
Picking Up the Threads: Long-Term Outcomes of the Sutured Haemorrhoidopexy: A Retrospective Single-Centre Cohort Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
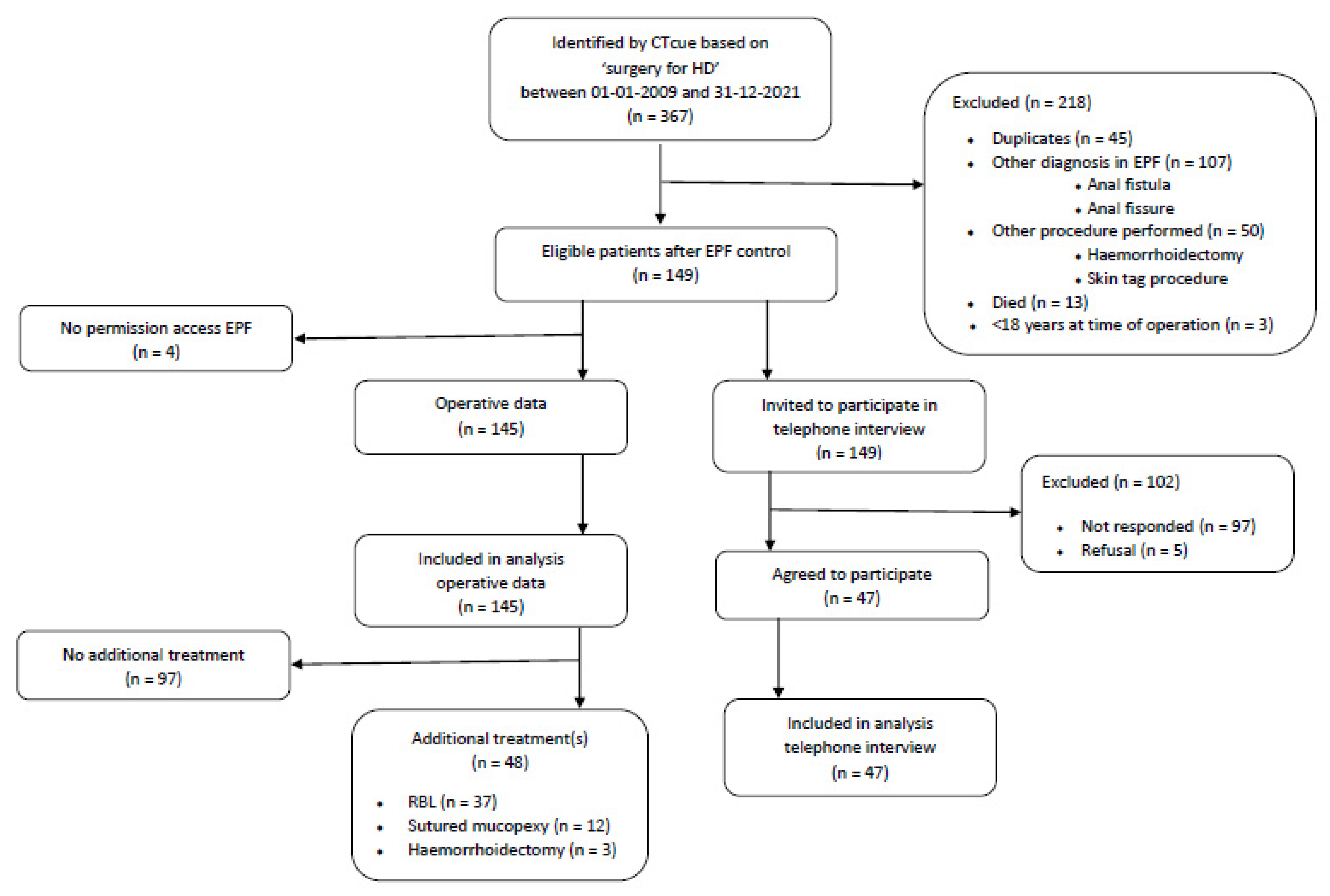
2.1. Patients
2.2. Surgical Procedure
2.3. Outcomes and Instruments
2.3.1. Treatment Characteristics and Perioperative Outcomes
2.3.2. Outcomes According to the Core Outcome Set (COS) for Haemorrhoids
2.3.3. Recurrence and Re-Treatment
2.4. Data Analysis
3. Results
3.1. Patients
3.2. Outcomes
3.2.1. Treatment Characteristics and Perioperative Outcomes
3.2.2. Outcomes According to the Core Outcome Set (COS) for Haemorrhoids
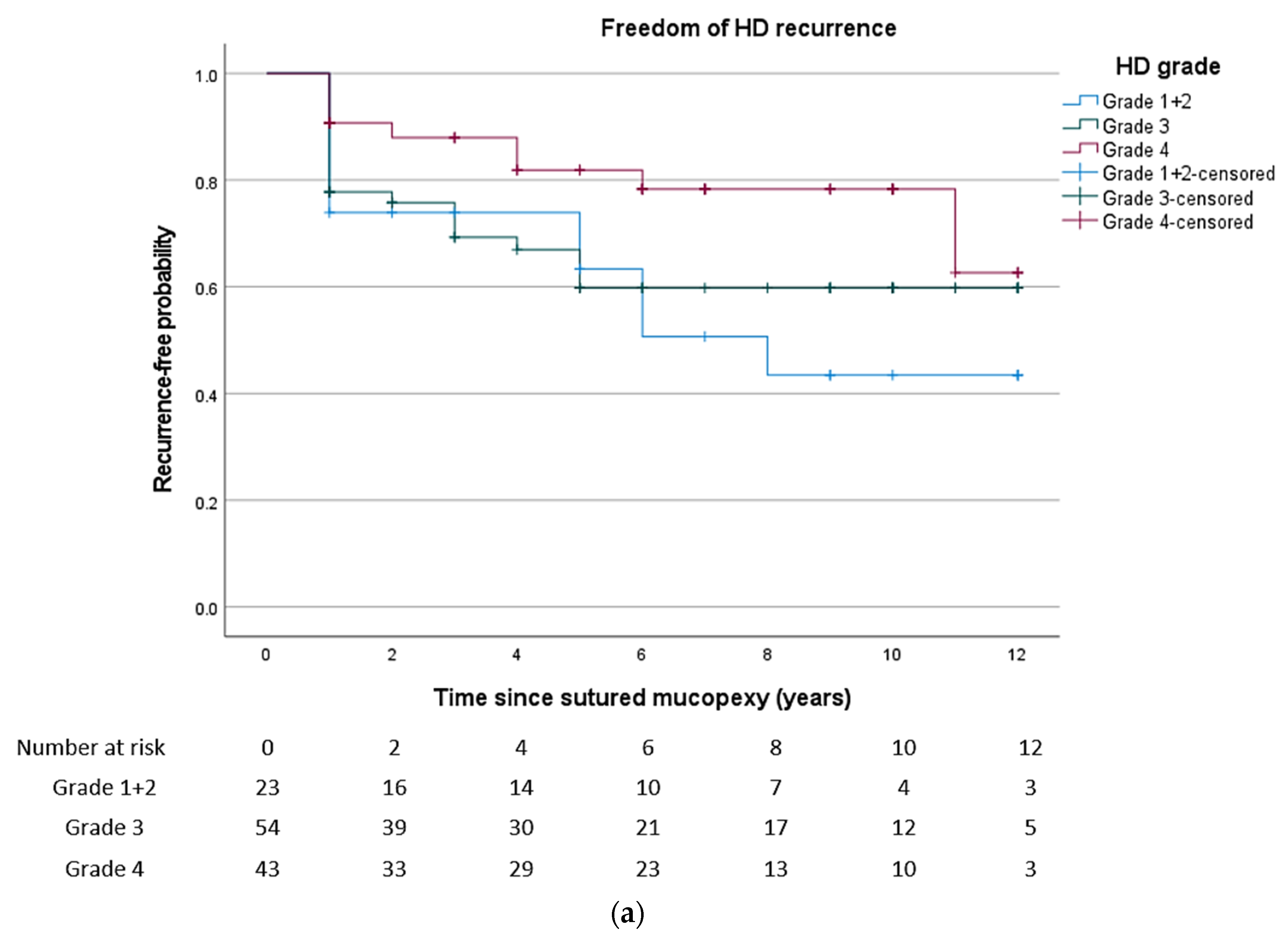
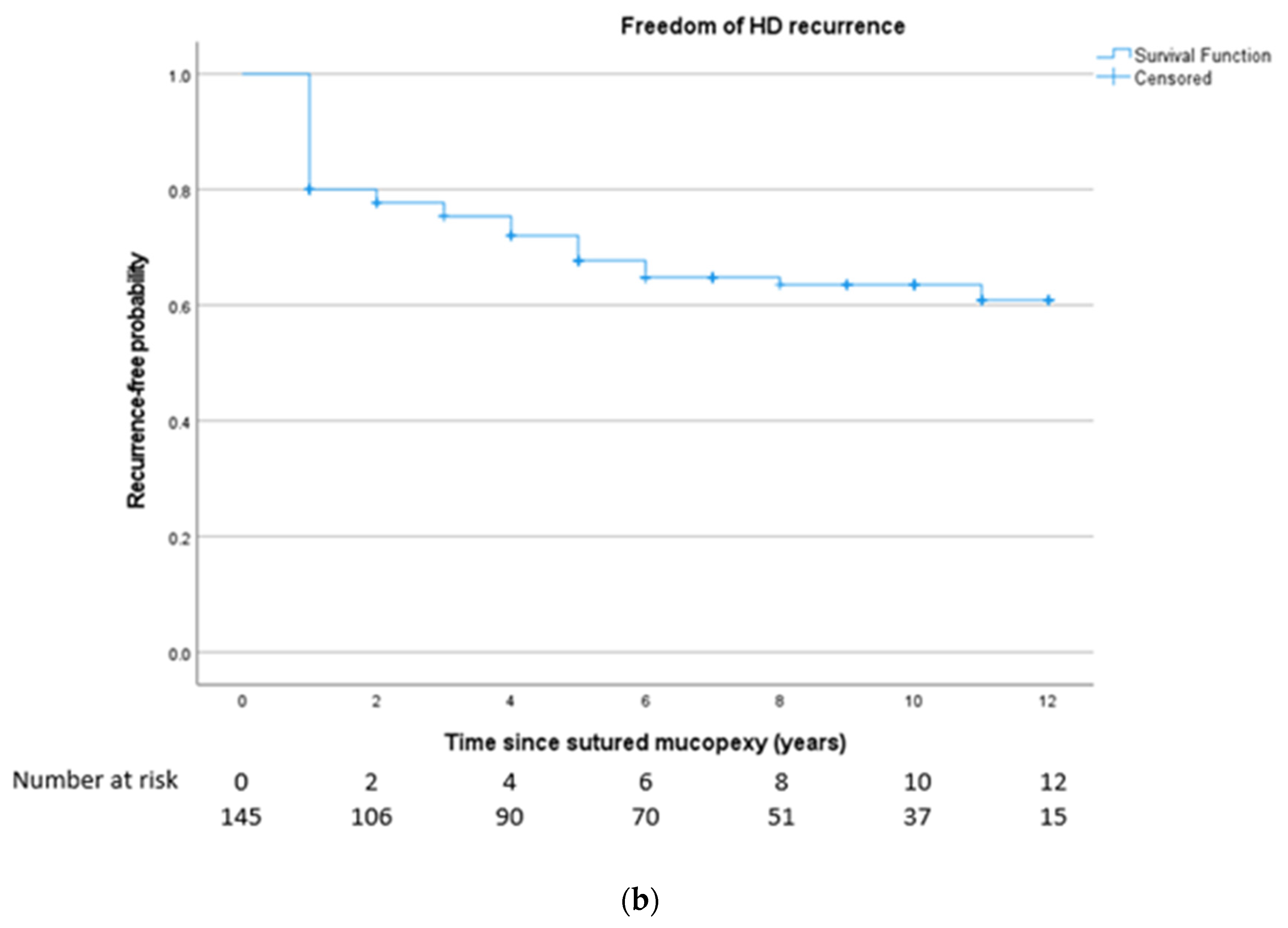
3.2.3. Recurrence and Re-Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Riss, S.; Weiser, F.A.; Schwameis, K.; Riss, T.; Mittlböck, M.; Steiner, G.; Stift, A. The prevalence of hemorrhoids in adults. Int. J. Color. Dis. 2012, 27, 215–220. [Google Scholar] [CrossRef]
- Van Tol, R.R.; Kleijnen, J.; Watson, A.J.M.; Jongen, J.; Altomare, D.F.; Qvist, N.; Higuero, T.; Muris, J.W.M.; Breukink, S.O.; Henquet, C.J.M. European Society of ColoProctology: Guideline for haemorrhoidal disease. Color. Dis. 2020, 22, 650–662. [Google Scholar]
- Davis, B.R.; Lee-Kong, S.A.; Migaly, J.; Feingold, D.L.; Steele, S.R. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids. Dis. Colon Rectum 2018, 61, 284–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pata, F.; Gallo, G.; Pellino, G.; Vigorita, V.; Podda, M.; Di Saverio, S.; D’Ambrosio, G.; Sammarco, G. Evolution of Surgical Management of Hemorrhoidal Disease: An Historical Overview. Front. Surg. 2021, 8, 727059. