
Serum sCD40L and IL-31 in Association with Early Phase of IgA Nephropathy
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Ethical Issue
2.3. Multiplex Assay for Cytokines
2.4. Serum Gd-IgA1 Measurement
2.5. Histological Assessment
2.6. Statistical Analyses
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wyatt, R.J.; Julian, B.A. IgA nephropathy. N. Engl. J. Med. 2013, 368, 2402–2414. [Google Scholar] [CrossRef] [Green Version]
- Kiryluk, K.; Novak, J. The genetics and immunobiology of IgA nephropathy. J. Clin. Investig. 2014, 124, 2325–2332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radford, M.G.; Donadio, J.V.; Bergstralh, E.J.; Grande, J.P. Predicting renal outcome in IgA nephropathy. J. Am. Soc. Nephrol. 1997, 8, 199–207. [Google Scholar] [CrossRef] [PubMed]
- A Working Group of the International IgA Nephropathy Network and the Renal Pathology Society; Cattran, D.C.; Coppo, R.; Cook, H.T.; Feehally, J.; Roberts, I.S.; Troyanov, S.; Alpers, C.E.; Amore, A.; Barratt, J.; et al. The Oxford classification of IgA nephropathy: Rationale, clinicopathological correlations, and classification. Kidney Int. 2009, 76, 534–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A Working Group of the International IgA Nephropathy Network and the Renal Pathology Society; Roberts, I.S.; Cook, H.T.; Troyanov, S.; Alpers, C.E.; Amore, A.; Barratt, J.; Berthoux, F.; Bonsib, S.; Bruijn, J.A.; et al. The Oxford classification of IgA nephropathy: Pathology definitions, correlations, and reproducibility. Kidney Int. 2009, 76, 546–556. [Google Scholar] [CrossRef] [Green Version]
- Coppo, R.; Troyanov, S.; Bellur, S.; Cattran, D.; Cook, H.T.; Feehally, J.; Roberts, I.S.; Morando, L.; Camilla, R.; Tesar, V.; et al. Validation of the Oxford classification of IgA nephropathy in cohorts with different presentations and treatments. Kidney Int. 2014, 86, 828–836. [Google Scholar] [CrossRef] [Green Version]
- Barbour, S.J.; Coppo, R.; Zhang, H.; Liu, Z.H.; Suzuki, Y.; Matsuzaki, K.; Katafuchi, R.; Er, L.; Espino-Hernandez, G.; Kim, S.J.; et al. Evaluating a New International Risk-Prediction Tool in IgA Nephropathy. JAMA Intern. Med. 2019, 179, 942–952. [Google Scholar] [CrossRef]
