

Selective Decontamination of the Digestive Tract in Pancreatic Head Resections—A Propensity Score-Matched Analysis
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Basic Study Characteristics
2.2. Preoperative Selective Decontamination of the Digestive Tract
2.3. Additional Antibiotic Application and Intraoperative Bile Smear Test
2.4. Postoperative Management
2.5. Primary Endpoint
2.6. Secondary Endpoint
2.7. Statistical Analysis
3. Results
3.1. Description of the Study Cohort
3.2. Primary Endpoint: Intraoperative Bile Duct Smear Test/Bacterial Differentiation
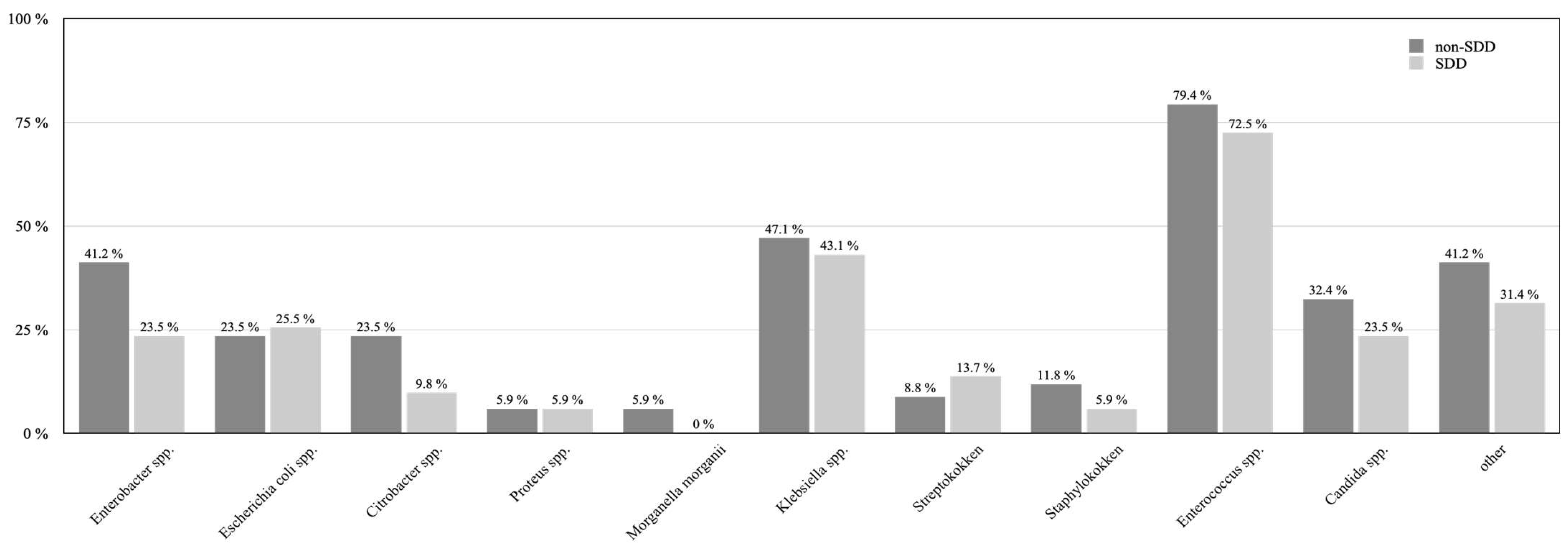
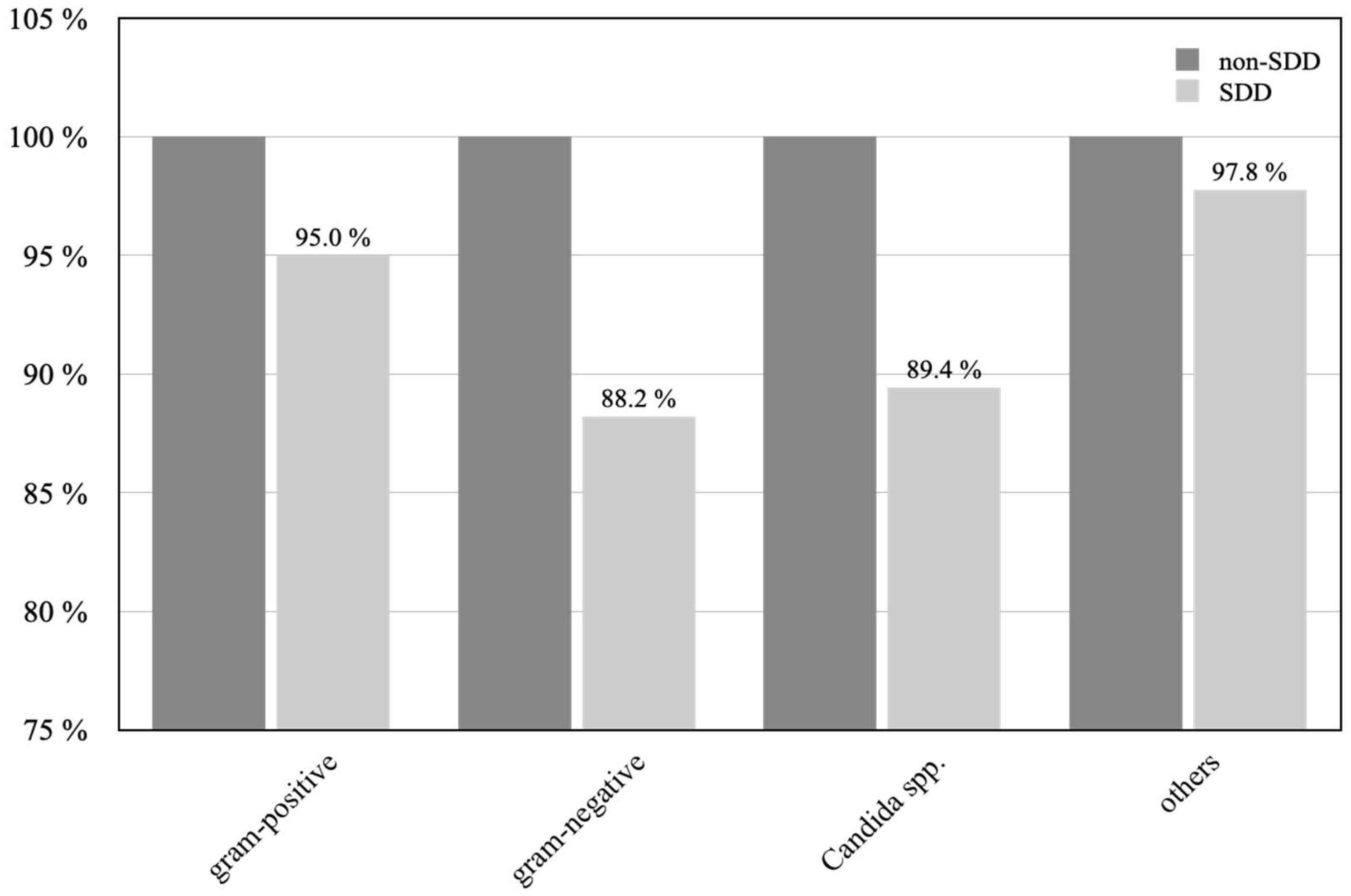
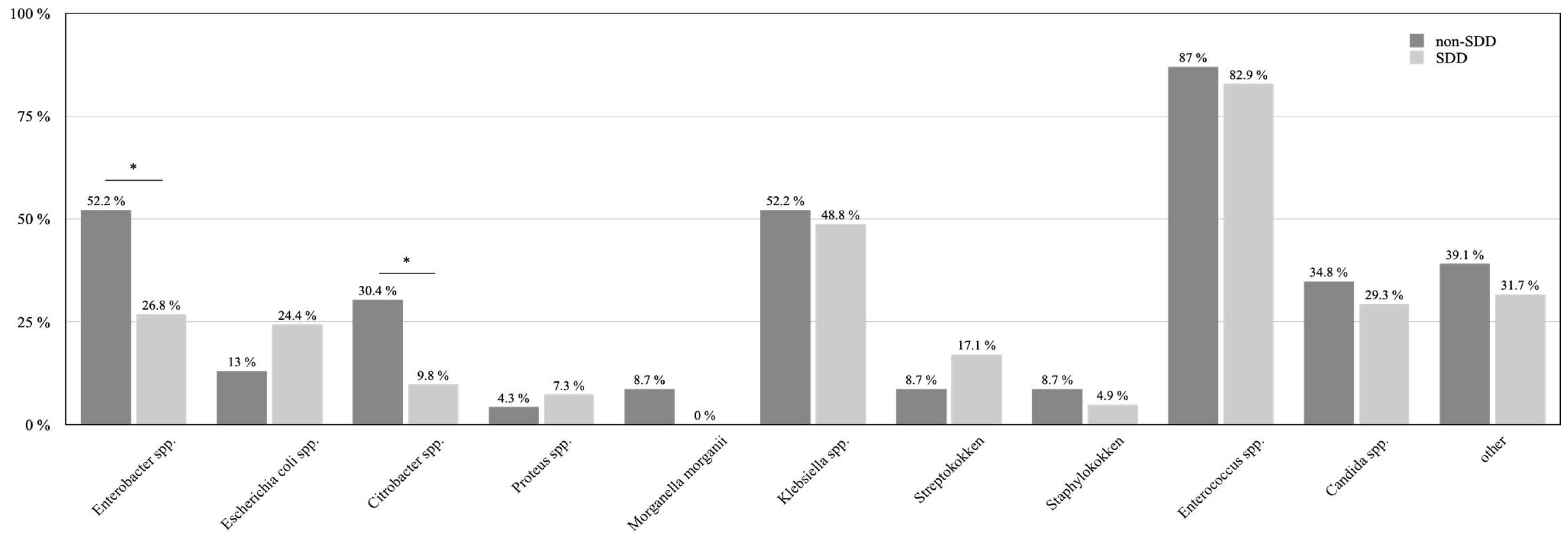
3.3. Bacterial Load and Bacterial Differentiation
3.4. Intraoperative Bile Duct Smear Test of Stent Patients
3.5. Outcome Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ferrie, S.; Webster, A.; Wu, B.; Tan, C.; Carey, S. Gastrointestinal surgery and the gut microbiome: A systematic literature review. Eur. J. Clin. Nutr. 2021, 75, 12–25. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.S.; Graham, L.A.; Chu, D.I.; Cannon, J.A.; Hawn, M.T. Oral Antibiotic Bowel Preparation Significantly Reduces Surgical Site Infection Rates and Readmission Rates in Elective Colorectal Surgery. Ann. Surg. 2015, 261, 1034–1040. [Google Scholar] [CrossRef] [PubMed]
- Scarborough, J.E.; Mantyh, C.R.; Sun, Z.; Migaly, J. Combined Mechanical and Oral Antibiotic Bowel Preparation Reduces Incisional Surgical Site Infection and Anastomotic Leak Rates after Elective Colorectal Resection: An Analysis of Colectomy-Targeted ACS NSQIP. Ann. Surg. 2015, 262, 331–337. [Google Scholar] [CrossRef]
- Kiran, R.P.; Murray, A.C.; Chiuzan, C.; Estrada, D.; Forde, K. Combined preoperative mechanical bowel preparation with oral antibiotics significantly reduces surgical site infection, anastomotic leak, and ileus after colorectal surgery. Ann. Surg. 2015, 262, 416–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Althumairi, A.A.; Canner, J.K.; Pawlik, T.M.; Schneider, E.; Nagarajan, N.; Safar, B.; Efron, J.E. Benefits of Bowel Preparation Beyond Surgical Site Infection: A Retrospective Study. Ann. Surg. 2016, 264, 1051–1057. [Google Scholar] [CrossRef]