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.J.; Hudson, J.; Wood, J.; Kilonzo, M.; Brown, S.R.; McDonald, A.; Norrie, J.; Bruhn, H.; Cook, J.A.; eTHoS Study Group. Comparison of stapled haemorrhoidopexy with traditional excisional surgery for haemorrhoidal disease (eTHoS): A pragmatic, multicentre, randomised controlled trial. Lancet 2016, 388, 2375–2385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johannsson, H.O.; Pahlman, L.; Graf, W. Functional and structural abnormalities after milligan hemorrhoidectomy: A comparison with healthy subjects. Dis. Colon Rectum 2013, 56, 903–908. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.R.; Tiernan, J.P.; Watson, A.J.; Biggs, K.; Shephard, N.; Wailoo, A.J.; Bradburn, M.; Alshreef, A.; Hind, D.; HubBLe Study team. Haemorrhoidal artery ligation versus rubber band ligation for the management of symptomatic second-degree and third-degree haemorrhoids (HubBLe): A multicentre, open-label, randomised controlled trial. Lancet 2016, 388, 356–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cotton, M.H. Pelvic sepsis after stapled hemorrhoidectomy. J. Am. Coll. Surg. 2005, 200, 983. [Google Scholar] [CrossRef]
- Kilonzo, M.M.; Brown, S.R.; Bruhn, H.; Cook, J.A.; Hudson, J.; Norrie, J.; Watson, A.J.; Wood, J. Cost Effectiveness of Stapled Haemorrhoidopexy and Traditional Excisional Surgery for the Treatment of Haemorrhoidal Disease. Pharm. Open 2018, 2, 271–280. [Google Scholar] [CrossRef] [Green Version]
- Ripetti, V.; Caricato, M.; Arullani, A. Rectal perforation, retropneumoperitoneum, and pneumomediastinum after stapling procedure for prolapsed hemorrhoids: Report of a case and subsequent considerations. Dis. Colon Rectum 2002, 45, 268–270. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.Y.; Fu, Y.J.; Li, G.M.; Xiao, G.Z.; Guo, Z.W.; Ren, D.L.; Cao, B.; Lin, H.C. Mucocele: A rare complication following stapled haemorrhoidopexy. BMC Surg. 2022, 22, 298. [Google Scholar] [CrossRef]
