
The Beneficial Effect of Preoperative Exercise on Postoperative Clinical Outcome, Quality of Life and Return to Work after Microsurgical Resection of Spinal Meningiomas
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Surgery
3.3. Outcome
3.4. Return to Work
3.5. Sports
3.5.1. Regular Physical Activity before Surgery
3.5.2. Regular Physical Activity after Surgery
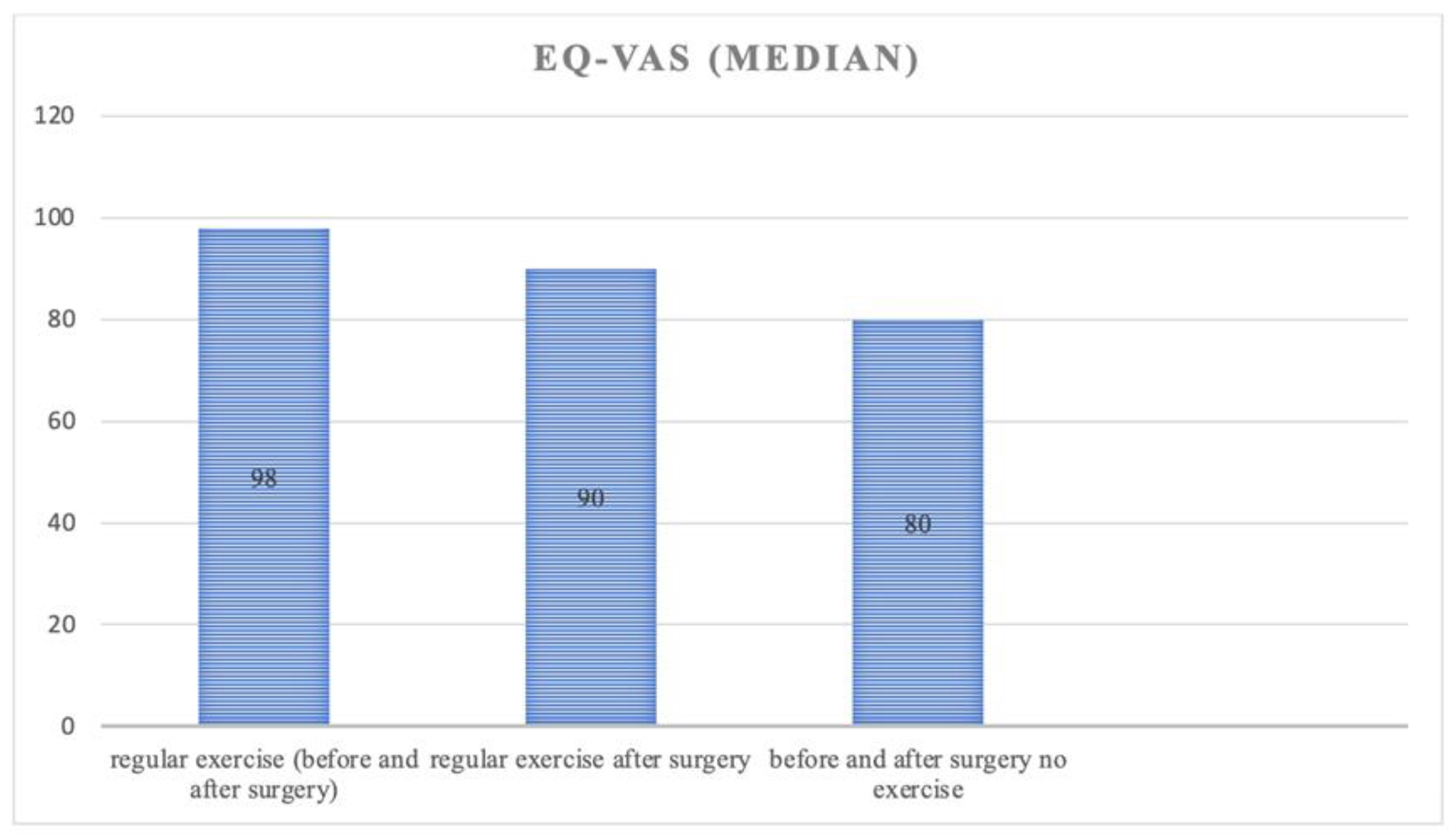
3.5.3. Health Related Quality of Life (HRQoL)
4. Discussion
5. Conclusions
5.1. Limitations
5.2. Disclosures
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maiuri, F.; De Caro, M.D.B.; de Divitiis, O.; Vergara, P.; Mariniello, G. Spinal meningiomas: Age-related features. Clin. Neurol. Neurosurg. 2011, 113, 34–38. [Google Scholar] [CrossRef]
- Duong, L.M.; McCarthy, B.J.; McLendon, R.E.; Dolecek, T.A.; Kruchko, C.; Douglas, L.L.; Ajani, U.A. Descriptive epidemiology of malignant and nonmalignant primary spinal cord, spinal meninges, and cauda equina tumors, United States, 2004–2007. Cancer 2012, 118, 4220–4227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westwick, H.J.; Shamji, M.F. Effects of sex on the incidence and prognosis of spinal meningiomas: A Surveillance, Epidemiology, and End Results study. J. Neurosurg. Spine 2015, 23, 368–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solero, C.L.; Fornari, M.; Giombini, S.; Lasio, G.; Oliveri, G.; Cimino, C.; Pluchino, F. Spinal Meningiomas: Review of 174 Operated Cases. Neurosurgery 1989, 25, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Gottfried, O.N.; Gluf, W.; Quinones-Hinojosa, A.; Kan, P.; Schmidt, M.H. Spinal meningiomas: Surgical management and outcome. Neurosurg. Focus 2003, 14, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roux, F.X.; Nataf, F.; Pinaudeau, M.; Borne, G.; Devaux, B.; Meder, J.F. Intraspinal meningiomas: Review of 54 cases with discussion of poor prognosis factors and modern therapeutic management. Surg. Neurol. 1996, 46, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Levy, W.J.; Bay, J.; Dohn, D. Spinal cord meningioma. J. Neurosurg. 1982, 57, 804–812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arwert, H.J.; Schults, M.; Meesters, J.J.L.; Wolterbeek, R.; Boiten, J.; Vliet Vlieland, T. Return to Work 2–5 Years After Stroke: A Cross Sectional Study in a Hospital-Based Population. J. Occup. Rehabil. 2017, 27, 239–246. [Google Scholar] [CrossRef]
