
Controversial Outcomes in Neck Rehabilitation between Surgically and Conservatively Treated Patients—Results of an Observational Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedure
2.2. Outcome Measures
2.2.1. Range of Motion (ROM)
2.2.2. Numeric Pain Rating Scale (NPRS)
2.2.3. Health Assessment Questionnaire (HAQ)
2.2.4. EuroQol—5 Dimensions—5 Levels (EQ-5D-5L)
2.2.5. Neck Disability Index (NDI)
2.3. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Rehabilitation Treatment
3.3. Association of PROMs and ROM
3.4. Mean Changes during Rehabilitation Treatment
3.5. Critical Success Factors for Neck Disability Score at the End of Treatment (T2)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blanpied, P.R.; Gross, A.R.; Elliott, J.M.; Devaney, L.L.; Clewley, D.; Walton, D.M.; Sparks, C.; Robertson, E.K. Neck Pain: Revision 2017. J. Orthop. Sports Phys. Ther. 2017, 47, A1–A83. [Google Scholar] [CrossRef] [Green Version]
- Clarke, M.J.; Schiefer, T.K.; Pichelmann, M.A.; Krauss, W.E. Axial neck pain: A surgeon’s perspective. Clin. Pract. 2011, 8, 763. [Google Scholar] [CrossRef]
- McLean, S.M.; Burton, M.; Bradley, L.; Littlewood, C. Interventions for enhancing adherence with physiotherapy: A systematic review. Man. Ther. 2010, 15, 514–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutting, N.; Mourad, F.; Kranenburg, R.; Wilbrink, W.; Kerry, R.; Taylor, A. What to look out for, what to do, and when: 3 key messages for safely treating neck pain, headache and/or orofacial symptoms in musculoskeletal rehabilitation settings. J. Orthop. Sports Phys. Ther. 2022, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Bowden, R.E.M. Cervical Spondylosis: The Applied Anatomy of the Cervical Spine and Brachial Plexus. Proc. R. Soc. Med. 1966, 59, 1141–1146. [Google Scholar] [CrossRef] [Green Version]
- Recenti, M.; Ricciardi, C.; Edmunds, K.; Jacob, D.; Gambacorta, M.; Gargiulo, P. Testing soft tissue radiodensity parameters interplay with age and self-reported physical activity. Eur. J. Transl. Myol. 2021, 31. [Google Scholar] [CrossRef] [PubMed]
- Hindman, B.J.; Palecek, J.P.; Posner, K.L.; Traynelis, V.C.; Lee, L.A.; Sawin, P.D.; Tredway, T.L.; Todd, M.M.; Domino, K.B. Cervical spinal cord, root, and bony spine injuries: A closed claims analysis. Anesthesiology 2011, 114, 782–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yukawa, Y.; Kato, F.; Suda, K.; Yamagata, M.; Ueta, T. Age-related changes in osseous anatomy, alignment, and range of motion of the cervical spine. Part I: Radiographic data from over 1200 asymptomatic subjects. Eur. Spine J. 2012, 21, 1492–1498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrop, J.S.; Hanna, A.; Silva, M.T.; Sharan, A. Neurological manifestations of cervical spondylosis: An overview of signs, symptoms, and pathophysiology. Neurosurgery 2007, 60, S14–S20. [Google Scholar] [CrossRef]