- Aigner, F.; Kronberger, I.; Oberwalder, M.; Loizides, A.; Ulmer, H.; Gruber, L.; Pratschke, J.; Peer, S.; Gruber, H. Doppler-guided haemorrhoidal artery ligation with suture mucopexy compared with suture mucopexy alone for the treatment of Grade III haemorrhoids: A prospective randomized controlled trial. Color. Dis. 2016, 18, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Alemrajabi, M.; Akbari, A.; Sohrabi, S.; Rezazadehkermani, M.; Moradi, M.; Agah, S.; Masoodi, M. Simple mucopexy and hemorrhoidal arterial ligation with and without Doppler guide: A randomized clinical trial for short-term outcome. Ann. Coloproctol. 2022; Epub ahead of print. [Google Scholar] [CrossRef]
- Sun, Z.; Migaly, J. Review of Hemorrhoid Disease: Presentation and Management. Clin. Colon Rectal Surg. 2016, 29, 22–29. [Google Scholar] [PubMed] [Green Version]
- Pakravan, F.; Helmes, C.; Baeten, C. Transanal open hemorrhoidopexy. Dis. Colon Rectum 2009, 52, 503–506. [Google Scholar] [CrossRef] [PubMed]
- Pakravan, F.H.C.; Alldinger, I. Transanale offene Hämorrhoidopexie. Coloproctology 2018, 40, 352–356. [Google Scholar] [CrossRef]
- Van Tol, R.R.; Kimman, M.L.; Melenhorst, J.; Stassen, L.P.S.; Dirksen, C.D.; Breukink, S.O.; Steering Group; Salat, A.; Ommer, A.; Giordano, P.; et al. European Society of Coloproctology Core Outcome Set for haemorrhoidal disease: An international Delphi study among healthcare professionals. Color. Dis. 2019, 21, 570–580. [Google Scholar]
- Jorge, J.M.; Wexner, S.D. Etiology and management of fecal incontinence. Dis. Colon Rectum 1993, 36, 77–97. [Google Scholar] [CrossRef]
- Rothbarth, J.; Bemelman, W.A.; Meijerink, W.J.; Stiggelbout, A.M.; Zwinderman, A.H.; Buyze-Westerweel, M.E.; Delemarre, J.B. What is the impact of fecal incontinence on quality of life? Dis. Colon Rectum 2001, 44, 67–71. [Google Scholar] [CrossRef]
- Kuiper, S.Z.; Kimman, M.L.; Van Tol, R.R.; Waardenburg, S.F.; Van Kuijk, S.M.; Dirksen, C.D.; Breukink, S.O. Patient reported outcome measure-haemorrhoidal impact and satisfaction score (PROM-HISS): Development, reliability and construct validity. Color. Dis. 2022, 24, 992–999. [Google Scholar] [CrossRef]
