
Data Resource Profile: The Multiple Sclerosis Documentation System 3D and AOK PLUS Linked Database (MSDS-AOK PLUS)



Abstract
:1. Introduction
2. Data Resource Basics
2.1. MSDS3D
2.2. AOK PLUS
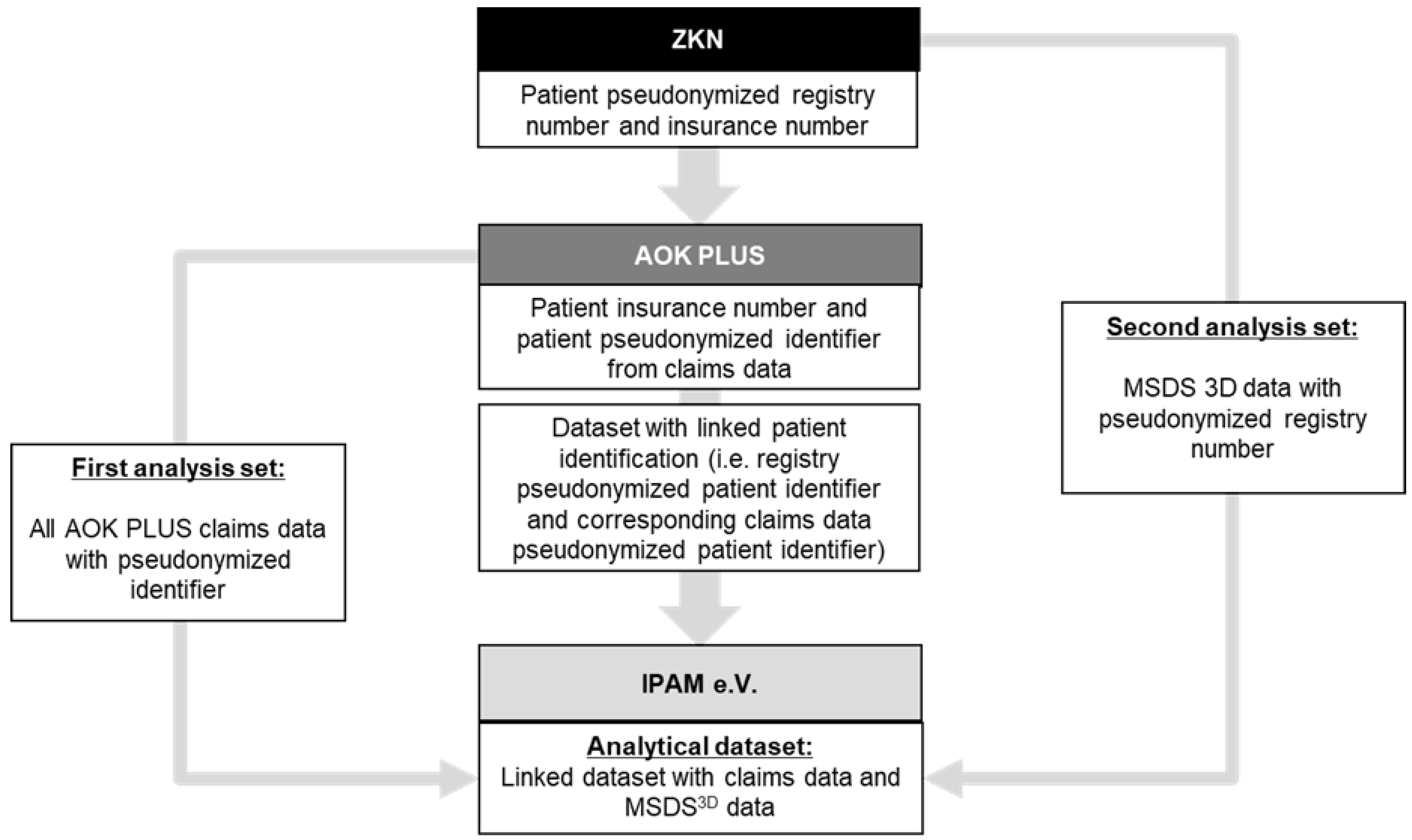
2.3. Linkage: MSDS-AOK PLUS
2.4. Ethical Considerations
3. Database Description
3.1. Setting
3.2. Data Contents
3.3. Purpose & Applications
3.3.1. The MSDS-AOK PLUS Mission
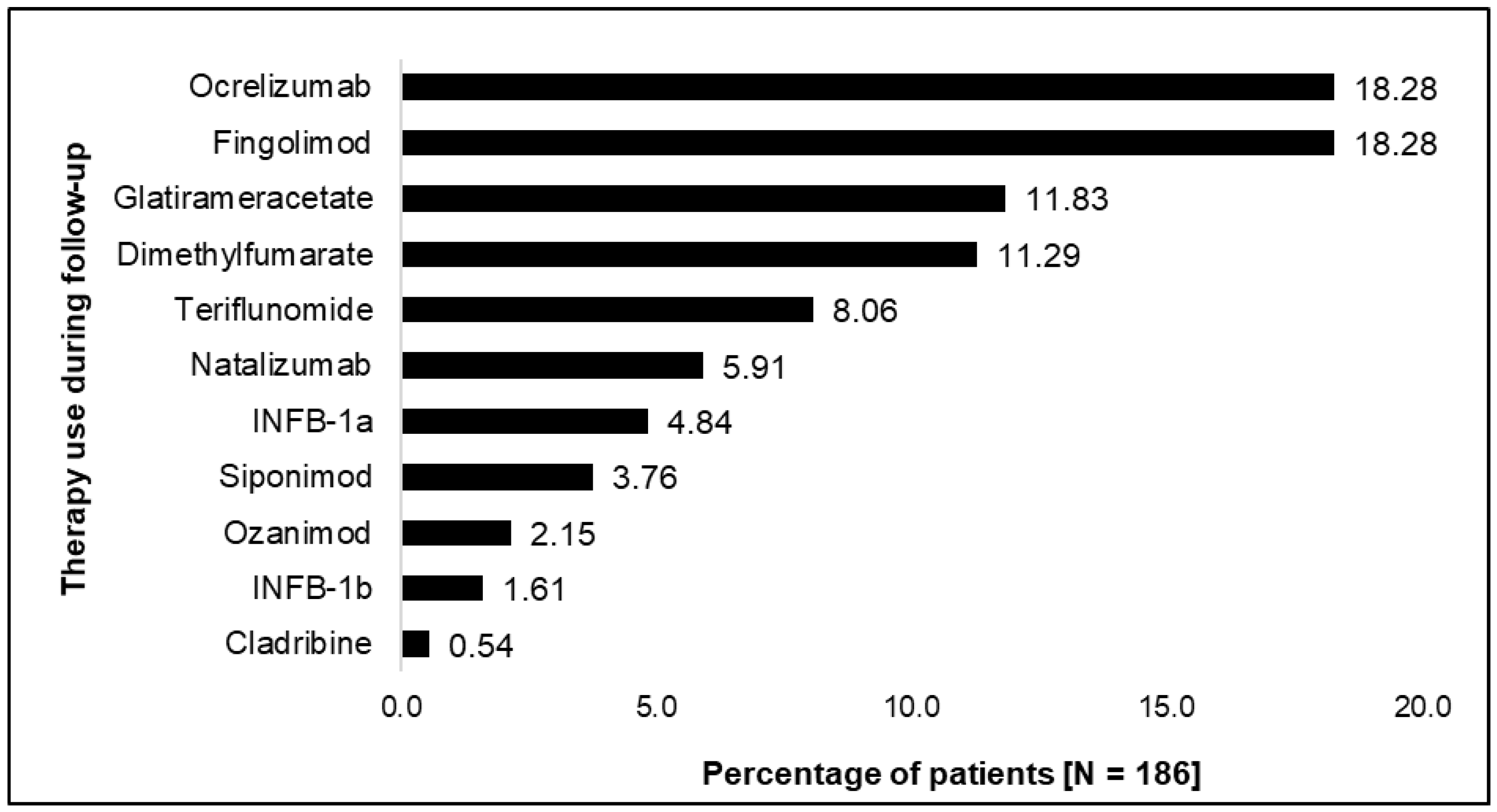
3.3.2. Use Case: Baseline Characteristics and Resource Consumption of a Selected MSDS-AOK PLUS Patient Cohort
4. Discussion
4.1. Significance of MSDS-AOK PLUS
4.2. Limitations
4.3. Data Access and Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cohen, J.A.; Trojano, M.; Mowry, E.M.; Uitdehaag, B.M.J.; Reingold, S.C.; Marrie, R.A. Leveraging real-world data to investigate multiple sclerosis disease behavior, prognosis, and treatment. Mult. Scler. J. 2019, 26, 23–37. [Google Scholar] [CrossRef]
- Ziemssen, T.; Hillert, J.; Butzkueven, H. The importance of collecting structured clinical information on multiple sclerosis. BMC Med. 2016, 14, 81. [Google Scholar] [CrossRef]
- Trojano, M.; Tintore, M.; Montalban, X.; Hillert, J.; Kalincik, T.; Iaffaldano, P.; Spelman, T.; Sormani, M.P.; Butzkueven, H. Treatment decisions in multiple sclerosis—Insights from real-world observational studies. Nat. Rev. Neurol. 2017, 13, 105–118. [Google Scholar] [CrossRef]
- Bebo, B.F., Jr.; Fox, R.J.; Lee, K.; Utz, U.; Thompson, A.J. Landscape of MS patient cohorts and registries: Recommendations for maximizing impact. Mult. Scler. J. 2018, 24, 579–586. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- Inojosa, H.; Schriefer, D.; Ziemssen, T. Clinical outcome measures in multiple sclerosis: A review. Autoimmun. Rev. 2020, 19, 102512. [Google Scholar] [CrossRef]
- Jette, N.; Atwood, K.; Hamilton, M.; Hayward, R.; Day, L.; Mobach, T.; Maxwell, C.; Fortin, C.M.; Fiebelkorn, G.; Barlow, K.; et al. Linkage between neurological registry data and administrative data. Can. J. Neurol. Sci. 2013, 40, S32–S34. [Google Scholar] [CrossRef]
- Leray, E.; Vukusic, S.; Debouverie, M.; Clanet, M.; Brochet, B.; de Sèze, J.; Zéphir, H.; Defer, G.; Lebrun-Frenay, C.; Moreau, T.; et al. Excess Mortality in Patients with Multiple Sclerosis Starts at 20 Years from Clinical Onset: Data from a Large-Scale French Observational Study. PLoS ONE 2015, 10, e0132033. [Google Scholar] [CrossRef]
- McKay, K.A.; Tremlett, H.; Fisk, J.D.; Zhang, T.; Patten, S.B.; Kastrukoff, L.; Campbell, T.; Marrie, R.A. Psychiatric comorbidity is associated with disability progression in multiple sclerosis. Neurology 2018, 90, e1316–e1323. [Google Scholar] [CrossRef]
- Marrie, R.A.; Cutter, G.R.; Fox, R.J.; Vollmer, T.; Tyry, T.; Salter, A. NARCOMS and Other Registries in Multiple Sclerosis: Issues and Insights. Int. J. MS Care 2021, 23, 276–284. [Google Scholar] [CrossRef]
- Berkovich, R.; Fox, E.; Okai, A.; Ding, Y.; Gorritz, M.; Bartolome, L.; Wade, R.L.; Su, W.; Johnson, K.M.; Russo, P. Identifying disability level in multiple sclerosis patients in a U.S.-based health plan claims database. J. Med. Econ. 2021, 24, 46–53. [Google Scholar] [CrossRef]
- Culpepper, W.J.; Marrie, R.A.; Langer-Gould, A.; Wallin, M.T.; Campbell, J.D.; Nelson, L.M.; Kaye, W.E.; Wagner, L.; Tremlett, H.; Chen, L.H.; et al. Validation of an algorithm for identifying MS cases in administrative health claims datasets. Neurology 2019, 92, e1016–e1028. [Google Scholar] [CrossRef]
