
Cannabis Use Is Inversely Associated with Metabolic Disorders in Hepatitis C-Infected Patients (ANRS CO22 Hepather Cohort)
 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Design
2.2. Data Collection
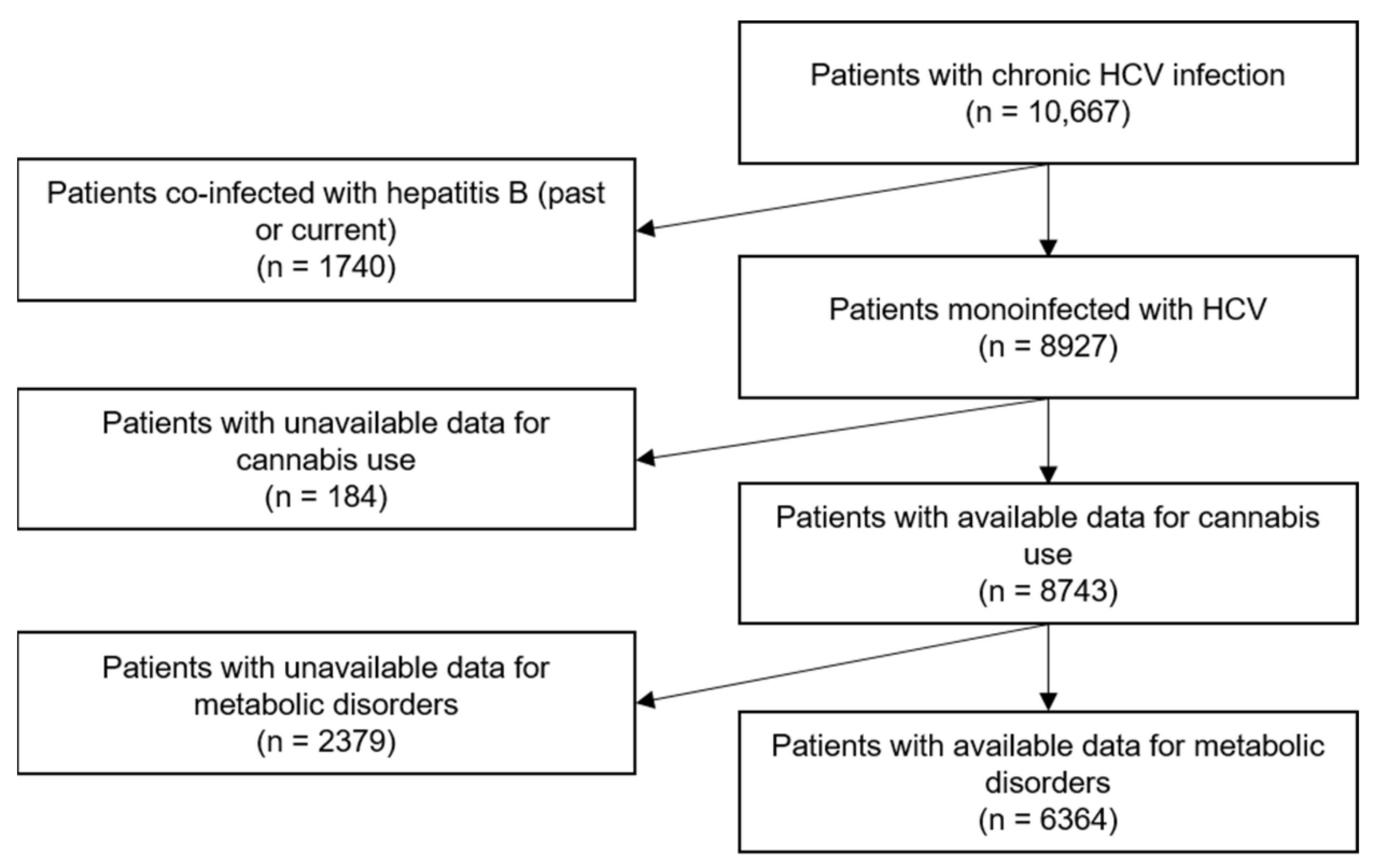
2.3. Study Population
2.4. Outcomes
2.5. Explanatory Variables
2.6. Statistical Analyses
3. Results
3.1. Study Population Characteristics
3.2. Factors Associated with Dyslipidemia
3.3. Factors Associated with Hypertension
3.4. Factors Associated with the Number of Metabolic Disorders
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Scientific Committee
References
- Wang, C.-C.; Cheng, P.-N.; Kao, J.-H. Systematic review: Chronic viral hepatitis and metabolic derangement. Aliment. Pharmacol. Ther. 2020, 51, 216–230. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.-H.; Kee, K.-M.; Wang, J.-H.; Hsu, N.-T.; Hsiao, C.-C.; Chen, Y.; Lu, S.-N. Association between chronic viral hepatitis and metabolic syndrome in southern Taiwan: A large population-based study. Aliment. Pharmacol. Ther. 2018, 48, 993–1002. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.-L. Metabolic alterations and hepatitis C: From bench to bedside. World J. Gastroenterol. 2016, 22, 1461–1476. [Google Scholar] [CrossRef]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed] [Green Version]
- McPherson, S.; Gosrani, S.; Hogg, S.; Patel, P.; Wetten, A.; Welton, R.; Hallsworth, K.; Campbell, M. Increased cardiovascular risk and reduced quality of life are highly prevalent among individuals with hepatitis C. BMJ Open Gastroenterol. 2020, 7, e000470. [Google Scholar] [CrossRef] [PubMed]
- Badawi, A.; Di Giuseppe, G.; Arora, P. Cardiovascular disease risk in patients with hepatitis C infection: Results from two general population health surveys in Canada and the United States (2007–2017). PLoS ONE 2018, 13, e0208839. [Google Scholar] [CrossRef] [Green Version]
- Chaudhari, R.; Fouda, S.; Sainu, A.; Pappachan, J.M. Metabolic complications of hepatitis C virus infection. World J. Gastroenterol. 2021, 27, 1267–1282. [Google Scholar] [CrossRef]
- Grattagliano, I.; Rossi, A.; Marconi, E.; Lapi, F.; Cricelli, C. Determinants of HCV-related complications in Italian primary care patients. Liver Int. 2021, 41, 2857–2865. Available online: http://onlinelibrary.wiley.com/doi/abs/10.1111/liv.15017 (accessed on 17 December 2021). [CrossRef]
- Wong, A.; Le, A.; Lee, M.-H.; Lin, Y.-J.; Nguyen, P.; Trinh, S.; Dang, H.; Nguyen, M.H. Higher risk of hepatocellular carcinoma in Hispanic patients with hepatitis C cirrhosis and metabolic risk factors. Sci. Rep. 2018, 8, 7164. [Google Scholar] [CrossRef] [Green Version]
- Siphepho, P.Y.; Liu, Y.-T.; Shabangu, C.S.; Huang, J.-F.; Huang, C.-F.; Yeh, M.-L.; Yu, M.-L.; Wang, S.-C. The Impact of Steatosis on Chronic Hepatitis C Progression and Response to Antiviral Treatments. Biomedicines 2021, 9, 1491. [Google Scholar] [CrossRef]
- Asrih, M.; Jornayvaz, F.R. Metabolic syndrome and nonalcoholic fatty liver disease: Is insulin resistance the link? Mol. Cell. Endocrinol. 2015, 418 Pt 1, 55–65. [Google Scholar] [CrossRef] [Green Version]
