
Determinants of Renal Micro-Perfusion as Assessed with Contrast-Enhanced Ultrasound in Healthy Males and Females
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design and Settings
2.3. Laboratory
2.4. Renal Ultrasound Parameters
2.5. Statistics
3. Results
3.1. Participants and Baseline Characteristics
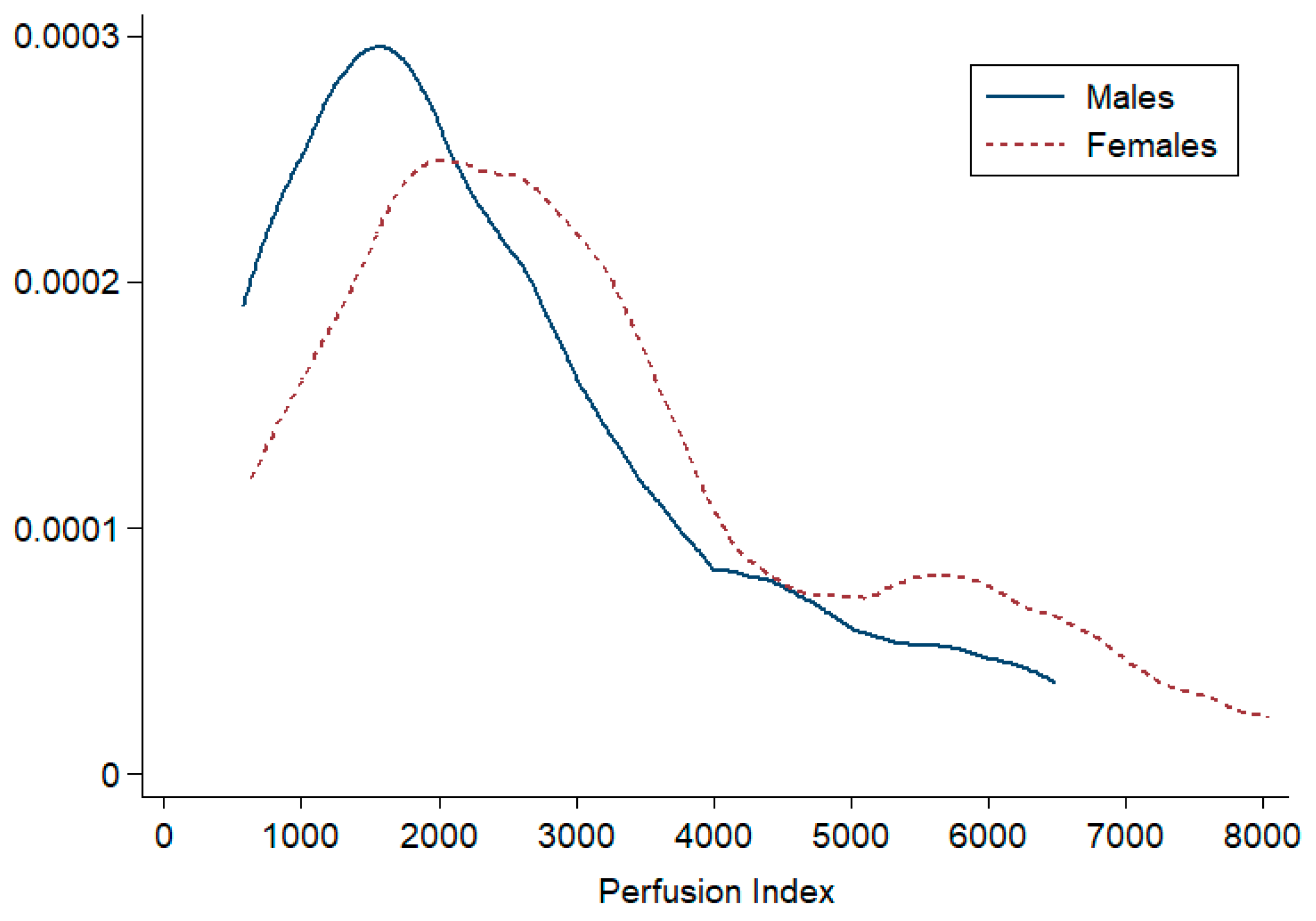
3.2. Doppler US and CEUS Parameters
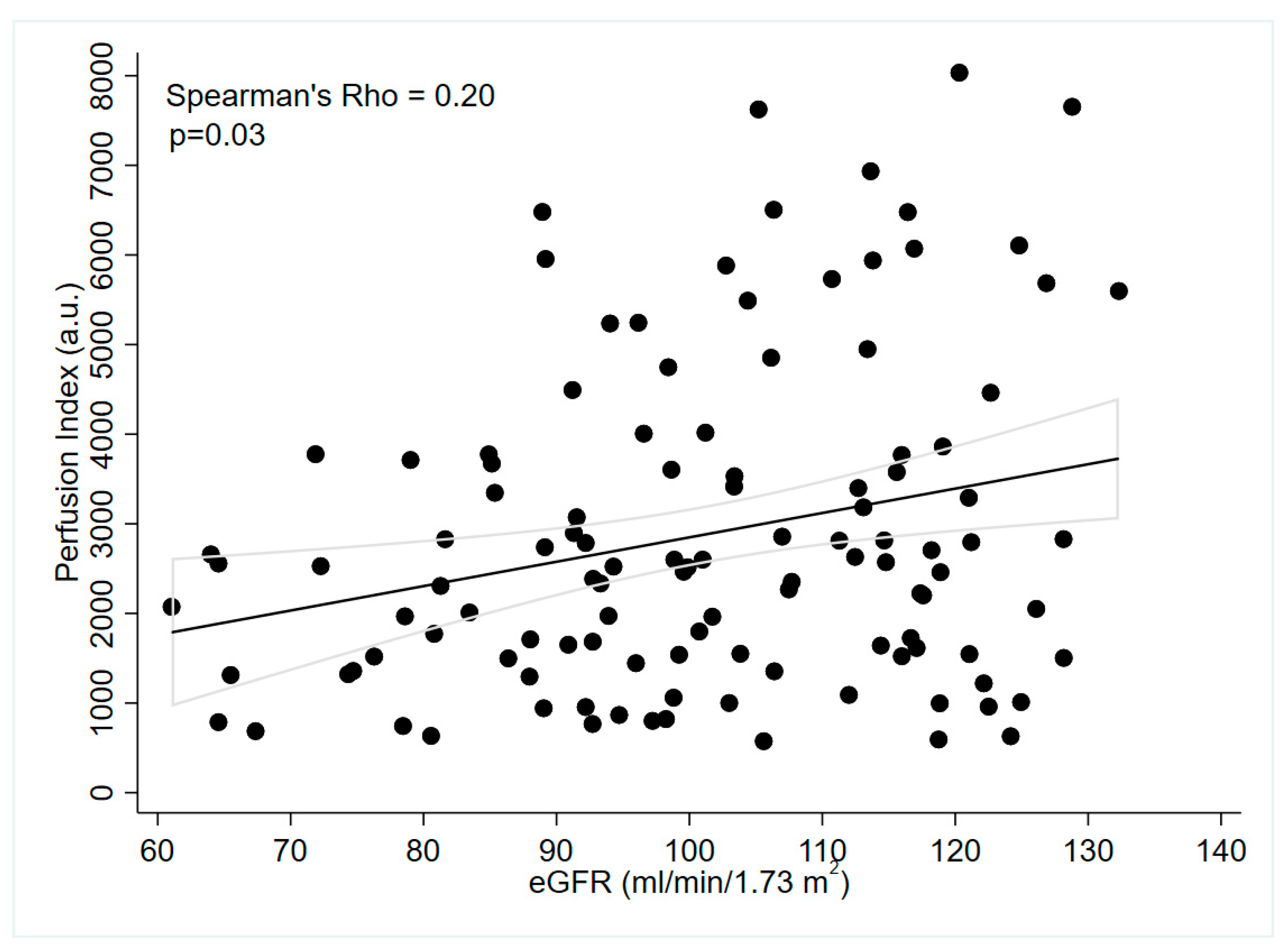
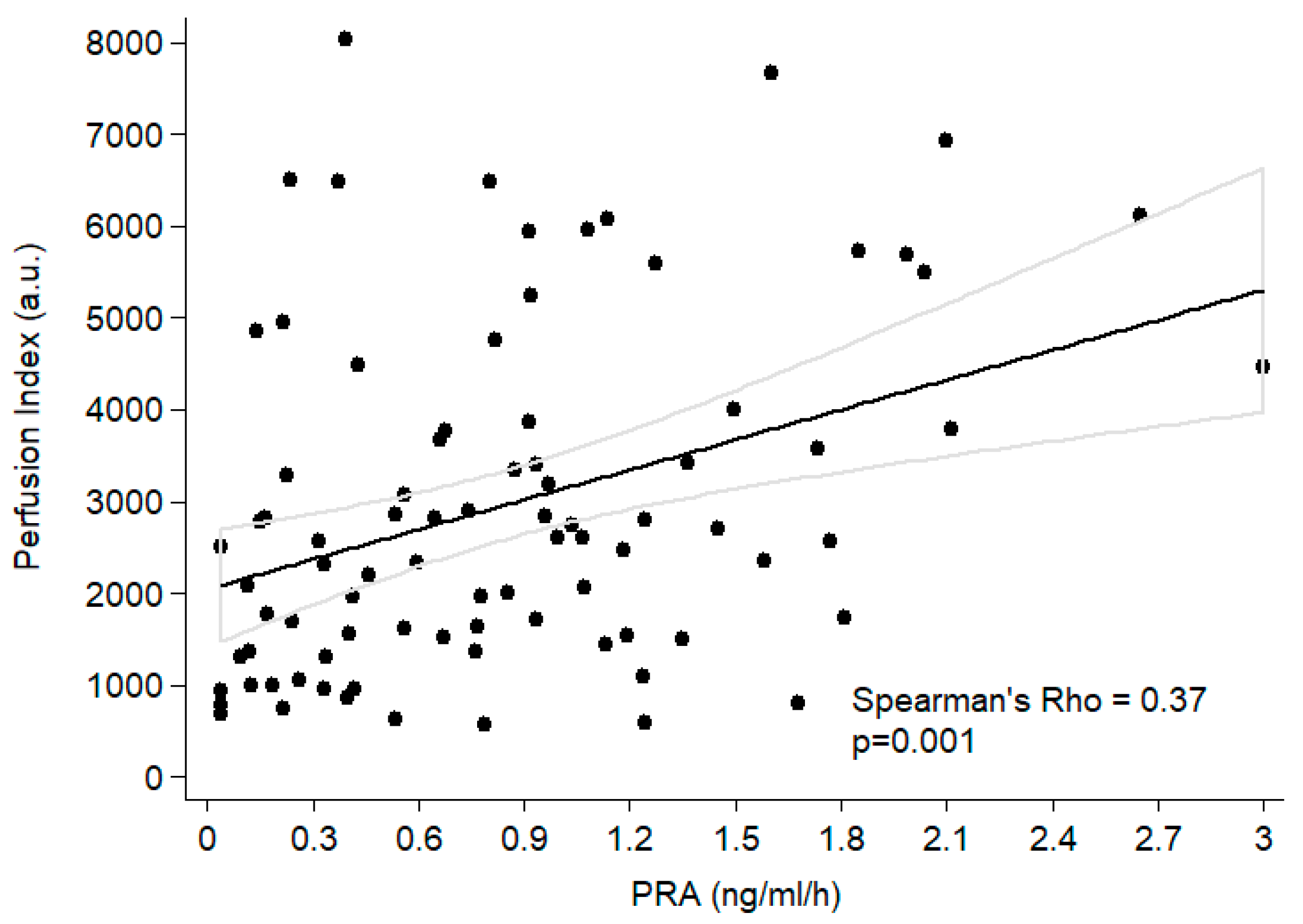
3.3. Associations between CEUS Indices and Clinical and Laboratory Variables
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prowle, J.R.; Ishikawa, K.; May, C.N.; Bellomo, R. Renal blood flow during acute renal failure in man. Blood Purif. 2009, 28, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.L.; Lee, V.S. Renal perfusion imaging by MRI. J. Magn. Reson. Imaging 2020, 52, 369–379. [Google Scholar] [CrossRef]
- Qian, X.; Zhen, J.; Meng, Q.; Li, L.; Yan, J. Intrarenal Doppler approaches in hemodynamics: A major application in critical care. Front. Physiol. 2022, 13, 951307. [Google Scholar] [CrossRef]
- Fan, L.; Wang, S.; He, X.; Gonzalez-Fernandez, E.; Lechene, C.; Fan, F.; Roman, R.J. Visualization of the intrarenal distribution of capillary blood flow. Physiol. Rep. 2019, 7, e14065. [Google Scholar] [CrossRef] [Green Version]
- Chade, A.R. Small Vessels, Big Role: Renal Microcirculation and Progression of Renal Injury. Hypertension 2017, 69, 551–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.; Wang, F.; Sun, D. The renal microcirculation in chronic kidney disease: Novel diagnostic methods and therapeutic perspectives. Cell Biosci. 2021, 11, 90. [Google Scholar] [CrossRef]
- Carrero, J.J.; Hecking, M.; Chesnaye, N.C.; Jager, K.J. Sex and gender disparities in the epidemiology and outcomes of chronic kidney disease. Nat. Rev. Nephrol. 2018, 14, 151–164. [Google Scholar] [CrossRef]
