
Transvenous Lead Extraction during Cardiac Implantable Device Upgrade: Results from the Multicenter Swiss Lead Extraction Registry

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Patient Population
2.2. Study Objectives
2.3. Definitions
2.4. Statistical Analysis
3. Results
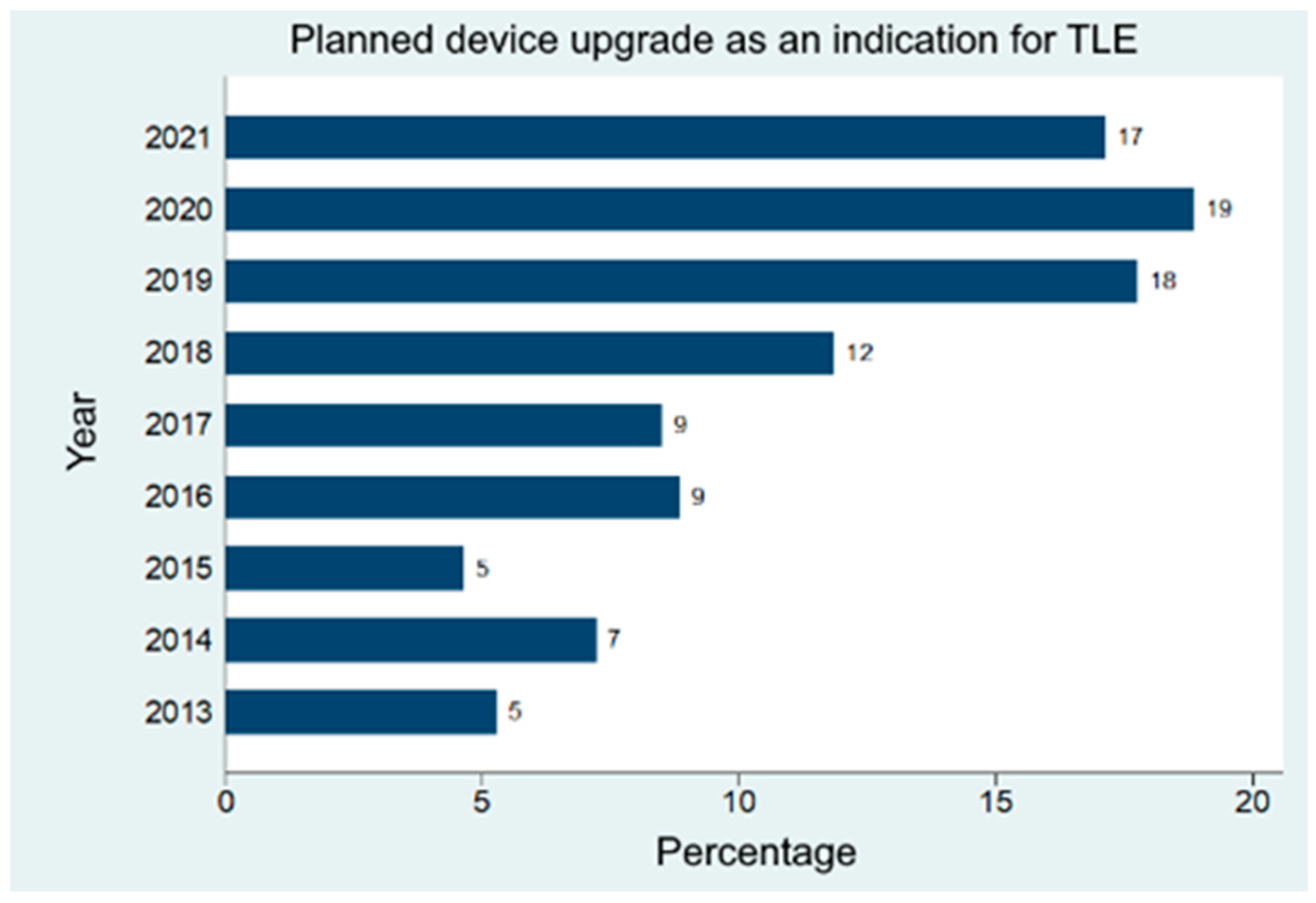
3.1. Patient Characteristics and the Increasing Importance of TLE during Upgrade
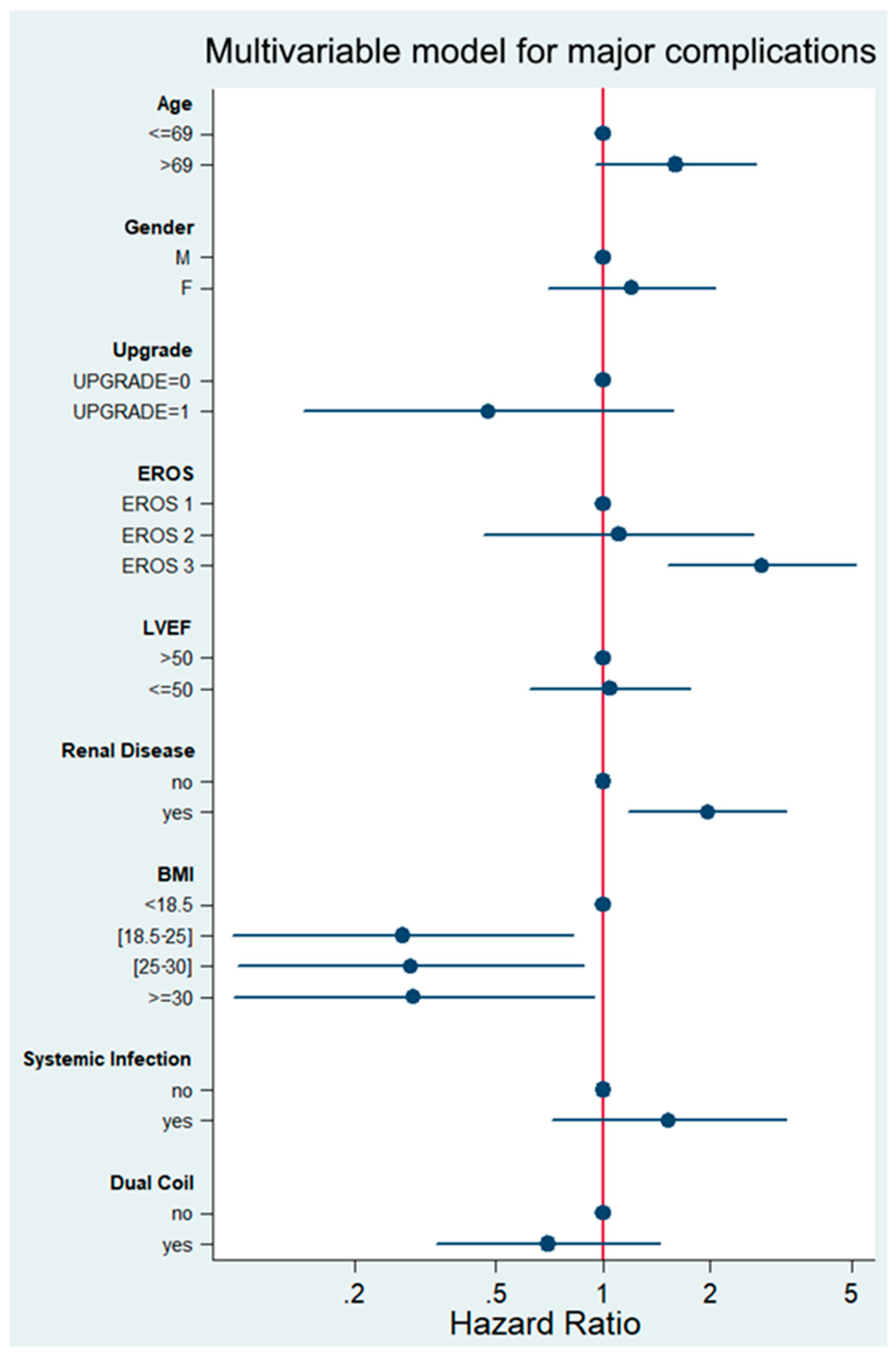