- Marrie, R.A.; Tan, Q.; Ekuma, O.; Marriott, J.J. Development and Internal Validation of a Disability Algorithm for Multiple Sclerosis in Administrative Data. Front. Neurol. 2021, 12, 754144. [Google Scholar] [CrossRef]
- Ziemssen, T.; Kempcke, R.; Eulitz, M.; Großmann, L.; Suhrbier, A.; Thomas, K.; Schultheiss, T. Multiple sclerosis documentation system (MSDS): Moving from documentation to management of MS patients. J. Neural Transm. 2013, 120 (Suppl. S1), S61–S66. [Google Scholar] [CrossRef]
- Ziemssen, T.; Kern, R.; Voigt, I.; Haase, R. Data Collection in Multiple Sclerosis: The MSDS Approach. Front. Neurol. 2020, 11, 445. [Google Scholar] [CrossRef]
- Kern, R.; Haase, R.; Eisele, J.C.; Thomas, K.; Ziemssen, T. Designing an Electronic Patient Management System for Multiple Sclerosis: Building a Next Generation Multiple Sclerosis Documentation System. Interact. J. Med. Res. 2016, 5, e2. [Google Scholar] [CrossRef]
- Pette, M.; Eulitz, M. The Multiple Sclerosis Documentation System MSDS. Discussion of a documentation standard for multiple sclerosis. Nervenarzt 2002, 73, 144–148. [Google Scholar] [CrossRef]
- Pette, M.; Zettl, U.K. The use of multiple sclerosis databases at neurological university hospitals in Germany. Mult. Scler. J. 2002, 8, 265–267. [Google Scholar] [CrossRef]
- Schultheiss, T.; Kempcke, R.; Kratzsch, F.; Eulitz, M.; Pette, M.; Reichmann, H.; Ziemssen, T. Multiple sclerosis management system 3D. Moving from documentation towards management of patients. Nervenarzt 2012, 83, 450–457. [Google Scholar] [CrossRef]
- Mowry, E.M.; Bermel, R.A.; Williams, J.R.; Benzinger, T.L.S.; de Moor, C.; Fisher, E.; Hersh, C.M.; Hyland, M.H.; Izbudak, I.; Jones, S.E.; et al. Harnessing Real-World Data to Inform Decision-Making: Multiple Sclerosis Partners Advancing Technology and Health Solutions (MS PATHS). Front. Neurol. 2020, 11, 632. [Google Scholar] [CrossRef]
- Ziemssen, T.; Hoffmann, O.; Klotz, L.; Schreiber, H.; Weber, M.S.; Rauser, B. Gaining First Insights on Secondary Progressive Multiple Sclerosis Patients Treated With Siponimod in Clinical Routine: Protocol of the Noninterventional Study AMASIA. JMIR Res. Protoc. 2020, 9, e19598. [Google Scholar] [CrossRef]
- Ziemssen, T.; Kern, R.; Cornelissen, C. Study design of PANGAEA 2.0, a non-interventional study on RRMS patients to be switched to fingolimod. BMC Neurol. 2016, 16, 129. [Google Scholar] [CrossRef]
- Ziemssen, T.; Gass, A.; Wuerfel, J.; Bayas, A.; Tackenberg, B.; Limmroth, V.; Linker, R.; Mäurer, M.; Haas, J.; Stangel, M.; et al. Design of TRUST, a non-interventional, multicenter, 3-year prospective study investigating an integrated patient management approach in patients with relapsing-remitting multiple sclerosis treated with natalizumab. BMC Neurol. 2016, 16, 98. [Google Scholar] [CrossRef] [PubMed]
- Ziemssen, T.; Kern, R.; Cornelissen, C. The PANGAEA study design—A prospective, multicenter, non-interventional, long-term study on fingolimod for the treatment of multiple sclerosis in daily practice. BMC Neurol. 2015, 15, 93. [Google Scholar] [CrossRef]
- Dirks, P.; Zingler, V.; Leemhuis, J.; Berthold, H.; Hieke-Schulz, S.; Wormser, D.; Ziemssen, T. Design of a non-interventional post-marketing study to assess the long-term safety and effectiveness of ocrelizumab in German real world multiple sclerosis cohorts—The CONFIDENCE study protocol. BMC Neurol. 2020, 20, 95. [Google Scholar] [CrossRef]