- Wong, J.J.; Cote, P.; Quesnele, J.J.; Stern, P.J.; Mior, S.A. The course and prognostic factors of symptomatic cervical disc herniation with radiculopathy: A systematic review of the literature. Spine J. 2014, 14, 1781–1789. [Google Scholar] [CrossRef]
- Zielinska, N.; Podgorski, M.; Haladaj, R.; Polguj, M.; Olewnik, L. Risk Factors of Intervertebral Disc Pathology—A Point of View Formerly and Today—A Review. J. Clin. Med. 2021, 10, 409. [Google Scholar] [CrossRef] [PubMed]
- Petersen, J.A.; Brauer, C.; Thygesen, L.C.; Flachs, E.M.; Lund, C.B.; Thomsen, J.F. Prospective, population-based study of occupational movements and postures of the neck as risk factors for cervical disc herniation. BMJ Open 2022, 12, e053999. [Google Scholar] [CrossRef] [PubMed]
- Rao, R. Neck pain, cervical radiculopathy, and cervical myelopathy: Pathophysiology, natural history, and clinical evaluation. J. Bone Jt. Surg. 2002, 84, 1872–1881. [Google Scholar] [CrossRef] [PubMed]
- Fritz, J.M.; Brennan, G.P. Preliminary examination of a proposed treatment-based classification system for patients receiving physical therapy interventions for neck pain. Phys. Ther. 2007, 87, 513–524. [Google Scholar] [CrossRef] [Green Version]
- Engquist, M.; Lofgren, H.; Oberg, B.; Holtz, A.; Peolsson, A.; Soderlund, A.; Vavruch, L.; Lind, B. Factors Affecting the Outcome of Surgical Versus Nonsurgical Treatment of Cervical Radiculopathy: A Randomized, Controlled Study. Spine 2015, 40, 1553–1563. [Google Scholar] [CrossRef] [Green Version]
- Snodgrass, S.J.; Cleland, J.A.; Haskins, R.; Rivett, D.A. The clinical utility of cervical range of motion in diagnosis, prognosis, and evaluating the effects of manipulation: A systematic review. Physiotherapy 2014, 100, 290–304. [Google Scholar] [CrossRef]
- Patrick, D.L.; Deyo, R.A. Generic and disease-specific measures in assessing health status and quality of life. Med. Care 1989, 27, S217–S232. [Google Scholar] [CrossRef]
- Brinker, M.R.; O’Connor, D.P. Stakeholders in outcome measures: Review from a clinical perspective. Clin. Orthop. Relat. Res. 2013, 471, 3426–3436. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, D.M.; Stratford, P.W.; Wessel, J.; Gollish, J.D.; Penney, D. Assessing stability and change of four performance measures: A longitudinal study evaluating outcome following total hip and knee arthroplasty. BMC Musculoskelet. Disord. 2005, 6, 3. [Google Scholar] [CrossRef] [Green Version]