- Dong, T.S.; Aby, E.; Benhammou, J.; Kawamoto, J.; Han, S.-H.; May, F.; Pisegna, J.R. Metabolic syndrome does not affect sustained virologic response of direct-acting antivirals while hepatitis C clearance improves hemoglobin A1c. World J. Hepatol. 2018, 10, 612–621. [Google Scholar] [CrossRef]
- Drazilova, S.; Gazda, J.; Janicko, M.; Jarcuska, P. Chronic Hepatitis C Association with Diabetes Mellitus and Cardiovascular Risk in the Era of DAA Therapy. Can. J. Gastroenterol. Hepatol. 2018, 2018, 6150861. [Google Scholar] [CrossRef]
- Cacciola, I.; Russo, G.; Filomia, R.; Pitrone, C.; Caccamo, G.; Giandalia, A.; Alibrandi, A.; Franzè, M.S.; Porcari, S.; Maimone, S.; et al. Over time evaluation of glycaemic control in di-rect-acting-antiviral treated HCV/diabetic individuals with chronic hepatitis or with cirrhosis. Liver Int. 2021, 41, 2059–2067. [Google Scholar] [CrossRef]
- Weidner, P.; Boettche, D.; Zimmerer, T.; Burgermeister, E.; Teufel, A.; Ebert, M.P.; Antoni, C. Impact of Direct Acting Antiviral (DAA) Treatment on Glucose Metabolism and Reduction of Pre-diabetes in Patients with Chronic Hepatitis C. J. Gastrointest. Liver Dis. 2018, 27, 281–289. [Google Scholar] [CrossRef] [Green Version]
- Váncsa, S.; Németh, D.; Hegyi, P.; Szakács, Z.; Farkas, Á.; Kiss, S.; Hegyi, P.J.; Kanjo, A.; Sarlós, P.; Erőss, B.; et al. Diabetes Mellitus Increases the Risk of Hepatocellular Car-cinoma After Direct-Acting Antiviral Therapy: Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 744512. [Google Scholar] [CrossRef]
- Schlevogt, B.; Boeker, K.H.W.; Mauss, S.; Klinker, H.; Heyne, R.; Link, R.; Simon, K.-G.; Sarrazin, C.; Serfert, Y.; Manns, M.P.; et al. Weight Gain after Interferon-Free Treatment of Chronic Hepatitis C—Results from the German Hepatitis C-Registry (DHC-R). Biomedicines 2021, 9, 1495. [Google Scholar] [CrossRef]
- Minami, T.; Tateishi, R.; Fujiwara, N.; Nakagomi, R.; Nakatsuka, T.; Sato, M.; Uchino, K.; Enooku, K.; Nakagawa, H.; Fujinaga, H.; et al. Impact of Obesity and Heavy Alcohol Consumption on Hepatocellular Carcinoma Development after HCV Eradication with Antivirals. Liver Cancer 2021, 10, 309–319. [Google Scholar] [CrossRef]
- Kolonko, A.; Musialik, J.; Chudek, J.; Bartmańska, M.; Słabiak-Błaż, N.; Kujawa-Szewieczek, A.; Kuczera, P.; Kwiecień-Furmańczuk, K.; Więcek, A. Changes in Office Blood Pressure Control, Augmentation Index, and Liver Steatosis in Kidney Transplant Patients after Successful Hepatitis C Infection Treatment with Direct Antiviral Agents. J. Clin. Med. 2020, 9, 948. [Google Scholar] [CrossRef] [Green Version]
- Villani, R.; Di Cosimo, F.; Romano, A.D.; Sangineto, M.; Serviddio, G. Serum lipid profile in HCV patients treated with direct-acting antivirals: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 13944. [Google Scholar] [CrossRef]
- Wang, Y.-W.; Lee, W.-P.; Huang, Y.-H.; Hou, M.-C.; Lan, K.-H. Effect of sofosbuvir-based DAAs on changes in lower-density lipoprotein in HCV patients: A systematic review and meta-analysis. BMC Infect. Dis. 2021, 21, 984. [Google Scholar] [CrossRef]
- Barré, T.; Nishimwe, M.L.; Protopopescu, C.; Marcellin, F.; Carrat, F.; Dorival, C.; Delarocque-Astagneau, E.; Larrey, D.; Bourlière, M.; Petrov-Sanchez, V.; et al. Cannabis use is associated with a lower risk of diabetes in chronic hepatitis C-infected patients (ANRS CO22 Hepather cohort). J. Viral Hepat. 2020, 27, 1473–1483. [Google Scholar] [CrossRef]