- Suzuki, H.; Fan, R.; Zhang, Z.; Brown, R.; Hall, S.; Julian, B.A.; Chatham, W.W.; Suzuki, Y.; Wyatt, R.J.; Moldoveanu, Z.; et al. Aberrantly glycosylated IgA1 in IgA nephropathy patients is recognized by IgG antibodies with restricted heterogeneity. J. Clin. Investig. 2009, 119, 1668–1677. [Google Scholar] [CrossRef] [Green Version]
- Berthoux, F.; Suzuki, H.; Thibaudin, L.; Yanagawa, H.; Maillard, N.; Mariat, C.; Tomino, Y.; Julian, B.A.; Novak, J. Autoantibodies targeting galactose-deficient IgA1 associate with progression of IgA nephropathy. J. Am. Soc. Nephrol. 2012, 23, 1579–1587. [Google Scholar] [CrossRef] [Green Version]
- Yeo, S.C.; Cheung, C.K.; Barratt, J. New insights into the pathogenesis of IgA nephropathy. Pediatr. Nephrol. 2018, 33, 763–777. [Google Scholar] [CrossRef] [Green Version]
- Inoue, T.; Sugiyama, H.; Hiki, Y.; Takiue, K.; Morinaga, H.; Kitagawa, M.; Maeshima, Y.; Fukushima, K.; Nishizaki, K.; Akagi, H.; et al. Differential expression of glycogenes in tonsillar B lymphocytes in association with proteinuria and renal dysfunction in IgA nephropathy. Clin. Immunol. 2010, 136, 447–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruszkowski, J.; Lisowska, K.A.; Pindel, M.; Heleniak, Z.; Debska-Slizien, A.; Witkowski, J.M. T cells in IgA nephropathy: Role in pathogenesis, clinical significance and potential therapeutic target. Clin. Exp. Nephrol. 2019, 23, 291–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rauen, T.; Eitner, F.; Fitzner, C.; Sommerer, C.; Zeier, M.; Otte, B.; Panzer, U.; Peters, H.; Benck, U.; Mertens, P.R.; et al. Intensive Supportive Care plus Immunosuppression in IgA Nephropathy. N. Engl. J. Med. 2015, 373, 2225–2236. [Google Scholar] [CrossRef] [PubMed]
- Lv, J.; Zhang, H.; Wong, M.G.; Jardine, M.J.; Hladunewich, M.; Jha, V.; Monaghan, H.; Zhao, M.; Barbour, S.; Reich, H.; et al. Effect of Oral Methylprednisolone on Clinical Outcomes in Patients with IgA Nephropathy: The TESTING Randomized Clinical Trial. JAMA 2017, 318, 432–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A.; et al. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef]
- Yasutake, J.; Suzuki, Y.; Suzuki, H.; Hiura, N.; Yanagawa, H.; Makita, Y.; Kaneko, E.; Tomino, Y. Novel lectin-independent approach to detect galactose-deficient IgA1 in IgA nephropathy. Nephrol. Dial. Transplant. 2015, 30, 1315–1321. [Google Scholar] [CrossRef] [Green Version]
