magnesium and its alloys as orthopedic biomaterials: A review. J. Biomater. 2006, 27, 1728–1734. [Google Scholar] [CrossRef]
- Nguyen, T.Q.; Buckley, J.M.; Ames, C.; Deviren, V. The fatigue life of contoured cobalt chrome posterior spinal fusion rods. Proc. Inst. Mech. Eng. H 2011, 225, 194–198. [Google Scholar] [CrossRef]
- Demura, S.; Murakami, H.; Hayashi, H.; Kato, S.; Yoshioka, K.; Yokogawa, N.; Ishii, T.; Igarashi, T.; Fang, X.; Tsuchiya, H. Influence of Rod Contouring on Rod Strength and Stiffness in Spine Surgery. Orthopedics 2015, 38, e520-3. [Google Scholar] [CrossRef]
- Solla, F.; Barrey, C.Y.; Burger, E.; Kleck, C.J.; Fière, V. Patient-specific Rods for Surgical Correction of Sagittal Imbalance in Adults: Technical Aspects and Preliminary Results. Clin. Spine Surg. 2019, 32, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Solla, F.; Clément, J.L.; Cunin, V.; Bertoncelli, C.M.; Fière, V.; Rampal, V. Patient-specific rods for thoracic kyphosis correction in adolescent idiopathic scoliosis surgery: Preliminary results. Orthop. Traumatol. Surg. Res. 2020, 106, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Prost, S.; Farah, K.; Pesenti, S.; Tropiano, P.; Fuentes, S.; Blondel, B. “Patient-specific” rods in the management of adult spinal deformity. One-year radiographic results of a prospective study about 86 patients. Neurochirurgie 2020, 66, 162–167. [Google Scholar] [CrossRef]
- Barton, C.; Noshchenko, A.; Patel, V.; Kleck, C.; Burger, E. Early Experience and Initial Outcomes with Patient-Specific Spine Rods for Adult Spinal Deformity. Orthopedics 2016, 39, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Qin, X.; He, Z.; Yin, R.; Qiu, Y.; Zhu, Z. Where to stop distally in Lenke modifier C AIS with lumbar curve more than 60°: L3 or L4? Clin. Neurol. Neurosurg. 2019, 178, 77–81. [Google Scholar] [CrossRef]
- LaValva, S.M.; Anari, J.B.; Flynn, J.M. Risk factors for persistent coronal imbalance or revision surgery following L3 LIV selection in adolescent idiopathic scoliosis (AIS). Spine Deform. 2021, 9, 1063–1072. [Google Scholar] [CrossRef]
- Chang, D.G.; Suk, S.I.; Song, K.S.; Kim, Y.H.; Oh, I.S.; Kim, S.I.; Park, H.Y.; Kim, G.U.; Lee, J.W.; Park, J.B.; et al. How to Avoid Distal Adding-on Phenomenon for Rigid Curves in Major Thoracolumbar and Lumbar Adolescent Idiopathic Scoliosis? Identifying the Incidence of Distal Adding-on by Selection of Lowest Instrumented Vertebra. World Neurosurg. 2019, 132, e472–e478. [Google Scholar] [CrossRef]
- Yamada, K.; Sudo, H.; Abe, Y.; Kokabu, T.; Tachi, H.; Endo, T.; Ohnishi, T.; Ukeba, D.; Ura, K.; Takahata, M.; et al. Influence of Lateral Translation of Lowest Instrumented Vertebra on L4 Tilt and Coronal Balance for Thoracolumbar and Lumbar Curves in Adolescent Idiopathic Scoliosis. J. Clin. Med. 2023, 12, 1389. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Radiographic Parameter | Pre-Operative | Postoperative | p Value |
|---|---|---|---|