- Ziemssen, T.; Engelmann, U.; Jahn, S.; Leptich, A.; Kern, R.; Hassoun, L.; Thomas, K. Rationale, design, and methods of a non-interventional study to establish safety, effectiveness, quality of life, cognition, health-related and work capacity data on Alemtuzumab in multiple sclerosis patients in Germany (TREAT-MS). BMC Neurol. 2016, 16, 109. [Google Scholar] [CrossRef]
- Rudick, R.A.; Miller, D.; Bethoux, F.; Rao, S.M.; Lee, J.C.; Stough, D.; Reece, C.; Schindler, D.; Mamone, B.; Alberts, J. The Multiple Sclerosis Performance Test (MSPT): An iPad-based disability assessment tool. J. Vis. Exp. 2014, e51318. [Google Scholar] [CrossRef]
- Ness, N.H.; Haase, R.; Kern, R.; Schriefer, D.; Ettle, B.; Cornelissen, C.; Akguen, K.; Ziemssen, T. The Multiple Sclerosis Health Resource Utilization Survey (MS-HRS): Development and Validation Study. J. Med. Internet Res. 2020, 22, e17921. [Google Scholar] [CrossRef]
- Cella, D.; Lai, J.S.; Nowinski, C.J.; Victorson, D.; Peterman, A.; Miller, D.; Bethoux, F.; Heinemann, A.; Rubin, S.; Cavazos, J.E.; et al. Neuro-QOL: Brief measures of health-related quality of life for clinical research in neurology. Neurology 2012, 78, 1860–1867. [Google Scholar] [CrossRef]
- Ziemssen, T.; Phillips, G.; Shah, R.; Mathias, A.; Foley, C.; Coon, C.; Sen, R.; Lee, A.; Agarwal, S. Development of the multiple sclerosis (MS) early mobility impairment questionnaire (EMIQ). J. Neurol. 2016, 263, 1969–1983. [Google Scholar] [CrossRef]
- Hobart, J.C.; Riazi, A.; Lamping, D.L.; Fitzpatrick, R.; Thompson, A.J. Measuring the impact of MS on walking ability: The 12-Item MS Walking Scale (MSWS-12). Neurology 2003, 60, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Busse, R.; Blümel, M. Germany: Health System Review; World Health Organization: Geneva, Switzerland, 2014; Volume 16, 296p. [Google Scholar]
- Learmonth, Y.C.; Motl, R.W.; Sandroff, B.M.; Pula, J.H.; Cadavid, D. Validation of patient determined disease steps (PDDS) scale scores in persons with multiple sclerosis. BMC Neurol. 2013, 13, 37. [Google Scholar] [CrossRef] [PubMed]
- Flachenecker, P.; Stuke, K.; Elias, W.; Freidel, M.; Haas, J.; Pitschnau-Michel, D.; Schimrigk, S.; Zettl, U.K.; Rieckmann, P. Multiple sclerosis registry in Germany: Results of the extension phase 2005/2006. Dtsch. Ärzteblatt Int. 2008, 105, 113–119. [Google Scholar] [CrossRef]
- Middleton, R.M.; Rodgers, W.J.; Chataway, J.; Schmierer, K.; Rog, D.; Galea, I.; Akbari, A.; Tuite-Dalton, K.; Lockhart-Jones, H.; Griffiths, D.; et al. Validating the portal population of the United Kingdom Multiple Sclerosis Register. Mult. Scler. Relat. Disord. 2018, 24, 3–10. [Google Scholar] [CrossRef]
- Hillert, J.; Magyari, M.; Soelberg Sørensen, P.; Butzkueven, H.; Van Der Welt, A.; Vukusic, S.; Trojano, M.; Iaffaldano, P.; Pellegrini, F.; Hyde, R.; et al. Treatment Switching and Discontinuation Over 20 Years in the Big Multiple Sclerosis Data Network. Front. Neurol. 2021, 12, 647811. [Google Scholar] [CrossRef]
- Geys, L.; Parciak, T.; Pirmani, A.; McBurney, R.; Schmidt, H.; Malbaša, T.; Ziemssen, T.; Bergmann, A.; Rojas, J.I.; Cristiano, E.; et al. The Multiple Sclerosis Data Alliance Catalogue: Enabling Web-Based Discovery of Metadata from Real-World Multiple Sclerosis Data Sources. Int. J. MS Care 2021, 23, 261–268. [Google Scholar] [CrossRef]
- Wolf, A.; Dedman, D.; Campbell, J.; Booth, H.; Lunn, D.; Chapman, J.; Myles, P. Data resource profile: Clinical Practice Research Datalink (CPRD) Aurum. Int. J. Epidemiol. 2019, 48, 1740–1740g. [Google Scholar] [CrossRef]