- Haas, M.; Verhave, J.C.; Liu, Z.H.; Alpers, C.E.; Barratt, J.; Becker, J.U.; Cattran, D.; Cook, H.T.; Coppo, R.; Feehally, J.; et al. A Multicenter Study of the Predictive Value of Crescents in IgA Nephropathy. J. Am. Soc. Nephrol. 2017, 28, 691–701. [Google Scholar] [CrossRef] [Green Version]
- Trimarchi, H.; Barratt, J.; Cattran, D.C.; Cook, H.T.; Coppo, R.; Haas, M.; Liu, Z.H.; Roberts, I.S.; Yuzawa, Y.; Zhang, H.; et al. Oxford Classification of IgA nephropathy 2016: An update from the IgA Nephropathy Classification Working Group. Kidney Int. 2017, 91, 1014–1021. [Google Scholar] [CrossRef] [Green Version]
- Coppo, R.; D’Arrigo, G.; Tripepi, G.; Russo, M.L.; Roberts, I.S.D.; Bellur, S.; Cattran, D.; Cook, T.H.; Feehally, J.; Tesar, V.; et al. Is there long-term value of pathology scoring in immunoglobulin A nephropathy? A validation study of the Oxford Classification for IgA Nephropathy (VALIGA) update. Nephrol. Dial. Transplant. 2020, 35, 1002–1009. [Google Scholar] [CrossRef]
- Suzuki, Y.; Matsuzaki, K.; Suzuki, H.; Okazaki, K.; Yanagawa, H.; Ieiri, N.; Sato, M.; Sato, T.; Taguma, Y.; Matsuoka, J.; et al. Serum levels of galactose-deficient immunoglobulin (Ig) A1 and related immune complex are associated with disease activity of IgA nephropathy. Clin. Exp. Nephrol. 2014, 18, 770–777. [Google Scholar] [CrossRef] [Green Version]
- Tang, Y.; He, H.; Hu, P.; Xu, X. T lymphocytes in IgA nephropathy. Exp. Ther. Med. 2020, 20, 186–194. [Google Scholar] [CrossRef] [Green Version]
- Elgueta, R.; Benson, M.J.; de Vries, V.C.; Wasiuk, A.; Guo, Y.; Noelle, R.J. Molecular mechanism and function of CD40/CD40L engagement in the immune system. Immunol. Rev. 2009, 229, 152–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagy, B., Jr.; Miszti-Blasius, K.; Kerenyi, A.; Clemetson, K.J.; Kappelmayer, J. Potential therapeutic targeting of platelet-mediated cellular interactions in atherosclerosis and inflammation. Curr. Med. Chem. 2012, 19, 518–531. [Google Scholar] [CrossRef] [PubMed]
- Aloui, C.; Prigent, A.; Sut, C.; Tariket, S.; Hamzeh-Cognasse, H.; Pozzetto, B.; Richard, Y.; Cognasse, F.; Laradi, S.; Garraud, O. The signaling role of CD40 ligand in platelet biology and in platelet component transfusion. Int. J. Mol. Sci. 2014, 15, 22342–22364. [Google Scholar] [CrossRef] [Green Version]