- Corrigan, J.D.; Bogner, J.A.; Mysiw, W.J.; Clinchot, D.; Fugate, L. Life Satisfaction After Traumatic Brain Injury. J. Head Trauma Rehabil. 2001, 16, 543–555. [Google Scholar] [CrossRef]
- Passier, P.E.; Visser-Meily, J.M.; Rinkel, G.J.; Lindeman, E.; Post, M.W. Life Satisfaction and Return to Work After Aneurysmal Subarachnoid Hemorrhage. J. Stroke Cerebrovasc. Dis. 2011, 20, 324–329. [Google Scholar] [CrossRef]
- Zamanipoor Najafabadi, A.H.; Peeters, M.C.M.; Dirven, L.; Lobatto, D.J.; Groen, J.L.; Broekman, M.L.D.; Peerdeman, S.M.; Peul, W.C.; Taphoorn, M.J.B.; van Furth, W.R. Impaired health-related quality of life in meningioma patients-a systematic review. Neuro Oncol. 2017, 19, 897–907. [Google Scholar] [CrossRef] [PubMed]
- Moons, P.; Budts, W.; de Geest, S. Critique on the conceptualisation of quality of life: A review and evaluation of different conceptual approaches. Int. J. Nurs. Stud. 2006, 43, 891–901. [Google Scholar] [CrossRef]
- Kilinc, F.; Setzer, M.; Marquardt, G.; Keil, F.; Dubinski, D.; Bruder, M.; Seifert, V.; Behmanesh, B. Functional outcome and morbidity after microsurgical resection of spinal meningiomas. Neurosurg. Focus. 2021, 50, E20. [Google Scholar] [CrossRef] [PubMed]
- Brooks, R. EuroQol: The current state of play. Health Policy 1996, 37, 53–72. [Google Scholar] [CrossRef] [PubMed]
- Buchholz, I.; Janssen, M.F.; Kohlmann, T.; Feng, Y.S. A Systematic Review of Studies Comparing the Measurement Properties of the Three-Level and Five-Level Versions of the EQ-5D. Pharmacoeconomics 2018, 36, 645–661. [Google Scholar] [CrossRef] [Green Version]
- Schiavolin, S.; Mariniello, A.; Broggi, M.; Acerbi, F.; Schiariti, M.; Franzini, A.; Di Meco, F.; Ferroli, P.; Leonardi, M. Characteristics of Patients Returning to Work After Brain Tumor Surgery. Front. Hum. Neurosci. 2020, 14. [Google Scholar] [CrossRef]
- Pettersson-Segerlind, J.; von Vogelsang, A.-C.; Fletcher-Sandersjöö, A.; Tatter, C.; Mathiesen, T.; Edström, E.; Elmi-Terander, A. Health-Related Quality of Life and Return to Work after Surgery for Spinal Meningioma: A Population-Based Cohort Study. Cancers 2021, 13, 6371. [Google Scholar] [CrossRef] [PubMed]
- Thurin, E.; Corell, A.; Gulati, S.; Smits, A.; Henriksson, R.; Bartek, J., Jr.; Salvesen, Ø.; Jakola, A.S. Return to work following meningioma surgery: A Swedish nationwide registry-based matched cohort study. Neurooncol. Pract. 2020, 7, 320–328. [Google Scholar] [CrossRef]