- Zhai, M.; Zhang, Y.A.; Wang, Z.Y.; Sun, J.H.; Wen, J.; Zhang, Q.; Li, J.D.; Wu, Y.Z.; Zhou, F.; Xu, H.L. A Randomized Controlled Trial Comparing Suture-Fixation Mucopexy and Doppler-Guided Hemorrhoidal Artery Ligation in Patients with Grade III Hemorrhoids. Gastroenterol. Res. Pract. 2016, 2016, 8143703. [Google Scholar] [CrossRef] [Green Version]
- Johanson, J.F.; Sonnenberg, A. The prevalence of hemorrhoids and chronic constipation. An epidemiologic study. Gastroenterology 1990, 98, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, P.; Regnier, C.; Goron, F.; Salmat, G. The prevalence, characteristics and treatment of hemorrhoidal disease: Results of an international web-based survey. J. Comp. Eff. Res. 2020, 9, 1219–1232. [Google Scholar] [CrossRef] [PubMed]
- De Robles, M.S.; Young, C.J. Surgical technique is the main predictor of recurrence in the management of haemorrhoids. ANZ J. Surg. 2021, 91, 1854–1858. [Google Scholar] [CrossRef]
- Holzheimer, R.G. Hemorrhoidectomy: Indications and risks. Eur. J. Med. Res. 2004, 9, 18–36. [Google Scholar] [PubMed]
- Bouchard, D.; Abramowitz, L.; Castinel, A.; Suduca, J.M.; Staumont, G.; Soudan, D.; Devulder, F.; Pigot, F.; Varastet, M.; Ganansia, R.; et al. One-year outcome of haemorrhoidectomy: A prospective multicentre French study. Color. Dis. 2013, 15, 719–726. [Google Scholar] [CrossRef]
- Sielezneff, I.; Salle, E.; Lecuyer, J.; Brunet, C.; Sarles, J.C.; Sastre, B. Early postoperative morbidity after hemorrhoidectomy using the Milligan-Morgan technic. A retrospective studies of 1134 cases. J. Chir. 1997, 134, 243–247. [Google Scholar]
- Simillis, C.; Thoukididou, S.N.; Slesser, A.A.; Rasheed, S.; Tan, E.; Tekkis, P.P. Systematic review and network meta-analysis comparing clinical outcomes and effectiveness of surgical treatments for haemorrhoids. Br. J. Surg. 2015, 102, 1603–1618. [Google Scholar] [CrossRef]