- Swartling, O.; Rydell, H.; Stendahl, M.; Segelmark, M.; Trolle Lagerros, Y.; Evans, M. CKD Progression and Mortality Among Men and Female: A Nationwide Study in Sweden. Am. J. Kidney Dis. 2021, 78, 190–199.e191. [Google Scholar] [CrossRef]
- Pechère-Bertschi, A.; Maillard, M.; Stalder, H.; Bischof, P.; Fathi, M.; Brunner, H.R.; Burnier, M. Renal hemodynamic and tubular responses to salt in female using oral contraceptives. Kidney Int. 2003, 64, 1374–1380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pechère-Bertschi, A.; Maillard, M.; Stalder, H.; Brunner, H.R.; Burnier, M. Renal segmental tubular response to salt during the normal menstrual cycle. Kidney Int. 2002, 61, 425–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, A.G.; Hofmann, L.; Wuerzner, G.; Glatz, N.; Maillard, M.; Meuwly, J.Y.; Eggimann, P.; Burnier, M.; Vogt, B. Renal perfusion evaluation with contrast-enhanced ultrasonography. Nephrol. Dial. Transplant. 2012, 27, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Garessus, J.; Brito, W.; Loncle, N.; Vanelli, A.; Hendriks-Balk, M.; Wuerzner, G.; Schneider, A.; Burnier, M.; Pruijm, M. Cortical perfusion as assessed with contrast-enhanced ultrasound is lower in patients with chronic kidney disease than in healthy subjects but increases under low salt conditions. Nephrol. Dial. Transplant. 2022, 37, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Han, B.H.; Park, S.B. Usefulness of Contrast-enhanced Ultrasound in the Evaluation of Chronic Kidney Disease. Curr. Med. Imaging 2021, 17, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Hendriks-Balk, M.C.; Damianaki, A.; Polychronopoulou, E.; Brito, W.; Pruijm, M.; Wuerzner, G. Contrast-Enhanced Ultrasonography Enables the Detection of a Cold Pressor Test-Induced Increase in Renal Microcirculation in Healthy Participants. Front. Cardiovasc. Med. 2022, 9, 899327. [Google Scholar] [CrossRef]