- Sekely, A.; Zakzanis, K.K.; Mabbott, D.; Tsang, D.S.; Kongkham, P.; Zadeh, G.; Edelstein, K. Long-term neurocognitive, psychological, and return to work outcomes inmeningioma patients. Support. Care Cancer 2022, 30, 3893–3902. [Google Scholar] [CrossRef] [PubMed]
- Schepers, V.; Vossen, S.; Sprenkel, J.; Visser-Meily, J.; Post, M. Participation restrictions in patients after surgery for cerebral meningioma. J. Rehabil. Med. 2018, 50, 879–885. [Google Scholar] [CrossRef] [Green Version]
- Behmanesh, B.; Gessler, F.; Won, S.-Y.; Dubinski, D.; Quick-Weller, J.; Imoehl, L.; Seifert, V.; Marquardt, G. Return to work and clinical outcome after surgical treatment and conservative management of patients with intramedullary spinal cord ependymoma. Sci. Rep. 2020, 10, 2335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McVeigh, S.A.; Hitzig, S.L.; Craven, B.C. Influence of Sport Participation on Community Integration and Quality of Life: A Comparison between Sport Participants and Non-Sport Participants with Spinal Cord Injury. J. Spinal Cord. Med. 2009, 32, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Cormie, P.; Nowak, A.K.; Chambers, S.K.; Galvão, D.A.; Newton, R.U. The Potential Role of Exercise in Neuro-Oncology. Front. Oncol. 2015, 5, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, P.T. Reduced Risk of Brain Cancer Mortality from Walking and Running. Med. Sci. Sports Exerc. 2014, 46, 927–932. [Google Scholar] [CrossRef]
- Fanelli, E.; Daga, F.A.; Pappaccogli, M.; Eula, E.; Astarita, A.; Mingrone, G.; Fasano, C.; Magnino, C.; Schiavone, D.; Rabbone, I.; et al. A structured physical activity program in an adolescent population with overweight or obesity: A prospective interventional study. Appl. Physiol. Nutr. Metab. 2022, 47, 253–260. [Google Scholar] [CrossRef]
- Ford, E.S.; Moriarty, D.G.; Zack, M.M.; Mokdad, A.H.; Chapman, D.P. Self-Reported Body Mass Index and Health-Related Quality of Life: Findings from the Behavioral Risk Factor Surveillance System. Obes. Res. 2001, 9, 21–31. [Google Scholar] [CrossRef]
- Heo, M.; Allison, D.B.; Faith, M.S.; Zhu, S.; Fontaine, K.R. Obesity and Quality of Life: Mediating Effects of Pain and Comorbidities. Obes. Res. 2003, 11, 209–216. [Google Scholar] [CrossRef]