- Ahola, R.; Sand, J.; Laukkarinen, J. Centralization of Pancreatic Surgery Improves Results: Review. Scand. J. Surg. 2020, 109, 4–10. [Google Scholar] [CrossRef] [Green Version]
- Maatman, T.K.; Weber, D.J.; Qureshi, B.; Ceppa, E.P.; Nakeeb, A.; Schmidt, C.M.; Zyromski, N.J.; House, M.G. Does the Microbiology of Bactibilia Drive Postoperative Complications after Pancreatoduodenectomy? J. Gastrointest. Surg. 2020, 24, 2544–2550. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [Green Version]
- Keats, A.S. The ASA classification of physical status—A recapitulation. Anesthesiology 1978, 49, 233–236. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Bassi, C.; Marchegiani, G.; Dervenis, C.; Sarr, M.; Abu Hilal, M.; Adham, M.; Allen, P.; Andersson, R.; Asbun, H.J.; Besselink, M.G.; et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 Years after. Surgery 2017, 161, 584–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wente, M.N.; Bassi, C.; Dervenis, C.; Fingerhut, A.; Gouma, D.J.; Izbicki, J.R.; Neoptolemos, J.P.; Padbury, R.T.; Sarr, M.G.; Traverso, L.W.; et al. Delayed gastric emptying (DGE) after pancreatic surgery: A suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2007, 142, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Wente, M.N.; Veit, J.A.; Bassi, C.; Dervenis, C.; Fingerhut, A.; Gouma, D.J.; Izbicki, J.R.; Neoptolemos, J.P.; Padbury, R.T.; Sarr, M.G.; et al. Postpancreatectomy hemorrhage (PPH): An International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery 2007, 142, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Taylor, E.W.; Lindsay, G. Selective decontamination of the colon before elective colorectal surgery. West of Scotland Surgical Infection Study Group. World J. Surg. 1994, 18, 926–931. [Google Scholar] [CrossRef]
