


Feasibility and Acceptance of Self-Guided Mobile Ultrasound among Pregnant Women in Routine Prenatal Care
 , , , , and
, , , , and
Abstract
:1. Introduction
Purpose
2. Methods
2.1. Study Design and Population
2.2. Study Procedures and Data Collection
- Recording a video of the fetal heartbeat for 30 s;
- Taking a picture and recording a video of the fetal profile for 60 s;
- Taking a picture and recording a 15-s video of the amniotic fluid in each of the four quadrants of the abdomen.
2.3. Ultrasound Devices and Settings
2.4. Evaluation of Image and Video Quality
- Images or videos that showed the required target structure (e.g., heartbeat, fetal profile or amniotic fluid) were marked as “target located.”
- Images or videos in which the required target structure was not shown were marked as “target structure not located.”
- Images or videos that showed the required target structure, but with poor quality that was not suitable for medical assessment, were marked as “target structure located, but quality low” (e.g., the image quality was blurred, or the target structure was not completely visible).
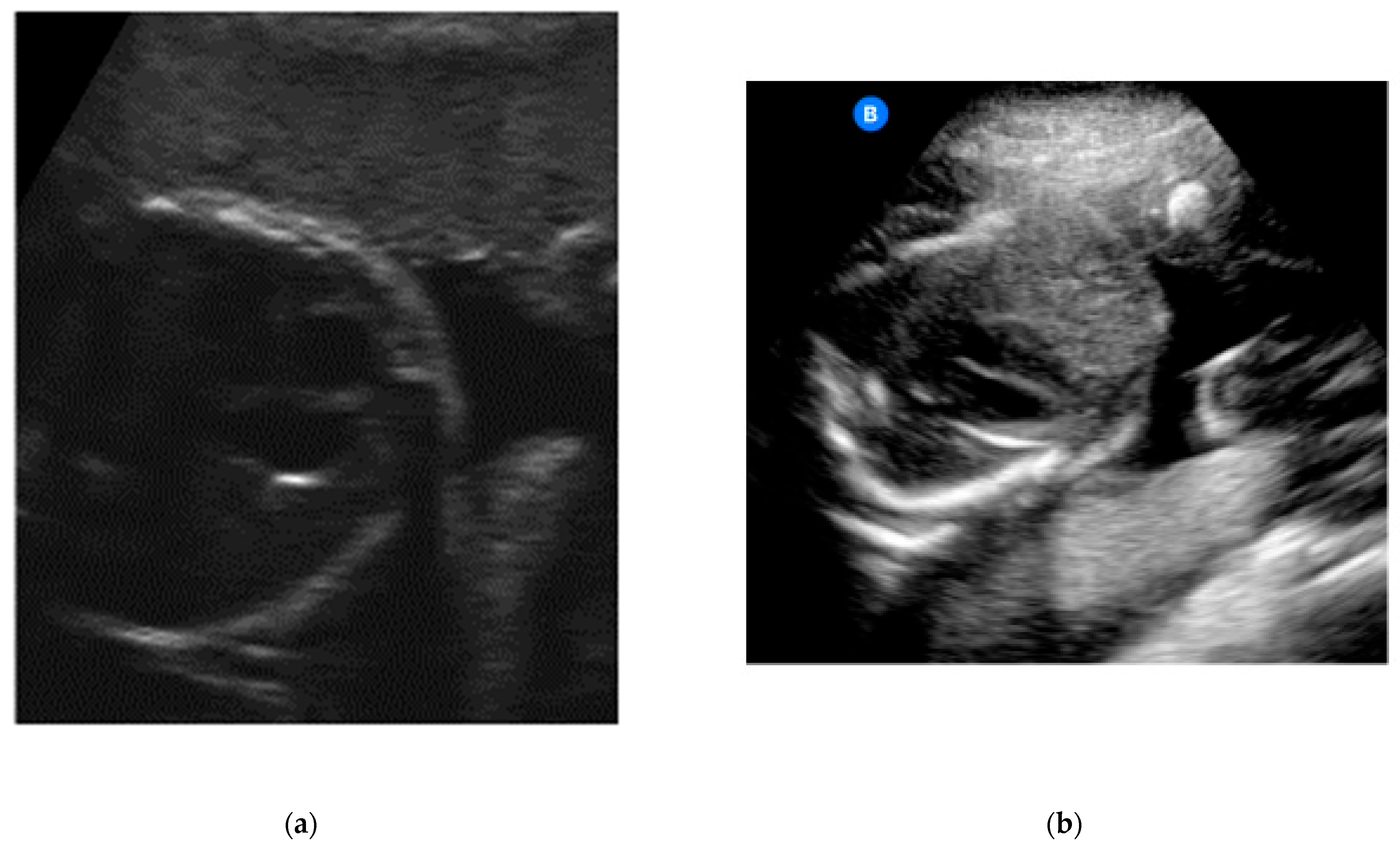
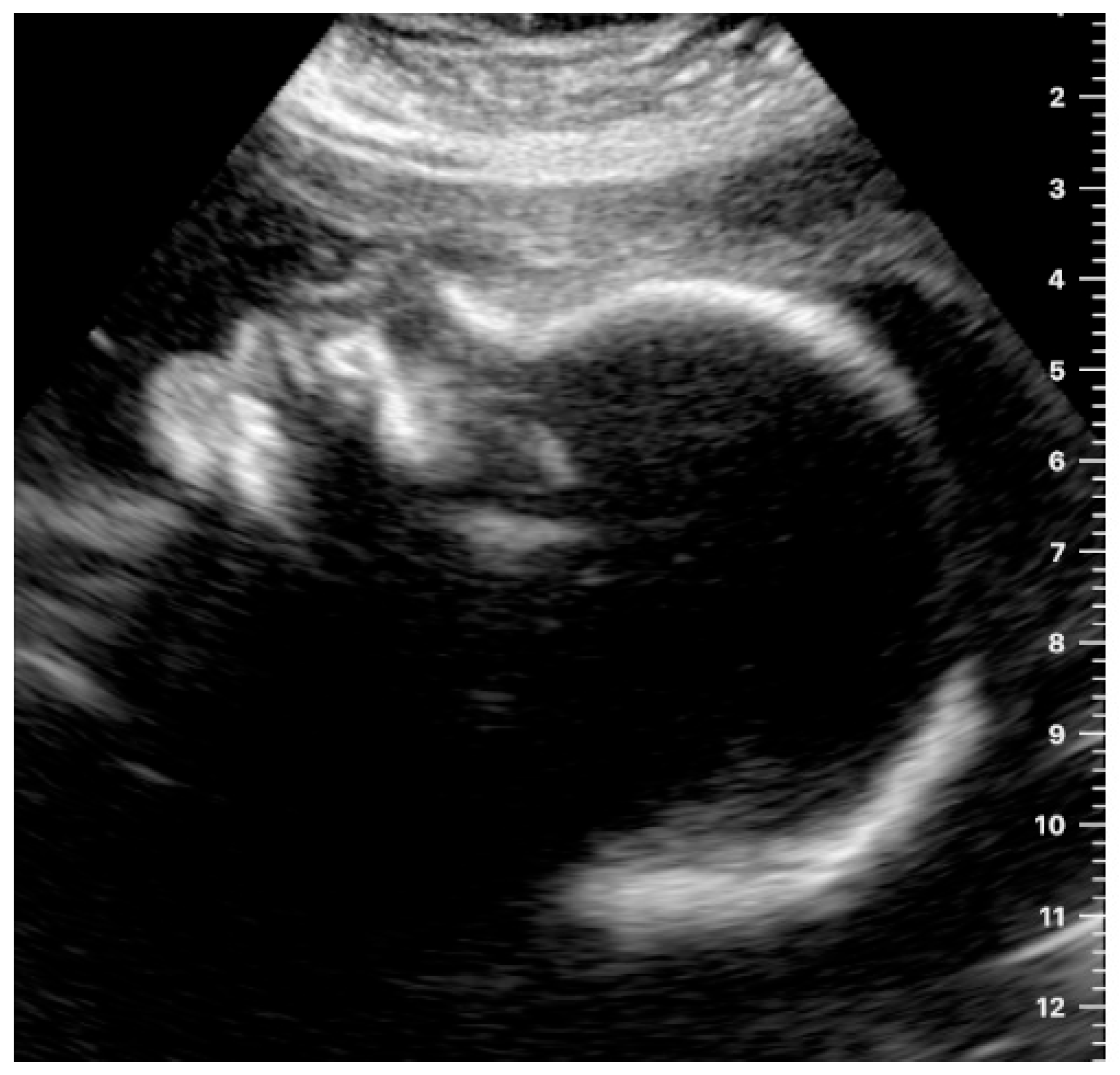
- If the participant was able to show the fetal heartbeat for at least one second during the video sequence lasting 30 s, it was marked as “target located.” For a satisfactory presentation of the fetal profile, the forehead, tip of the nose and chin had to be clearly visible (example in Figure 1). Images and videos taken by the participants in which the fetal profile was also not visible (n = 18) were excluded.