| Thoracolumbar/lumbar curve (°) | 42.2 ± 6.6 | 5.9 ± 2.4 | <0.01 |
| Thoracic curve (°) | 22.0 ± 8.5 | 11.9 ± 8.0 | <0.01 |
| L4 tilt (°) | 20.7 ± 4.3 | 6.7 ± 3.2 | <0.01 |
| Thoracic kyphosis (T5-12) (°) | 24.9 ± 11.1 | 29.8 ± 8.0 | 0.02 |
| Lumbar lordosis (L1-S1) (°) | 46.4 ± 14.5 | 50.6 ± 12.2 | 0.04 |
| C7 translation from CSVL (mm) | 24.7 ± 14.6 | 16.9 ± 10.1 | 0.05 |
| Apical vertebral translation (mm) | 43.1 ± 9.3 | 8.9 ± 4.3 | <0.01 |
| Sagittal vertical axis (mm) | −0.4 ± 28.6 | 5.5 ± 25.2 | 0.34 |
| Vertebral rotation (°) | 20.3 ± 10.8 | 12.4 ± 5.0 | <0.01 |
| Proximal rod angle (°) | 18.3 ± 6.7 | 9.3 ± 3.3 | <0.01 |
| Distal rod angle (°) | 30.8 ± 8.0 | 15.9 ± 4.6 | <0.01 |
| Variable | Rod Deformation (ΔθP) | Rod Deformation (ΔθD) | ||
|---|---|---|---|---|
| Correlation Coefficient | Statistical Significance | Correlation Coefficient | Statistical Significance | |
| Postoperative main Cobb angle | r = 0.07 | p = 0.76 | r = 0.29 | p = 0.18 |
| Change in main Cobb angle | r = −0.20 | p = 0.37 | r = 0.01 | p = 0.96 |
| Postoperative L4 tilt | r = 0.03 | p = 0.88 | r = 0.25 | p = 0.25 |
| Change in L4 tilt | r = −0.10 | p = 0.65 | r = 0.11 | p = 0.61 |
| Postoperative lumbar lordosis | r = 0.21 | p = 0.35 | r = 0.01 | p = 0.95 |
| Change in lumbar lordosis | r = 0.30 | p = 0.17 | r = −0.36 | p = 0.10 |
| Postoperative thoracic kyphosis | r = 0.15 | p = 0.50 | r = 0.18 | p = 0.43 |
| Change in thoracic kyphosis | r = 0.22 | p = 0.32 | r = −0.23 | p = 0.31 |
| The Value between Each Point Cloud | The Value between Best-Fitted Curvature and the Other Point Clouds | |||
|---|---|---|---|---|
| Drms | Dmax | Drms | Dmax | |
| Cluster 1 | 0.72 | 0.99 | 0.21 | 0.46 |
| Cluster 2 | 3.98 | 8.35 | 1.18 | 4.32 |
| Cluster 3 | 4.52 | 8.78 | 1.91 | 4.67 |
| Cluster 4 | 1.35 | 2.19 | 0.57 | 1.16 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishikawa, Y.; Kanai, S.; Ura, K.; Kokabu, T.; Yamada, K.; Abe, Y.; Tachi, H.; Suzuki, H.; Ohnishi, T.; Endo, T.; et al. Development of Notch-Free, Pre-Bent Rod Applicable for Posterior Corrective Surgery of Thoracolumbar/Lumbar Adolescent Idiopathic Scoliosis. J. Clin. Med. 2023, 12, 5750. https://doi.org/10.3390/jcm12175750
Ishikawa Y, Kanai S, Ura K, Kokabu T, Yamada K, Abe Y, Tachi H, Suzuki H, Ohnishi T, Endo T, et al. Development of Notch-Free, Pre-Bent Rod Applicable for Posterior Corrective Surgery of Thoracolumbar/Lumbar Adolescent Idiopathic Scoliosis. Journal of Clinical Medicine. 2023; 12(17):5750. https://doi.org/10.3390/jcm12175750
Chicago/Turabian StyleIshikawa, Yoko, Satoshi Kanai, Katsuro Ura, Terufumi Kokabu, Katsuhisa Yamada, Yuichiro Abe, Hiroyuki Tachi, Hisataka Suzuki, Takashi Ohnishi, Tsutomu Endo, and et al. 2023. "Development of Notch-Free, Pre-Bent Rod Applicable for Posterior Corrective Surgery of Thoracolumbar/Lumbar Adolescent Idiopathic Scoliosis" Journal of Clinical Medicine 12, no. 17: 5750. https://doi.org/10.3390/jcm12175750