
Clinical Effects of Photofunctionalization on Implant Stability and Marginal Bone Loss: Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Focused Question
2.2. PICOS Criteria
2.3. Eligibility Criteria
2.4. Search Strategy and Study Selection
2.5. Data Extraction
2.6. Risk-of-Bias Assessment
2.7. Data Analysis
3. Results
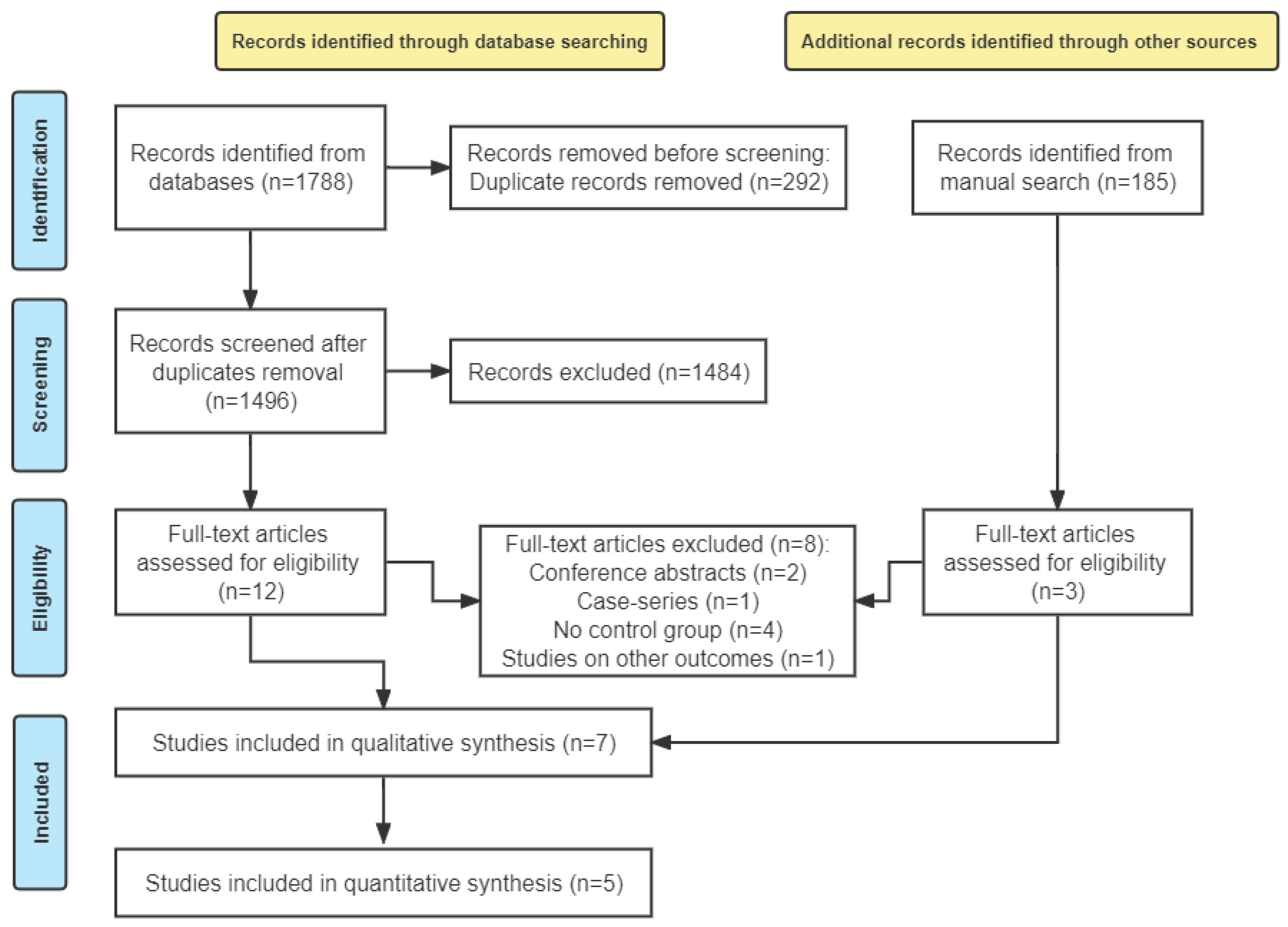
3.1. Study Selection
3.2. Study Characteristics
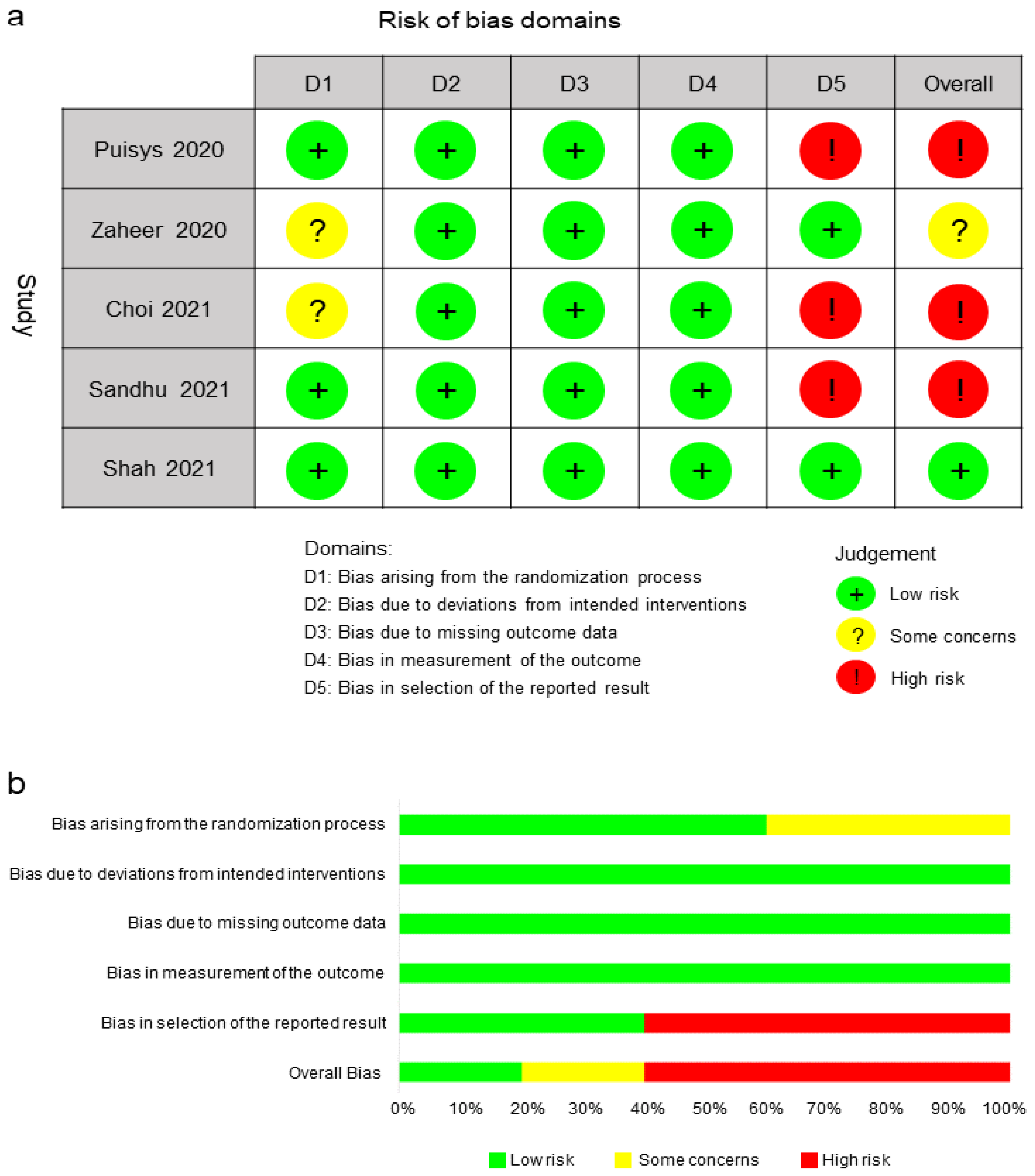
3.3. Risk of Bias
3.4. Meta-Analyses
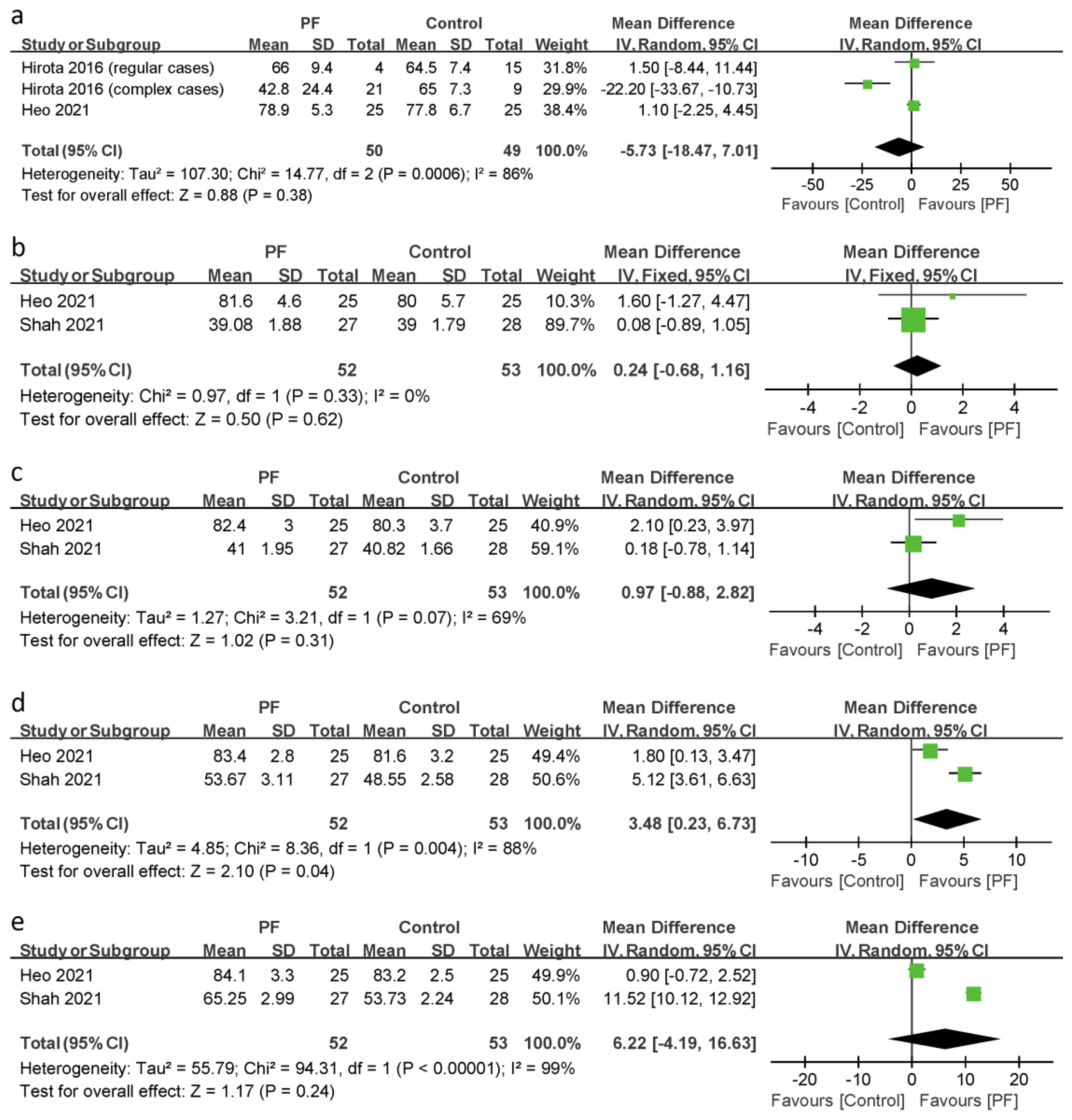
3.4.1. Implant Stability
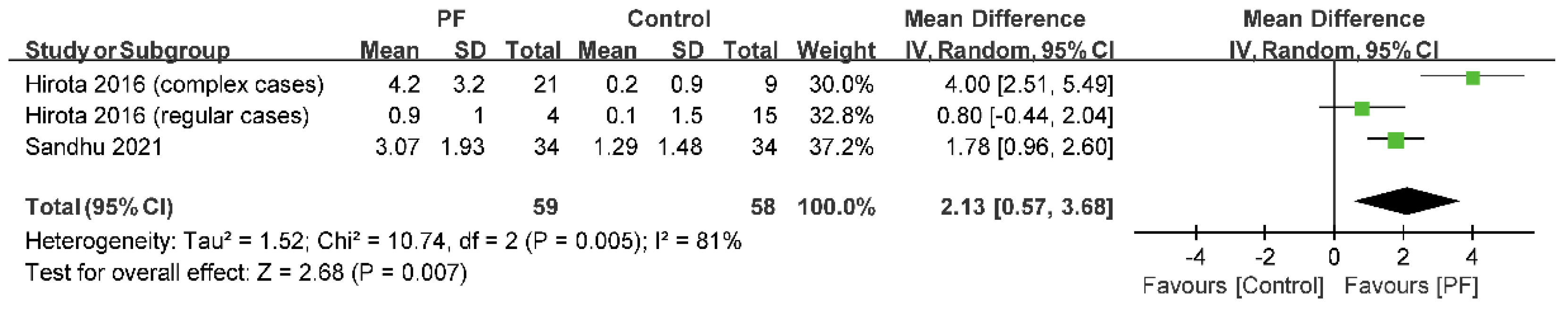
3.4.2. OSI
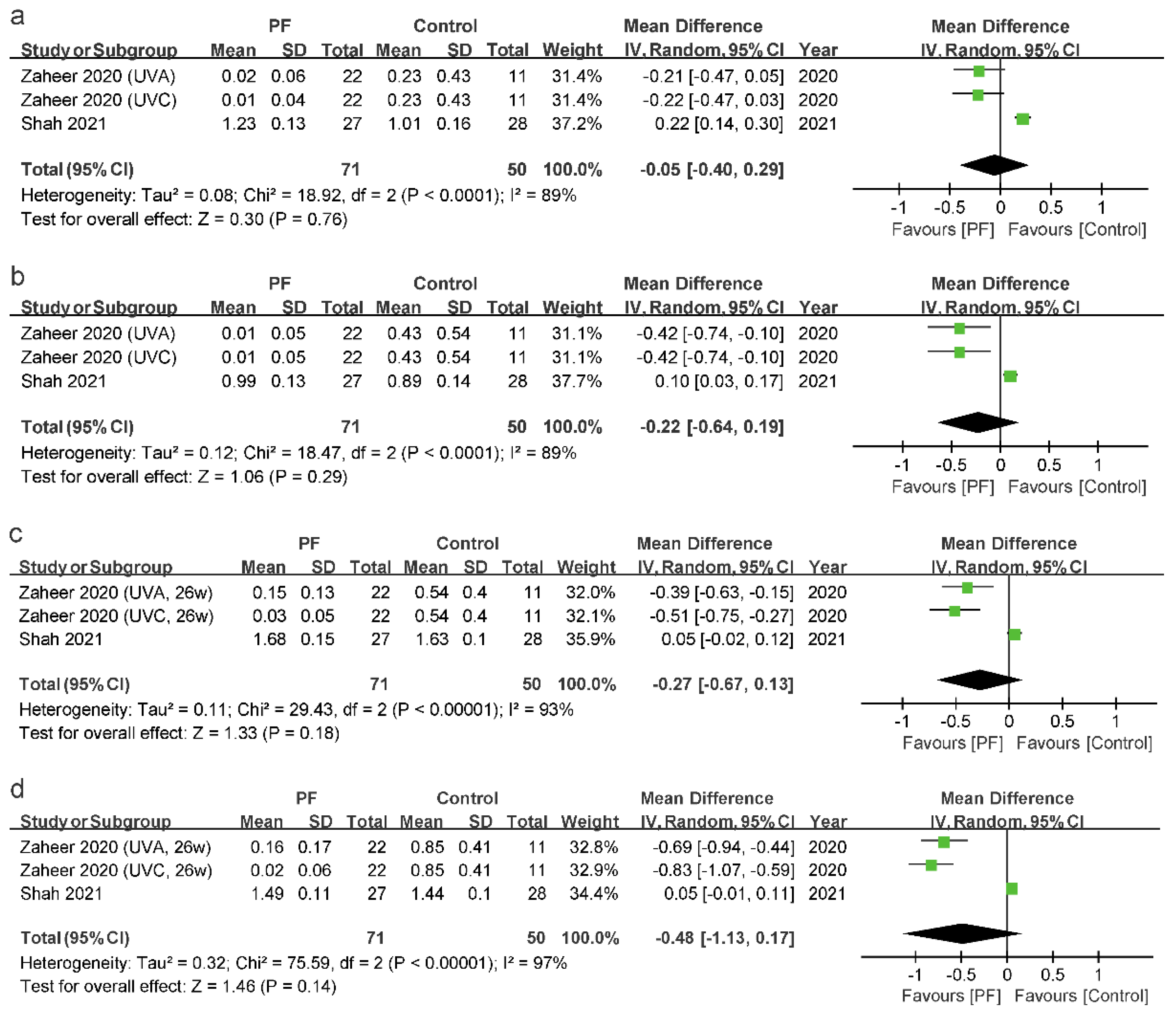
3.4.3. MBL
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, Y.; Bäumer, D.; Ozga, A.-K.; Körner, G.; Bäumer, A. Patient satisfaction and oral health-related quality of life 10 years after implant placement. BMC Oral Health 2021, 21, 30. [Google Scholar] [CrossRef] [PubMed]
- Moraschini, V.; Poubel, L.D.C.; Ferreira, V.; Barboza, E.D.S. Evaluation of survival and success rates of dental implants reported in longitudinal studies with a follow-up period of at least 10 years: A systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Branemark, P.-I. Osseointegration and its experimental background. J. Prosthet. Dent. 1983, 50, 399–410. [Google Scholar] [CrossRef]
- Javed, F.; Romanos, G.E. The role of primary stability for successful immediate loading of dental implants. A literature review. J. Dent. 2010, 38, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Karl, M.; Grobecker-Karl, T. Effect of bone quality, implant design, and surgical technique on primary implant stability. Quintessence Int. 2018, 49, 189–198. [Google Scholar] [CrossRef]
- Elias, C.N.; Rocha, F.A.; Nascimento, A.L.; Coelho, P.G. Influence of implant shape, surface morphology, surgical technique and bone quality on the primary stability of dental implants. J. Mech. Behav. Biomed. Mater. 2012, 16, 169–180. [Google Scholar] [CrossRef]
- Tatarakis, N.; Bashutski, J.; Wang, H.-L.; Oh, T.-J. Early Implant Bone Loss: Preventable or Inevitable? Implant Dent. 2012, 21, 379–386. [Google Scholar] [CrossRef]