- Bily, W.; Jauker, J.; Nics, H.; Grote, V.; Pirchl, M.; Fischer, M.J. Associations between Patient-Reported and Clinician-Reported Outcome Measures in Patients after Traumatic Injuries of the Lower Limb. Int. J. Environ. Res. Public Health 2022, 19, 3140. [Google Scholar] [CrossRef]
- Zdravkovic, A.; Grote, V.; Pirchl, M.; Stockinger, M.; Crevenna, R.; Fischer, M.J. Comparison of patient- and clinician-reported outcome measures in lower back rehabilitation: Introducing a new integrated performance measure (t2D). Qual. Life Res. 2022, 31, 303–315. [Google Scholar] [CrossRef] [PubMed]
- Bruce, B.; Fries, J. Longitudinal comparison of the Health Assessment Questionnaire (HAQ) and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). Arthritis Rheum. 2004, 51, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Vernon, H.; Mior, S. The Neck Disability Index: A study of reliability and validity. J. Manip. Physiol. Ther. 1991, 14, 409–415. [Google Scholar]
- Bachner, F.; Bobek, J.; Habimana, K.; Ladurner, J.; Lepuschutz, L.; Ostermann, H.; Rainer, L.; Schmidt, A.E.; Zuba, M.; Quentin, W.; et al. Austria: Health System Review. Health Syst. Transit. 2018, 20, 1–254. [Google Scholar]
- Grote, V.; Unger, A.; Bottcher, E.; Muntean, M.; Puff, H.; Marktl, W.; Mur, E.; Kullich, W.; Holasek, S.; Hofmann, P.; et al. General and Disease-Specific Health Indicator Changes Associated with Inpatient Rehabilitation. J. Am. Med. Dir. Assoc. 2020, 21, 2017.e10–2017.e27. [Google Scholar] [CrossRef]
- Grote, V.; Unger, A.; Puff, H.; Böttcher, E. What to Expect: Medical Quality Outcomes and Achievements of a Multidisciplinary Inpatient Musculoskeletal System Rehabilitation. In Physical Therapy Effectiveness; Mario, B.-F., Danúbiada Cunha de, S.-C., Redha, T., Eds.; IntechOpen: London, UK, 2020. [Google Scholar]
- de Koning, C.H.; van den Heuvel, S.P.; Staal, J.B.; Smits-Engelsman, B.C.; Hendriks, E.J. Clinimetric evaluation of active range of motion measures in patients with non-specific neck pain: A systematic review. Eur. Spine J. 2008, 17, 905–921. [Google Scholar] [CrossRef] [Green Version]
- Lemeunier, N.; Jeoun, E.B.; Suri, M.; Tuff, T.; Shearer, H.; Mior, S.; Wong, J.J.; da Silva-Oolup, S.; Torres, P.; D’Silva, C.; et al. Reliability and validity of clinical tests to assess posture, pain location, and cervical spine mobility in adults with neck pain and its associated disorders: Part 4. A systematic review from the cervical assessment and diagnosis research evaluation (CADRE) collaboration. Musculoskelet. Sci. Pract. 2018, 38, 128–147. [Google Scholar] [CrossRef]
- Gajdosik, R.L.; Bohannon, R.W. Clinical measurement of range of motion. Review of goniometry emphasizing reliability and validity. Phys. Ther. 1987, 67, 1867–1872. [Google Scholar] [CrossRef]
