
Adropin Predicts Chronic Kidney Disease in Type 2 Diabetes Mellitus Patients with Chronic Heart Failure
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
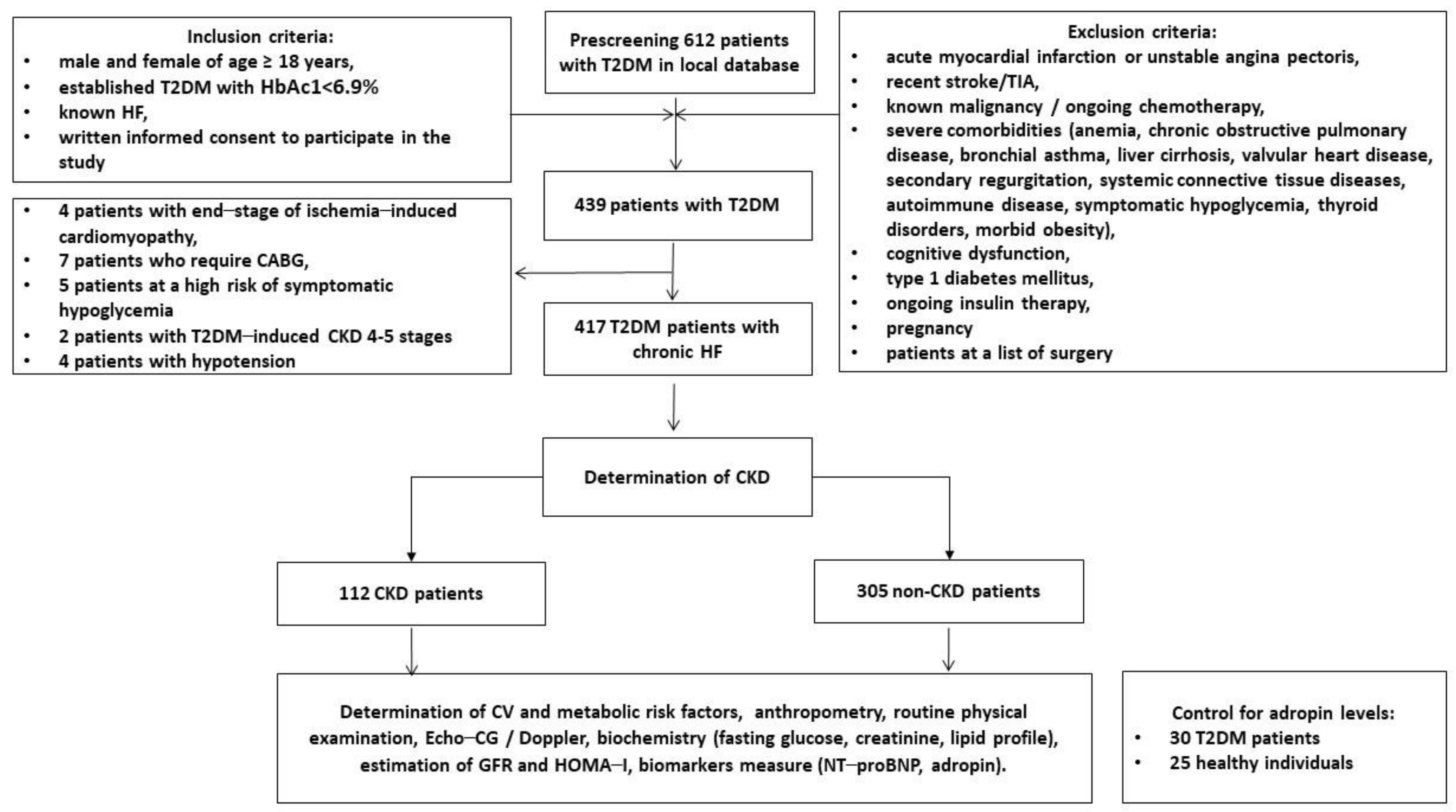
2.1. Research Object and Patient Characteristics
2.2. Determination of Anthropometric Parameters, Co-Morbidities, and Concomitant Diseases
2.3. Hemodynamic Features
2.4. Blood Sampling and Determination of Glomerular Filtration Rate and Insulin Resistance
2.5. Biomarker Determination
2.6. Statistics
3. Results
3.1. General Characteristics of the Patients
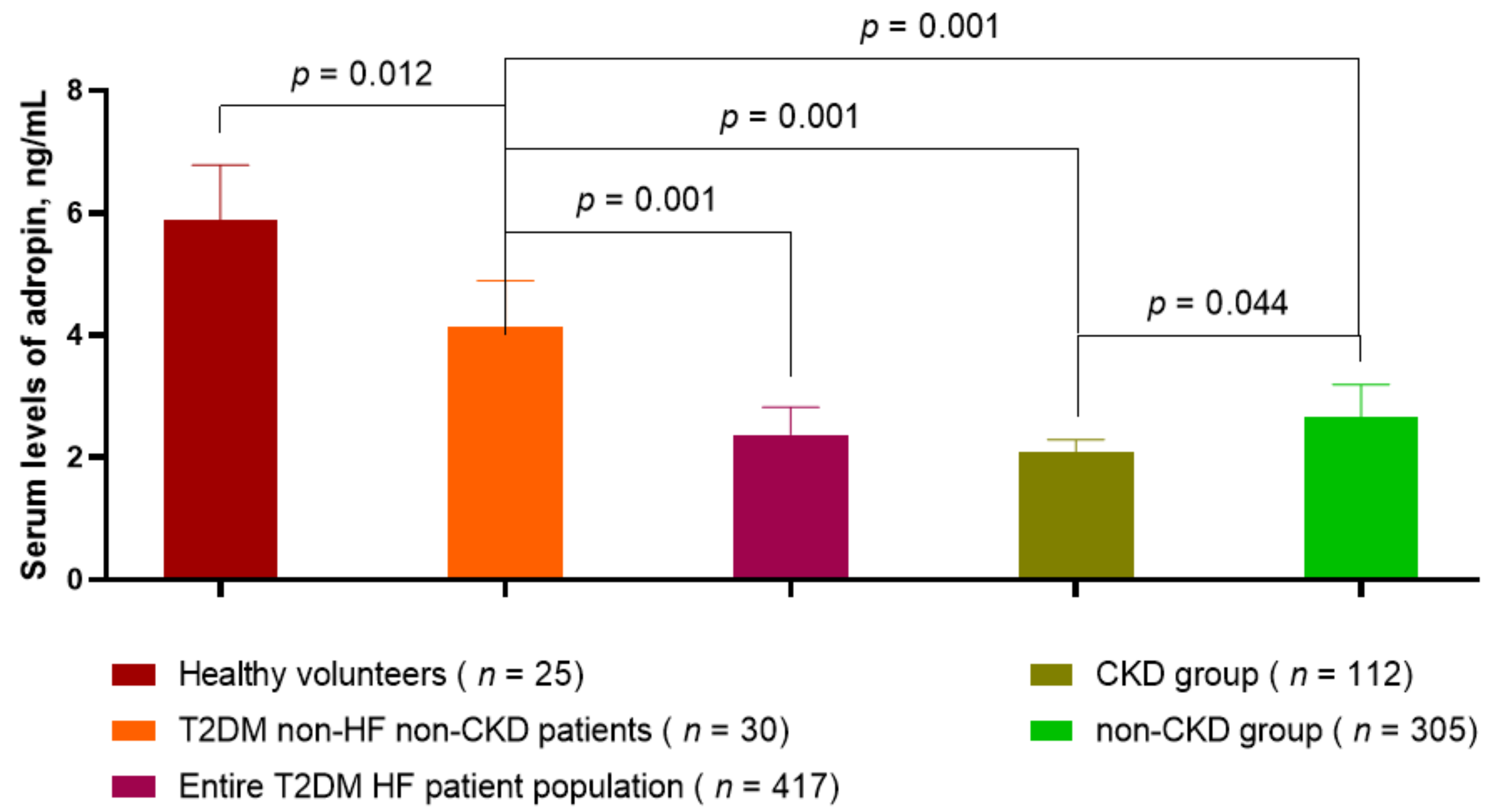
3.2. Circulating Levels of Adropin in T2DM HF Patients with and without CKD Compared with Healthy Volunteers and Non-HF/Non-CKD Diabetics
3.3. Spearman’s Correlation between Circulating Levels of Myokines and Other Parameters
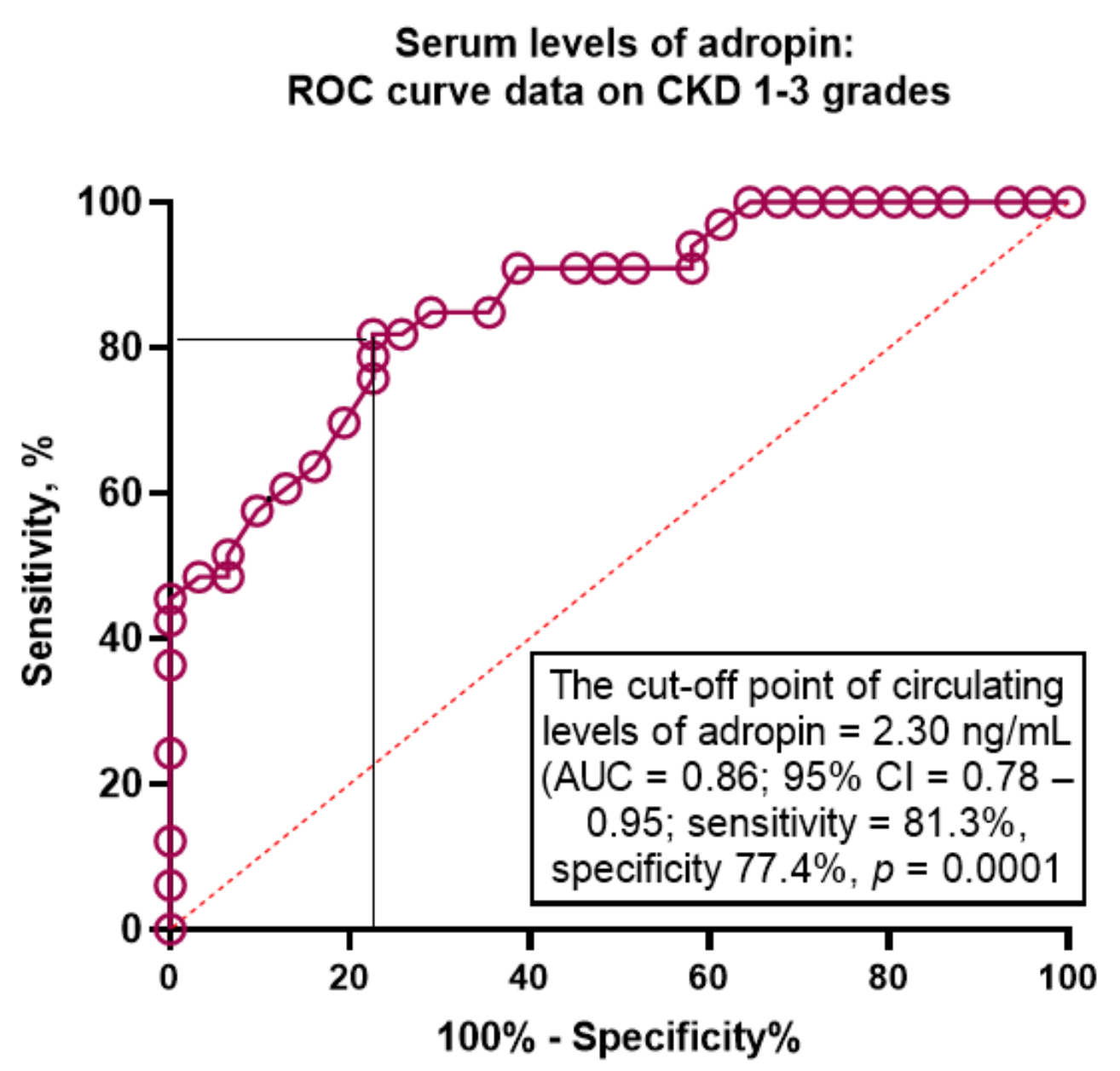
3.4. ROC Curve Analysis of the Predictive Value of Adropin for CKD in T2DM Patients with HF
3.5. Predictive Models for CKD in T2DM Patients with HF: Univariate and Multivariate Logistic Regression Analysis Adjusted to Albuminuria/Proteinuria
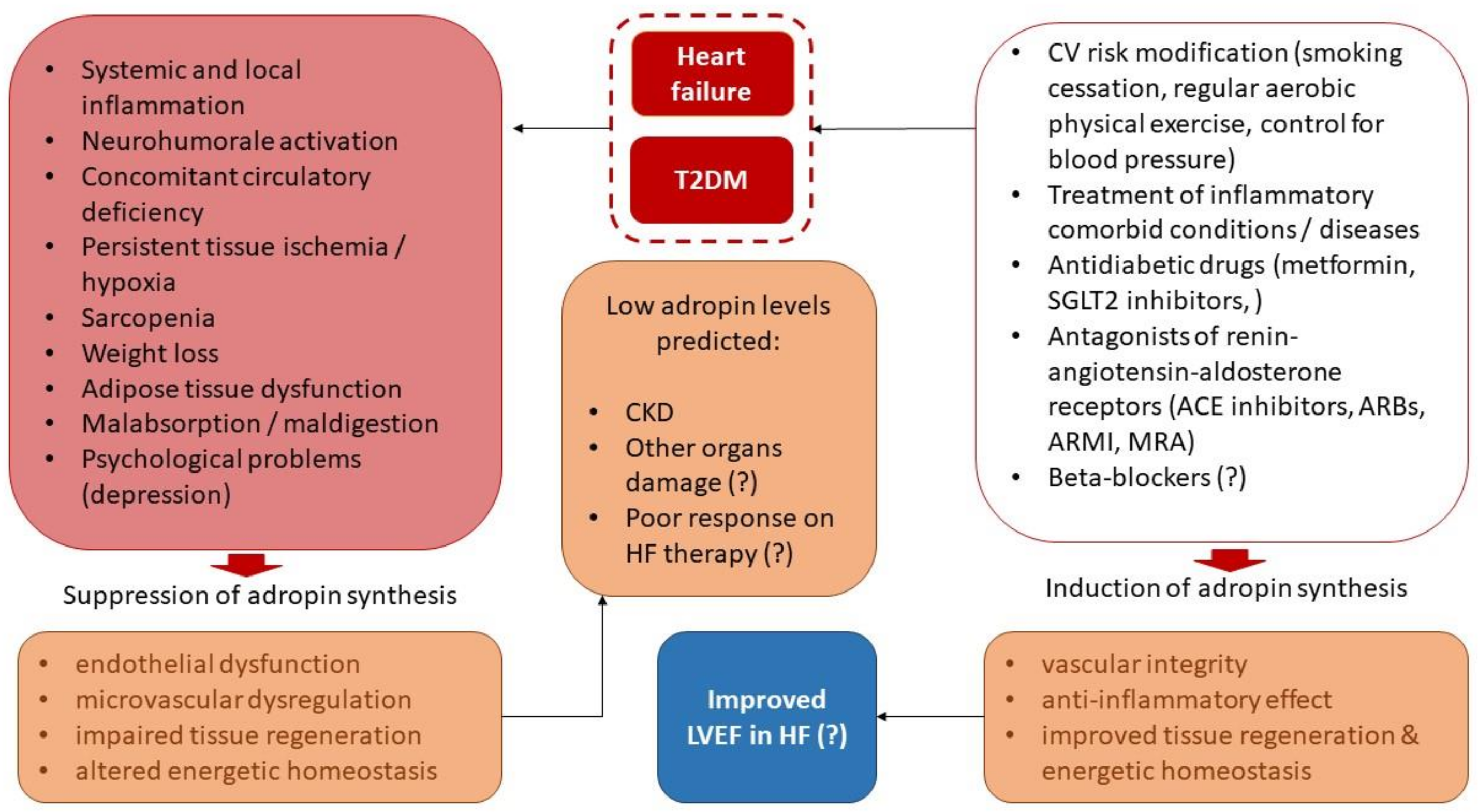
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haynes, R.; Zhu, D.; Judge, P.K.; Herrington, W.G.; Kalra, P.A.; Baigent, C. Chronic kidney disease, heart failure and neprilysin inhibition. Nephrol Dial. Transpl. 2020, 35, 558–564. [Google Scholar] [CrossRef] [Green Version]
- Beldhuis, I.E.; Lam, C.S.; Testani, J.M.; Voors, A.A.; Van Spall, H.G.; ter Maaten, J.M.; Damman, K. Evidence-Based Medical Therapy in Patients with Heart Failure With Reduced Ejection Fraction and Chronic Kidney Disease. Circulation 2022, 145, 693–712. [Google Scholar] [CrossRef]
- Tuegel, C.; Bansal, N. Heart failure in patients with kidney disease. Heart 2017, 103, 1848–1853. [Google Scholar] [CrossRef]
- Mitsas, A.C.; Elzawawi, M.; Mavrogeni, S.; Boekels, M.; Khan, A.; Eldawy, M.; Stamatakis, I.; Kouris, D.; Daboul, B.; Gunkel, O.; et al. Heart Failure and Cardiorenal Syndrome: A Narrative Review on Pathophysiology, Diagnostic and Therapeutic Regimens-From a Cardiologist’s View. J. Clin. Med. 2022, 11, 7041. [Google Scholar] [CrossRef]
- Smith, D.H.; Thorp, M.L.; Gurwitz, J.H.; McManus, D.D.; Goldberg, R.J.; Allen, L.A.; Hsu, G.; Sung, S.H.; Magid, D.J.; Go, A.S. Chronic kidney disease and outcomes in heart failure with preserved versus reduced ejection fraction: The Cardiovascular Research Network PRESERVE Study. Circ. Cardiovasc. Qual. Outcomes 2013, 6, 333–342. [Google Scholar] [CrossRef] [Green Version]
- House, A.A.; Wanner, C.; Sarnak, M.J.; Piña, I.L.; McIntyre, C.W.; Komenda, P.; Kasiske, B.L.; Deswal, A.; Defilippi, C.R.; Cleland, J.G.F.; et al. Conference Participants. Heart failure in chronic kidney disease: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019, 95, 1304–1317. [Google Scholar] [CrossRef] [Green Version]
- Schefold, J.C.; Filippatos, G.; Hasenfuss, G.; Anker, S.D.; von Haehling, S. Heart failure and kidney dysfunction: Epidemiology, mechanisms and management. Nat. Rev. Nephrol. 2016, 12, 610–623. [Google Scholar] [CrossRef]