- Ting, M.; Tenaglia, M.S.; Jones, G.H.; Suzuki, J.B. Surgical and Patient Factors Affecting Marginal Bone Levels around Dental Implants: A Comprehensive Overview of Systematic Reviews. Implant Dent. 2017, 26, 303–315. [Google Scholar] [CrossRef]
- Hameed, M.-H.; Khan, F.-R.; Ghafoor, R.; Azam, S.-I. Marginal bone loss around cement and screw-retained fixed implant prosthesis. J. Clin. Exp. Dent. 2018, 10, e949–e954. [Google Scholar] [CrossRef]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.R. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int. J. Oral Maxillofac. Implant. 1986, 1, 11–25. [Google Scholar]
- Hori, N.; Ueno, T.; Suzuki, T.; Yamada, M.; Att, W.; Okada, S.; Ohno, A.; Aita, H.; Kimoto, K.; Ogawa, T. Ultraviolet light treatment for the restoration of age-related degradation of titanium bioactivity. Int. J. Oral Maxillofac. Implant. 2010, 25, 49–62. [Google Scholar]
- Hori, N.; Ueno, T.; Minamikawa, H.; Iwasa, F.; Yoshino, F.; Kimoto, K.; Lee, M.C.-I.; Ogawa, T. Electrostatic control of protein adsorption on UV-photofunctionalized titanium. Acta Biomater. 2010, 6, 4175–4180. [Google Scholar] [CrossRef]
- Att, W.; Ogawa, T. Biological aging of implant surfaces and their restoration with ultraviolet light treatment: A novel understanding of osseointegration. Int. J. Oral Maxillofac. Implant. 2012, 27, 753–761. [Google Scholar]
- Gajiwala, M.; Paliwal, J.; Husain, S.Y.; Dadarwal, A.; Kalla, R.; Sharma, V.; Sharma, M. Influence of surface modification of titanium implants on improving osseointegration: An in vitro study. J. Prosthet. Dent. 2021, 126, 405.e1–405.e7. [Google Scholar] [CrossRef]
- Aita, H.; Hori, N.; Takeuchi, M.; Suzuki, T.; Yamada, M.; Anpo, M.; Ogawa, T. The effect of ultraviolet functionalization of titanium on integration with bone. Biomaterials 2009, 30, 1015–1025. [Google Scholar] [CrossRef]
- Kim, M.-Y.; Choi, H.; Lee, J.-H.; Kim, J.-H.; Jung, H.-S.; Kim, J.-H.; Park, Y.-B.; Moon, H.-S. UV Photofunctionalization Effect on Bone Graft in Critical One-Wall Defect around Implant: A Pilot Study in Beagle Dogs. BioMed Res. Int. 2016, 2016, 4385279. [Google Scholar] [CrossRef] [Green Version]