- Bogduk, N.; Mercer, S. Biomechanics of the cervical spine. I: Normal kinematics. Clin. Biomech. 2000, 15, 633–648. [Google Scholar] [CrossRef]
- Breivik, H.; Borchgrevink, P.C.; Allen, S.M.; Rosseland, L.A.; Romundstad, L.; Hals, E.K.; Kvarstein, G.; Stubhaug, A. Assessment of pain. Br. J. Anaesth. 2008, 101, 17–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dworkin, R.H.; Turk, D.C.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Katz, N.P.; Kerns, R.D.; Stucki, G.; Allen, R.R.; Bellamy, N.; et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 2005, 113, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Ferreira-Valente, M.A.; Pais-Ribeiro, J.L.; Jensen, M.P. Validity of four pain intensity rating scales. Pain 2011, 152, 2399–2404. [Google Scholar] [CrossRef]
- Fries, J.F.; Spitz, P.; Kraines, R.G.; Holman, H.R. Measurement of patient outcome in arthritis. Arthritis Rheum. 1980, 23, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Buchholz, I.; Janssen, M.F.; Kohlmann, T.; Feng, Y.S. A Systematic Review of Studies Comparing the Measurement Properties of the Three-Level and Five-Level Versions of the EQ-5D. Pharmacoeconomics 2018, 36, 645–661. [Google Scholar] [CrossRef] [Green Version]
- Devlin, N.J.; Brooks, R. EQ-5D and the EuroQol Group: Past, Present and Future. Appl. Health Econ. Health Policy 2017, 15, 127–137. [Google Scholar] [CrossRef] [Green Version]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Fairbank, J.C.; Pynsent, P.B. The Oswestry Disability Index. Spine 2000, 25, 2940–2952; discussion 2952. [Google Scholar] [CrossRef]
- McCarthy, M.J.; Grevitt, M.P.; Silcocks, P.; Hobbs, G. The reliability of the Vernon and Mior neck disability index, and its validity compared with the short form-36 health survey questionnaire. Eur. Spine J. 2007, 16, 2111–2117. [Google Scholar] [CrossRef] [Green Version]
- Wagner, B.; Zdravkovic, A.; Pirchl, M.; Puhan, M.A.; Zwick, R.H.; Grote, V.; Crevenna, R.; Fischer, M.J. Performance Score (T2D)—A New Perspective in the Assessment of Six-Minute Walking Tests in Pulmonary Rehabilitation. Diagnostics 2022, 12, 2402. [Google Scholar] [CrossRef]
- Grote, V.; Pirchl, M.; Fischer, M.J. A new perspective on stratified outcome evaluation. J. Int. Soc. Phys. Rehabil. Med. 2021, 4, 118. [Google Scholar] [CrossRef]
- Grote, V.; Fischer, M.J. Prospects for translational research on outcome measures in musculoskeletal rehabilitation: The search for critical success factors. Eur. J. Transl. Myol. 2022, 32, 81–82. [Google Scholar] [CrossRef]
- Ellis, P.D. The Essential Guide to Effect Sizes; Cambridge University Press: Cambridge, UK, 2012. [Google Scholar]