3.2. Risk Factors for TLE during Device Upgrade
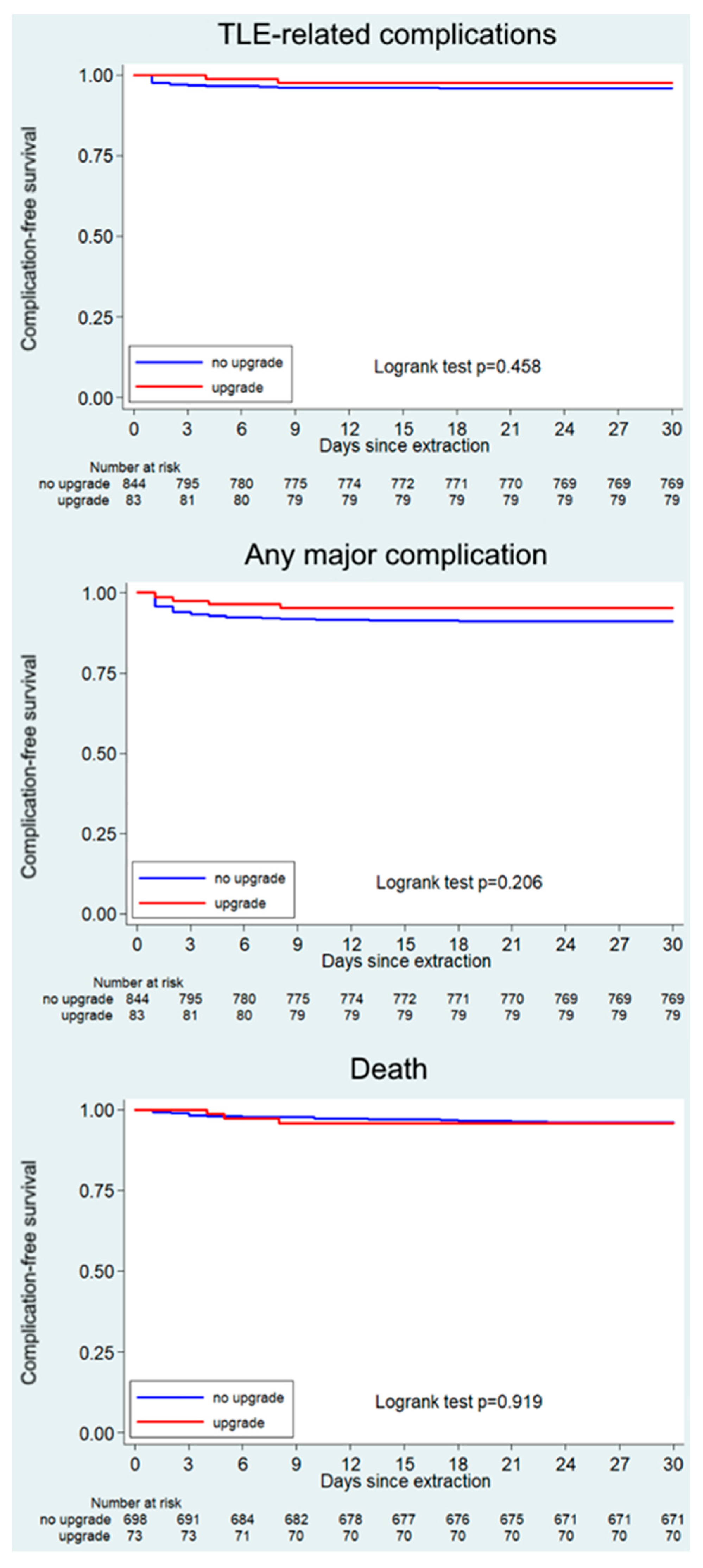
3.3. Comparative Outcomes of Upgraded Patients and Patients with Other Indications for TLE
4. Discussion
- The incidence of upgrade-associated TLE has increased by a factor of three in the last years compared to the number of such interventions almost ten years ago;
- TLE success rates during device upgrade interventions were >97% despite a considerable median lead dwell time of >6.5 years;
- In upgraded patients, the intraprocedural mortality rate was 2.4%, the rate of acute major complications was 7.2%, and an additional 1.2% of patients experienced complications during the first 30 days after TLE. Complication rates were not different than in other patients;
- TLE during device upgrade in patients with long-dwelling pacemakers (>15 years) or defibrillation (>10 years) leads is associated with a higher risk of major complications at 30 days [15].