- Park, K.-H.; Koak, J.-Y.; Kim, S.-K.; Han, C.-H.; Heo, S.J. The Effect of Ultraviolet-C Irradiation Via a Bactericidal Ultraviolet Sterilizer on an Anodized Titanium Implant: A Study in Rabbits. Int. J. Oral Maxillofac. Implant. 2013, 28, 57–66. [Google Scholar] [CrossRef] [Green Version]
- Ueno, T.; Yamada, M.; Hori, N.; Suzuki, T.; Ogawa, T. Effect of ultraviolet photoactivation of titanium on osseointegration in a rat model. Int. J. Oral Maxillofac. Implant. 2010, 25, 287–294. [Google Scholar]
- Pesce, P.; Menini, M.; Santori, G.; De Giovanni, E.; Bagnasco, F.; Canullo, L. Photo and Plasma Activation of Dental Implant Titanium Surfaces. A Systematic Review with Meta-Analysis of Pre-Clinical Studies. J. Clin. Med. 2020, 9, 2817. [Google Scholar] [CrossRef]
- Dini, C.; Nagay, B.E.; Magno, M.B.; Maia, L.C.; Barão, V.A.R. Photofunctionalization as a suitable approach to improve the osseointegration of implants in animal models—A systematic review and meta-analysis. Clin. Oral Implant. Res. 2020, 31, 785–802. [Google Scholar] [CrossRef]
- Funato, A.; Yamada, M.; Ogawa, T. Success Rate, Healing Time, and Implant Stability of Photofunctionalized Dental Implants. Int. J. Oral Maxillofac. Implant. 2013, 28, 1261–1271. [Google Scholar] [CrossRef] [PubMed]
- Funato, A.; Ogawa, T. Photofunctionalized Dental Implants: A Case Series in Compromised Bone. Int. J. Oral Maxillofac. Implant. 2013, 28, 1589–1601. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Kobayashi, H.; Ogawa, T. Implant Stability Change and Osseointegration Speed of Immediately Loaded Photofunctionalized Implants. Implant Dent. 2013, 22, 481–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirota, M.; Ozawa, T.; Iwai, T.; Ogawa, T.; Tohnai, I. Implant Stability Development of Photofunctionalized Implants Placed in Regular and Complex Cases: A Case-Control Study. Int. J. Oral Maxillofac. Implant. 2016, 31, 676–686. [Google Scholar] [CrossRef] [PubMed]
- Kitajima, H.; Ogawa, T. The Use of Photofunctionalized Implants for Low or Extremely Low Primary Stability Cases. Int. J. Oral Maxillofac. Implant. 2016, 31, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Hirota, M.; Ozawa, T.; Iwai, T.; Mitsudo, K.; Ogawa, T. UV-Mediated Photofunctionalization of Dental Implant: A Seven-Year Results of a Prospective Study. J. Clin. Med. 2020, 9, 2733. [Google Scholar] [CrossRef]
