
Case Series of Precision Delivery of Methylprednisolone in Pediatric Inflammatory Bowel Disease: Feasibility, Clinical Outcomes, and Identification of a Vasculitic Transcriptional Program
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection and Chart Review
2.2. Imaging
2.3. Methylprednisolone Therapy Administration
2.4. Transcriptomic and Single Cell Analysis
2.5. Statistics and Data Presentation
3. Results
3.1. Clinical Outcomes
3.2. Feasibility and Adverse Events
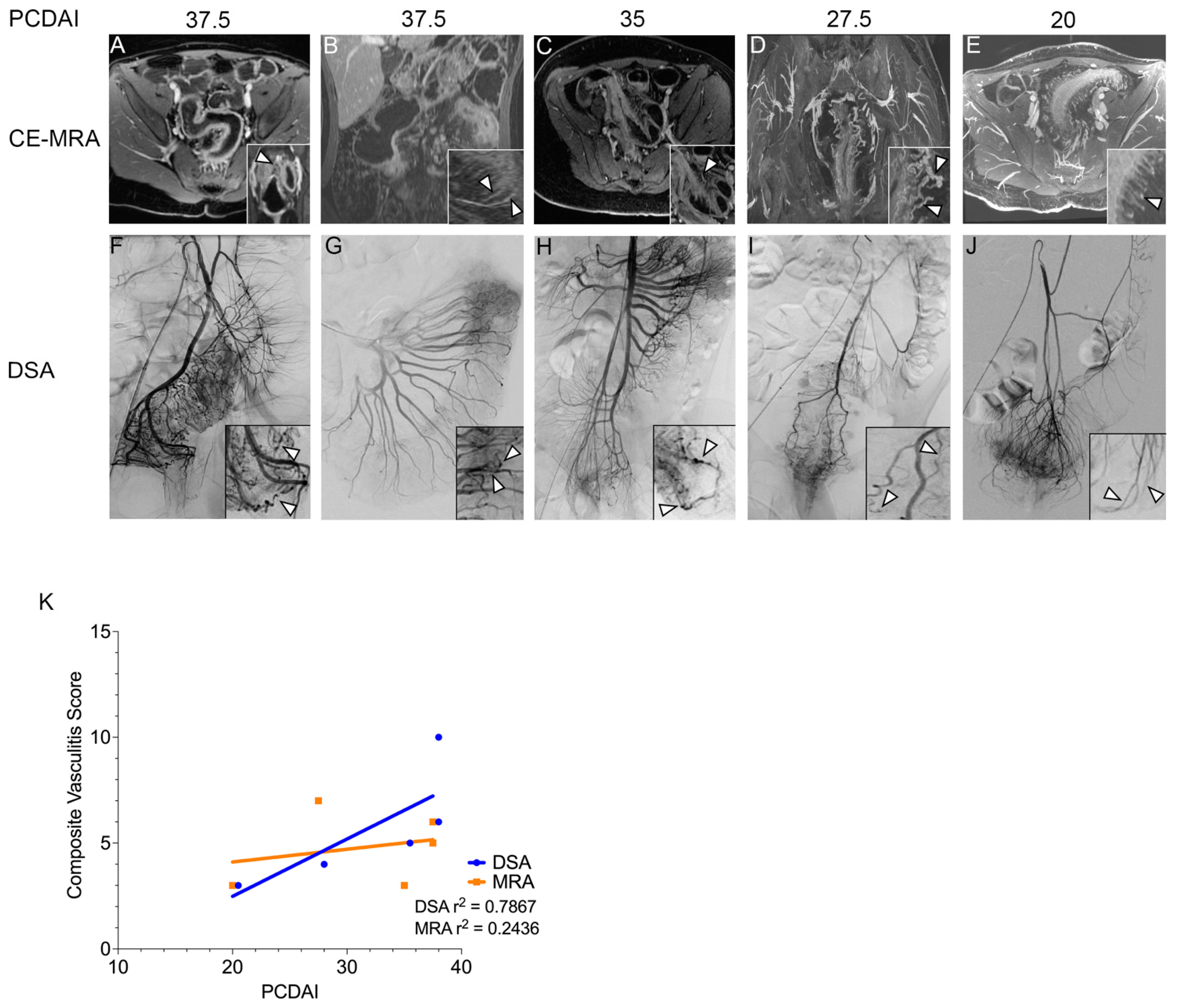
3.3. Vascular Findings in Patients with CD
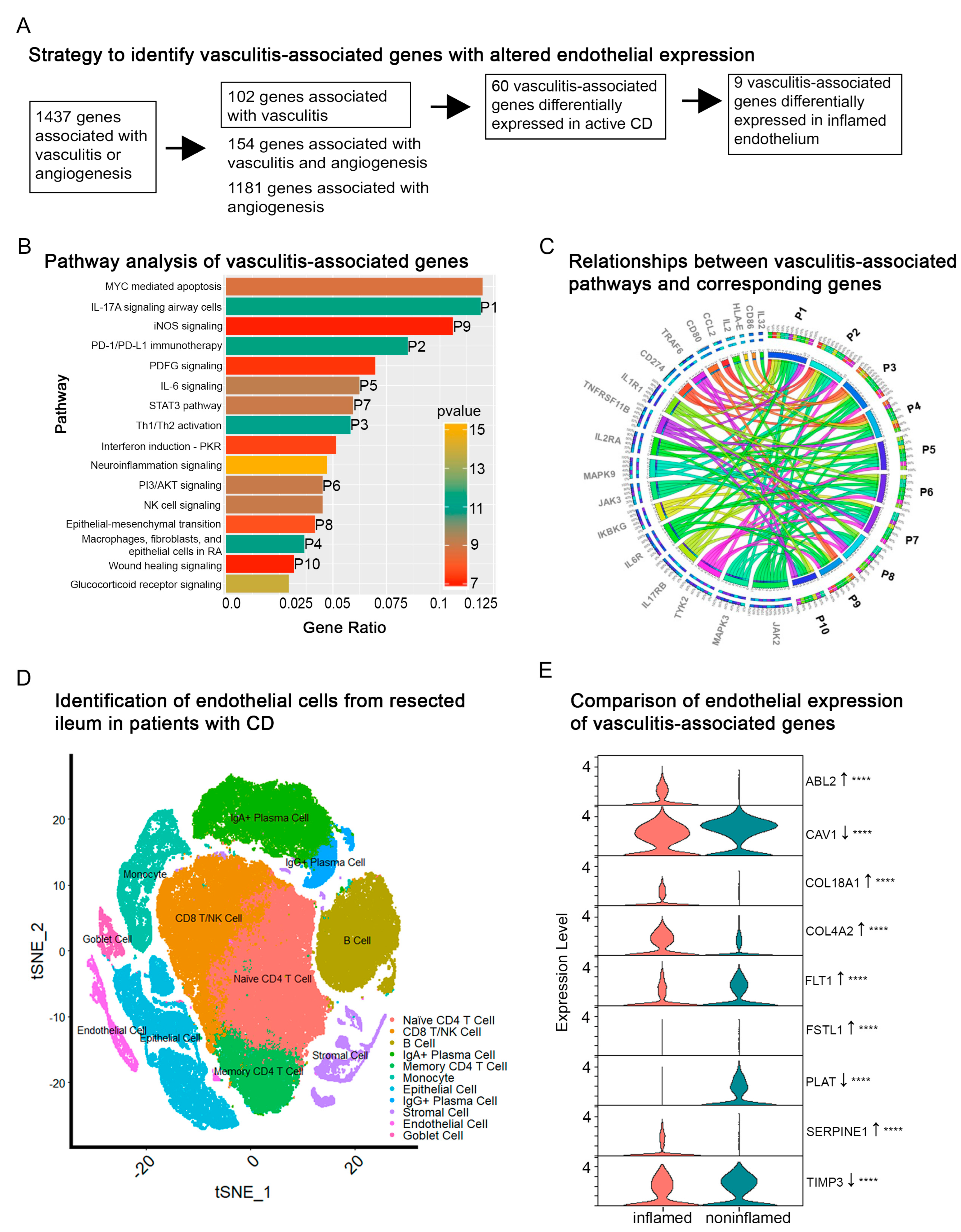
3.4. Transcriptomic Analysis of Vasculitis-Associated Genes in CD
3.5. Single-Cell Analysis of Vasculitis-Associated Genes in the Endothelium of Active CD
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moon, J.S. Clinical Aspects and Treatments for Pediatric Inflammatory Bowel Diseases. Pediatr. Gastroenterol. Hepatol. Nutr. 2019, 22, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Lunderquist, A.; Knutsson, H. Angiography in Crohn’s disease of the small bowel and colon. Am. J. Roentgenol. Radium. Ther. Nucl. Med. 1967, 101, 338–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danese, S.; Sans, M.; de la Motte, C.; Graziani, C.; West, G.; Phillips, M.H.; Pola, R.; Rutella, S.; Willis, J.; Gasbarrini, A.; et al. Angiogenesis as a novel component of inflammatory bowel disease pathogenesis. Gastroenterology 2006, 130, 2060–2073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakefield, A.J.; Sawyerr, A.M.; Dhillon, A.P.; Pittilo, R.M.; Rowles, P.M.; Lewis, A.A.; Pounder, R.E. Pathogenesis of Crohn’s disease: Multifocal gastrointestinal infarction. Lancet 1989, 2, 1057–1062. [Google Scholar] [CrossRef]
- Saranathan, M.; Rettmann, D.W.; Hargreaves, B.A.; Clarke, S.E.; Vasanawala, S.S. DIfferential Subsampling with Cartesian Ordering (DISCO): A high spatio-temporal resolution Dixon imaging sequence for multiphasic contrast enhanced abdominal imaging. J. Magn. Reson. Imaging 2012, 35, 1484–1492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, Y.W.; Thomsen, H.S. Contrast-enhanced peripheral MRA: Technique and contrast agents. Acta Radiol. 