- Stergiou, G.S.; Palatini, P.; Parati, G.; O’Brien, E.; Januszewicz, A.; Lurbe, E.; Persu, A.; Mancia, G.; Kreutz, R. 2021 European Society of Hypertension practice guidelines for office and out-of-office blood pressure measurement. J. Hypertens. 2021, 39, 1293–1302. [Google Scholar] [CrossRef]
- Dong, Y.; Wang, W.P.; Cao, J.; Fan, P.; Lin, X. Early assessment of chronic kidney dysfunction using contrast-enhanced ultrasound: A pilot study. Br. J. Radiol. 2014, 87, 20140350. [Google Scholar] [CrossRef] [Green Version]
- Odudu, A.; Nery, F.; Harteveld, A.A.; Evans, R.G.; Pendse, D.; Buchanan, C.E.; Francis, S.T.; Fernández-Seara, M.A. Arterial spin labelling MRI to measure renal perfusion: A systematic review and statement paper. Nephrol. Dial. Transplant. 2018, 33, ii15–ii21. [Google Scholar] [CrossRef] [Green Version]
- Mora-Gutiérrez, J.M.; Garcia-Fernandez, N.; Slon Roblero, M.F.; Páramo, J.A.; Escalada, F.J.; Wang, D.J.; Benito, A.; Fernández-Seara, M.A. Arterial spin labeling MRI is able to detect early hemodynamic changes in diabetic nephropathy. J. Magn. Reason. Imaging 2017, 46, 1810–1817. [Google Scholar] [CrossRef]
- Pruijm, M.; Hofmann, L.; Piskunowicz, M.; Muller, M.E.; Zweiacker, C.; Bassi, I.; Vogt, B.; Stuber, M.; Burnier, M. Determinants of renal tissue oxygenation as measured with BOLD-MRI in chronic kidney disease and hypertension in humans. PLoS ONE 2014, 9, e95895. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, A.; Sridharan, A.; Walmer, R.W.; Kasoji, S.K.; Burke, L.M.B.; Dayton, P.A.; Johnson, K.A.; Chang, E.H. Association of Contrast-Enhanced Ultrasound-Derived Kidney Cortical Microvascular Perfusion with Kidney Function. Kidney360 2022, 3, 647–656. [Google Scholar] [CrossRef]
- Maric-Bilkan, C.; Manigrasso, M.B. Sex differences in hypertension: Contribution of the renin-angiotensin system. Gend. Med. 2012, 9, 287–291. [Google Scholar] [CrossRef]