- Puisys, A.; Schlee, M.; Linkevicius, T.; Petrakakis, P.; Tjaden, A. Photo-activated implants: A triple-blinded, split-mouth, randomized controlled clinical trial on the resistance to removal torque at various healing intervals. Clin. Oral Investig. 2019, 24, 1789–1799. [Google Scholar] [CrossRef]
- Zaheer, N.; Bin Rajion, Z.A.; Shahbaz, M.; Zaheer, U.; Saeed, M.Q.; Razak, N.H.A. Bone Density and Marginal Bone Loss around Implants Post Ultraviolet A and Ultraviolet C Irradiation. Sains Malays. 2020, 49, 1411–1420. [Google Scholar] [CrossRef]
- Choi, B.; Lee, Y.C.; Oh, K.C.; Lee, J.H. Effects of photofunctionalization on early osseointegration of titanium dental implants in the maxillary posterior region: A randomized double-blinded clinical trial. Int. J. Implant Dent. 2021, 7, 37. [Google Scholar] [CrossRef]
- Sandhu, R.; Kheur, M.; Lakha, T.; Kheur, S.; Le, B. Comparative evaluation of implant stability quotient trends, crestal bone loss and survival of photofunctionalised and untreated dental implants: A split-mouth randomised controlled clinical trial. Int. J. oral Implant. 2021, 14, 127–138. [Google Scholar]
- Singh, B.P.; Shah, S.A.; Rao, J.; Kumar, L.; Singh, M.; Singh, P.K. Biological and esthetic outcome of immediate dental implant with the adjunct pretreatment of immediate implants with platelet-rich plasma or photofunctionalization: A randomized controlled trial. J. Indian Prosthodont. Soc. 2021, 21, 348. [Google Scholar] [CrossRef]
- Heo, Y.-R.; Kang, J.; Son, M.-K. Evaluation of Dental Implant Stability with or without Photoactivated Surface Treatment. J. Implant. Appl. Sci. 2021, 25, 57–63. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Hirota, M.; Ozawa, T.; Iwai, T.; Ogawa, T.; Tohnai, I. Effect of Photofunctionalization on Early Implant Failure. Int. J. Oral Maxillofac. Implants 2018, 33, 1098–1102. [Google Scholar] [CrossRef]