2012, 53, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Vasanawala, S.S.; Nguyen, K.L.; Hope, M.D.; Bridges, M.D.; Hope, T.A.; Reeder, S.B.; Bashir, M.R. Safety and technique of ferumoxytol administration for MRI. Magn. Reson. Med. 2016, 75, 2107–2111. [Google Scholar] [CrossRef] [Green Version]
- Bashir, M.R.; Bhatti, L.; Marin, D.; Nelson, R.C. Emerging applications for ferumoxytol as a contrast agent in MRI. J. Magn. Reson. Imaging 2015, 41, 884–898. [Google Scholar] [CrossRef] [PubMed]
- Bruining, D.H.; Zimmermann, E.M.; Loftus, E.V.; Sandborn, W.J.; Sauer, C.G.; Strong, S.A.; Al-Hawary, M.; Anupindi, S.; Baker, M.E.; Bruining, D.; et al. Consensus Recommendations for Evaluation, Interpretation, and Utilization of Computed Tomography and Magnetic Resonance Enterography in Patients With Small Bowel Crohn’s Disease. Radiology 2018, 286, 776–799. [Google Scholar] [CrossRef] [Green Version]
- Hyams, J.S.; Ferry, G.D.; Mandel, F.S.; Gryboski, J.D.; Kibort, P.M.; Kirschner, B.S.; Griffiths, A.M.; Katz, A.J.; Grand, R.J.; Boyle, J.T. Development and validation of a pediatric Crohn’s disease activity index. J. Pediatr. Gastroenterol. Nutr. 1991, 12, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Guglielmo, F.F.; Anupindi, S.A.; Fletcher, J.G.; Al-Hawary, M.M.; Dillman, J.R.; Grand, D.J.; Bruining, D.H.; Chatterji, M.; Darge, K.; Fidler, J.L.; et al. Small Bowel Crohn Disease at CT and MR Enterography: Imaging Atlas and Glossary of Terms. Radiographics 2020, 40, 354–375. [Google Scholar] [CrossRef]
- Martin, J.C.; Chang, C.; Boschetti, G.; Ungaro, R.; Giri, M.; Grout, J.A.; Gettler, K.; Chuang, L.S.; Nayar, S.; Greenstein, A.J.; et al. Single-Cell Analysis of Crohn’s Disease Lesions Identifies a Pathogenic Cellular Module Associated with Resistance to Anti-TNF Therapy. Cell 2019, 178, 1493–1508.e20. [Google Scholar] [CrossRef]
- MacArthur, J.; Bowler, E.; Cerezo, M.; Gil, L.; Hall, P.; Hastings, E.; Junkins, H.; McMahon, A.; Milano, A.; Morales, J.; et al. The new NHGRI-EBI Catalog of published genome-wide association studies (GWAS Catalog). Nucleic Acids Res. 2017, 45, D896–D901. [Google Scholar] [CrossRef] [PubMed]