- Reckelhoff, J.F. Gender differences in the regulation of blood pressure. Hypertension 2001, 37, 1199–1208. [Google Scholar] [CrossRef] [Green Version]
- Guerci, P.; Ergin, B.; Ince, C. The macro- and microcirculation of the kidney. Best Pract. Res. Clin. Anaesthesiol. 2017, 31, 315–329. [Google Scholar] [CrossRef]
- Mirabito, K.M.; Hilliard, L.M.; Kett, M.M.; Brown, R.D.; Booth, S.C.; Widdop, R.E.; Moritz, K.M.; Evans, R.G.; Denton, K.M. Sex- and age-related differences in the chronic pressure-natriuresis relationship: Role of the angiotensin type 2 receptor. Am. J. Physiol. Renal. Physiol. 2014, 307, F901–F907. [Google Scholar] [CrossRef] [Green Version]
- Hilliard, L.M.; Nematbakhsh, M.; Kett, M.M.; Teichman, E.; Sampson, A.K.; Widdop, R.E.; Evans, R.G.; Denton, K.M. Gender differences in pressure-natriuresis and renal autoregulation: Role of the Angiotensin type 2 receptor. Hypertension 2011, 57, 275–282. [Google Scholar] [CrossRef] [Green Version]
- Krejza, J.; Ustymowicz, A.; Szylak, A.; Tomaszewski, M.; Hryniewicz, A.; Jawad, A. Assessment of variability of renal blood flow Doppler parameters during the menstrual cycle in female. Ultrasound Obstet. Gynecol. 2005, 25, 60–69. [Google Scholar] [CrossRef]
- Di Nicolò, P.; Granata, A. Renal Resistive Index: Not only kidney. Clin. Exp. Nephrol. 2017, 21, 359–366. [Google Scholar] [CrossRef]
- Berkowitz, H.D.; Galvin, C.C.; Miller, L.D. The control of renal cortical perfusion by the renin angiotensin system. Ann. Surg. 1974, 179, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.H.; Ferris, T.F. The physiology of renin. Arch. Intern. Med. 1973, 131, 860–872. [Google Scholar] [CrossRef] [PubMed]