- Alaaeddine, N.; Hassan, G.S.; Yacoub, D.; Mourad, W. CD154: An immunoinflammatory mediator in systemic lupus erythematosus and rheumatoid arthritis. Clin. Dev. Immunol. 2012, 2012, 490148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biancone, L.; Andres, G.; Ahn, H.; DeMartino, C.; Stamenkovic, I. Inhibition of the CD40-CD40ligand pathway prevents murine membranous glomerulonephritis. Kidney Int. 1995, 48, 458–468. [Google Scholar] [CrossRef] [Green Version]
- Kalled, S.L.; Cutler, A.H.; Datta, S.K.; Thomas, D.W. Anti-CD40 ligand antibody treatment of SNF1 mice with established nephritis: Preservation of kidney function. J. Immunol. 1998, 160, 2158–2165. [Google Scholar] [CrossRef]
- Zhang, S.; Breidenbach, J.D.; Russell, B.H.; George, J.; Haller, S.T. CD40/CD40L Signaling as a Promising Therapeutic Target for the Treatment of Renal Disease. J. Clin. Med. 2020, 9, 3653. [Google Scholar] [CrossRef]
- Doublier, S.; Zennaro, C.; Musante, L.; Spatola, T.; Candiano, G.; Bruschi, M.; Besso, L.; Cedrino, M.; Carraro, M.; Ghiggeri, G.M.; et al. Soluble CD40 ligand directly alters glomerular permeability and may act as a circulating permeability factor in FSGS. PLoS ONE 2017, 12, e0188045. [Google Scholar] [CrossRef] [Green Version]
- Kuo, H.L.; Huang, C.C.; Lin, T.Y.; Lin, C.Y. IL-17 and CD40 ligand synergistically stimulate the chronicity of diabetic nephropathy. Nephrol. Dial. Transplant. 2018, 33, 248–256. [Google Scholar] [CrossRef] [Green Version]
- Yellin, M.J.; D’Agati, V.; Parkinson, G.; Han, A.S.; Szema, A.; Baum, D.; Estes, D.; Szabolcs, M.; Chess, L. Immunohistologic analysis of renal CD40 and CD40L expression in lupus nephritis and other glomerulonephritides. Arthritis Rheum. 1997, 40, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Rigothier, C.; Daculsi, R.; Lepreux, S.; Auguste, P.; Villeneuve, J.; Dewitte, A.; Doudnikoff, E.; Saleem, M.; Bourget, C.; Combe, C.; et al. CD154 Induces Matrix Metalloproteinase-9 Secretion in Human Podocytes. J. Cell. Biochem. 2016, 117, 2737–2747. [Google Scholar] [CrossRef] [PubMed]