- Amado-Azevedo, J.; van Stalborch, A.D.; Valent, E.T.; Nawaz, K.; van Bezu, J.; Eringa, E.C.; Hoevenaars, F.P.M.; De Cuyper, I.M.; Hordijk, P.L.; van Hinsbergh, V.W.M.; et al. Depletion of Arg/Abl2 improves endothelial cell adhesion and prevents vascular leak during inflammation. Angiogenesis 2021, 24, 677–693. [Google Scholar] [CrossRef]
- Moulton, K.S.; Olsen, B.R.; Sonn, S.; Fukai, N.; Zurakowski, D.; Zeng, X. Loss of collagen XVIII enhances neovascularization and vascular permeability in atherosclerosis. Circulation 2004, 110, 1330–1336. [Google Scholar] [CrossRef] [Green Version]
- Seillier, C.; Hélie, P.; Petit, G.; Vivien, D.; Clemente, D.; Le Mauff, B.; Docagne, F.; Toutirais, O. Roles of the tissue-type plasminogen activator in immune response. Cell Immunol. 2022, 371, 104451. [Google Scholar] [CrossRef] [PubMed]
- Momoshima, S.; Kohda, E.; Hiramatsu, K.; Asakura, H. Intraarterial prednisolone infusion therapy in ulcerative colitis. AJR Am. J. Roentgenol. 1985, 145, 1057–1060. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; de Ferranti, S.; Després, J.P.; Fullerton, H.J.; Howard, V.J.; et al. Heart disease and stroke statistics--2015 update: A report from the American Heart Association. Circulation 2015, 131, e29–e322. [Google Scholar] [CrossRef] [Green Version]
- Fifi, J.T.; Meyers, P.M.; Lavine, S.D.; Cox, V.; Silverberg, L.; Mangla, S.; Pile-Spellman, J. Complications of modern diagnostic cerebral angiography in an academic medical center. J. Vasc. Interv. Radiol. 2009, 20, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Burger, I.M.; Murphy, K.J.; Jordan, L.C.; Tamargo, R.J.; Gailloud, P. Safety of cerebral digital subtraction angiography in children: Complication rate analysis in 241 consecutive diagnostic angiograms. Stroke 2006, 37, 2535–2539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauzier, D.C.; Osbun, J.W.; Chatterjee, A.R.; Moran, C.J.; Kansagra, A.P. Safety of pediatric cerebral angiography. J. Neurosurg. Pediatr. 