- Barré, T.; Carrat, F.; Ramier, C.; Fontaine, H.; di Beo, V.; Bureau, M.; Dorival, C.; Larrey, D.; Delarocque-Astagneau, E.; Mathurin, P.; et al. Cannabis use as a factor of lower corpulence in hepatitis C-infected patients: Results from the ANRS CO22 Hepather cohort. J. Cannabis Res. 2022, 4, 31. [Google Scholar] [CrossRef]
- Vidot, D.C.; Prado, G.; Hlaing, W.M.; Florez, H.J.; Arheart, K.L.; Messiah, S.E. Metabolic Syndrome Among Marijuana Users in the United States: An Analysis of National Health and Nutrition Examination Survey Data. Am. J. Med. 2016, 129, 173–179. [Google Scholar] [CrossRef] [Green Version]
- Meier, M.; Pardini, D.; Beardslee, J.; Matthews, K.A. Associations Between Cannabis Use and Cardiometabolic Risk Factors: A Longitudinal Study of Men. Psychosom. Med. 2019, 81, 281–288. [Google Scholar] [CrossRef]
- Vidot, D.C.; Powers, M.; Gonzalez, R.; Jayaweera, D.T.; Roy, S.; Dong, C.; Messiah, S.E. Blood Pressure and Marijuana Use: Results from a Decade of NHANES Data. Am. J. Health Behav. 2019, 43, 887–897. [Google Scholar] [CrossRef]
- Alshaarawy, O.; Elbaz, H.A. Cannabis Use and Blood Pressure Levels: United States National Health and Nutrition Ex-amination Survey, 2005–2012. J. Hypertens. 2016, 34, 1507–1512. [Google Scholar] [CrossRef] [Green Version]
- Haleem, A.; Hwang, Y.J.; Elton-Marshall, T.; Rehm, J.; Imtiaz, S. The longitudinal relationship between cannabis use and hyper-tension. Drug Alcohol Rev. 2021, 40, 914–919. [Google Scholar] [CrossRef]
- Abuhasira, R.; Haviv, Y.S.; Leiba, M.; Leiba, A.; Ryvo, L.; Novack, V. Cannabis is associated with blood pressure reduction in older adults—A 24-hours ambulatory blood pressure monitoring study. Eur. J. Intern. Med. 2021, 86, 79–85. [Google Scholar] [CrossRef]
- Lazarte, J.; Hegele, R.A. Cannabis effects on lipoproteins. Curr. Opin. Lipidol. 2019, 30, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Pol, S.; Bourliere, M.; Lucier, S.; Hezode, C.; Dorival, C.; Larrey, D.; Bronowicki, J.-P.; Ledinghen, V.D.E.; Zoulim, F.; Tra, A.; et al. Safety and efficacy of daclatasvir-sofosbuvir in HCV gen-otype 1-mono-infected patients. J. Hepatol. 2017, 66, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, M.E.; Protopopescu, C.; Sogni, P.; Yaya, I.; Piroth, L.; Bailly, F.; Marcellin, F.; Esterle, L.; Wittkop, L.; Rosenthal, E.; et al. HCV-Related Mortality among HIV/HCV Co-infected Patients: The Importance of Behaviors in the HCV Cure Era (ANRS CO13 HEPAVIH Cohort). AIDS Behav. 2020, 24, 1069–1084. [Google Scholar] [CrossRef] [PubMed]
- Haute Autorité de Santé (French National Authority for Health). Screening Tool for Early Detection and Brief Intervention (Outil d’aide au Repérage Précoce et à L’intervention Brève). Available online: https://www.has-sante.fr/jcms/c_1795221/fr/outil-d-aide-au-reperage-precoce-et-intervention-breve-alcool-cannabis-tabac-chez-l-adulte (accessed on 24 October 2019).
- Institut National de la Statistique et des Etudes Economiques. Définition—Pauvreté monétaire/Seuil de pauvreté/Seuil de pauvreté|Insee. Available online: https://www.insee.fr/fr/metadonnees/definition/c1653 (accessed on 10 December 2021).