- Kheur, M.; Lakha, T.; Kheur, S. A Split Mouth Study Evaluating the ISQ Trends, Radiographic Bone Loss and Implant Survival of Photofunctionalized and Untreated Dental Implants. Clin. Oral Implants Res. 2018, 29, 102. [Google Scholar] [CrossRef] [Green Version]
- Masuda, I. Clinical Study of Nongrafted Sinus Lift Using Titanium Plate and Screw for a Single Tooth Defect- Consideration for Cases Combined with UV-Photofunctionalization. Clin. Oral Implants Res. 2018, 29, 371. [Google Scholar] [CrossRef] [Green Version]
- Tuna, T.; Wein, M.; Swain, M.; Fischer, J.; Att, W. Influence of ultraviolet photofunctionalization on the surface characteristics of zirconia-based dental implant materials. Dent. Mater. 2015, 31, e14–e24. [Google Scholar] [CrossRef]
- Henningsen, A.; Smeets, R.; Hartjen, P.; Heinrich, O.; Heuberger, R.; Heiland, M.; Precht, C.; Cacaci, C. Photofunctionalization and non-thermal plasma activation of titanium surfaces. Clin. Oral Investig. 2017, 22, 1045–1054. [Google Scholar] [CrossRef]
- Gupta, R.K.; Padmanabhan, T.V. An Evaluation of the Resonance Frequency Analysis Device: Examiner Reliability and Repeatability of Readings. J. Oral Implant. 2013, 39, 704–707. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.-L.; Tsai, M.-T.; Su, K.-C.; Li, Y.-F.; Hsu, J.-T.; Chang, C.-H.; Fuh, L.-J.; Wu, A.Y.-J. Relation between initial implant stability quotient and bone-implant contact percentage: An in vitro model study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, e356–e361. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Wu, G.; Hunziker, E. The clinical significance of implant stability quotient (ISQ) measurements: A literature review. J. Oral Biol. Craniofacial Res. 2020, 10, 629–638. [Google Scholar] [CrossRef]
- Swami, V.; Vijayaraghavan, V.; Swami, V. Current trends to measure implant stability. J. Indian Prosthodont. Soc. 2016, 16, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, D.Y.; Sherwood, R.L.; Collins, T.A.; Krogh, P.H. The reverse-torque test: A clinical report. Int. J. Oral Maxillofac. Implant. 1996, 11, 179–185. [Google Scholar]
- Ogawa, T. Ultraviolet Photofunctionalization of Titanium Implants. Int. J. Oral Maxillofac. Implant. 2014, 29, e95–e102. [Google Scholar] [CrossRef]