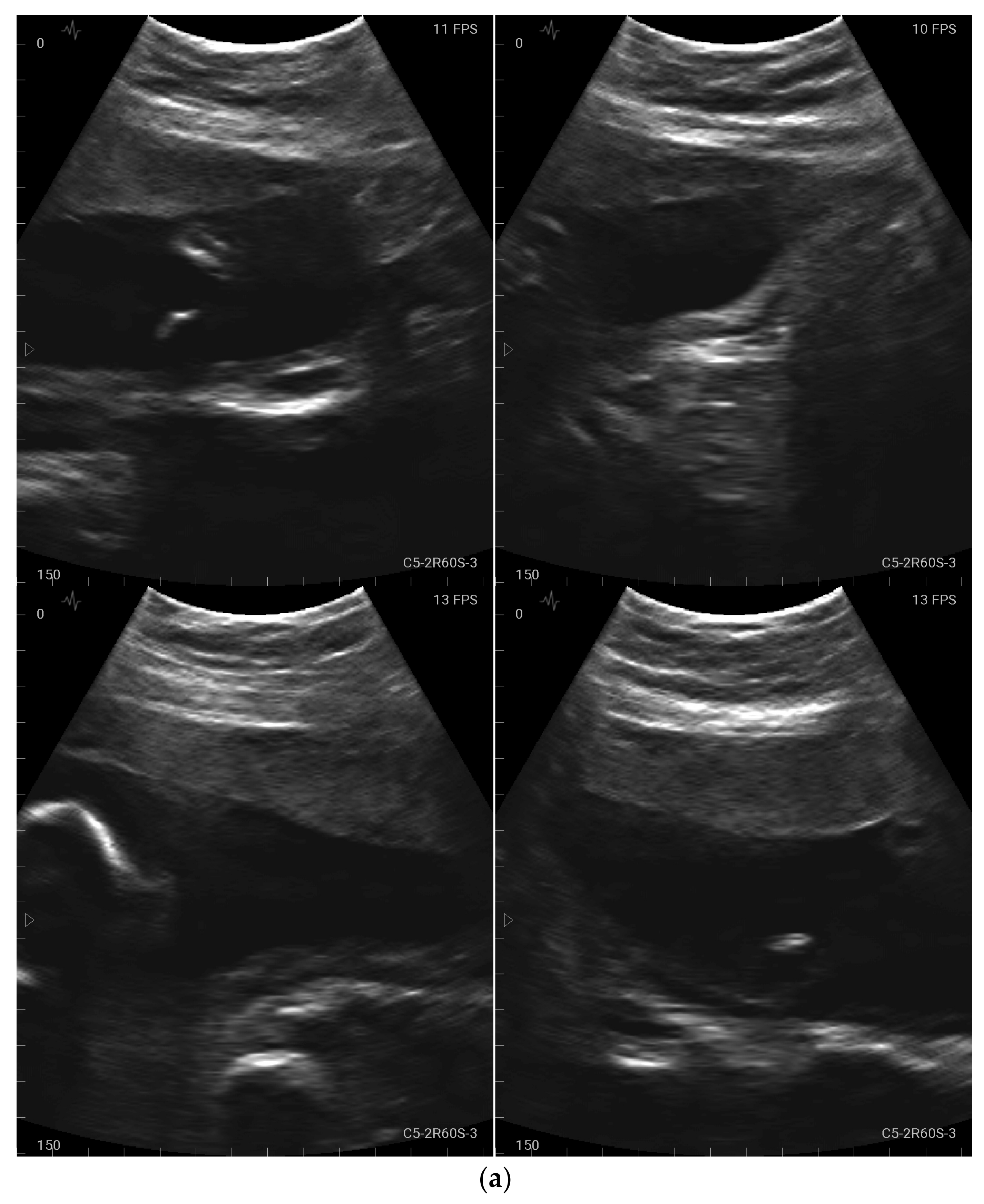
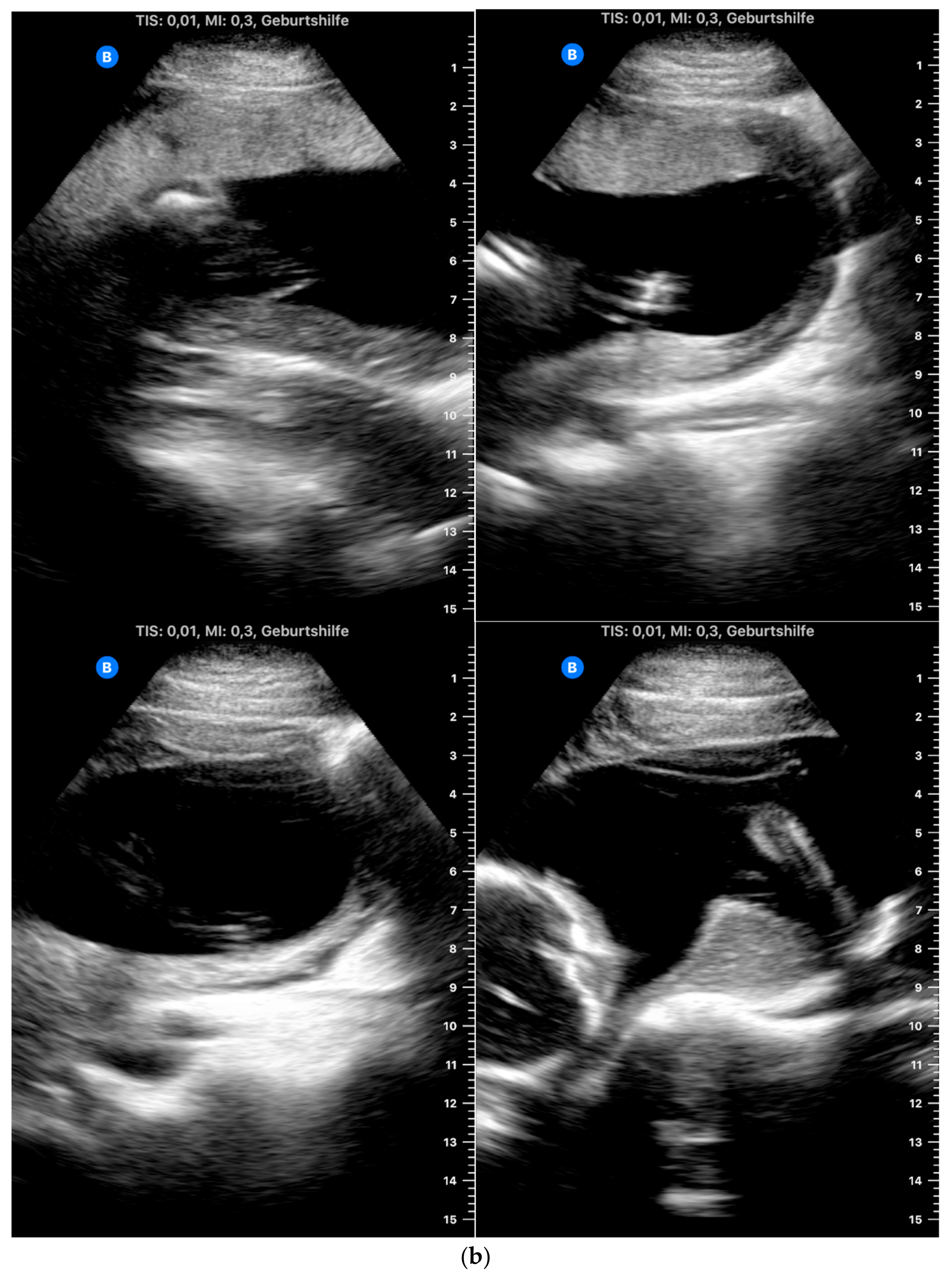
- For a satisfactory presentation of images and videos of the amniotic fluid, hypoechoic areas had to be clearly demarcated from parts of the fetus. The four images and four video sequences representing the amniotic fluid were evaluated separately. If the amniotic fluid was clearly displayed in one quadrant, the respective videos or image sequences were marked as “target located.” It was also examined whether the women were able to display the amniotic fluid in all four quadrants so that retrospective evaluation of a normal amount of amniotic fluid in a participant would be possible. Accordingly, the videos were marked as “4 out of 4 with sufficient quality” only if the amniotic fluid was visible in all four video sequences.