- Ness, N.H. Relapses increase the financial burden of RRMS. Pharm. Outcomes News 2020, 853, 24. [Google Scholar] [CrossRef]
- Ness, N.H.; Schriefer, D.; Haase, R.; Ettle, B.; Cornelissen, C.; Ziemssen, T. Differentiating societal costs of disability worsening in multiple sclerosis. J. Neurol. 2020, 267, 1035–1042. [Google Scholar] [CrossRef]
- Schriefer, D.; Ness, N.H.; Haase, R.; Ziemssen, T. Gender disparities in health resource utilization in patients with relapsing-remitting multiple sclerosis: A prospective longitudinal real-world study with more than 2000 patients. Ther. Adv. Neurol. Disord. 2020, 13, 1756286420960274. [Google Scholar] [CrossRef]
- Hoffmann, F. Review on use of German health insurance medication claims data for epidemiological research. Pharmacoepidemiol. Drug Saf. 2009, 18, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Andersohn, F.; Garbe, E. Pharmakoepidemiologische Forschung mit Routinedaten des Gesundheitswesens. Bundesgesundheitsblatt Gesundh. Gesundh. 2008, 51, 1135. [Google Scholar] [CrossRef]
- Schubert, I.; Köster, I.; Küpper-Nybelen, J.; Ihle, P. Versorgungsforschung mit GKV-Routinedaten. Bundesgesundheitsblatt Gesundh. Gesundh. 2008, 51, 1095–1105. [Google Scholar] [CrossRef]
- Ghiani, M.; Lehne, M.; Ziemssen, T.; Dillenseger, A.; Maywald, U.; Wilke, T. RWD24 Assessing the Performance of Propensity Score Methods in Balancing Unobservable Confounders: Evidence From Linked Data in Multiple Sclerosis. Value Health 2022, 25, S452. [Google Scholar] [CrossRef]
- Zhuleku, E.; Ziemssen, T.; Dillenseger, A.; Maywald, U.; Wilke, T.; Ghiani, M. RWD58 Coding of Multiple Sclerosis Subtypes in German Administrative Claims Data: A Validation Study Using the MSDS-AOK PLUS Linked Database. Value Health 2022, 25, S459. [Google Scholar] [CrossRef]
- Zhuleku, E.; Ziemssen, T.; Dillenseger, A.; Maywald, U.; Wilke, T.; Ghiani, M. RWD126 Introducing the German MSDS-AOK PLUS Database: Linkage of Administrative Claims Data and a Patient Registry for Advanced RWE Capabilities in Multiple Sclerosis. Value Health 2022, 25, S473. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Description |
|---|---|
| Coverage | Regional coverage of MS patients insured in the regions of Saxony and Thuringia visiting the ZKN center in Dresden |
| Data type | Retrospective claims and medical records supplemented with prospective data collection of medical records via MSDS3D |
| Sample size | 500 patients a |
| Data coverage | Administrative claims (AOK PLUS): 1 January 2014 to 31 March 2022 a Electronic Medical Records (MSDS3D): starting from initial MS diagnosis and onset of first symptoms, with regular documentation from patient’s first appearance at the clinic to date |
| Data access | Data available via access through university affiliated research institute (IPAM e.V.). Indirect access is not available |
| Ethical approval | Ethics Committee at the Technical University of Dresden and the Ministry of Saxonia (SGB § 75). No further ethical approval is required |
| Data Field | Description | Data Source | |||
|---|---|---|---|---|---|
| AOK PLUS | MSDS3D | ||||
| Availability | Details | Availability | Details | ||
| Sex | Categorical variable for male/female as documented in both databases | X | X | Documented at baseline | |