- Ceriello, A.; Catrinoiu, D.; Chandramouli, C.; Cosentino, F.; Dombrowsky, A.C.; Itzhak, B.; Nebojsa, M.L.; Francesco, P.; Schnell, O.; et al.; D&CVD EASD Study Group Heart failure in type 2 diabetes: Current perspectives on screening, diagnosis and management. Cardiovasc. Diabetol. 2021, 20, 218. [Google Scholar] [CrossRef]
- Han, X.; Zhang, S.; Chen, Z.; Adhikari, B.K.; Zhang, Y.; Zhang, J.; Sun, J.; Wang, Y. Cardiac biomarkers of heart failure in chronic kidney disease. Clin. Chim. Acta. 2020, 510, 298–310. [Google Scholar] [CrossRef]
- Maltês, S.; Cunha, G.J.; Rocha, B.M.; Presume, J.; Guerreiro, R.; Henriques, C.; Rodrigues, C.; Araújo, I.; Fonseca, C. Dapagliflozin in a Real-World Chronic Heart Failure Population: How Many Are Actually Eligible? Cardiology 2021, 146, 201–206. [Google Scholar] [CrossRef]
- Butt, J.H.; Adamson, C.; Docherty, K.F.; de Boer, R.A.; Petrie, M.C.; Inzucchi, S.E.; Kosiborod, M.N.; Langkilde, A.M.; Lindholm, D.; Martinez, F.A.; et al. Efficacy and Safety of Dapagliflozin in Heart Failure with Reduced Ejection Fraction According to N-Terminal Pro-B-Type Natriuretic Peptide: Insights From the DAPA-HF Trial. Circ. Heart Fail. 2021, 14, e008837. [Google Scholar] [CrossRef]
- Berezin, A.E.; Berezin, A.A. Biomarkers in heart failure: From research to clinical practice. Ann. Lab. Med. 2023, 43, 225–236. [Google Scholar] [CrossRef]
- Mushala, B.A.S.; Scott, I. Adropin: A hepatokine modulator of vascular function and cardiac fuel metabolism. Am. J. Physiol. Heart Circ. Physiol. 2021, 320, H238–H244. [Google Scholar] [CrossRef]
- Stein, L.M.; Yosten, G.L.; Samson, W.K. Adropin acts in brain to inhibit water drinking: Potential interaction with the orphan G protein-coupled receptor, GPR19. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2016, 310, R476–R480. [Google Scholar] [CrossRef] [Green Version]
- Thapa, D.; Stoner, M.W.; Zhang, M.; Xie, B.; Manning, J.; Guimaraes, D.; Shiva, S.; Jurczak, M.J.; Scott, I. Adropin regulates pyruvate dehydrogenase in cardiac cells via a novel GPCR-MAPK-PDK4 signaling pathway. Redox Biol. 2018, 18, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Lovren, F.; Pan, Y.; Quan, A.; Singh, K.K.; Shukla, P.C.; Gupta, M.; Al-Omran, M.; Teoh, H.; Verma, S. Adropin is a novel regulator of endothelial function. Circulation 2010, 122 (Suppl. 11), S185–S192. [Google Scholar] [CrossRef] [Green Version]
- Ali, I.I.; D’Souza, C.; Singh, J.; Adeghate, E. Adropin’s Role in Energy Homeostasis and Metabolic Disorders. Int. J. Mol. Sci. 2022, 23, 8318. [Google Scholar] [CrossRef] [PubMed]
- Ghoshal, S.; Stevens, J.R.; Billon, C.; Girardet, C.; Sitaula, S.; Leon, A.S.; Rao, D.; Skinner, J.S.; Rankinen, T.; Bouchard, C.; et al. Adropin: An endocrine link between the biological clock and cholesterol homeostasis. Mol. Metab. 2018, 8, 51–64. [Google Scholar] [CrossRef] [PubMed]