- Ho, Y.H.; Seow-Choen, F.; Goh, H.S. Haemorrhoidectomy and disordered rectal and anal physiology in patients with prolapsed haemorrhoids. Br. J. Surg. 1995, 82, 596–598. [Google Scholar] [CrossRef]
- Johannsson, H.O.; Pahlman, L.; Graf, W. Randomized clinical trial of the effects on anal function of Milligan-Morgan versus Ferguson haemorrhoidectomy. Br. J. Surg. 2006, 93, 1208–1214. [Google Scholar] [CrossRef]
- Lohsiriwat, V. Treatment of hemorrhoids: A coloproctologist’s view. World J. Gastroenterol. 2015, 21, 9245–9252. [Google Scholar] [CrossRef]
- Gupta, P.J.; Kalaskar, S. Ligation and mucopexy for prolapsing hemorrhoids—A ten year experience. Ann. Surg. Innov. Res. 2008, 2, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohsiriwat, D.; Lohsiriwat, V. Outpatient hemorrhoidectomy under perianal anesthetics infiltration. J. Med. Assoc. Thailand 2005, 88, 1821–1824. [Google Scholar]
- Lohsiriwat, V.; Jitmungngan, R. Strategies to Reduce Post-Hemorrhoidectomy Pain: A Systematic Review. Medicina 2022, 58, 418. [Google Scholar] [CrossRef] [PubMed]
- Yeo, D.; Tan, K.Y. Hemorrhoidectomy—Making sense of the surgical options. World J. Gastroenterol. 2014, 20, 16976–16983. [Google Scholar] [CrossRef] [PubMed]
- Talari, K.; Goyal, M. Retrospective studies—Utility and caveats. J. R. Coll. Physicians Edinb. 2020, 50, 398–402. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 145) | Subgroup 1 (n = 50) |
|---|---|---|
| Female, n (%) | 70 (48.3%) | 21 (42.0%) |
| Age, mean, ±SD, y | 61 ± 12.8 | 62 ± 11 |
| Years between surgery and follow-up, median (IQR), y | 9 [5,6,7,8,9,10,11] | 7 [3,4,5,6,7,8,9,10] |
| Goligher’s classification, n (%) | ||
| Grade I + II | 23 (15.9%) | 5 (10.0%) |
| Grade III | 54 (37.2%) | 18 (36.0%) |
| Grade IV | 43 (29.7%) | 18 (36.0%) |
| Unknown | 25 (17.2%) | 9 (18.0%) |
| Characteristics | Outcome |
|---|---|
| Number of sutures | 3 [1,2,3,4,5,6,7,8] |
| Operation time, min | 18.1 ± 7.7 |
| Perioperative complications | 4 (2.8%) |