- Cha, E.D.K.; Lynch, C.P.; Jadczak, C.N.; Mohan, S.; Geoghegan, C.E.; Singh, K. Impact of Depression Severity on Patient-Reported Outcome Measures Following Multilevel Anterior Cervical Discectomy and Fusion. Int. J. Spine Surg. 2022, 16, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Colantonio, D.F.; Nassr, A.; Freedman, B.A.; Elder, B.D.; Bydon, M.; Helgeson, M.D.; Kepler, C.K.; Sebastian, A.S.; Wagner, S.C. The Effect of Preoperative Mental Health Status on Outcomes After Anterior Cervical Discectomy and Fusion. Int. J. Spine Surg. 2022, 16, 233–239. [Google Scholar] [CrossRef] [PubMed]
- De Pauw, R.; Kregel, J.; De Blaiser, C.; Van Akeleyen, J.; Logghe, T.; Danneels, L.; Cagnie, B. Identifying prognostic factors predicting outcome in patients with chronic neck pain after multimodal treatment: A retrospective study. Man. Ther. 2015, 20, 592–597. [Google Scholar] [CrossRef]
- Giesinger, K.; Hamilton, D.F.; Jost, B.; Holzner, B.; Giesinger, J.M. Comparative responsiveness of outcome measures for total knee arthroplasty. Osteoarthr. Cartil. 2014, 22, 184–189. [Google Scholar] [CrossRef] [Green Version]
- Kauther, M.D.; Piotrowski, M.; Hussmann, B.; Lendemans, S.; Wedemeyer, C. Cervical range of motion and strength in 4293 young male adults with chronic neck pain. Eur. Spine J. 2012, 21, 1522–1527. [Google Scholar] [CrossRef] [Green Version]
- Multanen, J.; Hakkinen, A.; Kautiainen, H.; Ylinen, J. Associations of neck muscle strength and cervical spine mobility with future neck pain and disability: A prospective 16-year study. BMC Musculoskelet. Disord. 2021, 22, 911. [Google Scholar] [CrossRef]
- Lee, H.; Hubscher, M.; Moseley, G.L.; Kamper, S.J.; Traeger, A.C.; Mansell, G.; McAuley, J.H. How does pain lead to disability? A systematic review and meta-analysis of mediation studies in people with back and neck pain. Pain 2015, 156, 988–997. [Google Scholar] [CrossRef] [Green Version]
- De Zoete, R.M.; Armfield, N.R.; McAuley, J.H.; Chen, K.; Sterling, M. Comparative effectiveness of physical exercise interventions for chronic non-specific neck pain: A systematic review with network meta-analysis of 40 randomised controlled trials. Br. J. Sports Med. 2021, 55, 730–742. [Google Scholar] [CrossRef]
- Monticone, M.; Cedraschi, C.; Ambrosini, E.; Rocca, B.; Fiorentini, R.; Restelli, M.; Gianola, S.; Ferrante, S.; Zanoli, G.; Moja, L. Cognitive-behavioural treatment for subacute and chronic neck pain. Cochrane Database Syst. Rev. 2015, 2015, CD010664. [Google Scholar] [CrossRef]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Suvinen, T.I.; Reade, P.C.; Kemppainen, P.; Kononen, M.; Dworkin, S.F. Review of aetiological concepts of temporomandibular pain disorders: Towards a biopsychosocial model for integration of physical disorder factors with psychological and psychosocial illness impact factors. Eur. J. Pain 2005, 9, 613–633. [Google Scholar] [CrossRef] [PubMed]