| Date of birth | AOK PLUS: Year in which patient was born MSDS3D: Day, month, and year in which the patient was born | X | X | Documented at baseline | |
| Weight | Weight in kg | X | Documented every 3–6 months | ||
| Height | Height in cm | X | Documented every 3–6 months | ||
| Date of initial MS diagnosis | Day, month, year of first MS diagnosis | Partial | If first diagnoses (ICD-10-GM) occur within data availability; based on proxy employing washout period | X | Documented at baseline; missing for some patients |
| Date of initial MS symptom | Day, month, year of onset of first MS symptom | Partial | X | Documented at baseline; missing for some patients | |
| Type of first symptoms | AOK PLUS: Symptoms based on ICD-10-GM coding MSDS3D: Free text entry of type of symptoms observed at baseline | Partial | Based on available ICD-10-GM coding | X | Documented at baseline; missing for some patients |
| MS subtype | MS type coded as per ICD-10-GM as newly diagnosed/CIS, RRMS, PPMS, SPMS, or unspecified and development over time | X | X | Documented every 3–6 months if applicable | |
| Concomitant diseases/diagnoses | AOK PLUS: Record of all diagnoses of patient under insurance based on inpatient and outpatient diagnoses MSDS3D: Record of MS symptoms and related comorbidities | X | Partial | Documented every 3–6 months if applicable | |
| Death | Binary variable indicating whether the patient has died (yes/no); if yes, day, month, and year of death | X | X | ||
| Lab tests | AOK PLUS: All laboratory tests documented through EBM codes MSDS3D: All laboratory tests that are run within patients’ visits at ZKN. Partial external lab data available if provided by patients. | X | Partial | Documented every 3–6 months depending on DMT use; conditional availability | |
| Lab test results | All laboratory test results that are run within patients´ visits at ZKN. Partial external lab data available if provided by patients. | Partial | Documented every 3–6 months depending on DMT use; conditional availability | ||
| Imaging | AOK PLUS: All imaging procedures (MRI, OCT, etc.) as documented by OPS and EBM codes MSDS3D: MS specific imaging procedures including MRI and OCT | X | X | Documented every 3–6 months or once a year depending on DMT use | |
| Imaging results | MS specific MRI and OCT images and neuroradiological findings over time as text describing amount and location of new lesions | X | Documented every 3–6 months or once a year depending on DMT use | ||
| General practitioner (GP) visits | AOK PLUS: GP visit documented by GP specialty code a MSDS3D: GP visits conditional on if physician letter is provided by patient | X | Partial | Conditional availability; diagnosis code not always available | |
| Neurologist visits | AOK PLUS: Neurologists visit documented by Neurologist specialty code a MSDS3D: Neurologist visits taking place at ZKN. Partial documentation of external neurologist visits, depending on if physician letter is provided. | X | Partial | Documented every 3–6 months; conditional availability of external neurologist visits | |
| Inpatient prescriptions | AOK PLUS: For expensive drugs, inpatient OPS or NUB codes are used to identify inpatient prescriptions of agents. MSDS3D: DMT use and other agents used to treat MS symptoms, conditional on if hospital discharge/physician letter is provided by patient | Partial | Partial | Documented every 3–6 months; conditional availability | |