4.1. Efficacy of TLE during Device Upgrade
4.2. Safety of TLE during Device Upgrade
4.3. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raatikainen, M.J.P.; Arnar, D.O.; Merkely, B.; Nielsen, J.C.; Hindricks, G.; Heidbuchel, H.; Camm, J. A Decade of Information on the Use of Cardiac Implantable Electronic Devices and Interventional Electrophysiological Procedures in the European Society of Cardiology Countries: 2017 Report from the European Heart Rhythm Association. Europace 2017, 19, ii1–ii90. [Google Scholar] [CrossRef] [PubMed]
- Perino, A.C.; Wang, P.J.; Lloyd, M.; Zanon, F.; Fujiu, K.; Osman, F.; Briongos-Figuero, S.; Sato, T.; Aksu, T.; Jastrzebski, M.; et al. Worldwide survey on implantation of and outcomes for conduction system pacing with His bundle and left bundle branch area pacing leads. J. Interv. Card. Electrophysiol. Int. J. Arrhythm. Pacing 2023, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Poole, J.E.; Gleva, M.J.; Mela, T.; Chung, M.K.; Uslan, D.Z.; Borge, R.; Gottipaty, V.; Shinn, T.; Dan, D.; Feldman, L.A.; et al. Complication rates associated with pacemaker or implantable cardioverter-defibrillator generator replacements and upgrade procedures: Results from the REPLACE registry. Circulation 2010, 122, 1553–1561. [Google Scholar] [CrossRef]
- Maytin, M.; Epstein, L.M. Lead Extraction Is Preferred for Lead Revisions and System Upgrades: When Less Is More. Circ. Arrhythmia Electrophysiol. 2010, 3, 413–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bongiorni, M.G.; Kennergren, C.; Butter, C.; Deharo, J.C.; Kutarski, A.; Rinaldi, C.A.; Romano, S.L.; Maggioni, A.P.; Andarala, M.; Auricchio, A.; et al. The European Lead Extraction ConTRolled (ELECTRa) study: A European Heart Rhythm Association (EHRA) Registry of Transvenous Lead Extraction Outcomes. Eur. Heart J. 2017, 38, 2995–3005. [Google Scholar] [CrossRef] [PubMed]
- Starck, C.T.; Gonzalez, E.; Al-Razzo, O.; Mazzone, P.; Delnoy, P.P.; Breitenstein, A.; Steffel, J.; Eulert-Grehn, J.; Lanmüller, P.; Melillo, F.; et al. Results of the Patient-Related Outcomes of Mechanical lead Extraction Techniques (PROMET) study: A multicentre retrospective study on advanced mechanical lead extraction techniques. Europace 2020, 22, 1103–1110. [Google Scholar] [CrossRef]
- Wazni, O.; Epstein, L.M.; Carrillo, R.G.; Love, C.; Adler, S.W.; Riggio, D.W.; Karim, S.S.; Bashir, J.; Greenspon, A.J.; DiMarco, J.P.; et al. Lead extraction in the contemporary setting: The LExICon study: An observational retrospective study of consecutive laser lead extractions. J. Am. Coll. Cardiol. 2010, 55, 579–586. [Google Scholar] [CrossRef] [Green Version]