- Means-Christensen, A.J.; Roy-Byrne, P.P.; Sherbourne, C.D.; Craske, M.G.; Stein, M.B. Relationships among pain, anxiety, and depression in primary care. Depress. Anxiety 2008, 25, 593–600. [Google Scholar] [CrossRef] [PubMed]
- de Heer, E.W.; Gerrits, M.M.; Beekman, A.T.; Dekker, J.; van Marwijk, H.W.; de Waal, M.W.; Spinhoven, P.; Penninx, B.W.; van der Feltz-Cornelis, C.M. The association of depression and anxiety with pain: A study from NESDA. PLoS ONE 2014, 9, e106907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cashin, A.G.; McAuley, J.H.; Lamb, S.E.; Lee, H. Disentangling contextual effects from musculoskeletal treatments. Osteoarthr. Cartil. 2021, 29, 297–299. [Google Scholar] [CrossRef]
- Whitney, C.W.; Von Korff, M. Regression to the mean in treated versus untreated chronic pain. Pain 1992, 50, 281–285. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total n = 162 | Cons-Group n = 107 | Op-Group n = 55 | ||||||
|---|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | χ2 | p-Value | |
| Male | 64 | (39.5%) | 41 | (38.3%) | 23 | (41.8%) | 0.186 | 0.66 |
| Female | 98 | (60.5%) | 66 | (61.6%) | 32 | (58.1%) | ||
| Smoker | 43 | (27.2%) | 25 | (24.3%) | 18 | (32.7%) | 1.294 | 0.26 |
| mean | (SD) | mean | (SD) | mean | (SD) | t-value | p-value | |
| Mean age | 52.7 | (8.6) | 52.4 | (8.2) | 53.5 | (9.3) | 0.802 | 0.42 |
| Height (cm) | 170 | (7.4) | 170.6 | (7.6) | 172 | (6.9) | 1.424 | 0.16 |
| Weight (kg) | 77 | (13.9) | 76 | (13.9) | 79 | (13.8) | 0.819 | 0.42 |
| BMI | 26.4 | (4.1) | 26.4 | (4.2) | 26.5 | (3.8) | 0.124 | 0.90 |
| ROM | 58.2 | (16.4) | 61.6 | (14.1) | 51.5 | (18.6) | 3.895 | 0.001 *** |
| NPRS | 5.1 | (2.1) | 5.1 | (2.0) | 5.1 | (2.1) | 0.017 | 0.99 |
| EQ-5D-5L | 8.3 | (2.1) | 8.3 | (1.9) | 8.5 | (2.5) | 0.586 | 0.56 |
| mobility | 1.2 | (0.5) | 1.3 | (0.6) | 1.1 | (0.3) | 2.20 | 0.029 * |
| self-care | 1.1 | (0.4) | 1.0 | (0.2) | 1.1 | (0.6) | 0.86 | 0.39 |
| usual activities | 1.7 | (0.9) | 1.6 | (0.9) | 1.7 | (0.9) | 0.07 | 0.95 |
| pain/discomfort | 2.9 | (0.8) | 3.0 | (0.7) | 2.9 | (0.8) | 0.20 | 0.84 |
| anxiety/depression | 1.5 | (0.9) | 1.4 | (0.6) | 1.7 | (1.1) | 2.04 | 0.045 * |
| HAQ | 0.16 | (0.23) | 0.15 | (0.25) | 0.17 | (0.20) | 0.505 | 0.62 |
| NDI | 29.1 | (14.0) | 28.1 | (13.2) | 30.9 | (15.4) | 1.165 | 0.25 |
| NPRS (T1) | EQ-5D-5L (T1) | HAQ (T1) | ROM (T1) | |
|---|---|---|---|---|
| NDI (T1) | 0.58 *** | 0.74 *** | 0.57 *** | −0.05 |
| NPRS (T1) | - | 0.52 *** | 0.34 *** | −0.07 |
| EQ-5D-5L (T1) | - | - | 0.67 *** | −0.11 |