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. comparison with liver biopsy and fibrotest. Hepatol. Baltim. Md. 2007, 46, 32–36. [Google Scholar] [CrossRef]
- Sersté, T.; Nkuize, M.; Moucari, R.; Van Gossum, M.; Reynders, M.; Scheen, R.; Vertongen, F.; Buset, M.; Mulkay, J.P.; Marcellin, P. Metabolic disorders associated with chronic hepatitis C: Impact of genotype and ethnicity. Liver Int. 2010, 30, 1131–1136. [Google Scholar] [CrossRef]
- Rodondi, N.; Pletcher, M.J.; Liu, K.; Hulley, S.B.; Sidney, S.; Coronary Artery Risk Development in Young Adults (CARDIA) Study. Marijuana use, diet, body mass index, and cardiovascular risk factors (from the CARDIA study). Am. J. Cardiol. 2006, 98, 478–484. [Google Scholar] [CrossRef]
- Alshaarawy, O.; Vanderziel, A. Visit-to-visit variability in blood pressure among cannabis users participating in the Third National Health and Nutrition Examination Survey. J. Hypertens. 2021, 39, 621–626. [Google Scholar] [CrossRef]
- Nightingale, T.E.; Tejpar, T.; O’Connell, C.; Krassioukov, A.V. Using Cannabis to Control Blood Pressure After Spinal Cord Injury: A Case Report. Ann. Intern. Med. 2020, 173, 668–670. [Google Scholar] [CrossRef]
- Vandrey, R.; Umbricht, A.; Strain, E.C. Increased Blood Pressure After Abrupt Cessation of Daily Cannabis Use. J. Addict. Med. 2011, 5, 16–20. [Google Scholar] [CrossRef]
- Bonnet, U. Abrupt Quitting of Long-term Heavy Recreational Cannabis Use is Not Followed by Significant Changes in Blood Pressure and Heart Rate. Pharmacopsychiatry 2016, 49, 23–25. [Google Scholar] [CrossRef]
- Goyal, H.; Awad, H.H.; Ghali, J.K. Role of cannabis in cardiovascular disorders. J. Thorac. Dis. 2017, 9, 2079–2092. [Google Scholar] [CrossRef] [Green Version]
- Boggs, D.L.; Nguyen, J.; Morgenson, D.; Taffe, M.A.; Ranganathan, M. Clinical and Preclinical Evidence for Functional Interactions of Cannabidiol and Δ9-Tetrahydrocannabinol. Neuropsychopharmacology 2018, 43, 142–154. [Google Scholar] [CrossRef] [Green Version]
- Lapadula, G.; Torti, C.; Paraninfo, G.; Castelnuovo, F.; Uccelli, M.C.; Costarelli, S.; Ladisa, N.; Maserati, R.; Di Pietro, M.; De Silvestri, A.; et al. Influence of hepatitis C genotypes on lipid levels in HIV-positive patients during highly active antiretroviral therapy. Antivir. Ther. 2006, 11, 521–527. [Google Scholar] [CrossRef]
- De Gottardi, A.; Pazienza, V.; Pugnale, P.; Bruttin, F.; Rubbia-Brandt, L.; Juge-Aubry, C.E.; Meier, C.A.; Hadengue, A.; Negro, F. Peroxisome proliferator-activated receptor-alpha and -gamma mRNA levels are reduced in chronic hepatitis C with steatosis and genotype 3 infection. Aliment. Pharm. Ther. 2006, 23, 107–114. [Google Scholar] [CrossRef]
- Dharancy, S.; Lemoine, M.; Mathurin, P.; Serfaty, L.; Dubuquoy, L. Peroxisome Proliferator-Activated Receptors in HCV-Related Infection. PPAR Res. 2009, 2009, 357204. [Google Scholar] [CrossRef] [Green Version]
- Rojas, Á.; del Campo, J.A.; Maraver, M.; Aparcero, R.; García-Valdecasas, M.; Diago, M.; Carmona, I.; Andrade, R.J.; Solà, R.; Romero-Gómez, M. Hepatitis C virus infection alters lipid metabolism depending on IL28B polymorphism and viral genotype and modulates gene expression in vivo and in vitro. J. Viral Hepat. 2014, 21, 19–24. [Google Scholar] [CrossRef]
- Clark, P.J.; Thompson, A.J.; Vock, D.M.; Kratz, L.E.; Tolun, A.A.; Muir, A.J.; McHutchison, J.G.; Subramanian, M.; Millington, D.M.; Kelley, R.I.; et al. Hepatitis C virus selectively perturbs the distal cho-lesterol synthesis pathway in a genotype-specific manner. Hepatol. Baltim. Md. 2012, 56, 49–56. [Google Scholar] [CrossRef]
- D’Avigdor, W.M.H.; Budzinska, M.A.; Lee, M.; Lam, R.; Kench, J.; Stapelberg, M.; McLennan, S.V.; Farrell, G.; George, J.; McCaughan, G.W.; et al. Virus Genotype-Dependent Transcriptional Alterations in Lipid Metabolism and Inflammation Pathways in the Hepatitis C Virus-infected Liver. Sci. Rep. 2019, 9, 10596. [Google Scholar] [CrossRef] [Green Version]