- Zhao, G.; Schwartz, Z.; Wieland, M.; Rupp, F.; Geis-Gerstorfer, J.; Cochran, D.L.; Boyan, B.D. High surface energy enhances cell response to titanium substrate microstructure. J. Biomed. Mater. Res. Part A 2005, 74A, 49–58. [Google Scholar] [CrossRef]
- Leon-Ramos, J.-R.; Diosdado-Cano, J.-M.; López-Santos, C.; Barranco, A.; Torres-Lagares, D.; Serrera-Figallo, M. Influence of Titanium Oxide Pillar Array Nanometric Structures and Ultraviolet Irradiation on the Properties of the Surface of Dental Implants—A Pilot Study. Nanomaterials 2019, 9, 1458. [Google Scholar] [CrossRef] [Green Version]
- Att, W.; Hori, N.; Iwasa, F.; Yamada, M.; Ueno, T.; Ogawa, T. The effect of UV-photofunctionalization on the time-related bioactivity of titanium and chromium–cobalt alloys. Biomaterials 2009, 30, 4268–4276. [Google Scholar] [CrossRef]
- Pacheco, V.N.; Nolde, J.; de Quevedo, A.S.; Visioli, F.; Ponzoni, D. Improvement in the chemical structure and biological activity of surface titanium after exposure to UVC light. Odontology 2020, 109, 271–278. [Google Scholar] [CrossRef]
- Gao, Y.; Liu, Y.; Zhou, L.; Guo, Z.; Rong, M.; Liu, X.; Lai, C.; Ding, X. The Effects of Different Wavelength UV Photofunctionalization on Micro-Arc Oxidized Titanium. PLoS ONE 2013, 8, e68086. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Country | Study Design | Patients | Mean Age (Range) | Gender (M/F) | Implants | Arch | Immediate Implant | Time Period of Placement—Final Reconstruction |
|---|---|---|---|---|---|---|---|---|---|
| Hirota (2016) [24] | Japan | Case-control study | 7 | 47–63 | 3/4 | 49 | Max/Mnd | Yes/No | 3–8 months |
| Puisys (2020) [27] | Lithuania | RCT S | 180 | 50.65 (24–78) | 69/111 | 360 | Max/Mnd | No | NR |
| Zaheer (2020) [28] | Pakistan | RCT | 66 | 40.6 ± 12.1 | 24/42 | 66 | Max/Mnd | No | NR |
| Choi (2021) [29] | Korea | RCT | 34 | 66.13 (32–88) | 15/19 | 57 | Max | No | 4 months |
| Sandhu (2021) [30] | India | RCT S | 34 | 46.94 ± 12.03 | 20/14 | 68 | Max/Mnd | No | 3 months |
| Shah (2021) [31] | India | RCT | 84 | 50.7 ± 7.1 | 47/37 | 84 | Max | Yes | 6 months |
| Heo (2021) [32] | Korea | CCT | 25 | 63.9 | 12/13 | 50 | Max/Mnd | No | NR |