| Outpatient prescriptions | AOK PLUS: All prescriptions documented by ATC codes, with associated date of prescription, number, and strength of packages; treatment duration can be estimated. MSDS3D: DMT use and other agents used to treat MS symptoms | X | Partial | ||
| Hospitalizations | AOK PLUS: All admissions and discharge dates of hospitalizations with associated diagnoses MSDS3D: Admission and discharge dates of hospitalization if information provided by the patient or with patient permission | X | Partial | Conditional availability | |
| Emergency Room (ER) visits | AOK PLUS: ER visits admission and discharge dates associated with overnight inpatient admission (including diagnoses) or emergency services on evenings, weekends, or public holidays in the outpatient setting via EBM codes MSDS3D: Admission and discharge dates of ER visits if information provided by the patient or with patient permission | Partial | Partial | Conditional availability | |
| Rehabilitation stays | AOK PLUS: All admission and discharge dates of inpatient rehabilitation stays with associated diagnoses paid by the sickness fund b MSDS3D: Admission and discharge dates of rehabilitation stays if provided by the patient or with patient permission | X | Partial | Conditional availability | |
| Aids and remedies | AOK PLUS: Therapeutic devices (walkers, wheelchairs, etc.) captured via Hilfsmittel codes and remedy services provided by medically trained staff (physical, speech, occupational therapy, etc.) via Heilmittel codes MSDS3D: Partial capture of select aids (unstructured) c | X | Partial | Aids every 3–6 months or yearly; remedies not currently available | |
| Surgical procedures | AOK PLUS: Inpatient and outpatient procedures as documented by OPS and EBM codes, respectively MSDS3D: Any procedures or health-related assessments as provided by patients or with patient permission | X | Partial | Conditional availability | |
| Non-surgical procedures | AOK PLUS: Inpatient and outpatient procedures as documented by OPS and EBM codes, respectively MSDS3D: Any procedures or health-related assessments as provided by patients or with patient permission | X | Partial | Conditional availability | |
| Primary care costs (GP) | Total associated costs of GP visits documented by GP specialty code with associated diagnoses d | X | |||
| Outpatient specialist costs | Total associated costs of specialist visits (ex. neurologist) documented by physician specialty codes with associated diagnoses (all-cause vs. MS-specific) d | X | |||
| Inpatient admission costs | Costs reported per Diagnosis Related Group (DRG) codes, including total cost of inpatient stay with associated diagnoses (all-cause vs. MS-specific) | X | |||
| Prescription costs | Cost associated to any outpatient prescriptions with associated ATC code | X | |||
| Rehabilitation costs | Costs related to inpatient rehabilitation visits with associated diagnoses (all-cause vs. MS-specific) paid by the sickness fund b | X | |||
| Costs of aids & remedies | Costs of all therapeutic devices and remedy services by medically trained staff covered by the sickness fund | X | |||
| Indirect costs due to sick leave | Based on number of days absent from work multiplied with average gross salary (all-cause vs. MS-specific) | X | |||
| Relapses | Acute presentation of patients to ZKN at onset of new or worsening symptoms with subsequent evaluation to determine whether relapse or other cause is possible | X | General documentation every 3–6 months on disease activity | ||