- Jasaszwili, M.; Billert, M.; Strowski, M.Z.; Nowak, K.W.; Skrzypski, M. Adropin as A Fat-Burning Hormone with Multiple Functions-Review of a Decade of Research. Molecules 2020, 25, 549. [Google Scholar] [CrossRef] [Green Version]
- Skrzypski, M.; Kołodziejski, P.A.; Pruszyńska-Oszmałek, E.; Wojciechowicz, T.; Janicka, P.; Krążek, M.; Małek, E.; Strowski, M.Z.; Nowak, K.W. Daily Treatment of Mice with Type 2 Diabetes with Adropin for Four Weeks Improves Glucolipid Profile, Reduces Hepatic Lipid Content and Restores Elevated Hepatic Enzymes in Serum. Int. J. Mol. Sci. 2022, 23, 9807. [Google Scholar] [CrossRef]
- Jurrissen, T.J.; Ramirez-Perez, F.I.; Cabral-Amador, F.J.; Soares, R.N.; Pettit-Mee, R.J.; Betancourt-Cortes, E.E.; McMillan, N.J.; Sharma, N.; Rocha, H.N.M.; Fujie, S.; et al. Role of adropin in arterial stiffening associated with obesity and type 2 diabetes. Am. J. Physiol. Heart Circ. Physiol. 2022, 323, H879–H891. [Google Scholar] [CrossRef]
- Li, B.; Tian, X.; Guo, S.; Zhang, M.; Li, J.; Zhai, N.; Wang, H.; Zhang, Y. Pentraxin-3 and adropin as inflammatory markers of early renal damage in type 2 diabetes patients. Int. Urol. Nephrol. 2020, 52, 2145–2152. [Google Scholar] [CrossRef]
- Es-Haghi, A.; Al-Abyadh, T.; Mehrad-Majd, H. The Clinical Value of Serum Adropin Level in Early Detection of Diabetic Nephropathy. Kidney Blood Press Res. 2021, 46, 734–740. [Google Scholar] [CrossRef]
- Zang, H.; Jiang, F.; Cheng, X.; Xu, H.; Hu, X. Serum adropin levels are decreased in Chinese type 2 diabetic patients and negatively correlated with body mass index. Endocr. J. 2018, 65, 685–691. [Google Scholar] [CrossRef] [Green Version]
- Wei, W.; Liu, H.; Qiu, X.; Zhang, J.; Huang, J.; Chen, H.; Qiu, S.; Lin, R.; Li, S.; Tu, M. The association between serum adropin and carotid atherosclerosis in patients with type 2 diabetes mellitus: A cross-sectional study. Diabetol. Metab. Syndr. 2022, 14, 27. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; An, Y.; Zhang, L.; Zhang, Y.; Wang, G.; Liu, J. Regulation of Adropin by Sitagliptin monotherapy in participants with newly diagnosed type 2 Diabetes. BMC Endocr. Disord. 2022, 22, 306. [Google Scholar] [CrossRef] [PubMed]
- Berezin, A.A.; Obradovic, Z.; Novikov, E.V.; Boxhammer, E.; Lichtenauer, M.; Berezin, A.E. Interplay between Myokine Profile and Glycemic Control in Type 2 Diabetes Mellitus Patients with Heart Failure. Diagnostics 2022, 12, 2940. [Google Scholar] [CrossRef]
- Davoodi, M.; Hesamabadi, B.K.; Ariabood, E.; Izadi, M.R.; Afousi, A.G.; Bigi, M.A.B.; Asvadi-Fard, M.; Gaeini, A.A. Improved blood pressure and flow-mediated dilatation via increased plasma adropin and nitrate/nitrite induced by high-intensity interval training in patients with type 2 diabetes. Exp. Physiol. 2022, 107, 813–824. [Google Scholar] [CrossRef] [PubMed]
- Lian, W.; Gu, X.; Qin, Y.; Zheng, X. Elevated plasma levels of adropin in heart failure patients. Intern. Med. 2011, 50, 1523–1527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, W.; Qian, L.; Yuan, X.; Lu, Y. Combined effects of hydralazine and nitrate on serum biochemistry and left ventricular remodeling in chronic heart failure patients. Pak. J. Pharm. Sci. 2021, 34, 381–386. [Google Scholar] [PubMed]