| Author (Year) | Photofunctionalization Device | Wavelength (nm) | Photofunctionalization Time (min) |
|---|---|---|---|
| Hirota (2016) [24] | TheraBeam Affiny (Ushio) | A mixture of spectra TA | 15 |
| Puisys (2020) [27] | TheraBeam® SuperOsseo Device (Ushio Inc., Sazuchi Bessho-cho, Himejij, Hyogo, Japan) | A mixture of spectra TS | 12 |
| Zaheer (2020) [28] | UV ACUBE 100 (Honle, Grafelfing, Germany) | UVA, 382 | 10 |
| UVC, 260 | 10 | ||
| Choi (2021) [29] | TheraBeam Affiny (Ushio Inc., Tokyo, Japan) | A mixture of spectra TA | 15 |
| Sandhu (2021) [30] | Lelesil Innovative Systems (Thane, India) | NR | 15 |
| Shah (2021) [31] | Ultraviolet rays chamber (SK Dent) | 253.7 | 20 |
| Heo (2021) [32] | NR | NR | NR |
| Author (Year) | Main Findings | Conclusions |
|---|---|---|
| Hirota (2016) [24] | The average OSI and the OSI in complex cases were considerably greater for photofunctionalized implants than for as-received implants. Photofunctionalized implants showed significantly higher ISQ2 values than as-received implants. | Photofunctionalization accelerated the rate and enhanced the final level of implant stability development compared with as-received implants, particularly for implants placed into poor-quality bone and other complex cases. |
| Puisys (2020) [27] | At 2, 3, 4, and 8 weeks, the RT values were higher in photoactivated implants than those in control implants, being statistically significant. | The photoactivation of the surface of titanium implants improved healing and implant stability, especially in the early healing phase. |
| Zaheer (2020) [28] | Both UVA- and UVC-treated groups showed minimal MBL compared with control group, with no significant differences between the two experimental groups. | Photofunctionalized SLA-coated titanium dental implants showed positive biological response after the healing phase in contrast to the non-UV-treated group. |
| Choi (2021) [29] | In bone quality group III (grayscale value between 300 and 500), significant differences were observed in terms of the differences in the resonance frequency analysis values 4 weeks and 4 months postoperatively. In bone quality group II (grayscale value above 500), the UV-treated group showed significantly lesser bone loss 4 weeks postoperatively. | UV surface treatment on implants may increase the initial stability in the region of the maxilla with poor bone quality. |