- Kusumoto, F.M.; Schoenfeld, M.H.; Wilkoff, B.L.; Berul, C.I.; Birgersdotter-Green, U.M.; Carrillo, R.; Cha, Y.M.; Clancy, J.; Deharo, J.C.; Ellenbogen, K.A.; et al. 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm. 2017, 14, e503–e551. [Google Scholar] [CrossRef] [Green Version]
- Sohal, M.; Williams, S.; Akhtar, M.; Shah, A.; Chen, Z.; Wright, M.; O’Neill, M.; Patel, N.; Hamid, S.; Cooklin, M.; et al. Laser lead extraction to facilitate cardiac implantable electronic device upgrade and revision in the presence of central venous obstruction. Europace 2014, 16, 81–87. [Google Scholar] [CrossRef]
- Al-Maisary, S.; Romano, G.; Karck, M.; De Simone, R.; Kremer, J. The use of laser lead extraction sheath in the presence of supra-cardiac occlusion of the central veins for cardiac implantable electronic device lead upgrade or revision. PLoS ONE 2021, 16, e0251829. [Google Scholar] [CrossRef]
- Hussein, A.A.; Tarakji, K.G.; Martin, D.O.; Gadre, A.; Fraser, T.; Kim, A.; Brunner, M.P.; Barakat, A.F.; Saliba, W.I.; Kanj, M.; et al. Cardiac Implantable Electronic Device Infections: Added Complexity and Suboptimal Outcomes with Previously Abandoned Leads. JACC Clin. Electrophysiol. 2017, 3, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Barakat, A.F.; Wazni, O.M.; Tarakji, K.; Saliba, W.I.; Nimri, N.; Rickard, J.; Brunner, M.; Bhargava, M.; Kanj, M.; Baranowski, B.; et al. Transvenous lead extraction at the time of cardiac implantable electronic device upgrade: Complexity, safety, and outcomes. Heart Rhythm. 2017, 14, 1807–1811. [Google Scholar] [CrossRef] [PubMed]
- Stefańczyk, P.; Nowosielecka, D.; Polewczyk, A.; Jacheć, W.; Głowniak, A.; Kosior, J.; Kutarski, A. Efficacy and Safety of Transvenous Lead Extraction at the Time of Upgrade from Pacemakers to Cardioverter-Defibrillators and Cardiac Resynchronization Therapy. Int. J. Environ. Res. Public Health 2022, 20, 291. [Google Scholar] [CrossRef]
- Bongiorni, M.G.; Burri, H.; Deharo, J.C.; Starck, C.; Kennergren, C.; Saghy, L.; Rao, A.; Tascini, C.; Lever, N.; Kutarski, A.; et al. 2018 EHRA expert consensus statement on lead extraction: Recommendations on definitions, endpoints, research trial design, and data collection requirements for clinical scientific studies and registries: Endorsed by APHRS/HRS/LAHRS. Europace 2018, 20, 1217. [Google Scholar] [CrossRef]
- Sidhu, B.S.; Ayis, S.; Gould, J.; Elliott, M.K.; Mehta, V.; Kennergren, C.; Butter, C.; Deharo, J.C.; Kutarski, A.; Maggioni, A.P.; et al. Risk stratification of patients undergoing transvenous lead extraction with the ELECTRa Registry Outcome Score (EROS): An ESC EHRA EORP European lead extraction ConTRolled ELECTRa registry analysis. Europace 2021, 23, 1462–1471. [Google Scholar] [CrossRef] [PubMed]