| HAQ (T1) | - | - | - | −0.07 |
| NPRS (T2-T1) | EQ-5D-5L (T2-T1) | HAQ (T2-T1) | ROM (T2-T1) | |
|---|---|---|---|---|
| NDI (T2-T1) | 0.31 ** | 0.37 *** | 0.24 * | −0.11 |
| NPRS (T2-T1) | - | 0.12 | 0.02 | 0.06 |
| EQ-5D-5L (T2-T1) | - | - | 0.63 *** | −0.17 |
| HAQ (T2-T1) | - | - | - | −0.02 |
| NPRS (T2D) | EQ-5D-5L (T2D) | HAQ (T2D) | ROM (T2D) | |
|---|---|---|---|---|
| NDI (T2D) | 0.52 *** | 0.50 *** | 0.32 ** | −0.33 *** |
| NPRS (T2D) | - | 0.30 ** | 0.16 | −0.12 |
| EQ-5D-5L (T2D) | - | - | 0.61 *** | −0.26 ** |
| HAQ (T2D) | - | - | - | −0.18 |
| T1 | T2 | Time | Time × Group | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | (SD) | Mean | (SD) | Delta | p | η2 | p | η2 | ||
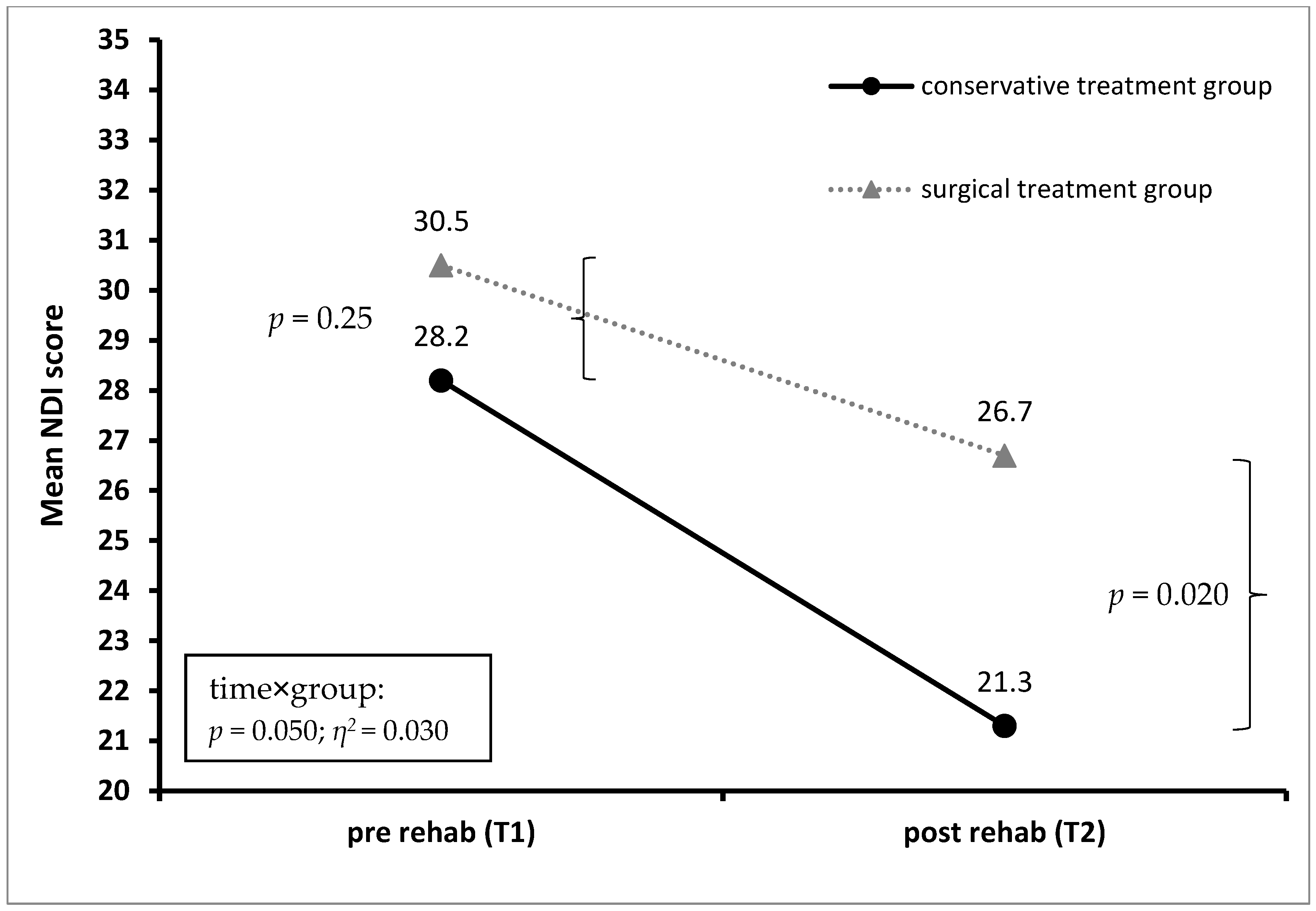
| NDI | Total sample | 28.9 | 13.6 | 22.7 | 12.8 | 6.2 | <0.001 | 0.24 | 0.050 | 0.03 |
| Cons-group | 28.2 | 13.2 | 21.3 | 11.7 | 6.9 | <0.001 | 0.29 | |||
| OP-group | 30.5 | 14.3 | 26.7 | 14.4 | 3.8 | 0.003 | 0.06 | |||
| NPRS | Total sample | 5.1 | 2.1 | 3.7 | 1.9 | 1.4 | <0.001 | 0.33 | 0.12 | 0.02 |
| Cons-group | 5.1 | 2.1 | 3.6 | 1.8 | 1.5 | <0.001 | 0.36 | |||
| OP-group | 5.2 | 2.1 | 4.1 | 1.9 | 1.1 | <0.001 | 0.11 | |||
| HAQ | Total sample | 0.16 | 0.22 | 0.15 | 0.24 | 0.01 | 0.57 | <0.01 | 0.74 | <0.01 |
| Cons-group | 0.16 | 0.25 | 0.15 | 0.28 | 0.01 | 0.42 | <0.01 | |||
| OP-group | 0.16 | 0.16 | 0.15 | 0.15 | 0.01 | 0.88 | <0.01 | |||
| EQ-5D-5L | Total sample | 8.3 | 2.1 | 7.4 | 1.8 | 0.9 | <0.001 | 0.18 | 0.61 | <0.01 |
| Cons-group | 8.3 | 1.9 | 7.4 | 1.6 | 0.9 | <0.001 | 0.17 | |||
| OP-group | 8.4 | 2.4 | 7.4 | 1.6 | 1.0 | 0.002 | 0.06 | |||
| EQ-5D-5L | Total sample | 1.21 | 0.54 | 1.17 | 0.44 | 0.04 | 0.41 | <0.01 | 0.54 | <0.01 |
| mobility | Cons-group | 1.27 | 0.62 | 1.20 | 0.48 | 0.03 | 0.20 | 0.01 | ||
| OP-group | 1.10 | 0.30 | 1.12 | 0.32 | 0.02 | 0.90 | <0.01 | |||
| EQ-5D-5L | Total sample | 1.06 | 0.38 | 1.08 | 0.42 | −0.02 | 0.96 | <0.01 | 0.09 | 0.02 |
| self-care | Cons-group | 1.04 | 0.24 | 1.11 | 0.50 | −0.07 | 0.12 | 0.02 | ||
| OP-group | 1.10 | 0.57 | 1.02 | 0.14 | 0.08 | 0.33 | 0.01 | |||
| EQ-5D-5L | Total sample | 1.63 | 0.86 | 1.47 | 0.78 | 0.16 | 0.035 | 0.03 | 0.90 | <0.01 |
| usual | Cons-group | 1.64 | 0.89 | 1.49 | 0.84 | 0.15 | 0.07 | 0.02 | ||
| activities | OP-group | 1.60 | 0.80 | 1.42 | 0.64 | 0.18 | 0.18 | 0.01 | ||
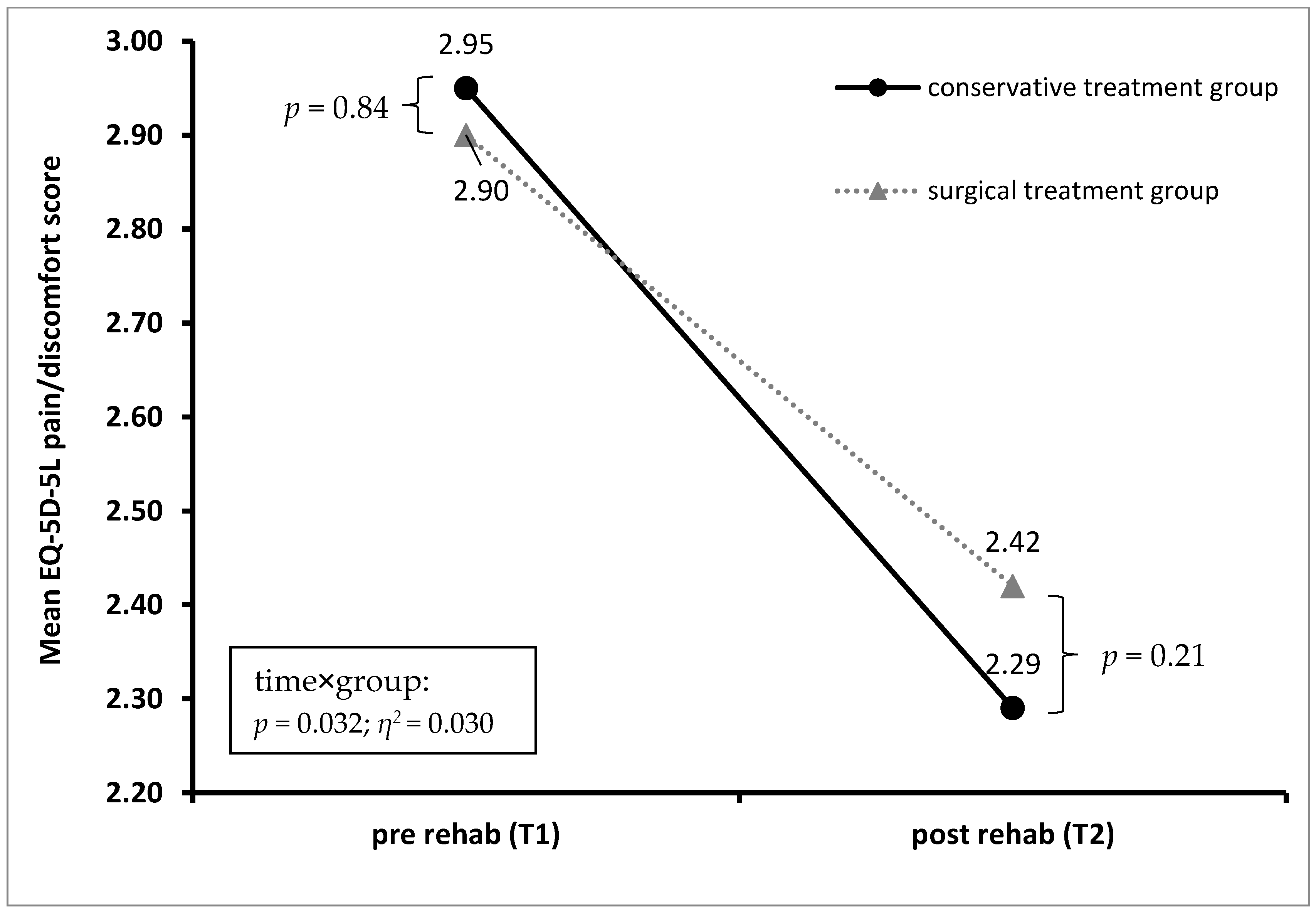
| EQ-5D-5L | Total sample | 2.94 | 0.77 | 2.33 | 0.70 | 0.61 | <0.001 | 0.33 | 0.032 | 0.03 |
| pain/ | Cons-group | 2.95 | 0.73 | 2.29 | 0.69 | 0.66 | <0.001 | 0.38 | ||
| discomfort | OP-group | 2.90 | 0.85 | 2.42 | 0.72 | 0.48 | <0.001 | 0.09 | ||
| EQ-5D-5L | Total sample | 1.49 | 0.83 | 1.30 | 0.57 | 0.19 | 0.007 | 0.05 | 0.98 | <0.01 |