2.5. Data Analysis
3. Results
3.1. General Maternal Characteristics
3.2. Evaluation of the Questionnaire on Feasibility and Acceptance
3.3. Assessment of Image and Video Quality
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Salomon, L.; Alfirevic, Z.; Da Silva Costa, F.; Deter, R.; Figueras, F.; Ghi, T.; Glanc, P.; Khalil, A.; Lee, W.; Napolitano, R.; et al. ISUOG Practice Guidelines: Ultrasound assessment of fetal biometry and growth. Ultrasound Obstet. Gynecol. 2019, 53, 715–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tolsgaard, M.G. Assessment and learning of ultrasound skills in Obstetrics & Gynecology. Dan. Med. J. 2018, 65, B5445. [Google Scholar]
- Gyselaers, W.; Lanssens, D.; Perry, H.; Khalil, A. Mobile Health Applications for Prenatal Assessment and Monitoring. Curr. Pharm. Des. 2019, 25, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Weichert, J.; Welp, A.; Scharf, J.L.; Dracopoulos, C.; Becker, W.H.; Gembicki, M. The Use of Artificial Intelligence in Automation in the Fields of Gynaecology and Obstetrics—An Assessment of the State of Play. Geburtshilfe Frauenheilkd. 2021, 81, 1203–1216. [Google Scholar] [CrossRef] [PubMed]
- Peahl, A.F.; Smith, R.D.; Moniz, M.H. Prenatal care redesign: Creating flexible maternity care models through virtual care. Am. J. Obstet. Gynecol. 2020, 223, 389.e1–389.e10. [Google Scholar] [CrossRef] [PubMed]
- Stumpfe, F.M.; Titzmann, A.; Schneider, M.O.; Stelzl, P.; Kehl, S.; Fasching, P.A.; Beckmann, M.W.; Ensser, A. SARS-CoV-2 Infection in Pregnancy—A Review of the Current Literature and Possible Impact on Maternal and Neonatal Outcome. Geburtshilfe Frauenheilkd. 2020, 80, 380–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorup, T.J.; Zingenberg, H. Use of ‘non-medical’ ultrasound imaging before mid-pregnancy in Copenhagen. Acta Obstet. Gynecol. Scand. 2015, 94, 102–105. [Google Scholar] [CrossRef]
- Grym, K.; Niela-Vilen, H.; Ekholm, E.; Hamari, L.; Azimi, I.; Rahmani, A.; Liljeberg, P.; Löyttyniemi, E.; Axelin, A. Feasibility of smart wristbands for continuous monitoring during pregnancy and one month after birth. BMC Pregnancy Childbirth 2019, 19, 34. [Google Scholar] [CrossRef]
- Kalafat, E.; Mir, I.; Perry, H.; Thilaganathan, B.; Khalil, A. Is home blood-pressure monitoring in hypertensive disorders of pregnancy consistent with clinic recordings? Ultrasound Obstet. Gynecol. 2018, 52, 515–521. [Google Scholar] [CrossRef] [Green Version]
- Aust, T.; Famoriyo, A. Caution with home fetal Doppler devices. BMJ 2009, 339, b3220. [Google Scholar] [CrossRef]
- Schramm, K.; Grassl, N.; Nees, J.; Hoffmann, J.; Stepan, H.; Bruckner, T.; Haun, M.W.; Maatouk, I.; Haist, M.; Schott, T.C.; et al. Women’s Attitudes Toward Self-Monitoring of Their Pregnancy Using Noninvasive Electronic Devices: Cross-Sectional Multicenter Study. JMIR Mhealth Uhealth 2019, 7, e11458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tolsgaard, M.G.; Rasmussen, M.B.; Tappert, C.; Sundler, M.; Sorensen, J.L.; Ottesen, B.; Ringsted, C.; Tabor, A. Which factors are associated with trainees’ confidence in performing obstetric and gynecological ultrasound examinations? Ultrasound Obstet. Gynecol. 2014, 43, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Wah, Y.M.; Chan, L.W.; Leung, T.Y.; Fung, T.Y.; Lau, T.K. How true is a ‘true’ midsagittal section? Ultrasound Obstet. Gynecol. 2008, 32, 855–859. [Google Scholar] [CrossRef] [PubMed]