- van Kooten, C.; van der Linde, X.; Woltman, A.M.; van Es, L.A.; Daha, M.R. Synergistic effect of interleukin-1 and CD40L on the activation of human renal tubular epithelial cells. Kidney Int. 1999, 56, 41–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartmann, K.; Wagner, N.; Rabenhorst, A.; Pflanz, L.; Leja, S.; Forster, A.; Gehring, M.; Kapp, A.; Raap, U. Serum IL-31 levels are increased in a subset of patients with mastocytosis and correlate with disease severity in adult patients. J. Allergy Clin. Immunol. 2013, 132, 232–235. [Google Scholar] [CrossRef] [PubMed]
- Rabenhorst, A.; Hartmann, K. Interleukin-31: A novel diagnostic marker of allergic diseases. Curr. Allergy Asthma Rep. 2014, 14, 423. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-García, J.D.J.; Rojas-Mayorquin, A.E.; Valle, Y.; Padilla-Gutierrez, J.R.; Castaneda-Moreno, V.A.; Mireles-Ramirez, M.A.; Munoz-Valle, J.F.; Ortuno-Sahagun, D. Decreased serum levels of sCD40L and IL-31 correlate in treated patients with Relapsing-Remitting Multiple Sclerosis. Immunobiology 2018, 223, 135–141. [Google Scholar] [CrossRef]
- Pastor Bandeira, I.; de Almeida Franzoi, A.E.; Murillo Wollmann, G.; de Medeiros Junior, W.L.G.; Nogueira Brandao, W.; Schatzmann Peron, J.P.; Becker, J.; Nascimento, O.J.M.; Magno Goncalves, M.V. Interleukin-31 and soluble CD40L: New candidate serum biomarkers that predict therapeutic response in multiple sclerosis. Neurol. Sci. 2022, 43, 6271–6278. [Google Scholar] [CrossRef]
- Ehara, T.; Shigematsu, H. Contribution of mast cells to the tubulointerstitial lesions in IgA nephritis. Kidney Int. 1998, 54, 1675–1683. [Google Scholar] [CrossRef] [Green Version]
- Konishi, Y.; Morikawa, T.; Okada, N.; Maeda, I.; Kitabayashi, C.; Yoshioka, K.; Okumura, M.; Nishiyama, A.; Ueda, M.; Takai, S.; et al. Evidence for abundant presence of chymase-positive mast cells in the kidneys of patients with immunoglobulin A nephropathy: Effect of combination therapy with prednisolone and angiotensin II receptor blocker valsartan. Hypertens. Res. 2008, 31, 1517–1524. [Google Scholar] [CrossRef] [Green Version]
- Johnson, R.J. Platelets in inflammatory glomerular injury. Semin. Nephrol. 1991, 11, 276–284. [Google Scholar]
- Couser, W.G. Pathogenesis of glomerular damage in glomerulonephritis. Nephrol. Dial. Transplant. 1998, 13 (Suppl S1), 10–15. [Google Scholar] [CrossRef] [Green Version]