| Expanded Disability Status Scale (EDSS) [5] | EDSS score (0–10) assessed by physicians with associated functional system sub-scores: Ambulation (0–10), Pyramidal (0–6), Cerebellar (0–5), Brainstem (0–5), Sensory (0–6), Bowel & Bladder (0–6), Visual (0–6), and Cerebral (0–5) | X | Documentation every 3–6 months; yearly for a subset of patients | ||
| MS Performance Test (MSPT) [27] | MSPT as a digital adaptation and expansion of the paper-based Multiple Sclerosis Functional Composite (MSFC) | X | Documentation every 3–6 months as of July 2017 | ||
| Processing Speed Test (PST), digital adaption to the Symbol Digit Modalities Test (SDMT) | X | Documentation every 3–6 months | |||
| Low Contrast Letter Acuity Test (LCLAT), showing the number of correct letters at 100% and 2.5% | X | Documentation every 3–6 months | |||
| Walking Speed Test (WST), digital adaptation to the Timed 25-Foot Walk (T25-FW); result as time in minutes | X | Documentation every 3–6 months | |||
| Manual Dexterity Test (MDT), digital adaptation to the 9-Hole Peg Test (9HPT); result as time in minutes per hand | X | Documentation every 3–6 months | |||
| Patient Determined Disease Steps (PDDS) [33], patient-reported outcome of disability in MS with nine ordinal levels ranging between 0 (normal) and 8 (bedridden) | X | Documentation every 3–6 months | |||
| Quality of Life in Neurological Disorders (NeuroQoL) [29], patient-reported outcome on physical, mental, and social effects experienced by patients with MS (anxiety, depression, fatigue, upper extremity function—fine motor/activities of daily living, lower extremity function—mobility, applied cognition—general concerns and cognition–executive function, emotional and behavioral dyscontrol, positive affect and well-being; sleep disturbance, ability to participate in social roles and activities, satisfaction with social roles and activities, stigma). | X | Documentation every 6 months to yearly | |||
| MS-Health Resource Survey (HRS) [28] | Patient-reported healthcare resource utilization survey reporting direct medical costs, direct nonmedical costs) and indirect costs. | X | Documentation yearly | ||
| Early Mobility Impairment Questionnaire (EMIQ) [30] | Patient-reported questionnaire scores for nine-item EMIQ for detecting mobility impairment | X | Documentation yearly | ||
| Multiple Sclerosis Walking Scale (MSWS-12) [31] | Patient-reported MSWS-12 scores based on 12 item questionnaire to determine how much MS has limited walking ability in the past two weeks | X | Documentation yearly | ||
| MSDS-AOK PLUS Applications |
|---|
| Comparative effectiveness |
|
| Post-authorization safety studies |
|
| Disease behavior & prognosis |
|
| Treatment patterns |
|
| Economic modeling |
|
| Outcome measure validation |
|
| Historical controls |
|
| Characteristic | MS Cohort (N = 186) | Data Source |
|---|---|---|
| Female, n (%) | 142 (76.34) | AOK PLUS |
| Age, years | AOK PLUS | |
| Mean (SD) | 49.14 (11.54) | |
| Median (Range) | 50.03 (22.01–79.05) | |
| Time since first diagnosis a, years | MSDS3D | |
| Mean (SD) | 12.07 (8.23) | |
| Median (Range) | 11.01 (0.67–44.03) | |
| MS subtype b, n (%) | MSDS3D | |
| First manifestation/CIS | 3 (1.61) | |
| RRMS | 144 (77.42) | |
| PPMS | 7 (3.76) | |
| SPMS | 18 (9.68) | |
| Not specified | 14 (7.53) | |
| Charlson Comorbidity Index (CCI) c | AOK PLUS | |
| 0 | 117 (62.90) | |
| 1–2 | 47 (25.26) | |
| 3–4 | 16 (8.60) | |