- Schardey, H.M.; Wirth, U.; Strauss, T.; Kasparek, M.S.; Schneider, D.; Jauch, K.W. Prevention of anastomotic leak in rectal cancer surgery with local antibiotic decontamination: A prospective, randomized, double-blind, placebo-controlled single center trial. Int. J. Color. Dis. 2020, 35, 847–857. [Google Scholar] [CrossRef]
- Schardey, H.M.; Joosten, U.; Finke, U.; Staubach, K.H.; Schauer, R.; Heiss, A.; Kooistra, A.; Rau, H.G.; Nibler, R.; Ludeling, S.; et al. The prevention of anastomotic leakage after total gastrectomy with local decontamination. A prospective, randomized, double-blind, placebo-controlled multicenter trial. Ann. Surg. 1997, 225, 172–180. [Google Scholar] [CrossRef]
- Scheufele, F.; Schirren, R.; Friess, H.; Reim, D. Selective decontamination of the digestive tract in upper gastrointestinal surgery: Systematic review with meta-analysis of randomized clinical trials. BJS Open 2020, 4, 1015–1021. [Google Scholar] [CrossRef]
- Alverdy, J.C.; Hyoju, S.K.; Weigerinck, M.; Gilbert, J.A. The gut microbiome and the mechanism of surgical infection. Br. J. Surg. 2017, 104, e14–e23. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, F.C.F.; Brenner, T.; Uhle, F.; Loesch, S.; Hackert, T.; Ulrich, A.; Hofer, S.; Dalpke, A.H.; Weigand, M.A.; Boutin, S. Gut microbiome patterns correlate with higher postoperative complication rates after pancreatic surgery. BMC Microbiol. 2019, 19, 42. [Google Scholar] [CrossRef] [Green Version]
- Gesualdo, M.; Rizzi, F.; Bonetto, S.; Rizza, S.; Cravero, F.; Saracco, G.M.; De Angelis, C.G. Pancreatic Diseases and Microbiota: A Literature Review and Future Perspectives. J. Clin. Med. 2020, 9, 3535. [Google Scholar] [CrossRef]