- Kobori, H.; Urushihara, M. Augmented intrarenal and urinary angiotensinogen in hypertension and chronic kidney disease. Pflugers Arch. 2013, 465, 3–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishiyama, A.; Kobori, H. Independent regulation of renin-angiotensin-aldosterone system in the kidney. Clin. Exp. Nephrol. 2018, 22, 1231–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burns, K.D. Angiotensin II and its receptors in the diabetic kidney. Am. J. Kidney Dis. 2000, 36, 449–467. [Google Scholar] [CrossRef] [PubMed]
- Guan, Z.; VanBeusecum, J.P.; Inscho, E.W. Endothelin and the renal microcirculation. Semin. Nephrol. 2015, 35, 145–155. [Google Scholar] [CrossRef] [Green Version]
- Kohan, D.E.; Inscho, E.W.; Wesson, D.; Pollock, D.M. Physiology of endothelin and the kidney. Compr. Physiol. 2011, 1, 883–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Total n = 115 | Males n = 38 | Females n = 77 | p |
|---|---|---|---|---|
| Age (years) | 37 ± 12 | 37 ± 13 | 37 ± 12 | 0.81 |
| BMI (kg/m2) | 24.1 ± 3.4 | 24.6 ± 3.4 | 23.8 ± 3.3 | 0.26 |
| SBP (mmHg) | 117 ± 11 | 124 ± 7 | 113 ± 10 | 0.00 |
| DBP (mmHg) | 71 ± 8 | 72 ± 9 | 70 ± 7 | 0.34 |
| MBP (mmHg) | 86 ± 8 | 89 ± 7 | 84 ± 7 | 0.00 |
| HR (bpm) | 66 ± 10 | 61 ± 10 | 68 ± 9 | 0.00 |
| Creatinine (µmol/L) | 72 ± 11 | 82 ± 10 | 67 ± 9 | 0.00 |
| eGFR (mL/min/1.73 m2) | 101 ± 17 | 91 ± 17 | 106 ± 15 | 0.00 |
| Sodium (mmol/L) | 140 ± 2 | 141 ± 1 | 140 ± 2 | 0.11 |
| Potassium (mmol/L) | 3.81 ± 0.27 | 3.89 ± 0.25 | 3.77 ± 0.27 | 0.03 |
| Uric acid (mmol/L) | 279 ± 119 | 321 ± 56 | 259 ± 135 | 0.01 |
| Bicarbonate (mmol/L) | 23 ± 2 | 24 ± 2 | 23 ± 1 | 0.00 |
| PRA (ng/mL/h) | 0.77 (0.33–1.19) | 0.40 (0.15–0.87) | 0.93(0.54–1.27) | 0.001 |
| PAC (pmol/L) | 127 (69–222) | 81 (34–149) | 164 (94–278) | 0.0002 |
| Parameters | Males n = 38 | Females n = 77 | p |
|---|---|---|---|
| PI (a.u) | 1965 (1294–3346) | 2705 (1641–3777) | 0.02 |
| rBV (a.u.) | 4149 (2386–6562) | 4895 (3330–7020) | 0.21 |
| mTT (s) | 2.15 (1.7–2.7) | 1.85 (1.53–2.34) | 0.09 |