- Silvestri, M.T.; Pettker, C.M.; Raney, J.H.; Xu, X.; Ross, J.S. Frequency and Importance of Incomplete Screening Fetal Anatomic Sonography in Pregnancy. J. Ultrasound Med. 2016, 35, 2665–2673. [Google Scholar] [CrossRef]
- Chaichanalap, R.; Hanprasertpong, T. Success rate to complete optimal 20 + 2 ISUOG planes for foetal ultrasonographic structural screening during early second trimester pregnancy in Thailand. Ultrasound J. 2021, 13, 36. [Google Scholar] [CrossRef]
- Hadar, E.; Wolff, L.; Tenenbaum-Gavish, K.; Eisner, M.; Shmueli, A.; Barbash-Hazan, S.; Bergel, R.; Shmuel, E.; Houri, O.; Dollinger, S.; et al. Mobile Self-Operated Home Ultrasound System for Remote Fetal Assessment During Pregnancy. Telemed. J. E. Health 2021, 28, 93–101. [Google Scholar] [CrossRef]
- Dalewyn, L.; Deschepper, E.; Gerris, J. Correlation between follicle dimensions recorded by patients at home (SOET) versus ultrasound performed by professional care providers. Facts Views Vis. Obgyn. 2017, 9, 153–156. [Google Scholar]
- Cuneo, B.F.; Sonesson, S.E.; Levasseur, S.; Moon-Grady, A.J.; Krishnan, A.; Donofrio, M.T.; Raboisson, M.-J.; Hornberger, L.K.; Van Eerden, P.; Sinkovskaya, E.; et al. Home Monitoring for Fetal Heart Rhythm During Anti-Ro Pregnancies. J. Am. Coll. Cardiol. 2019, 73, 1940–1951. [Google Scholar] [CrossRef]
- Kuleva, M.; Salomon, L.J.; Benoist, G.; Ville, Y.; Dumez, Y. The value of daily fetal heart rate home monitoring in addition to serial ultrasound examinations in pregnancies complicated by fetal gastroschisis. Prenat. Diagn. 2012, 32, 789–796. [Google Scholar] [CrossRef]
- Wainstock, T.; Anteby, E.; Glasser, S.; Shoham-Vardi, I.; Lerner-Geva, L. The association between prenatal maternal objective stress, perceived stress, preterm birth and low birthweight. J. Matern.-Fetal Neonatal. Med. 2013, 26, 973–977. [Google Scholar] [CrossRef]
- Coelho, H.F.; Murray, L.; Royal-Lawson, M.; Cooper, P.J. Antenatal anxiety disorder as a predictor of postnatal depression: A longitudinal study. J. Affect. Disord. 2011, 129, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Austin, M.P.; Tully, L.; Parker, G. Examining the relationship between antenatal anxiety and postnatal depression. J. Affect. Disord. 2007, 101, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Sullivan, E.A.; Forero, R.; Homer, C.S. The association of Emergency Department presentations in pregnancy with hospital admissions for postnatal depression (PND): A cohort study based on linked population data. BMC Emerg. Med. 2017, 17, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kollmann, C.; Jenderka, K.V.; Moran, C.M.; Draghi, F.; Jimenez Diaz, J.F.; Sande, R. EFSUMB Clinical Safety Statement for Diagnostic Ultrasound—(2019 revision). Ultraschall. Med. 2020, 41, 387–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Cohort A and B (n = 46) | Cohort A (n = 23) | Cohort B (n = 23) | |||
|---|---|---|---|---|---|---|
| Mean or n 1 | SD or % 1 | Mean or n 1 | SD or % 1 | Mean or n 1 | SD or % 1 | |
| Maternal age | 32.6 | 5.2 | 33.8 | 5.0 | 31.4 | 5.1 |
| Gestational week | 24.0 | 3.2 | 24.1 | 3.3 | 23.9 | 3.0 |
| Pregnancy | ||||||
| 1 | 18 | 39.1 | 8 | 34.8 | 10 | 43.5 |
| 2 | 16 | 34.8 | 8 | 34.8 | 8 | 34.8 |
| ≥3 | 12 | 26.1 | 7 | 30.4 | 5 | 21.7 |
| Educational level | ||||||
| No school-leaving qualification | 0 | 0 | 0 | 0 | 0 | 0 |