- Abis, G.S.A.; Stockmann, H.B.A.C.; Bonjer, H.J.; van Veenendaal, N.; van Doorn-Schepens, M.L.M.; Budding, A.E.; Wilschut, J.A.; van Egmond, M.; Oosterling, S.J.; Abis, G.S.A.; et al. Randomized clinical trial of selective decontamination of the digestive tract in elective colorectal cancer surgery (SELECT trial). Br. J. Surg. 2019, 106, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Langheinrich, M.; Wirtz, S.; Kneis, B.; Gittler, M.M.; Tyc, O.; Schierwagen, R.; Brunner, M.; Krautz, C.; Weber, G.F.; Pilarsky, C.; et al. Microbiome Patterns in Matched Bile, Duodenal, Pancreatic Tumor Tissue, Drainage, and Stool Samples: Association with Preoperative Stenting and Postoperative Pancreatic Fistula Development. J. Clin. Med. 2020, 9, 2785. [Google Scholar] [CrossRef] [PubMed]
- Kikuyama, M.; Sato, T.; Kurokami, T.; Ota, Y.; Yokoi, Y. Pancreatic Juice Culture in Acute Pancreatitis and Other Pancreatic Disorders. J. Pancreas. 2016, 17, 553–558. [Google Scholar]
- Rogers, M.B.; Aveson, V.; Firek, B.; Yeh, A.; Brooks, B.; Brower-Sinning, R.; Steve, J.; Banfield, J.F.; Zureikat, A.; Hogg, M.; et al. Disturbances of the Perioperative Microbiome Across Multiple Body Sites in Patients Undergoing Pancreaticoduodenectomy. Pancreas 2017, 46, 260–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheufele, F.; Aichinger, L.; Jager, C.; Demir, I.E.; Schorn, S.; Sargut, M.; Erkan, M.; Kleeff, J.; Friess, H.; Ceyhan, G.O. Effect of preoperative biliary drainage on bacterial flora in bile of patients with periampullary cancer. Br. J. Surg. 2017, 104, e182–e188. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.J.; Ho, T.W.; Wu, C.H.; Kuo, T.C.; Yang, C.Y.; Wu, J.M.; Tien, Y.W. Specific Bile Microorganisms Caused by Intra-Abdominal Abscess on Pancreaticoduodenectomy Patients: A Retrospective Cohort Study. Curr. Oncol. 2021, 29, 111–121. [Google Scholar] [CrossRef]
- Heckler, M.; Mihaljevic, A.L.; Winter, D.; Zhou, Z.; Liu, B.; Tanaka, M.; Heger, U.; Michalski, C.W.; Buchler, M.W.; Hackert, T. Escherichia coli Bacterobilia Is Associated with Severe Postoperative Pancreatic Fistula after Pancreaticoduodenectomy. J. Gastrointest. Surg. 2020, 24, 1802–1808. [Google Scholar] [CrossRef]