| Analgesics needed | 45 (31.0%) |
| Type of analgesic1 | |
| Acetaminophen | 25 (32.1%) |
| Non-steroidal analgesics | 23 (29.5%) |
| Oxycodone | 27 (34.6%) |
| Other | 3 (3.8%) |
| Hospital admission, days | 1 [1,2,3] |
| Blood Loss | Pain | Swelling | Itching | Fluid Loss | |
|---|---|---|---|---|---|
| Not at all | 31 (62.0%) | 31 (62.0%) | 22 (44.0%) | 37 (74%) | 38 (76.0%) |
| Very little | 9 (18.0%) | 7 (14.0%) | 7 (14.0%) | 9 (18.0%) | 5 (10.0%) |
| Somewhat | 7 (14.0%) | 4 (8.0%) | 10 (20.0%) | 3 (6.0%) | 3 (6.0%) |
| Quite a bit | 3 (6.0%) | 5 (10.0%) | 9 (18.0%) | 1 (2.0%) | 4 (8.0%) |
| A lot | 0 (0.0%) | 3 (6.0%) | 2 (4.0%) | 0 (0.0%) | 0 (0.0%) |
| Grade HD | (n = 145) | Recurrence |
|---|---|---|
| Grade I + II | 23 | 11 (47.8%) |
| Grade III | 54 | 20 (37.0%) |
| Grade IV | 43 | 9 (20.9%) |
| Unknown | 25 | 9 (36.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuiper, S.Z.; Van Dam, K.A.M.; Kimman, M.L.; Mitalas, L.; Koot, P.G.M.; Melenhorst, J.; Van Kuijk, S.M.J.; Dirksen, C.D.; Breukink, S.O. Picking Up the Threads: Long-Term Outcomes of the Sutured Haemorrhoidopexy: A Retrospective Single-Centre Cohort Study. J. Clin. Med. 2023, 12, 391. https://doi.org/10.3390/jcm12010391
Kuiper SZ, Van Dam KAM, Kimman ML, Mitalas L, Koot PGM, Melenhorst J, Van Kuijk SMJ, Dirksen CD, Breukink SO. Picking Up the Threads: Long-Term Outcomes of the Sutured Haemorrhoidopexy: A Retrospective Single-Centre Cohort Study. Journal of Clinical Medicine. 2023; 12(1):391. https://doi.org/10.3390/jcm12010391
Chicago/Turabian StyleKuiper, Sara Z., Kayleigh A. M. Van Dam, Merel L. Kimman, Litza Mitalas, Paula G. M. Koot, Jarno Melenhorst, Sander M. J. Van Kuijk, Carmen D. Dirksen, and Stephanie O. Breukink. 2023. "Picking Up the Threads: Long-Term Outcomes of the Sutured Haemorrhoidopexy: A Retrospective Single-Centre Cohort Study" Journal of Clinical Medicine 12, no. 1: 391. https://doi.org/10.3390/jcm12010391