- Groessl, E.J.; Kaplan, R.M.; Barrett-Connor, E.; Ganiats, T.G. Body mass index and quality of well-being in a community of older adults. Am. J. Prev. Med. 2004, 26, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Groeneveld, I.F.; de Boer, A.G.E.M.; Frings-Dresen, M.H.W. Physical exercise and return to work: Cancer survivors’ experiences. J. Cancer Surviv. 2013, 7, 237–246. [Google Scholar] [CrossRef]
- Hughes, M.J.; Hackney, R.J.; Lamb, P.J.; Wigmore, S.J.; Christopher Deans, D.A.; Skipworth, R.J.E. Prehabilitation Before Major Abdominal Surgery: A Systematic Review and Meta-analysis. World J. Surg. 2019, 43, 1661–1668. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n (%) | |
|---|---|
| Mean age, y (± SD) | 51 ± 12.5 |
| Male | 36 (27.7) |
| Female | 94 (72.3) |
| Tumor location | |
| Cervical | 41 (31.5) |
| Cervicothoracic | 5 (3.8) |
| Thoracic | 79 (60.8) |
| Thoracolumbar | 3 (2.3) |
| Lumbar | 2 (1.5) |
| Affected level | |
| 1 | 101 (78) |
| 2 | 26 (20.4) |
| >2 | 3 (2.3) |
| Charlson Comorbidity Index (CCI) | |
| 0 | 54 (41.5) |
| 1 | 35 (26.9) |
| 2 | 37 (28.5) |
| 3 | 3 (2.3) |
| 4 | 1 (0.7) |
| 5 | 0 (0) |
| Symptoms and signs | |
| Sensory deficit | 51 (38.9) |
| Motor weakness | 35 (26.8) |
| Gait ataxia | 30 (22.7) |
| Incidental finding | 14 (16.9) |
| Back pain | 21 (15.9) |
| Radicular pain | 18 (13.8) |
| Bladder/bowl dysfunction | 8 (5.9) |
| Symptoms duration until surgery | |
| 0–3 months | 48 (36.9) |
| 4–6 months | 32 (24.6) |
| 7–9 months | 16 (12.3) |
| 10–12 months | 14 (10.8) |
| >12 months | 20 (15.4) |
| Calcification None | 126 (96.9) |
| Partial | 4 (3.1) |
| BMI | |
| 18.5–24.9 (normal) | 75 (57.7) |
| 25.0–29.9 (overweight) | 30 (23.1) |
| 30.0–34.9 (obese Class I) | 19 (14.6) |
| 35.0–39.9 (obese Class II) | 6 (4.6) |
| n (%) | |
|---|---|
| Surgical approach Laminectomy | 89 (68.5) |
| Hemilaminectomy | 38 (29.2) |
| Laminoplasty | 3 (2.3) |
| EOR | |
| GTR | 119 (91.5) |
| STR | 11 (8.5) |
| Mean surgical time, min | 183 |
| ASA | |
| I | 5 (3.8) |
| II | 89 (68.5) |
| III | 33 (25.4) |
| IV | 3 (2.3) |
| Dural attachment | |
| Ventral | 13 (10.0) |
| Ventrolateral | 18 (13.8) |
| Lateral | 27 (20.8) |
| Dorsolateral | 28 (21.5) |
| Dorsal | 44 (33.8) |
| Surgeon´s experience | |
| <10 years | 7 (5.4) |
| >10 years | 123 (94.6) |
| Histology WHO 1 | |
| Meningothelial | 101 (77.7) |
| Psammomatous | 9 (6.9) |
| Fibromatose | 6 (4.6) |
| Transitional | 2 (1.5) |
| Angiomatous | 1 (0.8) |
| WHO grade 2 | 11 (8.5) |
| n (%) | |
|---|---|