- Ho, J.S.; Cannaday, J.J.; Barlow, C.E.; Mitchell, T.L.; Cooper, K.H.; FitzGerald, S.J. Relation of the Number of Metabolic Syndrome Risk Factors With All-Cause and Cardiovascular Mortality. Am. J. Cardiol. 2008, 102, 689–692. [Google Scholar] [CrossRef]
- Klein, B.E.; Klein, R.; Lee, K.E. Components of the Metabolic Syndrome and Risk of Cardiovascular Disease and Diabetes in Beaver Dam. Diabetes Care 2002, 25, 1790–1794. [Google Scholar] [CrossRef] [Green Version]
- Alshaarawy, O.; Anthony, J.C. Are cannabis users less likely to gain weight? Results from a national 3-year prospective study. Int. J. Epidemiol. 2019, 48, 1695–1700. [Google Scholar] [CrossRef] [Green Version]
- Clark, T.M.; Jones, J.M.; Hall, A.G.; Tabner, S.A.; Kmiec, R.L. Theoretical Explanation for Reduced Body Mass Index and Obesity Rates in Cannabis Users. Cannabis Cannabinoid Res. 2018, 3, 259–271. [Google Scholar] [CrossRef] [Green Version]
- Adejumo, A.C.; Adegbala, O.M.; Adejumo, K.L.; Bukong, T.N. Reduced Incidence and Better Liver Disease Outcomes among Chronic HCV Infected Patients Who Consume Cannabis. Can. J. Gastroenterol. Hepatol. 2018, 2018, 9430953. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Panjawatanan, P.; Ungprasert, P. Use of cannabis and risk of advanced liver fibrosis in patients with chronic hepatitis C virus infection: A systematic review and meta-analysis. J. Evid.-Based Med. 2018, 11, 272–277. [Google Scholar] [CrossRef]
- Naggie, S. Hepatitis C Virus, Inflammation, and Cellular Aging: Turning Back Time. Top. Antivir. Med. 2017, 25, 3–6. [Google Scholar]
- Li, H.; Huang, M.-H.; Jiang, J.-D.; Peng, Z.-G. Hepatitis C: From inflammatory pathogenesis to anti-inflammatory/hepatoprotective therapy. World J. Gastroenterol. 2018, 24, 5297–5311. [Google Scholar] [CrossRef]
- Zhan, Y.; Yu, J.; Chen, R.; Gao, J.; Ding, R.; Fu, Y.; Zhang, L.; Hu, D. Socioeconomic status and metabolic syndrome in the general population of China: A cross-sectional study. BMC Public Health 2012, 12, 921. [Google Scholar] [CrossRef] [Green Version]
- Vernay, M.; Salanave, B.; de Peretti, C.; Druet, C.; Malon, A.; Deschamps, V.; Hercberg, S.; Castetbon, K. Metabolic syndrome and socioeconomic status in France: The French Nutrition and Health Survey (ENNS, 2006–2007). Int. J. Public Health 2013, 58, 855–864. [Google Scholar] [CrossRef]
- Colombet, Z.; Perignon, M.; Salanave, B.; Landais, E.; Martin-Prevel, Y.; Allès, B.; Drogue, S.; Amiot, M.J.; Méjean, C. Socioeconomic inequalities in metabolic syndrome in the French West Indies. BMC Public Health 2019, 19, 1620. [Google Scholar] [CrossRef]
- Roguljic, H.; Nincevic, V.; Bojanic, K.; Kuna, L.; Smolic, R.; Vcev, A.; Primorac, D.; Vceva, A.; Wu, G.Y.; Smolic, M. Impact of DAA Treatment on Cardiovascular Disease Risk in Chronic HCV Infection: An Update. Front. Pharmacol. 2021, 12, 678546. Available online: https://www.frontiersin.org/articles/10.3389/fphar.2021.678546 (accessed on 4 October 2022). [CrossRef] [PubMed]
- Hengst, J.; Falk, C.S.; Schlaphoff, V.; Deterding, K.; Manns, M.P.; Cornberg, M.; Wedemeyer, H. Direct-Acting Antiviral–Induced Hepatitis C Virus Clearance Does Not Completely Restore the Altered Cytokine and Chemokine Milieu in Patients With Chronic Hepatitis C. J. Infect. Dis. 2016, 214, 1965–1974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoury, M.; Cohen, I.; Bar-Sela, G. “The Two Sides of the Same Coin”—Medical Cannabis, Cannabinoids and Immunity: Pros and Cons Explained. Pharmaceutics 2022, 14, 389. [Google Scholar] [CrossRef] [PubMed]
- Hotamisligil, G.S. Inflammation and metabolic disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef]