- Gremmel, T.; Frelinger, A.L., 3rd; Michelson, A.D. Soluble CD40 Ligand in Aspirin-Treated Patients Undergoing Cardiac Catheterization. PLoS ONE 2015, 10, e0134599. [Google Scholar] [CrossRef]
- Taji, Y.; Kuwahara, T.; Shikata, S.; Morimoto, T. Meta-analysis of antiplatelet therapy for IgA nephropathy. Clin. Exp. Nephrol. 2006, 10, 268–273. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IgAN | ADPKD | Healthy Control | |
|---|---|---|---|
| N | 114 | 10 | 5 |
| Age (years) | 41.7 ± 15.5 b* | 58.2 ± 16.8 a* | 37 ± 8.4 |
| Gender, male, n (%) | 57 (50) | 5 (50) | 3 (60) |
| eGFR (ml/min/1.73 m2) | 71.4 ± 27.3 b* | 41.8 ± 29.2 ac* | 79.5 ± 8.08 b* |
| UPCR (g/gCr) | 0.73 (0.28–1.59) bc* | 0.09 (0.07–0.51) ac* | 0.03 (0.02–0.05) ab* |
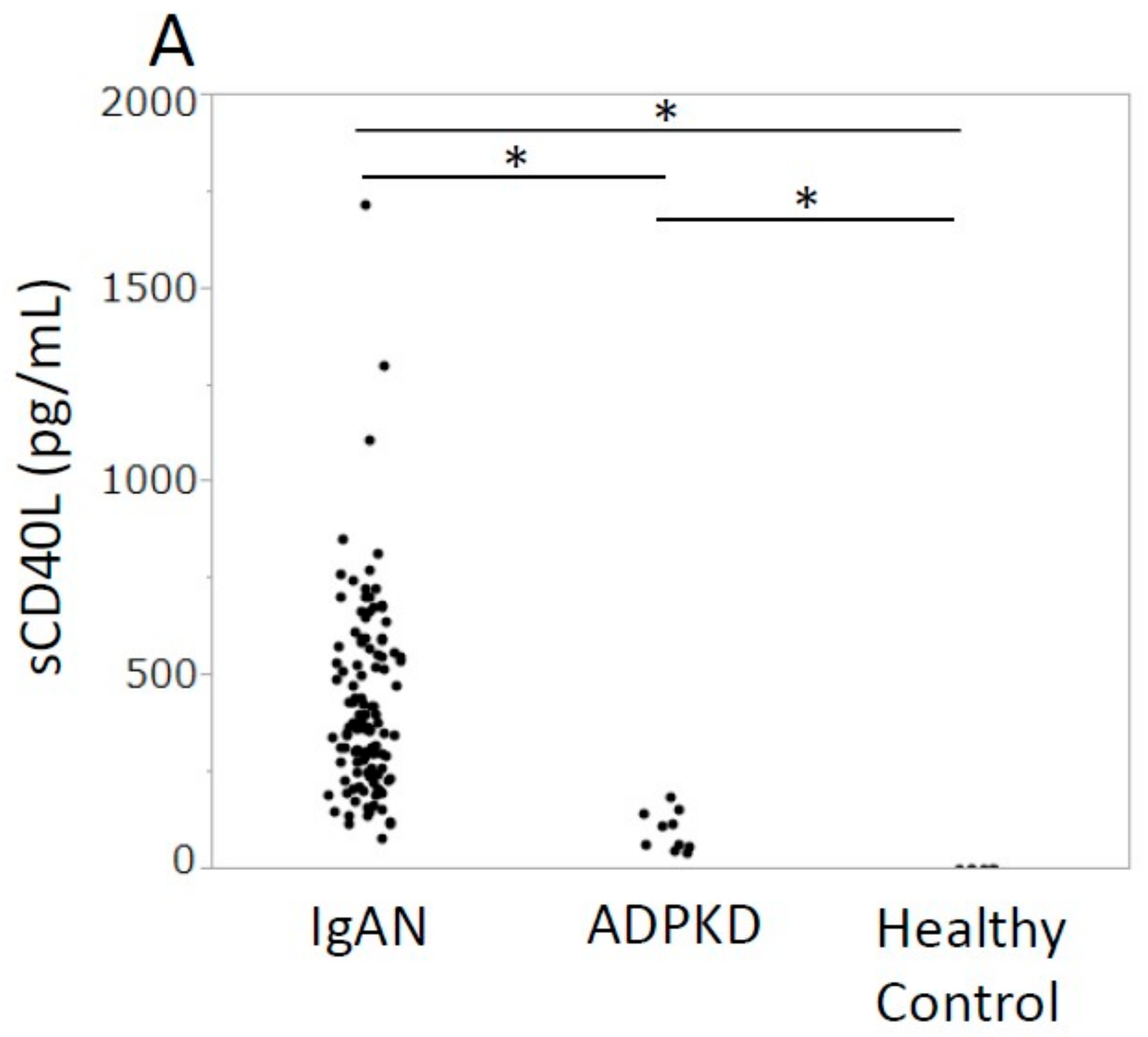
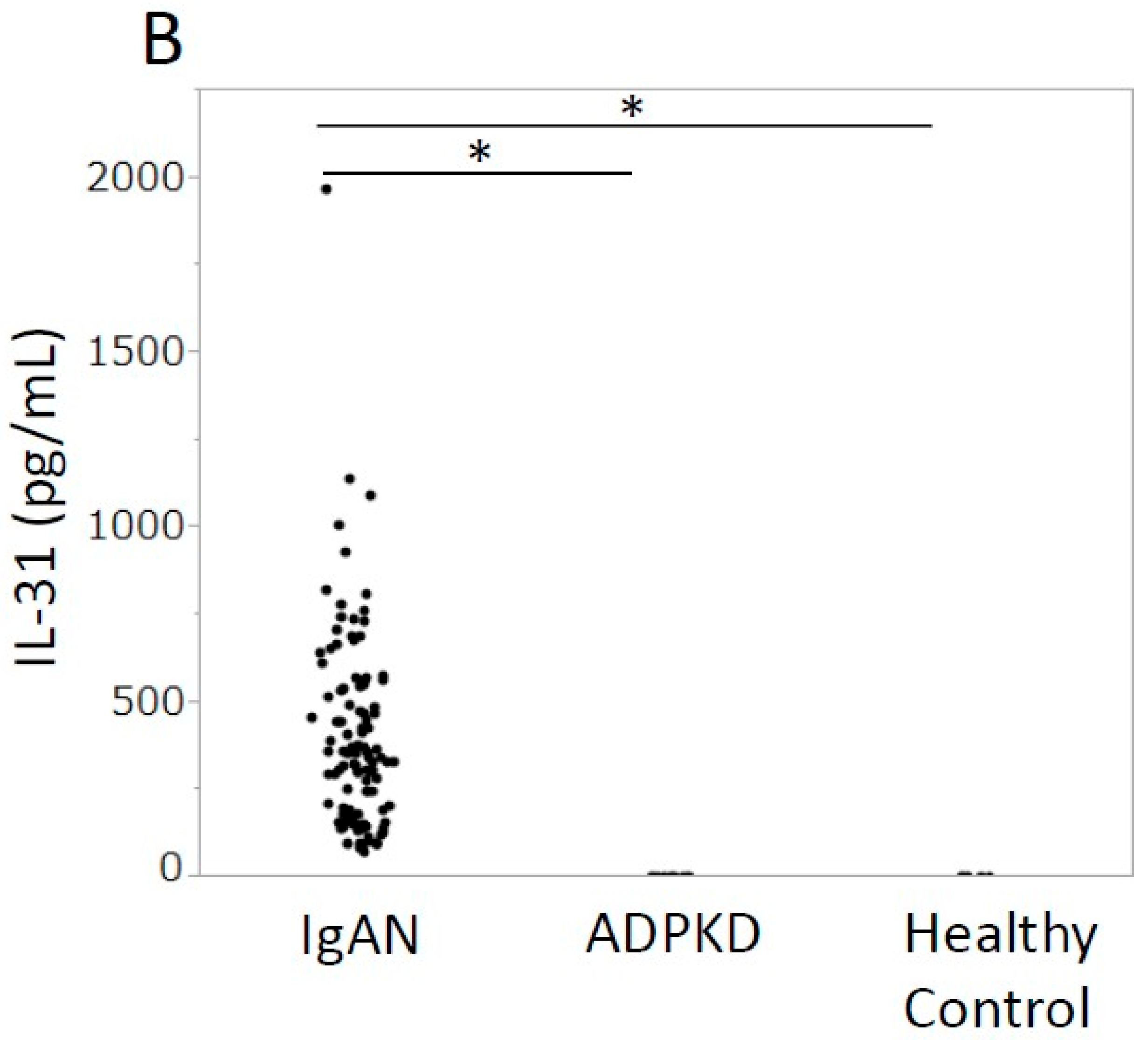
| Serum sCD40L (pg/mL) | 367 (252–560) bc* | 86.9 (55.4–146) ac* | 0.0 ab* |
| Serum IL-31 (pg/mL) | 348 (182–543) bc* | 0.0 a* | 0.0 a* |
| MBP (mmHg) | 94.8 (87–103) | 92.5 (74–101) | n.d. |
| Diabetes mellitus, n (%) | 10 (8.8) | 1 (10.0) | 0 (0.0) |
| Antihypertensive drugs, n (%) | 44 (30.1) | 7 (70.0) | 0 (0.0) |
| Oxford classification, n (%) | |||
| M1 | 4 (3.5) | - | - |
| E1 | 33 (28.9) | - | - |
| S1 | 50 (43.9) | - | |
| T1-2 | 34 (29.8) | - | - |
| C1-2 | 75 (65.8) | - | - |
| β | p | Model R2 | |
|---|---|---|---|
| Model 1 sCD40L ≥ median (pg/mL) | −0.37 | 0.011 * | 0.11 |
| Model 2 sCD40L ≥ median (pg/mL) | −0.35 | 0.016 * | 0.13 |
| eGFR < 60 (mL/min/1.73 m2) | 0.28 | 0.086 | |
| Model 3 sCD40L ≥ median (pg/mL) | −0.32 | 0.027 * | 0.14 |
| eGFR < 60 (mL/min/1.73 m2) | 0.28 | 0.091 | |
| MBP ≥ median (mmHg) | 0.20 | 0.16 |
| Odds Ratio | 95% CI | p | |
|---|---|---|---|
| Model 1 sCD40L (per 100 pg/mL) | 0.77 | 0.61–0.93 | 0.016 * |
| Model 2 sCD40L (per 100 pg/mL) | 0.78 | 0.63–0.95 | 0.023 * |
| eGFR (per 10 mL/min/1.73 m2) | 0.87 | 0.71–1.05 | 0.17 |
| Model 3 sCD40L (per 100 pg/mL) | 0.79 | 0.63–0.96 | 0.032 * |
| eGFR (per 10 mL/min/1.73 m2) | 0.88 | 0.71–1.08 | 0.23 |
| MBP (per 10 mmHg) | 1.07 | 0.77–1.52 | 0.65 |
| Odds Ratio | 95% CI | p | |
|---|---|---|---|
| Model 1 IL-31 (per 100 pg/mL) | 0.81 | 0.66–0.96 | 0.024 * |