| RRI (a.u.) | 0.60 (0.56–0.64) | 0.63 (0.60–0.66) | 0.0003 |
| Kidney Volume (mL) | 129 (97–159) | 109 (94–129) | 0.04 |
| Parameter | Follicular n = 15 | Luteal n = 11 | p |
|---|---|---|---|
| PI (a.u.) | 2857 (1445–4748) | 2571 (2224–3604) | 0.83 |
| rBV | 4895 (2872–7010) | 4982 (3322–5800) | 0.92 |
| mTT (s) | 1.68 (1.53–2.09) | 1.81 (1.50–2.34) | 0.84 |
| RRI | 0.61 (0.60–0.66) | 0.64 (0.62–0.65) | 0.31 |
| Clinical Variables | Fully Adjusted β (95% CI) | p |
|---|---|---|
| Sex (Female vs. Male) | 0.065 (−0.33 to 0.46) | 0.74 |
| eGFR (mL/min/1.73 m2) | 0.002 (−0.008 to 0.011) | 0.69 |
| SBP (mmHg) | −0.007 (−0.02 to 0.10) | 0.43 |
| HR (bpm) | 0.005 (−0.011 to 0.02) | 0.55 |
| Potassium (mmol/L) | −0.22 (−0.74 to 0.30) | 0.40 |
| Bicarbonates (mmol/L) | −0.05 (−0.15 to 0.05) | 0.35 |
| PRA-Log (ng/mL/h) | 0.17 (0.01 to 0.33) | 0.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ulpiano Trillig, A.; Damianaki, A.; Hendriks-Balk, M.; Brito, W.; Garessus, J.; Burnier, M.; Wuerzner, G.; Pruijm, M. Determinants of Renal Micro-Perfusion as Assessed with Contrast-Enhanced Ultrasound in Healthy Males and Females. J. Clin. Med. 2023, 12, 4141. https://doi.org/10.3390/jcm12124141
Ulpiano Trillig A, Damianaki A, Hendriks-Balk M, Brito W, Garessus J, Burnier M, Wuerzner G, Pruijm M. Determinants of Renal Micro-Perfusion as Assessed with Contrast-Enhanced Ultrasound in Healthy Males and Females. Journal of Clinical Medicine. 2023; 12(12):4141. https://doi.org/10.3390/jcm12124141
Chicago/Turabian StyleUlpiano Trillig, Antonio, Aikaterini Damianaki, Mariëlle Hendriks-Balk, Wendy Brito, Jonas Garessus, Michel Burnier, Grégoire Wuerzner, and Menno Pruijm. 2023. "Determinants of Renal Micro-Perfusion as Assessed with Contrast-Enhanced Ultrasound in Healthy Males and Females" Journal of Clinical Medicine 12, no. 12: 4141. https://doi.org/10.3390/jcm12124141