- Fischer, B.; Russell, C.; Sabioni, P.; van den Brink, W.; Le Foll, B.; Hall, W.; Rehm, J.; Room, R. Lower-Risk Cannabis Use Guidelines: A Compre-hensive Update of Evidence and Recommendations. Am. J. Public Health 2017, 107, e1–e12. [Google Scholar] [CrossRef]
- Braveman, P.; Gottlieb, L. The Social Determinants of Health: It’s Time to Consider the Causes of the Causes. Public Health Rep. 2014, 129, 19–31. [Google Scholar] [CrossRef] [Green Version]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.; Hosking, J.; Woodward, A.; Witten, K.; Macmillan, A.; Field, A.; Baas, P.; Mackie, H. Systematic literature review of built environment effects on physical activity and active transport—An update and new findings on health equity. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 158. [Google Scholar] [CrossRef]


{kind=link}
| Variables (% Missing Values) | Whole Study Population (n = 6364) | Cannabis Use | |||
|---|---|---|---|---|---|
| Never (n = 4283) | Former (n = 1296) | Current (n = 785) | p-Value † | ||
| n (%) or Median [IQR] | n (%) | n (%) | n (%) | ||
| Sex (0) | |||||
| Male | 3422 (53.8) | 1877 (43.8) | 927 (71.5) | 618 (78.7) | <10−3 |
| Female | 2942 (46.2) | 2406 (56.2) | 369 (28.5) | 167 (21.3) | |
| Age (years) (0) | |||||
| Median [IQR] | 56 [50;64] | 59 [51;68] | 52 [49;56] | 50 [46;55] | <10−3 |
| Place of birth (0) | |||||
| France | 4684 (73.6) | 2924 (68.3) | 1092 (84.3) | 668 (85.1) | <10−3 |
| Europe and America ‡ | 478 (7.5) | 340 (7.9) | 95 (7.3) | 43 (5.5) | |
| North Africa and Middle East | 576 (9.1) | 458 (10.7) | 71 (5.5) | 47 (6.0) | |
| Sub-Saharan Africa § | 423 (6.6) | 392 (9.2) | 19 (1.5) | 12 (1.5) | |
| Asia | 200 (3.1) | 166 (3.9) | 19 (1.5) | 15 (1.9) | |
| Coffee consumption (0.7) | |||||
| 0 cups/day | 1801 (28.5) | 1375 (32.3) | 273 (21.2) | 153 (19.6) | <10−3 |
| 1–2 cups/day | 2537 (40.1) | 1781 (41.9) | 488 (37.9) | 268 (34.4) | |
| ≥3 cups/day | 1981 (31.3) | 1096 (25.8) | 526 (40.9) | 359 (46.0) | |
| Tobacco use (0) | |||||
| Never | 2399 (37.7) | 2318 (54.1) | 55 (4.2) | 26 (3.3) | <10−3 |
| Former | 1750 (27.5) | 1131 (26.4) | 547 (42.2) | 72 (9.2) | |
| Current | 2214 (34.8) | 833 (19.5) | 694 (53.5) | 687 (87.5) | |
| Alcohol consumption ¶ (0.4) | |||||
| Abstinent with no history of unhealthy use | 2728 (43.0) | 2302 (53.9) | 274 (21.3) | 152 (19.6) | <10−3 |
| Moderate use | 2529 (39.9) | 1552 (36.3) | 614 (47.7) | 363 (46.7) | |
| Current or past unhealthy use | 1080 (17.0) | 418 (9.8) | 400 (31.1) | 262 (33.7) | |
| Living in poverty † † (2.6) | |||||
| No | 4317 (69.6) | 3015 (72.4) | 881 (69.6) | 421 (54.7) | <10−3 |
| Yes | 1885 (30.4) | 1151 (27.6) | 385 (30.4) | 349 (45.3) | |
| Educational level (1.1) | |||||
| <upper secondary school certificate | 3400 (54.0) | 2281 (53.8) | 645 (50.4) | 474 (60.8) | <10−3 |
| ≥ upper secondary school certificate | 2895 (46.0) | 1955 (46.2) | 635 (49.6) | 305 (39.2) | |
| Employment status (0.4) | |||||
| Having no job | 3526 (55.6) | 2648 (62.1) | 506 (39.1) | 372 (47.6) | <10−3 |
| Having a job | 2815 (44.4) | 1617 (37.9) | 788 (60.9) | 410 (52.4) | |
| Advanced liver fibrosis ‡ ‡ (6.5) | |||||
| No | 4404 (74.0) | 2897 (72.1) | 913 (76.3) | 594 (80.7) | <10−3 |
| Yes | 1545 (26.0) | 1120 (27.9) | 283 (23.7) | 142 (19.3) | |
| Time since HCV diagnosis (years) (2.0) | |||||
| Median [IQR] | 14.0 [6.8;19.8] | 13.7 [6.8;19.7] | 14.3 [6.3;19.7] | 15.4 [7.8;20.5] | 0.005 |
| HCV genotype | |||||
| 1 | 4133 (65.9) | 2850 (67.6) | 804 (63.0) | 479 (61.6) | <10−3 |
| 3 | 780 (12.4) | 351 (8.3) | 256 (20.1) | 173 (22.3) | |
| 4 | 761 (12.1) | 485 (11.5) | 174 (13.6) | 102 (13.1) | |
| 2/5/6/7 | 594 (9.5) | 529 (12.6) | 42 (3.3) | 23 (3.0) | |
| Central obesity (0) | |||||
| No | 2841 (44.6) | 1639 (38.3) | 682 (52.6) | 520 (66.2) | <10−3 |