| Follow up (median, months) | 96 |
| ECOG grade on admission | |
| 0 | 41 (31.5) |
| 1 | 64 (49.2) |
| 2 | 24 (18.5) |
| 3 | 1 (0.7) |
| 4 | 0 (0) |
| ECOG grade at the end of FU 0 | 124 (95.4) |
| 1 | 6 (4.6) |
| 2 | 0 (0) |
| 3 | 0 (0) |
| 4 | 0 (0) |
| Neurological status at the end of FU | |
| Stable | 113 (86.9) |
| Improved | 17 (13.1) |
| Preoperative Occupation | Postoperative Occupation | Change | |
|---|---|---|---|
| Full time | 108 (83.1) | 112 (86.2) | +3% |
| Part time | 22 (16.9) | 18 (13.8) | −3% |
| Intellectual work | 24 (18.5) | 24 (18.5) | |
| Manual labor | 26 (20.0) | 26 (20.0) | |
| Office work | 80 (61.5) | 80 (61.5) |
| Time to Return to Work (RtW) | n (%) |
|---|---|
| <1 month | 27 (20.8) |
| 1–3 months | 57 (43.8) |
| 3–6 months | 23 (17.7) |
| >9 months | 23 (17.7) |
| Univariate Analysis, p Value | Multivariate Analysis, p Value | |
|---|---|---|
| Weight | 0.033 | 0.627 |
| Age | 0.023 | 0.725 |
| Simpson | 0.698 | 0.887 |
| Calcification | 0.774 | 0.995 |
| Return to exercise (months) | <0.001 | 0.003 |
| Regular physical exercise | <0.001 | 0.036 |
| ASA | 0.109 | 0.734 |
| Dural attachment | 0.08 | 0.089 |
| CCI | 0.824 | 0.082 |
| Performed Job | 0.824 | 0.071 |
| ECOG FU | 0.129 | 0.139 |
| Surgeon’s experience | 0.098 | 0.099 |
| Individual Activities | n (%) |
|---|---|
| Walking | 10 (33.3) |
| Work outs/Fitness | 15 (16.7) |
| Gymnastic | 2 (20) |
| Bicycle riding | 3 (12.2) |
| 18.5–24.9 (normal) | 5 (35.7) |
| 25.0–29.9 (overweight) | 3 (21.4) |
| 30.0–34.9 (obese Class I) | 4 (28.6) |
| 35.0–39.9 (obese Class II) | 2 (14.3) |
| n (%) | ||
|---|---|---|
| Individual activities | Before | After |
| Walking | 30 (33.3) | 21 (23.3) |
| Work outs/Fitness | 15 (16.7) | 14 (15.6) |
| Gymnastic | 18 (20) | 22 (22.4) |
| Bicycle riding | 11 (12.2) | 9 (10) |
| Team sport | 15 (11.5) | |
| Golf/Tennis | 2 (2.2) | 1 (1.1) |
| Football | 26 (28.9) | 9 (10) |
| n (%) | |
|---|---|
| Sports/Excersice | |
| Regularly before surgery | 90 (69.2%) |
| Regularly after surgery | 104 (80.0%) |
| Time for RtS | |
| <1 month | 83 (63.9) |
| 1–3 months | 15 (11.5) |
| 3–6 months | 5 (7.2) |
| 6–9 months | 1 (0.8) |
| >9 months | 0 (0) |
| Return to work (median, days) | |
| Return to work, total | 45 |
| Return to work regular physical exercise | 30 |
| No physical exercise | 130 |
| Physical exercise after surgery | 52 |
| 18.5–24.9 (normal) | 64 (71) |