| ≥5 | 6 (3.23) | |
| EDSS | MSDS3D | |
| Mean (SD) | 3.35 (1.76) | |
| Median (Range) | 3 (1–8) | |
| EDSS distribution, n (%) | MSDS3D | |
| 1–1.5 | 33 (17.74) | |
| 2–2.5 | 51 (27.42) | |
| 3–3.5 | 30 (16.1) | |
| 4–4.5 | 22 (11.83) | |
| 5–5.5 | 2 (1.08) | |
| 6–6.5 | 26 (13.98) | |
| 7–7.5 | 6 (3.23) | |
| ≥8 | 1 (0.54) | |
| Not assessed | 15 (8.06) | |
| Comorbidities at baseline, n (%) | AOK PLUS | |
| Diabetes mellitus | 18 (9.68) | |
| Cardiovascular disease | 21 (11.29) | |
| Hypertension | 62 (33.33) | |
| Obesity | 18 (9.68) | |
| Depression & Anxiety | 61 (32.80) | |
| Outcome | MS Cohort (N = 186) |
|---|---|
| Follow-up time per patient (years) | 2.50 |
| Total patient years (PY) | 464.24 |
| Outpatient Healthcare Resource Use | |
| All outpatient visits | |
| Patients with ≥1 all-cause visit, n (%) | 185 (99.46) |
| Mean all-cause visits per PY (SD) | 12.99 (7.91) |
| Patients with ≥1 MS-related visit, n (%) | 183 (98.39) |
| Mean MS-related visits per PY (SD) | 6.69 (3.99) |
| GP visits | |
| Patients with ≥1 all-cause GP visit, n (%) | 183 (98.39) |
| Mean all-cause GP visits per PY (SD) | 3.49 (1.75) |
| Patients with ≥1 MS-related GP visit, n (%) | 178 (95.70) |
| Mean MS-related GP visits per PY (SD) | 3.12 (1.70) |
| Neurologist visits | |
| Patients with ≥1 all-cause visit, n (%) | 51 (27.42) |
| Mean all-cause visits per PY (SD) | 0.70 (1.38) |
| Patients with ≥1 MS-related visit, n (%) | 44 (23.66) |
| Mean MS-related visits per PY (SD) | 0.63 (1.32) |
| Inpatient Healthcare Resource Use | |
| Hospitalizations | |
| Patients with ≥1 all-cause admission, n (%) | 72 (38.71) |
| Mean all-cause admissions per PY (SD) | 0.40 (0.75) |
| Patients with ≥1 MS-related admission, n (%) | 61 (32.80) |
| Mean MS-related admissions per PY (SD) | 0.28 (0.57) |
| Outpatient Costs, € per PY | |
| All outpatient visits | |
| Mean cost of all-cause visits (SD) | 1028.89 (798.17) |
| Mean cost of MS-related visits (SD) | 431.00 (310.83) |
| GP visits | |
| Mean cost of all-cause GP visits (SD) | 230.68 (116.04) |
| Mean cost of MS-related GP visits (SD) | 206.28 (112.62) |
| Neurologist visits | |
| Mean cost of all-cause visits (SD) | 44.71 (87.60) |
| Mean cost of MS-related visits (SD) | 40.36 (84.05) |
| DMT prescriptions | |
| Mean cost of DMT prescriptions (SD) | 12,718.29 (8933.00) |
| Inpatient Costs, € per PY | |
| Hospitalizations | |
| Mean cost of all-cause admissions (SD) | 1699.37 (3871.59) |
| Mean cost of MS-related admissions (SD) | 1507.24 (3676.63) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghiani, M.; Zhuleku, E.; Dillenseger, A.; Maywald, U.; Fuchs, A.; Wilke, T.; Ziemssen, T. Data Resource Profile: The Multiple Sclerosis Documentation System 3D and AOK PLUS Linked Database (MSDS-AOK PLUS). J. Clin. Med. 2023, 12, 1441. https://doi.org/10.3390/jcm12041441
Ghiani M, Zhuleku E, Dillenseger A, Maywald U, Fuchs A, Wilke T, Ziemssen T. Data Resource Profile: The Multiple Sclerosis Documentation System 3D and AOK PLUS Linked Database (MSDS-AOK PLUS). Journal of Clinical Medicine. 2023; 12(4):1441. https://doi.org/10.3390/jcm12041441
Chicago/Turabian StyleGhiani, Marco, Evi Zhuleku, Anja Dillenseger, Ulf Maywald, Andreas Fuchs, Thomas Wilke, and Tjalf Ziemssen. 2023. "Data Resource Profile: The Multiple Sclerosis Documentation System 3D and AOK PLUS Linked Database (MSDS-AOK PLUS)" Journal of Clinical Medicine 12, no. 4: 1441. https://doi.org/10.3390/jcm12041441