| anxiety/ | Cons-group | 1.39 | 0.64 | 1.22 | 0.44 | 0.17 | 0.016 | 0.04 | ||
| depression | OP-group | 1.69 | 1.11 | 1.46 | 0.75 | 0.23 | 0.10 | 0.02 | ||
| ROM (%) | Total sample | 58.2 | 16.5 | 68.7 | 14.9 | 10.5 | <0.001 | 0.58 | 0.13 | 0.02 |
| Cons-group | 61.6 | 14.1 | 71.5 | 12.5 | 9.9 | <0.001 | 0.47 | |||
| OP-group | 51.1 | 18.7 | 62.9 | 17.8 | 11.8 | <0.001 | 0.38 | |||
| Step 1: Sociodemographic | Step 2: Treatment | Step 3: Baseline PROMs | Step 4: Baseline NDI | |||||
|---|---|---|---|---|---|---|---|---|
| β | p-Value | β | p-Value | β | p-Value | β | p-Value | |
| Sex | 0.18 | 0.019 | 0.08 | 0.32 | 0.06 | 0.37 | 0.03 | 0.66 |
| Age | 0.02 | 0.81 | 0.07 | 0.36 | −0.10 | 0.16 | −0.06 | 0.31 |
| BMI | −0.07 | 0.36 | −0.05 | 0.49 | −0.06 | 0.35 | −0.02 | 0.70 |
| Smoking | −0.03 | 0.65 | −0.07 | 0.33 | −0.12 | 0.07 | −0.07 | 0.21 |
| Nr. medications | 0.35 | <0.001 | 0.22 | 0.007 | 0.14 | 0.06 | 0.07 | 0.28 |
| Psych | - | - | 0.24 | 0.003 | 0.11 | 0.15 | 0.03 | 0.69 |
| Physio | - | - | 0.04 | 0.63 | 0.05 | 0.49 | 0.02 | 0.69 |
| Massage | - | - | −0.02 | 0.77 | 0.00 | 0.99 | 0.04 | 0.44 |
| Physician | - | - | 0.21 | 0.005 | 0.14 | 0.039 | 0.06 | 0.25 |
| Occupational | - | - | 0.06 | 0.39 | −0.02 | 0.72 | −0.01 | 0.84 |
| EQ-5D-5L (T1) | - | - | - | - | 0.14 | 0.13 | −0.08 | 0.32 |
| HAQ (T1) | - | - | - | - | 0.31 | <0.001 | 0.14 | 0.047 |
| NPRS (T1) | - | - | - | - | 0.11 | 0.13 | −0.02 | 0.73 |
| ROM (T1) | - | - | - | - | −0.18 | 0.008 | −0.17 | 0.003 |
| NDI (T1) | - | - | - | - | - | - | 0.66 | <0.001 |
| R2 (Sig. model) | 0.177 | (<0.001) | 0.284 | (<0.001) | 0.480 | (<0.001) | 0.637 | (<0.001) |
| Δ R2 (Sig. of Δ R2) | - | - | 0.107 | (0.001) | 0.196 | (<0.001) | 0.157 | (<0.001) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Missmann, M.; Grote, V.; Riedl, D.; Grenier, J.-P.; Fischer, M.J. Controversial Outcomes in Neck Rehabilitation between Surgically and Conservatively Treated Patients—Results of an Observational Study. J. Clin. Med. 2023, 12, 1004. https://doi.org/10.3390/jcm12031004
Missmann M, Grote V, Riedl D, Grenier J-P, Fischer MJ. Controversial Outcomes in Neck Rehabilitation between Surgically and Conservatively Treated Patients—Results of an Observational Study. Journal of Clinical Medicine. 2023; 12(3):1004. https://doi.org/10.3390/jcm12031004
Chicago/Turabian StyleMissmann, Martin, Vincent Grote, David Riedl, Jean-Pascal Grenier, and Michael J. Fischer. 2023. "Controversial Outcomes in Neck Rehabilitation between Surgically and Conservatively Treated Patients—Results of an Observational Study" Journal of Clinical Medicine 12, no. 3: 1004. https://doi.org/10.3390/jcm12031004