| 25.0–29.9 (overweight) | 15 (16.7) |
| 30.0–34.9 (obese Class I) | 8 (9) |
| 35.0–39.9 (obese Class II) | 3 (3.3) |
| EQ-5D-5L | Problem | Regular Exercise n = 90(%) | No Exercise n = 40(%) | p Value |
|---|---|---|---|---|
| Mobility | Level 1 | 88 (97.8) | 29 (72.5) | <0.001 |
| Level 2 | 2 (2.2) | 11 (27.5) | ||
| Level 3 | 0 (0) | 0 (0) | ||
| Level 4 | 0 (0) | 0 (0) | ||
| Level 5 | 0 (0) | 0 (0) | ||
| Self-care | Level 1 | 90 (100) | 32 (80) | <0.001 |
| Level 2 | 0 (0) | 5 (12.5) | ||
| Level 3 | 0 (0) | 3 (7.5) | ||
| Level 4 | 0 (0) | 0 (0) | ||
| Level 5 | 0 (0) | 0 (0) | ||
| Usual activity | Level 1 | 90 (100) | 31 (77.5) | <0.001 |
| Level 2 | 0 (0) | 5 (12.5) | ||
| Level 3 | 0 (0) | 4 (10) | ||
| Level 4 | 0 (0) | 0 (0) | ||
| Level 5 | 0 (0) | 0 (0) | ||
| Pain/discomfort | Level 1 | 90 (100) | 30 (75) | 0.001 |
| Level 2 | 0 (0) | 8 (20) | ||
| Level 3 | 0 (0) | 2 (5) | ||
| Level 4 | 0 (0) | 0 (0) | ||
| Level 5 | 0 (0) | 0 (0) | ||
| Anxiety/stress | Level 1 | 86 (95.6) | 30 (75) | 0.001 |
| Level 2 | 4 (4.4) | 9 (22.5) | ||
| Level 3 | 0 (0) | 1 (2.5) | ||
| Level 4 | 0 (0) | 0 (0) | ||
| Level 5 | 0 (0) | 0 (0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kilinc, F.; Setzer, M.; Prinz, V.; Jussen, D.; Marquardt, G.; Gessler, F.; Czabanka, M.; Freiman, T.; Dubinski, D.; Won, S.-Y.; et al. The Beneficial Effect of Preoperative Exercise on Postoperative Clinical Outcome, Quality of Life and Return to Work after Microsurgical Resection of Spinal Meningiomas. J. Clin. Med. 2023, 12, 2804. https://doi.org/10.3390/jcm12082804
Kilinc F, Setzer M, Prinz V, Jussen D, Marquardt G, Gessler F, Czabanka M, Freiman T, Dubinski D, Won S-Y, et al. The Beneficial Effect of Preoperative Exercise on Postoperative Clinical Outcome, Quality of Life and Return to Work after Microsurgical Resection of Spinal Meningiomas. Journal of Clinical Medicine. 2023; 12(8):2804. https://doi.org/10.3390/jcm12082804
Chicago/Turabian StyleKilinc, Fatma, Matthias Setzer, Vincent Prinz, Daniel Jussen, Gerhard Marquardt, Florian Gessler, Marcus Czabanka, Thomas Freiman, Daniel Dubinski, Sae-Yeon Won, and et al. 2023. "The Beneficial Effect of Preoperative Exercise on Postoperative Clinical Outcome, Quality of Life and Return to Work after Microsurgical Resection of Spinal Meningiomas" Journal of Clinical Medicine 12, no. 8: 2804. https://doi.org/10.3390/jcm12082804