- Oehme, F.; Hempel, S.; Pecqueux, M.; Mussle, B.; Hau, H.M.; Teske, C.; von Bechtolsheim, F.; Seifert, L.; Distler, M.; Welsch, T.; et al. Short-term preoperative drainage is associated with improved postoperative outcomes compared to that of long-term biliary drainage in pancreatic surgery. Langenbeck’s Arch. Surg. 2021, 407, 1055–1063. [Google Scholar] [CrossRef]
- Fang, Y.; Gurusamy, K.S.; Wang, Q.; Davidson, B.R.; Lin, H.; Xie, X.; Wang, C. Meta-analysis of randomized clinical trials on safety and efficacy of biliary drainage before surgery for obstructive jaundice. Br. J. Surg. 2013, 100, 1589–1596. [Google Scholar] [CrossRef]
- Coppola, A.; La Vaccara, V.; Farolfi, T.; Fiore, M.; Cascone, C.; Ramella, S.; Spoto, S.; Ciccozzi, M.; Angeletti, S.; Coppola, R.; et al. Different Biliary Microbial Flora Influence Type of Complications after Pancreaticoduodenectomy: A Single Center Retrospective Analysis. J. Clin. Med. 2021, 10, 2180. [Google Scholar] [CrossRef]
- Mussle, B.; von Bechtolsheim, F.; Marx, C.; Oehme, F.; Bogner, A.; Hempel, S.; Kahlert, C.; Distler, M.; Weitz, J.; Welsch, T. Antibiotic resistance patterns of bacterial bile cultures during pancreatic surgery—A single center analysis and systematic review. Langenbeck’s Arch. Surg. 2022, 407, 2777–2788. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Overall | Non-SDD | SDD | p Value | |
|---|---|---|---|---|
| patients [n (%)] | 200 | 100 (50) | 100 (50) | |
| sex [n (%)] | ||||
| m | 122 (61) | 61 (61) | 61 (61) | 1 |
| w | 78 (39) | 39 (39) | 39 (39) | |
| age [years] (IQR) | 65.3 (56.9–75) | 65.3 (56.9–73.6) | 66 (56.3–76) | 0.91 |
| median BMI [kg/m²] (IQR) | 25 (22.6–28) | 25.2 (23.6–28.4) | 24.7 (22.2–27.4) | 0.07 |
| smoking [n (%)] | 59 (29.5) | 27 (27) | 32 (32) | 0.44 |
| ASA score [n (%)] | ||||
| 1 | 6 (3) | 3 (3) | 3 (3) | 0.24 |
| 2 | 77 (38.5) | 44 (44) | 33 (33) | |
| 3 | 114 (57) | 52 (52) | 62 (62) | |
| 4 | 2 (1) | 0 | 2 (2) | |
| diabetes [n (%)] | 70 (35) | 36 (36) | 34 (34) | 0.76 |