| Sandhu (2021) [30] | The PF group showed a statistically significantly higher OSI than the control group. Statistically significantly higher crestal bone loss was observed in the control group as compared with the PF group. | Implants with photofunctionalized surfaces reduced overall healing time and crestal bone loss. Photofunctionalization was an effective aid for achieving faster osseointegration with good crestal bone stability. |
| Shah (2021) [31] | Mean MBL was not significantly different between the PF group and the control group. The PF group showed significantly greater implant stability than the control group. | Pretreatment of commercial dental implants with PF exhibited a statistically significant difference in implant stability but not in other outcomes. |
| Heo (2021) [32] | The photoactivated implants showed higher ISQ values than those without photoactivated surface treatment. However, there were no significant differences between the two implant groups. | The photoactivated implant surface appeared to have higher implant stability than that without photoactivation by increasing the hydrophilic surface. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lang, X.; Qiao, B.; Ge, Z.; Yan, J.; Zhang, Y. Clinical Effects of Photofunctionalization on Implant Stability and Marginal Bone Loss: Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 7042. https://doi.org/10.3390/jcm11237042
Lang X, Qiao B, Ge Z, Yan J, Zhang Y. Clinical Effects of Photofunctionalization on Implant Stability and Marginal Bone Loss: Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(23):7042. https://doi.org/10.3390/jcm11237042
Chicago/Turabian StyleLang, Xinrui, Bo Qiao, Ziyu Ge, Jiahui Yan, and Yanzhen Zhang. 2022. "Clinical Effects of Photofunctionalization on Implant Stability and Marginal Bone Loss: Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 23: 7042. https://doi.org/10.3390/jcm11237042