- McCanta, A.C.; Tanel, R.E.; Gralla, J.; Runciman, D.M.; Collins, K.K. The Fate of Nontargeted Endocardial Leads during the Extraction of One or More Targeted Leads in Pediatrics and Congenital Heart Disease. Pacing Clin. Electrophysiol. 2014, 37, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Di Monaco, A.; Pelargonio, G.; Narducci, M.L.; Manzoli, L.; Boccia, S.; Flacco, M.E.; Capasso, L.; Barone, L.; Perna, F.; Bencardino, G.; et al. Safety of transvenous lead extraction according to centre volume: A systematic review and meta-analysis. EP Eur. 2014, 16, 1496–1507. [Google Scholar] [CrossRef] [PubMed]
- Pecha, S.; Burger, H.; Chung, D.U.; Moller, V.; Madej, T.; Maali, A.; Osswald, B.; De Simone, R.; Monsefi, N.; Ziaukas, V.; et al. The GermAn Laser Lead Extraction RegistrY: GALLERY. Europace 2022, 24, 1627–1635. [Google Scholar] [CrossRef]
- Deshmukh, A.; Patel, N.; Noseworthy, P.A.; Patel, A.A.; Patel, N.; Arora, S.; Kapa, S.; Noheria, A.; Mulpuru, S.; Badheka, A.; et al. Trends in Use and Adverse Outcomes Associated with Transvenous Lead Removal in the United States. Circulation 2015, 132, 2363–2371. [Google Scholar] [CrossRef]
- Byrd, C.L.; Wilkoff, B.L.; Love, C.J.; Sellers, T.D.; Turk, K.T.; Reeves, R.; Young, R.; Crevey, B.; Kutalek, S.P.; Freedman, R.; et al. Intravascular extraction of problematic or infected permanent pacemaker leads: 1994–1996. U.S. Extraction Database, MED Institute. Pacing Clin. Electrophysiol. 1999, 22, 1348–1357. [Google Scholar] [CrossRef]
- Ghosh, N.; Yee, R.; Klein, G.J.; Quantz, M.; Novick, R.J.; Skanes, A.C.; Krahn, A.D. Laser lead extraction: Is there a learning curve? Pacing Clin. Electrophysiol. 2005, 28, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Haeberlin, A.; Holz, A.; Seiler, J.; Baldinger, S.; Tanner, H.; Roten, L.; Madaffari, A.; Servatius, H.; Jenni, H.; Kadner, A.; et al. Impact of a structured institutional lead management programme at a high volume centre for transvenous lead extractions in Switzerland. Cardiovasc. Med. 2023, 26, 28–33. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Upgrade Indication (n = 83) | Other Indications (n = 858) | Missing Data (%) | p-Value |
|---|---|---|---|---|
| Age | 65.5 (14.1) | 65.7 (15.9) | 1.3% | 0.668 |
| Male gender | 68 (81.9%) | 601 (70.0) | 1.3% | 0.031 |
| Body mass index [kg/m2] | 27.4 (5.4) | 26.6 (5.1) | 6.1% | 0.363 |
| Hypertension | 44 (53.0%) | 444 (51.7%) | 2.9% | 1.000 |
| Diabetes mellitus | 14 (16.9%) | 177 (20.6%) | 3.2% | 0.475 |
| Dyslipidemia | 38 (45.8%) | 389 (45.3%) | 3.2% | 1.000 |
| Chronic kidney disease | 18 (21.7%) | 216 (25.2%) | 5.4% | 0.429 |
| Chronic obstructive pulmonary disease | 7 (8.4%) | 73 (8.5%) | 6.2% | 0.834 |
| Known heart disease | 6.3% | 0.038 | ||
| Coronary artery disease (CAD) | 28 (33.7%) | 262 (29.4%) | ||
| Hypertrophic cardiomyopathy | 2 (2.4%) | 29 (3.4%) | ||