| insulin-dependent diabetes (IDDM) [n (%)] | 46 (23) | 22 (22) | 24 (24) | 0.74 |
| preoperative biliary drainage [n (%)] | 81 (40.5) | 38 (38) | 43 (43) | 0.47 |
| histopathological analysis [n (%)] | ||||
| malignancy | 142 (71) | 68 (68) | 74 (74) | 0.08 |
| chronic pancreatitis | 38 (19) | 17 (17) | 21 (21) | |
| cystic pancreatic lesion | 9 (4.5) | 7 (7) | 2 (2) | |
| benign tumor | 3 (1.5) | 1 (1) | 2 (2) | |
| operations performed [n (%)] | ||||
| pylorus-preserving PD (PPPD) | 143 (71.5) | 75 (75) | 68 (68) | 0.18 |
| classic PD (cPD) | 38 (19) | 14 (14) | 24 (24) | |
| duodenum-preserving pancreatic head resection (DPPHR) | 19 (9.5) | 11 (11) | 8 (8) | |
| intraoperative portal vein resected [n (%)] | 64 (32) | 26 (26) | 38 (38) | 0.07 |
| Intraoperative arterial resection [n (%)] | 18 (9) | 6 (6) | 12 (12) | 0.14 |
| fistula risk score (FRS) [IQR] | 3 (2–5) | 3 (2–5) | 3 (2–5) | 0.96 |
| Overall | Non-SDD | SDD | p Value | |
|---|---|---|---|---|
| patients [n (%)] | 200 | 100 (50) | 100 (50) | |
| intraoperative smear test [n (%)] | ||||
| available | 137 (68.5) | 50 (50) | 87 (87) | <0.001 |
| positive | 85 (62) | 34 (68) | 51 (58.6) | 0.28 |
| positive (patients without bile duct stent) | 21 (29.6) | 11 (44) | 10 (21.7) | 0.05 |
| absolute number of bacteria in bile duct culture [n] (IQR) | 2 (0–3) | 2 (0–4) | 1 (0–3) | 0.04 |
| bacterial load [n (%)] | ||||
| bile duct cultural bacterial load “none” | 52 (38) | 16 (32) | 36 (41.4) | 0.37 |
| bile duct cultural bacterial load “occasional” | 9 (6.6) | 4 (8) | 5 (5.7) | |
| bile duct cultural bacterial load “numerous” | 16 (11.7) | 4 (8) | 12 (13.8) | |
| bile duct cultural bacterial load “massive” | 60 (43.8) | 26 (52) | 34 (39.1) |
| Overall | Non-SDD | SDD | p-Value | |
|---|---|---|---|---|
| patients [n (%)] | 200 | 100 (50) | 100 (50) | |
| length of hospital stay (LOS) (IQR) | 16 (12–27) | 19 (14–30) | 14 (10–22.8) | <0.001 |
| length of intensive care unit stay (ICU stay) (IQR) | 2 (1–5) | 4 (2–6.5) | 2 (1–3) | <0.001 |