| Lower secondary school qualification | 1 | 2.2 | 0 | 0 | 1 | 4.3 |
| Intermediate school qualification | 6 | 13.0 | 3 | 13.0 | 3 | 13.0 |
| University entrance qualification | 4 | 8.7 | 3 | 13.0 | 1 | 4.3 |
| Apprenticeship qualification | 12 | 26.1 | 5 | 21.7 | 7 | 30.4 |
| Bachelor’s/master’s degree | 19 | 41.3 | 10 | 43.5 | 9 | 39.1 |
| Doctoral degree | 4 | 8.7 | 2 | 8.7 | 2 | 8.7 |
| Smartphone ownership | ||||||
| No smartphone | 0 | 0 | 0 | 0 | 0 | 0 |
| iOS | 20 | 43.5 | 8 | 34.8 | 12 | 52.2 |
| Android | 23 | 50.0 | 14 | 60.9 | 9 | 39.1 |
| iOS and Android | 2 | 4.3 | 1 | 4.3 | 1 | 4.3 |
| Unknown | 1 | 2.2 | 0 | 0 | 1 | 4.3 |
| Questions | Cohort A and B (n = 46) | Cohort A (n = 23) | Cohort B (n = 23) | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| How confident did you feel using the ultrasound probe? | ||||||
| Very confident | 2 | 4.3 | 2 | 8.7 | 0 | 0 |
| Confident | 17 | 37.0 | 7 | 30.4 | 10 | 43.5 |
| Partly/partially | 20 | 43.5 | 8 | 34.8 | 12 | 52.2 |
| Unsure | 7 | 15.2 | 6 | 26.1 | 1 | 4.3 |
| Very unsure | 0 | 0 | 0 | 0 | 0 | 0 |
| Could you imagine doing this examination at home by yourself? | ||||||
| Yes | 31 | 67.4 | 14 | 60.9 | 17 | 73.9 |
| No | 10 | 21.7 | 5 | 21.7 | 5 | 21.7 |
| I do not know | 5 | 10.9 | 4 | 17.4 | 1 | 4.3 |
| If you were to perform this examination at home, would you like the attending physician to provide live support via video telephony? | ||||||
| Yes | 40 | 87.0 | 20 | 87.0 | 20 | 87.0 |
| No | 2 | 4.3 | 1 | 4.3 | 1 | 4.3 |
| I do not know | 4 | 8.7 | 2 | 8.7 | 2 | 8.7 |
| If you were doing this examination at home, would it be okay for you if the doctor first had to evaluate and approve the ultrasound image before you could see it? | ||||||
| Yes | 21 | 45.7 | 9 | 39.1 | 12 | 52.2 |
| No | 16 | 34.8 | 9 | 39.1 | 7 | 30.4 |
| I do not know | 9 | 19.6 | 5 | 21.7 | 4 | 17.4 |
| Do you agree with the following statements? | ||||||
| The self-examination was fun | ||||||
| I completely agree | 31 | 67.4 | 14 | 60.9 | 17 | 73.9 |
| Agree | 12 | 26.1 | 7 | 30.4 | 5 | 21.7 |
| Neither agree nor disagree | 3 | 6.5 | 2 | 8.7 | 1 | 4.3 |
| A little | 0 | 0 | 0 | 0 | 0 | 0 |
| Not at all | 0 | 0 | 0 | 0 | 0 | 0 |
| I would like to do the self-examination more often | ||||||
| I completely agree | 18 | 39.1 | 8 | 34.8 | 10 | 43.5 |
| Agree | 15 | 32.6 | 8 | 34.8 | 7 | 30.4 |
| Neither agree nor disagree | 5 | 10.9 | 3 | 13.0 | 2 | 8.7 |
| A little | 8 | 17.4 | 4 | 17.4 | 4 | 17.4 |
| Not at all | 0 | 0 | 0 | 0 | 0 | 0 |
| The self-examination took too much time | ||||||
| I completely agree | 1 | 2.2 | 0 | 0 | 1 | 4.3 |
| Agree | 2 | 4.3 | 1 | 4.3 | 1 | 4.3 |
| Neither agree nor disagree | 1 | 2.2 | 0 | 0 | 1 | 4.3 |
| A little | 15 | 32.6 | 10 | 43.5 | 5 | 21.7 |
| Not at all | 27 | 58.7 | 12 | 52.2 | 15 | 65.2 |
| I was afraid of doing something wrong during the self-examination | ||||||
| I completely agree | 1 | 2.2 | 1 | 4.3 | 0 | 0 |
| Agree | 3 | 6.5 | 2 | 8.7 | 1 | 4.3 |
| Neither agree nor disagree | 10 | 21.7 | 4 | 17.4 | 6 | 26.1 |
| A little | 13 | 28.3 | 5 | 21.7 | 8 | 34.8 |
| Not at all | 19 | 41.3 | 11 | 47.8 | 8 | 34.8 |
| I would only do the self-examination under the supervision of a doctor | ||||||
| I completely agree | 10 | 21.7 | 6 | 26.1 | 4 | 17.4 |
| Agree | 8 | 17.4 | 5 | 21.7 | 3 | 13.0 |
| Neither agree nor disagree | 12 | 26.1 | 5 | 21.7 | 7 | 30.4 |