2021, 29, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Agnoletti, G.; Bonnet, C.; Boudjemline, Y.; Le Bihan, C.; Bonnet, D.; Sidi, D.; Bonhoeffer, P. Complications of paediatric interventional catheterisation: An analysis of risk factors. Cardiol. Young 2005, 15, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Lightdale, J.R.; Liu, Q.Y.; Sahn, B.; Troendle, D.M.; Thomson, M.; Fishman, D.S. Pediatric Endoscopy and High-risk Patients: A Clinical Report From the NASPGHAN Endoscopy Committee. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 595–606. [Google Scholar] [CrossRef]
- Eckman, W.W.; Patlak, C.S.; Fenstermacher, J.D. A critical evaluation of the principles governing the advantages of intra-arterial infusions. J. Pharmacokinet. Biopharm. 1974, 2, 257–285. [Google Scholar] [CrossRef] [PubMed]
- Czock, D.; Keller, F.; Rasche, F.M.; Häussler, U. Pharmacokinetics and pharmacodynamics of systemically administered glucocorticoids. Clin. Pharmacokinet. 2005, 44, 61–98. [Google Scholar] [CrossRef]
- Lahad, A.; Weiss, B. Current therapy of pediatric Crohn’s disease. World J. Gastrointest. Pathophysiol. 2015, 6, 33–42. [Google Scholar] [CrossRef] [Green Version]
- Saris, S.C.; Wright, D.C.; Oldfield, E.H.; Blasberg, R.G. Intravascular streaming and variable delivery to brain following carotid artery infusions in the Sprague-Dawley rat. J. Cereb. Blood Flow Metab. 1988, 8, 116–120. [Google Scholar] [CrossRef]
- Cibor, D.; Domagala-Rodacka, R.; Rodacki, T.; Jurczyszyn, A.; Mach, T.; Owczarek, D. Endothelial dysfunction in inflammatory bowel diseases: Pathogenesis, assessment and implications. World J. Gastroenterol. 2016, 22, 1067–1077. [Google Scholar] [CrossRef]
- Yarur, A.J.; Jain, A.; Sussman, D.A.; Barkin, J.S.; Quintero, M.A.; Princen, F.; Kirkland, R.; Deshpande, A.R.; Singh, S.; Abreu, M.T. The association of tissue anti-TNF drug levels with serological and endoscopic disease activity in inflammatory bowel disease: The ATLAS study. Gut 2016, 65, 249–255. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient Background | Age (y) | Sex | Weight (kg) | Pre-Procedure Disease Score | Vessel(s) Accessed and (Methylprednisolone Dose) | Post-Procedure Disease Score (Time) | Response Duration | Treatment Effect(s) |