| Arrhythmogenic dysplasia | 1 (1.2%) | 13 (1.5%) | ||
| Channelopathy | 0 (0.0%) | 11 (1.3%) | ||
| None | 9 (10.8%) | 163 (19.0%) | ||
| Other heart disease | 43 (51.8%) | 380 (44.3%) | ||
| Left ventricular ejection fraction (%) | 36.4 (11.9) | 47.2 (15.0) | 6.5% | <0.001 |
| Medication | ||||
| Anticoagulation | 50 (60.2%) | 403 (47.0%) | 3.1% | 0.050 |
| Anti-platelet therapy | 29 (34.9%) | 288 (33.6%) | 3.1% | 1.000 |
| Digoxin | 2 (2.5%) | 23 (2.7%) | 4.6% | 1.000 |
| Diuretics | 55 (66.3%) | 431 (50.2%) | 3.9% | 0.020 |
| ACEI/ARB/ARNI | 60 (72.3%) | 492 (57.3%) | 4.1% | 0.023 |
| Beta-blocker | 62 (74.7%) | 526 (61.3%) | 3.5% | 0.053 |
| Calcium-antagonist | 12 (14.5%) | 89 (10.4%) | 4.4% | 0.357 |
| Anti-arrhythmic drugs | 9 (10.8%) | 127 (14.8%) | 3.9% | 0.333 |
| Anti-aldosteronic agent | 26 (31.3%) | 185 (21.6%) | 3.9% | 0.077 |
| Statin | 38 (45.8%) | 388 (45.2%) | 3.9% | 0.818 |
| Implanted device history | 1.5% | <0.001 | ||
| Single/dual chamber pacemaker | 62 (74.7%) | 389 (45.3%) | ||
| Single/dual chamber ICD | 12 (14.5%) | 257 (30.0%) | ||
| CRT-P | 7 (8.4%) | 28 (3.3%) | ||
| CRT-D | 2 (2.4%) | 170 (19.8%) | ||
| Indication for extraction | 1.3% | <0.001 | ||
| Device upgrade | 83 (100.0%) | 0 (0.0%) | ||
| Lead malfunction | 0 (0.0%) | 426 (49.7%) | ||
| Infection | 0 (0.0%) | 337 (39.3%) | ||
| Venous stenosis or occlusion | 0 (0.0%) | 11 (1.3%) | ||
| Chronic pain | 0 (0.0%) | 10 (1.2%) | ||
| Recalled lead | 0 (0.0%) | 7 (0.8%) | ||
| Other | 0 (0.0%) | 67 (7.8%) |
| Variable | Upgrade Indication (n = 83) | Other Indications (n = 858) | Missing Data (%) | p-Value |
|---|---|---|---|---|
| TLE approach | 2.4% | 0.110 | ||
| Superior left | 56 (67.5%) | 612 (71.3%) | ||
| Superior right | 18 (21.7%) | 180 (21.0%) | ||
| Superior left and right | 6 (7.2%) | 32 (3.7%) | ||
| Superior left and femoral/jugular | 0 (0.0%) | 4 (0.5%) | ||
| Superior right and femoral/jugular | 3 (3.6%) | 6 (0.7%) | ||
| Femoral only | 0 (0.0%) | 1 (0.1%) | ||
| Lead targeted for TLE | - | |||
| Pacing and sensing lead | 132 (89.2%) | 1020 (66.8%) | <0.001 | |
| ICD single coil | 7 (4.7%) | 254 (16.6%) | 0.047 | |
| ICD dual coil | 6 (4.1%) | 158 (10.4%) | 0.013 | |
| CS bipolar | 2 (1.4%) | 43 (2.8%) | 0.425 | |
| CS multipolar | 1 (0.7%) | 39 (2.6%) | 0.248 | |
| Number of targeted leads per patient | 1.7 [1–2] | 1.8 [1–2] | 1.000 | |
| Median lead dwelling time | 6.6 [3.1–11.9] | 6.2 [3.0–9.8] | 0.072 | |
| TLE technique | 3.9% | |||
| Rotational mechanical | 49 (59.0%) | 366 (42.7%) | 0.015 | |
| Laser sheath | 11 (13.3%) | 214 (24.9%) | 0.011 | |
| Mechanical non-powered | 12 (14.5%) | 135 (15.7%) | 0.755 | |
| Stylet only (manual traction) | 8 (9.6%) | 68 (7.9%) | 0.677 | |
| Surgical | 0 (0.0%) | 1 (0.1%) | 1.000 | |