- Kalkan, A.K.; Cakmak, H.A.; Erturk, M.; Kalkan, K.E.; Uzun, F.; Tasbulak, O.; Diker, V.O.; Aydin, S.; Celik, A. Adropin and Irisin in Patients with Cardiac Cachexia. Arq. Bras. Cardiol. 2018, 111, 39–47. [Google Scholar] [CrossRef]
- Yosaee, S.; Soltani, S.; Sekhavati, E.; Jazayeri, S. Adropin- A Novel Biomarker of Heart Disease: A Systematic Review Article. Iran. J. Public Health 2016, 45, 1568–1576. [Google Scholar]
- de Boer, I.H.; Khunti, K.; Sadusky, T.; Tuttle, K.R.; Neumiller, J.J.; Rhee, C.M.; Rosas, S.E.; Rossing, P.; Bakris, G. Diabetes Management in Chronic Kidney Disease: A Consensus Report by the American Diabetes Association (ADA) and Kidney Disease: Improving Global Outcomes (KDIGO). Diabetes Care 2022, 45, dci220027. [Google Scholar] [CrossRef] [PubMed]
- Toto, R.D. Microalbuminuria: Definition, detection, and clinical significance. J. Clin. Hypertens. 2004, 6 (Suppl. 3), 2–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44 (Suppl. 1), S15–S33. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. ESC Scientific Document Group. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [Green Version]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference , B.A.; et al. ESC Scientific Document Group. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [Green Version]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott , E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [Green Version]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corra, U.; Cosyns, B.; Deaton , C.; et al. ESC Scientific Document Group. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Yamamoto, J.; Wakami, K.; Muto, K.; Kikuchi, S.; Goto, T.; Fukuta, H.; Seo, Y.; Ohte, N. Verification of Echocardiographic Assessment of Left Ventricular Diastolic Dysfunction in Patients with Preserved Left Ventricular Ejection Fraction Using the American Society of Echocardiography and European Association of Cardiovascular Imaging 2016 Recommendations. Circ. Rep. 2019, 1, 525–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J.-Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration); et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Castiglione, V.; Aimo, A.; Vergaro, G.; Saccaro, L.; Passino, C.; Emdin, M. Biomarkers for the diagnosis and management of heart failure. Heart Fail Rev. 2022, 27, 625–643. [Google Scholar] [CrossRef] [PubMed]
- Berezin, A.E. Circulating Biomarkers in Heart Failure. Adv. Exp. Med. Biol. 2018, 1067, 89–108. [Google Scholar] [CrossRef]
- Niepolski, L.; Grzegorzewska, A.E. Salusins and adropin: New peptides potentially involved in lipid metabolism and atherosclerosis. Adv. Med. Sci. 2016, 61, 282–287. [Google Scholar] [CrossRef]
- Fujie, S.; Hasegawa, N.; Horii, N.; Uchida, M.; Sanada, K.; Hamaoka, T.; Padilla, J.; Martinez-Lemus, L.A.; Maeda, S.; Iemitsu, M. Aerobic Exercise Restores Aging-Associated Reductions in Arterial Adropin Levels and Improves Adropin-Induced Nitric Oxide-Dependent Vasorelaxation. J. Am. Heart Assoc. 2021, 10, e020641. [Google Scholar] [CrossRef]