|---|---|---|---|---|---|---|---|---|
| CD * | ||||||||
| Distal colitis | 17 | M | 44 | PCDAI 27.5 | superior rectal artery (80 mg) | PCDAI 17.5 (1 week) | 1 month | Resolution of abdominal pain, improvement in hematochezia |
| Pancolitis | 10 | M | 24 | PCDAI 37.5 | superior rectal artery (50 mg), sigmoidal artery (50 mg) | PCDAI 7.5 (4 weeks) | Remains in remission | Resolution of hematochezia, resolution of abdominal pain; transitioned to adalimumab from vedolizumab |
| Intestinal fibrosis; ileal stricture | 19 | M | 57 | PCDAI 20 | SMA: ileocolic branch (30 mg), ileal branch (50 mg) | PCDAI 0 (3 weeks) | Remains in remission | Resolution of abdominal pain, resolution of nausea; successful endoscopic dilation |
| Intestinal fibrosis; ileal stricture | 17 | F | 73 | PCDAI 37.5 | ileocolic artery (50 mg), right colic artery (50 mg) | PCDAI 15 (2 days) | 2 weeks | Resolution of abdominal pain, resolution of vomiting; redeveloped obstruction |
| Intestinal fibrosis; jejunal stricture | 17 | F | 58 | PCDAI 35 | SMA: branch vessels supplying jejunum (300 mg) | Undetermined (4 weeks) | Remains in remission | Resolution of nausea and vomiting, abdominal pain unchanged; successful endoscopic dilation; transitioned to ustekinumab from adalimumab and methotrexate |
| Intestinal fibrosis; duodenal and jejunal strictures | 17 | M | 45 | PCDAI 32.5 | gastroduodenal artery and branches supplying jejunum (270 mg) | PCDAI 30 (2 days) | Transient | Improvement in nausea and pain; unsuccessful endoscopic dilation; underwent bowel resection |
| UC | ||||||||
| Pancolitis | 20 | M | 69 | PUCAI 60 | IMA (100 mg), ileocolic artery (100 mg), right colic artery (100 mg), left colic artery (60 mg), sigmoidal artery (40 mg) | PUCAI 15 (6 days) | >1 month | Improvement in abdominal pain and hematochezia; transitioned to ustekinumab from vedolizumab and infliximab |
| Pancolitis | 22 | F | 55 | PUCAI 50 | sigmoidal artery (125 mg) | PUCAI 50 (2 weeks) | 1 week | Improvement in diarrhea; transitioned to tofacitinib from vedolizumab and adalimumab |