| A little | 5 | 10.9 | 3 | 13.0 | 2 | 8.7 |
| Not at all | 11 | 23.9 | 4 | 17.4 | 7 | 30.4 |
| I am concerned that the self-examination may be harmful to me or the child | ||||||
| I completely agree | 0 | 0 | 0 | 0 | 0 | 0 |
| Agree | 0 | 0 | 0 | 0 | 0 | 0 |
| Neither agree nor disagree | 2 | 4.3 | 2 | 8.7 | 0 | 0 |
| A little | 11 | 23.9 | 4 | 17.4 | 7 | 30.4 |
| Not at all | 33 | 71.7 | 17 | 73.9 | 16 | 69.6 |
| I would like to do the self-examination at home | ||||||
| I completely agree | 18 | 39.1 | 7 | 30.4 | 11 | 47.8 |
| Agree | 9 | 19.6 | 6 | 26.1 | 3 | 13.0 |
| Neither agree nor disagree | 11 | 23.9 | 6 | 26.1 | 5 | 21.7 |
| A little | 7 | 15.2 | 4 | 17.4 | 3 | 13.0 |
| Not at all | 1 | 2.2 | 0 | 0 | 1 | 2.3 |
| Evaluation | Cohort A and B (n = 46) | Cohort A (n = 23) | Cohort B (n = 23) | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Amniotic fluid—images | ||||||
| Target structure located | 37 | 80.4 | 17 | 73.9 | 20 | 87.0 |
| Target structure not located | 3 | 6.5 | 1 | 4.3 | 2 | 8.7 |
| Target structure located, but quality low | 6 | 13.0 | 5 | 21.7 | 1 | 4.3 |
| Amniotic fluid—videos | ||||||
| Target structure located | 43 | 93.5 | 20 | 87.0 | 23 | 100 |
| Target structure not located | 1 | 2.2 | 1 | 4.3 | 0 | 0 |
| Target structure located, but quality low | 2 | 4.3 | 2 | 8.7 | 0 | 0 |
| Amniotic fluid—total images | ||||||
| 4 out of 4 with sufficient quality | 20 | 43.5 | 8 | 34.8 | 12 | 52.2 |
| Amniotic fluid—total videos | ||||||
| 4 out of 4 with sufficient quality | 24 | 52.2 | 10 | 43.5 | 14 | 60.9 |
| Heartbeat—videos | ||||||
| Target structure located | 24 | 52.2 | 6 | 26.1 | 18 | 78.3 |
| Target structure not located | 10 | 21.7 | 8 | 34.8 | 2 | 8.7 |
| Target structure located, but quality low | 12 | 26.1 | 9 | 39.1 | 3 | 13.0 |
| Fetal profile—images | 28 | 13 | 15 | |||
| Target structure located | 4 | 14.3 | 1 | 7.7 | 3 | 20.0 |
| Target structure not located | 23 | 82.1 | 11 | 84.6 | 12 | 80.0 |
| Target structure located, but quality low | 1 | 3.6 | 1 | 7.7 | 0 | 0 |
| Fetal profile—videos | 28 | 13 | 15 | |||
| Target structure located | 5 | 17.9 | 2 | 15.4 | 3 | 20.0 |
| Target structure not located | 23 | 82.1 | 11 | 84.6 | 12 | 80.0 |
| Target structure located, but quality low | 0 | 0 | 0 | 0 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pontones, C.A.; Titzmann, A.; Huebner, H.; Danzberger, N.; Ruebner, M.; Häberle, L.; Eskofier, B.M.; Nissen, M.; Kehl, S.; Faschingbauer, F.; et al. Feasibility and Acceptance of Self-Guided Mobile Ultrasound among Pregnant Women in Routine Prenatal Care. J. Clin. Med. 2023, 12, 4224. https://doi.org/10.3390/jcm12134224
Pontones CA, Titzmann A, Huebner H, Danzberger N, Ruebner M, Häberle L, Eskofier BM, Nissen M, Kehl S, Faschingbauer F, et al. Feasibility and Acceptance of Self-Guided Mobile Ultrasound among Pregnant Women in Routine Prenatal Care. Journal of Clinical Medicine. 2023; 12(13):4224. https://doi.org/10.3390/jcm12134224
Chicago/Turabian StylePontones, Constanza A., Adriana Titzmann, Hanna Huebner, Nina Danzberger, Matthias Ruebner, Lothar Häberle, Bjoern M. Eskofier, Michael Nissen, Sven Kehl, Florian Faschingbauer, and et al. 2023. "Feasibility and Acceptance of Self-Guided Mobile Ultrasound among Pregnant Women in Routine Prenatal Care" Journal of Clinical Medicine 12, no. 13: 4224. https://doi.org/10.3390/jcm12134224