- Yazgan, B.; Avcı, F.; Memi, G.; Tastekin, E. Inflammatory response and matrix metalloproteinases in chronic kidney failure: Modulation by adropin and spexin. Exp. Biol. Med. 2021, 246, 1917–1927. [Google Scholar] [CrossRef]
- Memi, G.; Yazgan, B. Adropin and spexin hormones regulate the systemic inflammation in adenine-induced chronic kidney failure in rat. Chin. J. Physiol. 2021, 64, 194–201. [Google Scholar] [CrossRef]
- Bozic, J.; Kumric, M.; Kurir, T.T.; Males, I.; Borovac, J.A.; Martinovic, D.; Vilovic, M. Role of Adropin in Cardiometabolic Disorders: From Pathophysiological Mechanisms to Therapeutic Target. Biomedicines 2021, 9, 1407. [Google Scholar] [CrossRef]
- Jensen-Cody, S.O.; Potthoff, M.J. 52. Jensen-Cody SO, Potthoff MJ. Hepatokines and metabolism: Deciphering communication from the liver. Mol. Metab. 2021, 44, 101138. [Google Scholar] [CrossRef]
- Yang, C.; DeMars, K.M.; Hawkins, K.E.; Candelario-Jalil, E. Adropin reduces paracellular permeability of rat brain endothelial cells exposed to ischemia-like conditions. Peptides 2016, 81, 29–37. [Google Scholar] [CrossRef]
- Dodd, W.S.; Patel, D.; Lucke-Wold, B.; Hosaka, K.; Chalouhi, N.; Hoh, B.L. Adropin decreases endothelial monolayer permeability after cell-free hemoglobin exposure and reduces MCP-1-induced macrophage transmigration. Biochem. Biophys. Res. Commun. 2021, 582, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Yamashita, T.; Shirai, R.; Shibata, K.; Okano, T.; Yamaguchi, M.; Mori, Y.; Hirano, T.; Watanabe, T. Adropin Contributes to Anti-Atherosclerosis by Suppressing Monocyte-Endothelial Cell Adhesion and Smooth Muscle Cell Proliferation. Int. J. Mol. Sci. 2018, 19, 1293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Jin, F.; Wang, P.; Hou, S.; Jin, T.; Chang, X.; Zhao, L. Adropin Inhibits Vascular Smooth Muscle Cell Osteogenic Differentiation to Alleviate Vascular Calcification via the JAK2/STAT3 Signaling Pathway. BioMed Res. Int. 2022, 2022, 9122264. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Wang, Z.; He, Y.; Chen, T.; Zhang, Y.; Yuan, X.; Li, P. Adropin Improves Radiation-Induced Myocardial Injury via VEGFR2/PI3K/Akt Pathway. Oxid. Med. Cell Longev. 2022, 2022, 8230214. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Fang, J.; Chen, L.; Zhao, Z.; Luo, Y.; Lin, C.; Fan, L. Low serum adropin is associated with coronary atherosclerosis in type 2 diabetic and non-diabetic patients. Clin. Chem. Lab. Med. 2014, 52, 751–758. [Google Scholar] [CrossRef]
- Gulen, B.; Eken, C.; Kucukdagli, O.T.; Serinken, M.; Kocyigit, A.; Kılıc, E.; Uyarel, H. Adropin levels and target organ damage secondary to high blood pressure in the ED. Am. J. Emerg. Med. 2016, 34, 2061–2064. [Google Scholar] [CrossRef]
- Gu, X.; Li, H.; Zhu, X.; Gu, H.; Chen, J.; Wang, L.; Harding, P.; Xu, W. Inverse Correlation Between Plasma Adropin and ET-1 Levels in Essential Hypertension: A Cross-Sectional Study. Medicine 2015, 94, e1712. [Google Scholar] [CrossRef]