| Pancolitis | 17 | M | 64 | PUCAI 65 | sigmoidal artery, superior rectal artery (450 mg total) | PUCAI 30 (3 days) | Remains in remission | Improvement in diarrhea, improvement in hematochezia; transitioned to tofacitinib from infliximab |
| Patient | Age at CD Diagnosis (y) | Sex | Age at Imaging (y) | PCDAI Score at Imaging | Montreal Classification, Disease Location | Montreal Classification, Disease Behavior | Predominant Areas of Inflammation on MRI |
|---|---|---|---|---|---|---|---|
| 1 | 12 | F | 17 | 37.5 | L4 | B2 | Proximal and distal terminal ileum |
| 2 | 3 | M | 10 | 37.5 | L2 | B2 | Sigmoid and upper rectum |
| 3 | 17 | F | 17 | 35 | L3 | B2 | Terminal ileum |
| 4 | 16 | M | 17 | 27.5 | L2 | B1 | Upper and middle rectum |
| 5 | 14 | M | 19 | 20 | L2 | B2 | Proximal terminal ileum |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levitte, S.; Yarani, R.; Ganguly, A.; Martin, L.; Gubatan, J.; Nadel, H.R.; Franc, B.; Gugig, R.; Syed, A.; Goyal, A.; et al. Case Series of Precision Delivery of Methylprednisolone in Pediatric Inflammatory Bowel Disease: Feasibility, Clinical Outcomes, and Identification of a Vasculitic Transcriptional Program. J. Clin. Med. 2023, 12, 2386. https://doi.org/10.3390/jcm12062386
Levitte S, Yarani R, Ganguly A, Martin L, Gubatan J, Nadel HR, Franc B, Gugig R, Syed A, Goyal A, et al. Case Series of Precision Delivery of Methylprednisolone in Pediatric Inflammatory Bowel Disease: Feasibility, Clinical Outcomes, and Identification of a Vasculitic Transcriptional Program. Journal of Clinical Medicine. 2023; 12(6):2386. https://doi.org/10.3390/jcm12062386
Chicago/Turabian StyleLevitte, Steven, Reza Yarani, Abantika Ganguly, Lynne Martin, John Gubatan, Helen R. Nadel, Benjamin Franc, Roberto Gugig, Ali Syed, Alka Goyal, and et al. 2023. "Case Series of Precision Delivery of Methylprednisolone in Pediatric Inflammatory Bowel Disease: Feasibility, Clinical Outcomes, and Identification of a Vasculitic Transcriptional Program" Journal of Clinical Medicine 12, no. 6: 2386. https://doi.org/10.3390/jcm12062386