| Yes | 3523 (55.4) | 2644 (61.7) | 614 (47.4) | 265 (33.8) | |
| Dyslipidemia (0) | |||||
| No | 5844 (91.8) | 3886 (90.7) | 1217 (93.9) | 741 (94.4) | <10−3 |
| Yes | 520 (8.2) | 397 (9.3) | 79 (6.1) | 44 (5.6) | |
| Hypertension (0) | |||||
| No | 4532 (71.2) | 2769 (64.7) | 1066 (82.3) | 697 (88.8) | <10−3 |
| Yes | 1832 (28.8) | 1514 (35.3) | 230 (17.7) | 88 (11.2) | |
| Diabetes (0) | |||||
| No | 5547 (87.2) | 3631 (84.8) | 1176 (90.7) | 740 (94.3) | <10−3 |
| Yes | 817 (12.8) | 652 (15.2) | 120 (9.3) | 45 (5.7) | |
| Number of metabolic disorders § § (0) | |||||
| 0 | 2145 (33.7) | 1136 (26.5) | 569 (43.9) | 440 (56.1) | <10−3 |
| 1 | 2376 (37.3) | 1628 (38.0) | 483 (37.3) | 265 (33.8) | |
| 2 | 1304 (20.5) | 1054 (24.6) | 185 (14.3) | 65 (8.3) | |
| 3 | 448 (7.0) | 389 (9.1) | 46 (3.5) | 13 (1.7) | |
| 4 | 91 (1.4) | 76 (1.8) | 13 (1.0) | 2 (0.3) | |
| Univariable Analyses | Multivariable Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | Dyslipidemia (n = 6364) | p-Value | Hypertension (n = 6364) | p-Value | Dyslipidemia (n = 6219) | p-Value | Hypertension (n = 6248) | p-Value |
| OR [95% CI] | OR [95% CI] | aOR [95% CI] | aOR [95% CI] | |||||
| Sex | ||||||||
| Male (ref.) | 1 | 1 | 1 | |||||
| Female | 1.01 [0.84;1.20] | 0.955 | 1.44 [1.29;1.61] | <10−3 | 0.87 [0.77;0.99] | 0.034 | ||
| Age (years) | 1.04 [1.03;1.04] | <10−3 | 1.08 [1.07;1.09] | <10−3 | 1.03 [1.02;1.04] | <10−3 | 1.07 [1.06;1.08] | <10−3 |
| Place of birth | 0.428 | <10−3 | <10−3 | |||||
| France (ref.) | 1 | 1 | 1 | |||||
| Europe and America † | 0.85 [0.59;1.21] | 0.362 | 1.26 [1.03;1.55] | 0.024 | 1.33 [1.07;1.67] | 0.011 | ||
| North Africa and Middle East | 0.86 [0.62;1.20] | 0.381 | 1.34 [1.11;1.61] | 0.002 | 1.04 [0.85;1.28] | 0.695 | ||
| Sub-Saharan Africa ‡ | 0.73 [0.49;1.09] | 0.126 | 2.25 [1.84;2.76] | <10−3 | 2.74 [2.19;3.43] | <10−3 | ||
| Asia | 0.81 [0.46;1.40] | 0.445 | 0.86 [0.62;1.20] | 0.389 | 1.06 [0.73;1.54] | 0.754 | ||
| Coffee consumption | 0.067 | <10−3 | 0.034 | |||||
| 0 cups/day (ref.) | 1 | 1 | 1 | |||||
| 1–2 cups/day | 1.28 [1.02;1.60] | 0.032 | 1.00 [0.88;1.13] | 0.959 | 1.05 [0.90;1.21] | 0.542 | ||
| ≥3 cups/day | 1.07 [0.84;1.36] | 0.600 | 0.53 [0.46;0.62] | <10−3 | 0.86 [0.73;1.01] | 0.070 | ||
| Cannabis use | <10−3 | <10−3 | <10−3 | |||||
| Never (ref.) | 1 | 1 | 1 | |||||
| Former | 0.64 [0.49;0.82] | <10−3 | 0.39 [0.34;0.46] | <10−3 | 0.74 [0.62;0.89] | 0.001 | ||
| Current | 0.58 [0.42;0.80] | 0.001 | 0.23 [0.18;0.29] | <10−3 | 0.45 [0.36;0.59] | <10−3 | ||
| Tobacco use | 0.026 | <10−3 | ||||||
| Never (ref.) | 1 | 1 | ||||||
| Former | 1.04 [0.84;1.29] | 0.723 | 0.72 [0.63;0.82] | <10−3 | ||||
| Current | 0.78 [0.63;0.97] | 0.023 | 0.32 [0.28;0.37] | <10−3 | ||||
| Alcohol consumption § | 0.100 | <10−3 | 0.006 | |||||
| Abstinent with no history of unhealthy use (ref.) | 1 | 1 | 1 | |||||
| Moderate use | 1.19 [0.98;1.44] | 0.084 | 0.65 [0.57;0.73] | <10−3 | 1.39 [1.14;1.70] | 0.001 | ||
| Current or past unhealthy use | 0.93 [0.71;1.22] | 0.591 | 0.62 [0.53;0.73] | <10−3 | 1.15 [0.87;1.52] | 0.331 | ||
| Living in poverty ¶ | ||||||||
| No (ref.) | 1 | 1 | ||||||
| Yes | 0.77 [0.63;0.95] | 0.014 | 0.96 [0.85;1.08] | 0.517 | ||||
| Educational level | ||||||||
| <upper secondary school certificate (ref.) | 1 | 1 | 1 | |||||
| ≥upper secondary school certificate | 0.98 [0.82;1.17] | 0.832 | 0.67 [0.60;0.75] | <10−3 | 0.79 [0.70;0.90] | <10−3 | ||
| Employment status | ||||||||
| Having no job (ref.) | 1 | 1 | 1 | 1 | ||||
| Having a job | 0.58 [0.48;0.70] | <10−3 | 0.38 [0.34;0.43] | <10−3 | 0.80 [0.64;1.00] | 0.046 | 0.80 [0.69;0.92] | 0.002 |
| Advanced liver fibrosis † † | ||||||||
| No (ref.) | 1 | 1 | ||||||
| Yes | 0.98 [0.79;1.21] | 0.843 | 1.66 [1.47;1.88] | <10−3 | ||||
| Time since HCV diagnosis (years) | 1.01 [1.00;1.02] | 0.026 | 1.01 [1.00;1.02] | 0.003 | ||||