- Hu, W.; Chen, L. Association of Serum Adropin Concentrations with Diabetic Nephropathy. Mediators. Inflamm. 2016, 2016, 6038261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, N.; Xie, G.; Zhou, B.; Qu, A.; Meng, H.; Liu, J.; Wang, G. Serum Adropin as a Potential Biomarker for Predicting the Development of Type 2 Diabetes Mellitus in Individuals witah Metabolic Dysfunction-Associated Fatty Liver Disease. Front. Physiol. 2021, 12, 696163. [Google Scholar] [CrossRef]
- Beigi, A.; Shirzad, N.; Nikpour, F.; Nasli Esfahani, E.; Emamgholipour, S.; Bandarian, F. Association between serum adropin levels and gestational diabetes mellitus; a case-control study. Gynecol. Endocrinol. 2015, 31, 939–941. [Google Scholar] [CrossRef]
- Yu, H.Y.; Zhao, P.; Wu, M.C.; Liu, J.; Yin, W. Serum adropin levels are decreased in patients with acute myocardial infarction. Regul. Pept. 2014, 190–191, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.P.; Xu, W.T.; Wang, L.; You, T.; Chan, S.P.; Zhao, X.; Yang, X.J. Serum adropin level in patients with stable coronary artery disease. Heart Lung Circ. 2015, 24, 975–979. [Google Scholar] [CrossRef] [PubMed]
- Berezin, A.A.; Obradovic, Z.; Fushtey, I.M.; Berezina, T.A.; Novikov, E.V.; Schmidbauer, L.; Lichtenauer, M.; Berezin, A.E. The Impact of SGLT2 Inhibitor Dapagliflozin on Adropin Serum Levels in Men and Women with Type 2 Diabetes Mellitus and Chronic Heart Failure. Biomedicines 2023, 11, 457. [Google Scholar] [CrossRef]
- Czerwińska, M.; Czarzasta, K.; Cudnoch-Jędrzejewska, A. New Peptides as Potential Players in the Crosstalk Between the Brain and Obesity, Metabolic and Cardiovascular Diseases. Front. Physiol. 2021, 12, 692642. [Google Scholar] [CrossRef]
- Verma, S.K.; Molitoris, B.A. Renal endothelial injury and microvascular dysfunction in acute kidney injury. Semin. Nephrol. 2015, 35, 96–107. [Google Scholar] [CrossRef] [Green Version]
- Berezin, A.E.; Berezin, A.A.; Lichtenauer, M. Myokines and Heart Failure: Challenging Role in Adverse Cardiac Remodeling, Myopathy, and Clinical Outcomes. Dis. Markers. 2021, 2021, 6644631. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Healthy Volunteers (n = 25) | T2DM Non-HF Patients without CKD (n = 30) | T2DM HF Patients | |||
|---|---|---|---|---|---|---|
| Entire Patient Cohort (n = 417) | CKD Patients (n = 112) | Non-CKD Patients (n = 305) | p Value | |||
| Demographics and anthropomorphic parameters | ||||||
| Age, year | 51 (47–55) | 52 (47–55) | 53 (41–64) | 56 (44–67) | 52 (40–65) | 0.12 |
| Male/female n (%) | 14 (56.0)/11 (44.0) | 17 (57.0)/13 (43.0) | 231 (55.4)/186 (44.6) | 62 (55.3)/50 (44.7) | 169 (55.4)/136 (44.6) | 0.90 |
| BMI, kg/m2 | 23.9 ± 2.7 | 24.1 ± 2.3 | 25.8 ± 2.8 | 25.0 ± 3.2 | 26.2 ± 2.3 | 0.66 |
| Waist circumference, cm | 86.1 ± 3.6 | 86.1 ± 3.6 | 95.1 ± 3.2 ** | 94.7 ± 3.0 | 96.2 ± 4.1 | 0.58 |
| WHR, units | 0.73 ± 0.04 | 0.84 ± 0.05 * | 0.85 ± 0.05 | 0.84 ± 0.06 | 0.87 ± 0.09 | 0.80 |
| Concomitant diseases and risk factors | ||||||