| Model 2 IL-31 (per 100 pg/mL) | 0.82 | 0.67–0.97 | 0.038 * |
| eGFR (per 10 mL/min/1.73 m2) | 0.87 | 0.71–1.06 | 0.19 |
| Model 3 IL-31 (per 100 pg/mL) | 0.82 | 0.67–0.98 | 0.049 * |
| eGFR (per 10 mL/min/1.73 m2) | 0.89 | 0.72–1.09 | 0.28 |
| MBP (per 10 mmHg) | 1.12 | 0.80–1.57 | 0.50 |
| β | p | Model R2 | |
|---|---|---|---|
| Model 1 IL-31 ≥ median (pg/mL) | −0.33 | 0.028 * | 0.098 |
| Model 2 IL-31 ≥ median (pg/mL) | −0.31 | 0.037 * | 0.12 |
| eGFR < 60 (mL/min/1.73 m2) | 0.29 | 0.081 | |
| Model 3 IL-31 ≥ median (pg/mL) | −0.29 | 0.051 | 0.14 |
| eGFR < 60 (mL/min/1.73 m2) | 0.28 | 0.089 | |
| MBP ≥ median (mmHg) | 0.24 | 0.10 |
| sCD40L (pg/mL) | IL-31 (pg/mL) | |||||
|---|---|---|---|---|---|---|
| Score 0 | Score 1 | p | Score 0 | Score 1 | p | |
| M | 367.9 (271.6–572.0) | 267.7 (136.8–398.5) | 0.332 | 352.9 (196.0–556.5) | 214.6 (124.6–304.6) | 0.232 |
| E | 367.6 (267.8–598.3) | 380.5 (249.1–520.6) | 0.511 | 361.1 (209.3–564.4) | 304.1 (191.7–494.8) | 0.310 |
| S | 425.4 (207.6–573.4) | 363.6 (290.5–567.1) | 0.696 | 361.1 (159.8–572.1) | 321.9 (247.0–507.1) | 0.671 |
| Score 0 | Score 1–2 | p | Score 0 | Score 1–2 | p | |
| T | 399.4 (295.2–595.9) | 314.2 (206.7–473.2) | 0.008 * | 370.6 (248.1–562.7) | 298.9 (136.8–396.5) | 0.006 * |
| C | 408.6 (318.4–660.0) | 351.9 (230.6–551.4) | 0.089 | 370.6 (279.3–569.2) | 321.9 (182.3–522.5) | 0.114 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, K.; Sugiyama, H.; Morinaga, H.; Kitagawa, M.; Kano, Y.; Onishi, Y.; Mise, K.; Tanabe, K.; Uchida, H.A.; Wada, J. Serum sCD40L and IL-31 in Association with Early Phase of IgA Nephropathy. J. Clin. Med. 2023, 12, 2023. https://doi.org/10.3390/jcm12052023
Tanaka K, Sugiyama H, Morinaga H, Kitagawa M, Kano Y, Onishi Y, Mise K, Tanabe K, Uchida HA, Wada J. Serum sCD40L and IL-31 in Association with Early Phase of IgA Nephropathy. Journal of Clinical Medicine. 2023; 12(5):2023. https://doi.org/10.3390/jcm12052023
Chicago/Turabian StyleTanaka, Keiko, Hitoshi Sugiyama, Hiroshi Morinaga, Masashi Kitagawa, Yuzuki Kano, Yasuhiro Onishi, Koki Mise, Katsuyuki Tanabe, Haruhito A. Uchida, and Jun Wada. 2023. "Serum sCD40L and IL-31 in Association with Early Phase of IgA Nephropathy" Journal of Clinical Medicine 12, no. 5: 2023. https://doi.org/10.3390/jcm12052023