| HCV genotype | <10−3 | <10−3 | 0.005 | |||||
| 1 (ref.) | 1 | 1 | 1 | |||||
| 3 | 0.51 [0.36;0.73] | <10−3 | 0.61 [0.51;0.74] | <10−3 | 0.63 [0.44;0.91] | 0.013 | ||
| 4 | 1.00 [0.76;1.32] | 0.993 | 0.95 [0.80;1.13] | 0.563 | 1.22 [0.92;1.62] | 0.176 | ||
| 2/5/6/7 | 1.48 [1.13;1.94] | 0.005 | 1.36 [1.14;1.63] | 0.001 | 1.31 [0.99;1.73] | 0.059 |
| Variables | Univariable Analyses (n = 6364) | p-Value | Multivariable Analysis (n = 5779) | p-Value |
|---|---|---|---|---|
| IRR [95% CI] | aIRR [95% CI] | |||
| Sex | ||||
| Male (ref.) | 1 | 1 | ||
| Female | 1.09 [1.02;1.17] | 0.017 | 0.82 [0.76;0.88] | <10−3 |
| Age (years) | 1.04 [1.04;1.05] | <10−3 | 1.03 [1.03;1.04] | <10−3 |
| Place of birth | <10−3 | <10−3 | ||
| France (ref.) | 1 | 1 | ||
| Europe and America † | 1.07 [0.93;1.22] | 0.358 | 1.08 [0.94;1.22] | 0.277 |
| North Africa and Middle East | 1.38 [1.24;1.54] | <10−3 | 1.10 [0.98;1.23] | 0.104 |
| Sub-Saharan Africa ‡ | 1.57 [1.39;1.76] | <10−3 | 1.53 [1.35;1.74] | <10−3 |
| Asia | 0.95 [0.75;1.20] | 0.675 | 1.08 [0.85;1.37] | 0.547 |
| Coffee consumption | <10−3 | 0.011 | ||
| 0 cups/day (ref.) | 1 | 1 | ||
| 1–2 cups/day | 1.06 [0.97;1.15] | 0.187 | 1.11 [1.02;1.21] | 0.011 |
| ≥3 cups/day | 0.71 [0.64;0.78] | <10−3 | 1.00 [0.90;1.11] | 0.962 |
| Cannabis use | <10−3 | <10−3 | ||
| Never (ref.) | 1 | 1 | ||
| Former | 0.55 [0.50;0.62] | <10−3 | 0.80 [0.71;0.90] | <10−3 |
| Current | 0.38 [0.32;0.44] | <10−3 | 0.53 [0.44;0.63] | <10−3 |
| Tobacco use | <10−3 | |||
| Never (ref.) | 1 | |||
| Former | 0.90 [0.83;0.98] | 0.011 | ||
| Current | 0.54 [0.49;0.59] | <10−3 | ||
| Alcohol consumption § | <10−3 | |||
| Abstinent with no history of unhealthy use (ref.) | 1 | |||
| Moderate use | 0.79 [0.73;0.85] | <10−3 | ||
| Current or past unhealthy use | 0.81 [0.73;0.90] | <10−3 | ||
| Living in poverty ¶ | ||||
| No (ref.) | 1 | |||
| Yes | 1.02 [0.94;1.10] | 0.695 | ||
| Educational level | ||||
| <upper secondary school certificate (ref.) | 1 | 1 | ||
| ≥upper secondary school certificate | 0.76 [0.71;0.82] | <10−3 | 0.87 [0.81;0.94] | <10−3 |
| Employment status | ||||
| Having no job (ref.) | 1 | 1 | ||
| Having a job | 0.51 [0.47;0.55] | <10−3 | 0.80 [0.73;0.88] | <10−3 |
| Advanced liver fibrosis † † | ||||
| No (ref.) | 1 | 1 | ||
| Yes | 1.47 [1.37;1.59] | <10−3 | 1.13 [1.05;1.22] | 0.002 |
| Time since HCV diagnosis (years) | 1.01 [1.00;1.01] | 0.001 | ||
| HCV genotype | <10−3 | 0.039 | ||
| 1 (ref.) | 1 | 1 | ||
| 3 | 0.68 [0.60;0.78] | <10−3 | 0.94 [0.83;1.08] | 0.404 |
| 4 | 1.03 [0.92;1.16] | 0.553 | 1.16 [1.03;1.31] | 0.013 |
| 2/5/6/7 | 1.21 [1.09;1.35] | 0.001 | 0.97 [0.87;1.08] | 0.528 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barré, T.; Bourlière, M.; Ramier, C.; Carrat, F.; Di Beo, V.; Protopopescu, C.; Marcellin, F.; Bureau, M.; Cagnot, C.; Dorival, C.; et al. Cannabis Use Is Inversely Associated with Metabolic Disorders in Hepatitis C-Infected Patients (ANRS CO22 Hepather Cohort). J. Clin. Med. 2022, 11, 6135. https://doi.org/10.3390/jcm11206135
Barré T, Bourlière M, Ramier C, Carrat F, Di Beo V, Protopopescu C, Marcellin F, Bureau M, Cagnot C, Dorival C, et al. Cannabis Use Is Inversely Associated with Metabolic Disorders in Hepatitis C-Infected Patients (ANRS CO22 Hepather Cohort). Journal of Clinical Medicine. 2022; 11(20):6135. https://doi.org/10.3390/jcm11206135
Chicago/Turabian StyleBarré, Tangui, Marc Bourlière, Clémence Ramier, Fabrice Carrat, Vincent Di Beo, Camelia Protopopescu, Fabienne Marcellin, Morgane Bureau, Carole Cagnot, Céline Dorival, and et al. 2022. "Cannabis Use Is Inversely Associated with Metabolic Disorders in Hepatitis C-Infected Patients (ANRS CO22 Hepather Cohort)" Journal of Clinical Medicine 11, no. 20: 6135. https://doi.org/10.3390/jcm11206135