| Dyslipidaemia, n (%) | - | 24 (80.0) | 346 (83.0) | 96 (85.7) | 250 (81.9) | 0.14 |
| Hypertension, n (%) | - | 13 (43.3) | 352 (84.4) ** | 105 (93.8) | 247 (81.0) | 0.04 |
| Stable CAD, n (%) | - | - | 141 (33.8) ** | 43 (38.4) | 98 (32.1) | 0.05 |
| Smoking, n (%) | 4 (16) | 11 (36.7) * | 168 (40.3) | 41 (36.6) | 127 (41.6) | 0.06 |
| Abdominal obesity, n (%) | - | 9 (30.0) * | 179 (42.9) ** | 45 (40.2) | 134 (43.9) | 0.22 |
| LV hypertrophy, n (%) | - | 7 (23.3) * | 334 (80.1) ** | 93 (83.1) | 241 (79.0) | 0.042 |
| AF, n (%) | - | - | 57 (13.7) ** | 21 (18.7) | 36 (11.8) | 0.04 |
| Albuminuria, n (%) | - | - | 75 (18.0) ** | 47 (42.0) | 28 (9.2) | 0.001 |
| Proteinuria, n (%) | - | - | 16 (3.8) ** | 16 (9.8) | - | 0.001 |
| HF phenotypes and functional classification | ||||||
| HFpEF, n (%) | - | - | 132 (31.7) ** | 32 (28.6) | 100 (32.3) | 0.10 |
| HFmrEF, n (%) | - | - | 140 (33.6) ** | 39 (34.8) | 101 (33.1) | 0.14 |
| HFrEF, n (%) | - | - | 145 (34.8) ** | 41 (36.6) | 103 (33.8) | 0.12 |
| I/II HF NYHA class, n (%) | - | - | 282 (67.6) ** | 68 (60.7) | 214 (70.1) | 0.04 |
| III HF NYHA class, n (%) | - | - | 135 (32.4) ** | 44 (39.3) | 91 (29.9) | 0.04 |
| Haemodynamic features | ||||||
| SBP, mm Hg | 124 ± 5 | 129 ± 7 | 132 ± 7 | 135 ± 6 | 130 ± 6 | 0.22 |
| DBP, mm Hg | 73 ± 4 | 76 ± 5 | 78 ± 5 | 79 ± 4 | 76 ± 5 | 0.20 |
| LVEDV, mL | 141 (122–155) | 144 (126–158) | 162 (154–170) ** | 165 (157–174) | 160 (153–168) | 0.05 |
| LVESV, mL | 52 (44–61) | 55 (47–64) | 86 (80–93) ** | 91 (82–97) | 85 (80–91) | 0.05 |
| LVEF, % | 63 (59–68) | 62 (56–67) | 46 (37–55) ** | 45 (35–56) | 46 (37–57) | 0.64 |
| LVMMI, g/m2 | 102 ± 4 | 108 ± 5 | 154 ± 5 ** | 156 ± 4 | 151 ± 7 | 0.48 |
| LAVI, mL/m2 | 31 (29–34) | 34 (30–36) | 43 (37–52) ** | 45 (38–50) | 42 (35–50) | 0.14 |
| E/e’, unit | 6.45 ± 0.3 | 6.51 ± 0.4 | 13.5 ± 0.3 ** | 15.1 ± 0.6 | 11.4 ± 0.5 | 0.001 |
| TAPSE, mm | 25 (21–28) | 24 (20–28) | 21 (18–25) | 19 (16–23) | 22 (20–26) | 0.052 |
| basal RV diameter, mm | 24 (12–36) | 26 (13–40) | 28 (15–43) | 29 (17–45) | 25 (15–42) | 0.050 |
| Biomarkers | ||||||
| eGFR, mL/min/1.73 m2 | 109 ± 6 | 109 ± 7 | 75 ± 18 ** | 63 ± 12 | 96 ± 6 | 0.02 |
| HOMA-IR | 4.32 ± 0.7 | 5.95 ± 0.9 * | 7.95 ± 2.3 | 8.60 ± 2.0 | 6.90 ± 2.2 | 0.40 |
| Fasting glucose, mmol/L | 5.1 ± 0.7 | 6.08 ± 0.8 * | 6.12 ± 1.3 | 6.20 ± 1.5 | 5.80 ± 1.6 | 0.80 |
| HbA1c, % | 5.20 ± 0.04 | 6.40 ± 0.05 * | 6.59 ± 0.02 | 6.71 ± 0.09 | 6.50 ± 0.03 | 0.68 |
| Creatinine, µmol/L | 69.5 ± 7.0 | 77.4 ± 8.0 | 108.6 ± 8.5 ** | 119.2 ± 5.5 | 96.3 ± 4.7 | 0.01 |
| TC, mmol/L | 4.93 ± 0.50 | 5.48 ± 0.40 * | 6.43 ± 0.60 ** | 6.50 ± 0.50 | 6.40 ± 0.40 | 0.78 |
| HDL-C, mmol/L | 1.04 ± 0.12 | 1.01 ± 0.15 | 0.97 ± 0.17 | 0.96 ± 0.16 | 0.99 ± 0.19 | 0.80 |
| LDL-C, mmol/L | 2.88 ± 0.13 | 3.10 ± 0.14 * | 4.38 ± 0.10 ** | 4.43 ± 0.13 | 4.30 ± 0.14 | 0.82 |
| TG, mmol/L | 1.70 ± 0.10 | 1.80 ± 0.12 | 2.21 ± 0.17 ** | 2.21 ± 0.14 | 2.22 ± 0.16 | 0.88 |
| hs-CRP, mg/L | 0.75 (0.32–1.10) | 4.03 (2.90–5.36) * | 7.12 (4.33–10.51) | 8.45 (5.12–11.30) | 6.24 (4.07–8.87) | 0.05 |