| Other tools | 3 (3.6%) | 37 (4.3%) | 1.000 | |
| Procedural data | ||||
| Total extraction time [min] | 18 [15–25] | 15 [10–25] | 39.3% | 0.674 |
| Total procedure time [min] | 160 [100–195] | 105 [65–150] | 16.3% | <0.001 |
| Total fluoroscopic time [min] | 20.5 [7.9–34.0] | 10.6 [5.0–24.0] | 49.9% | 0.030 |
| Radiological and clinical success | ||||
| Radiological success | 2.9% | 0.351 | ||
| Complete | 77 (92.8%) | 756 (88.1%) | ||
| Failure | 0 (0.0%) | 24 (2.8%) | ||
| Partial | 5 (6.0%) | 52 (6.1%) | ||
| Clinical success | 81 (97.6%) | 798 (93.0%) | 0.569 |
| Variable | Upgrade Indication (n = 83) | Other Indications (n = 858) | Missing Data (%) | p-Value |
|---|---|---|---|---|
| Acute major complications | 6 (7.2%) | 47 (5.5%) | - | 0.457 |
| Cardiac avulsion or tear | 0 (0.0%) | 4 (0.5%) | ||
| Vascular avulsion or tear | 0 (0.0%) | 6 (0.7%) | ||
| Major thromboembolic event | 0 (0.0%) | 3 (0.3%) | ||
| Pneumothorax | 0 (0.0%) | 2 (0.2%) | ||
| Stroke/TIA | 1 (1.2%) | 0 (0.0%) | ||
| Complication associated with re-implant | 4 (4.8%) | 21 (2.4%) | ||
| Other | 1 (1.2%) | 11 (1.3%) | ||
| Intraprocedural TLE-related death | 2 (2.4%) | 11 (1.3%) | - | 0.321 |
| Postprocedural complications | 1 (1.2%) | 33 (3.8%) | 1.4% | 0.354 |
| Death (not procedure-related) | 1 (1.2%) | 6 (0.7%) | ||
| Heart failure | 0 (0.0%) | 4 (0.5%) | ||
| Pocket hematoma | 0 (0.0%) | 6 (0.7%) | ||
| Progressive renal failure | 0 (0.0%) | 3 (0.3%) | ||
| Pneumonia | 0 (0.0%) | 1 (0.1%) | ||
| Recurrence of infection/sepsis | 0 (0.0%) | 4 (0.5%) | ||
| Other | 0 (0.0%) | 9 (1.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haeberlin, A.; Noti, F.; Breitenstein, A.; Auricchio, A.; Reichlin, T.; Conte, G.; Klersy, C.; Curti, M.; Pruvot, E.; Domenichini, G.; et al. Transvenous Lead Extraction during Cardiac Implantable Device Upgrade: Results from the Multicenter Swiss Lead Extraction Registry. J. Clin. Med. 2023, 12, 5175. https://doi.org/10.3390/jcm12165175
Haeberlin A, Noti F, Breitenstein A, Auricchio A, Reichlin T, Conte G, Klersy C, Curti M, Pruvot E, Domenichini G, et al. Transvenous Lead Extraction during Cardiac Implantable Device Upgrade: Results from the Multicenter Swiss Lead Extraction Registry. Journal of Clinical Medicine. 2023; 12(16):5175. https://doi.org/10.3390/jcm12165175
Chicago/Turabian StyleHaeberlin, Andreas, Fabian Noti, Alexander Breitenstein, Angelo Auricchio, Tobias Reichlin, Giulio Conte, Catherine Klersy, Moreno Curti, Etienne Pruvot, Giulia Domenichini, and et al. 2023. "Transvenous Lead Extraction during Cardiac Implantable Device Upgrade: Results from the Multicenter Swiss Lead Extraction Registry" Journal of Clinical Medicine 12, no. 16: 5175. https://doi.org/10.3390/jcm12165175