| ICU readmission [n (%)] | 32 (16) | 16 (16) | 17 (17) | 0.85 |
| postoperative complication [n (%)] | ||||
| CDC > 2 [n (%)] | 95 (47.5) | 49 (49) | 46 (46) | 0.67 |
| in-hospital mortality [n (%)] | 16 (8) | 8 (8) | 8 (8) | 1 |
| 30-day mortality [n (%)] | 24 (12) | 8 (8) | 16 (16) | 0.08 |
| 90-day mortality [n (%)] | 36 (18) | 14 (14) | 22 (22) | 0.14 |
| surgical site infection (SSI) [n (%)] | 44 (22) | 20 (20) | 24 (24) | 0.5 |
| deep organ space abscesses / fluid collection [n (%)] | 63 (31.5) | 36 (36) | 27 (27) | 0.17 |
| clinically relevant pancreatic fistula (POPF) [n (%)] | 40 (20) | 17 (17) | 23 (23) | 0.31 |
| postpancreatectomy hemorrhage (PPH) [n (%)] | 31 (15.5) | 13 (13) | 18 (18) | 0.34 |
| delayed gastric emptying (DGE) [n (%)] | 46 (23) | 22 (22) | 24 (24) | 0.74 |
| postoperative positive blood cultures [n (%)] | 25 (12.5) | 13 (13) | 12 (12) | 0.83 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radulova-Mauersberger, O.; Oehme, F.; Doerell, A.; Frohneberg, L.; Hempel, S.; Weitz, J.; Welsch, T.; Distler, M.; Teske, C. Selective Decontamination of the Digestive Tract in Pancreatic Head Resections—A Propensity Score-Matched Analysis. J. Clin. Med. 2023, 12, 250. https://doi.org/10.3390/jcm12010250
Radulova-Mauersberger O, Oehme F, Doerell A, Frohneberg L, Hempel S, Weitz J, Welsch T, Distler M, Teske C. Selective Decontamination of the Digestive Tract in Pancreatic Head Resections—A Propensity Score-Matched Analysis. Journal of Clinical Medicine. 2023; 12(1):250. https://doi.org/10.3390/jcm12010250
Chicago/Turabian StyleRadulova-Mauersberger, Olga, Florian Oehme, Alexandra Doerell, Laura Frohneberg, Sebastian Hempel, Jürgen Weitz, Thilo Welsch, Marius Distler, and Christian Teske. 2023. "Selective Decontamination of the Digestive Tract in Pancreatic Head Resections—A Propensity Score-Matched Analysis" Journal of Clinical Medicine 12, no. 1: 250. https://doi.org/10.3390/jcm12010250