| NT-proBNP, pmol/mL | 48 (10–95) | 56 (0–102) | 2615 (1380–3750) ** | 2844 (1560–3810) | 2598 (1280–3880) | 0.46 |
| Concomitant medications | ||||||
| ACEI, n (%) | - | 13 (43.3) * | 198 (47.5) | 52 (46.4) | 146 (47.9) | 0.78 |
| ARB, n (%) | - | - | 67 (16.1) ** | 27 (24.1) | 40 (13.1) | 0.02 |
| ARNI, n (%) | - | - | 165 (39.6) ** | 41 (36.6) | 124 (40.6) | 0.11 |
| Beta-blocker, n (%) | - | - | 372 (89.2) ** | 103 (92.0) | 269 (88.2) | 0.44 |
| Ivabradine, n (%) | - | - | 59 (14.1) ** | 12 (10.7) | 47 (15.4) | 0.05 |
| Calcium channel blocker, n (%) | - | 5 (16.7) * | 75 (18.0) | 22 (19.6) | 53 (17.3) | 0.06 |
| MRA, n (%) | - | - | 283 (67.8) ** | 46 (41.1) | 237 (77.7) | 0.01 |
| SGLT2 inhibitor, n (%) | - | 12 (40.0) * | 362 (86.8) ** | 92 (82.1) | 270 (88.5) | 0.20 |
| Loop diuretic, n (%) | - | - | 358 (85.9) ** | 110 (98.2) | 248 (81.3) | 0.04 |
| Antiplatelet, n (%) | - | - | 367 (88.0) ** | 98 (87.5) | 269 (88.2) | 0.86 |
| Anticoagulant, n (%) | - | - | 57 (13.7) ** | 21 (18.7) | 36 (11.8) | 0.04 |
| Metformin, n (%) | - | 30 (100) * | 387 (92.8) | 86 (76.8) | 301 (98.7) | 0.04 |
| Statins, n (%) | - | 24 (80.0) * | 408 (97.8) | 103 (92.0) | 305 (100) | 0.05 |
| Variables | Depending Variables: CKD 1–3 Grades | |||||
|---|---|---|---|---|---|---|
| Univariate Log Regression | Multivariate Log Regression | |||||
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Adropin < 2.30 ng/mL vs. ≥2.30 ng/mL | 1.84 | 1.34–2.41 | 0.001 | 1.55 | 1.38–1.86 | 0.001 |
| LVH vs. non LVH | 1.10 | 1.07–1.15 | 0.022 | 1.06 | 1.00–1.13 | 0.16 |
| BMI < 25.8 кг/м2 vs. ≥25.8 кг/м2 | 1.06 | 1.00–1.13 | 0.052 | - | ||
| Age ≥ 53 years vs. <53 years | 1.05 | 1.01–1.12 | 0.044 | 1.03 | 1.00–1.05 | 0.46 |
| Smoking vs. non-smoking | 1.02 | 0.93–1.12 | 0.88 | - | ||
| E/e’ > 13.5 vs. ≥13.5 units | 1.08 | 1.03–1.14 | 0.010 | 1.04 | 1.00–1.09 | 0.44 |
| LAVI ≥ 43 mL/m2 vs. <43 mL/m2 | 1.06 | 1.01–1.10 | 0.001 | 1.05 | 0.97–1.09 | 0.62 |
| Use of SGLT2i vs. unuse of SGLT2i | 0.92 | 0.87–1.01 | 0.72 | - | ||
| AF vs. non-AF | 1.10 | 0.88–1.24 | 0.86 | - | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berezina, T.A.; Obradovic, Z.; Boxhammer, E.; Berezin, A.A.; Lichtenauer, M.; Berezin, A.E. Adropin Predicts Chronic Kidney Disease in Type 2 Diabetes Mellitus Patients with Chronic Heart Failure. J. Clin. Med. 2023, 12, 2231. https://doi.org/10.3390/jcm12062231
Berezina TA, Obradovic Z, Boxhammer E, Berezin AA, Lichtenauer M, Berezin AE. Adropin Predicts Chronic Kidney Disease in Type 2 Diabetes Mellitus Patients with Chronic Heart Failure. Journal of Clinical Medicine. 2023; 12(6):2231. https://doi.org/10.3390/jcm12062231
Chicago/Turabian StyleBerezina, Tetiana A., Zeljko Obradovic, Elke Boxhammer, Alexander A. Berezin, Michael Lichtenauer, and Alexander E. Berezin. 2023. "Adropin Predicts Chronic Kidney Disease in Type 2 Diabetes Mellitus Patients with Chronic Heart Failure" Journal of Clinical Medicine 12, no. 6: 2231. https://doi.org/10.3390/jcm12062231