
A Prospective, Case-Control Study of Serum Metabolomics in Neonates with Late-Onset Sepsis and Necrotizing Enterocolitis

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Sample Collection and Preparation
2.2.1. Sample Collection
2.2.2. Sample Preparation
2.3. Liquid Chromatography–Quadrupole Time-of-Flight Mass Spectrometry (LC–QTOF-MS) Analysis
2.3.1. Liquid Chromatography
2.3.2. Mass Spectrometry
2.4. Data Handling and Statistical Analysis
3. Results
3.1. Demographic and Clinical Data of the Study Population
3.2. Untargeted Metabolomic Analysis
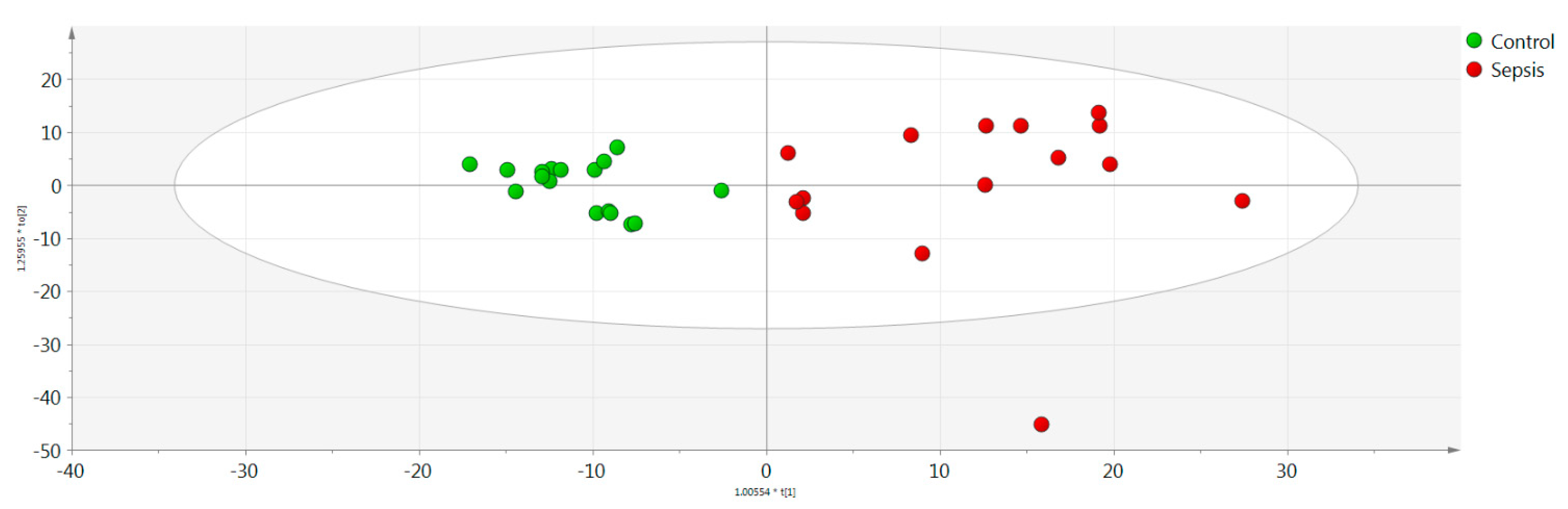
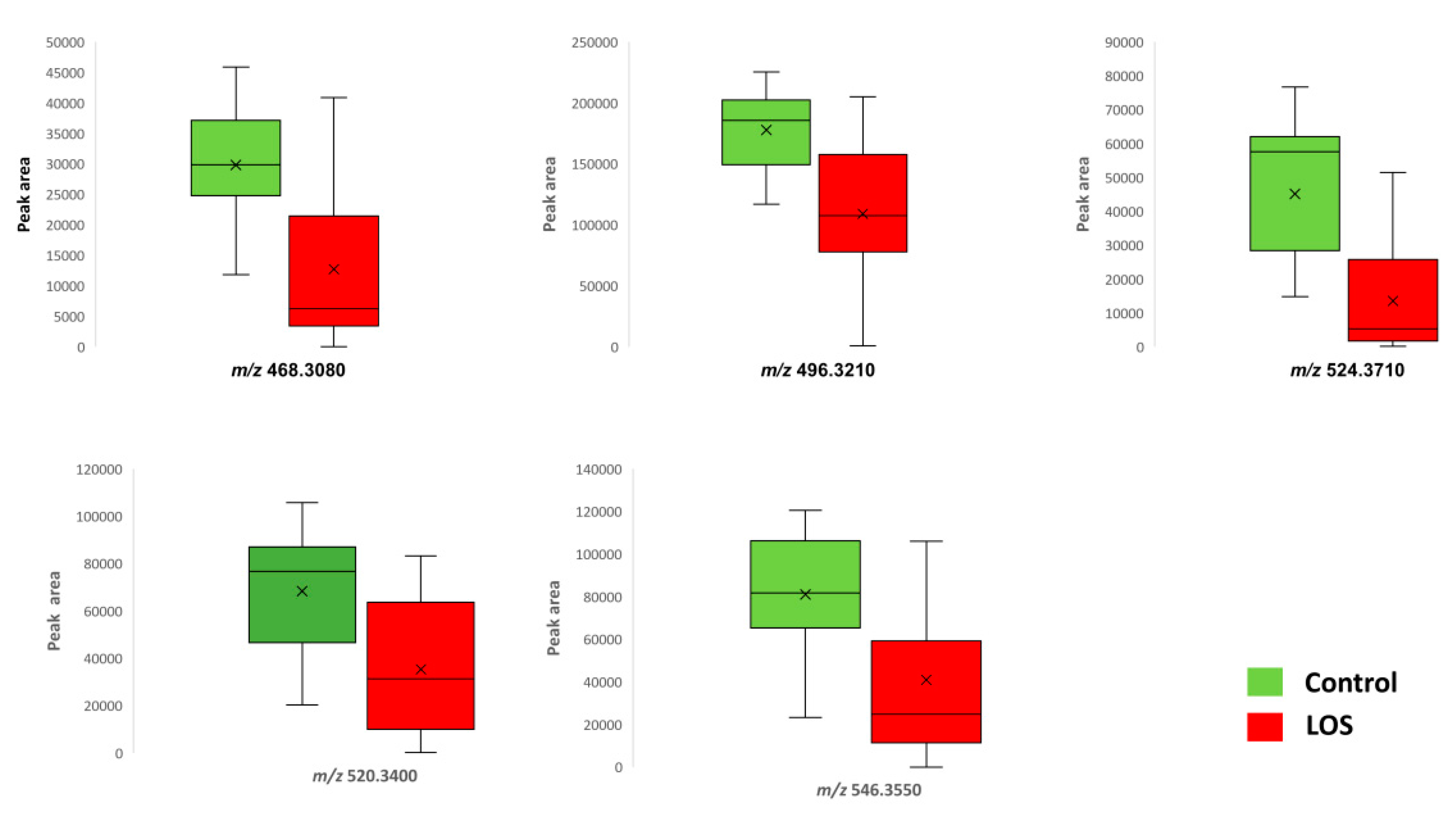
3.2.1. Untargeted Metabolomics LOS
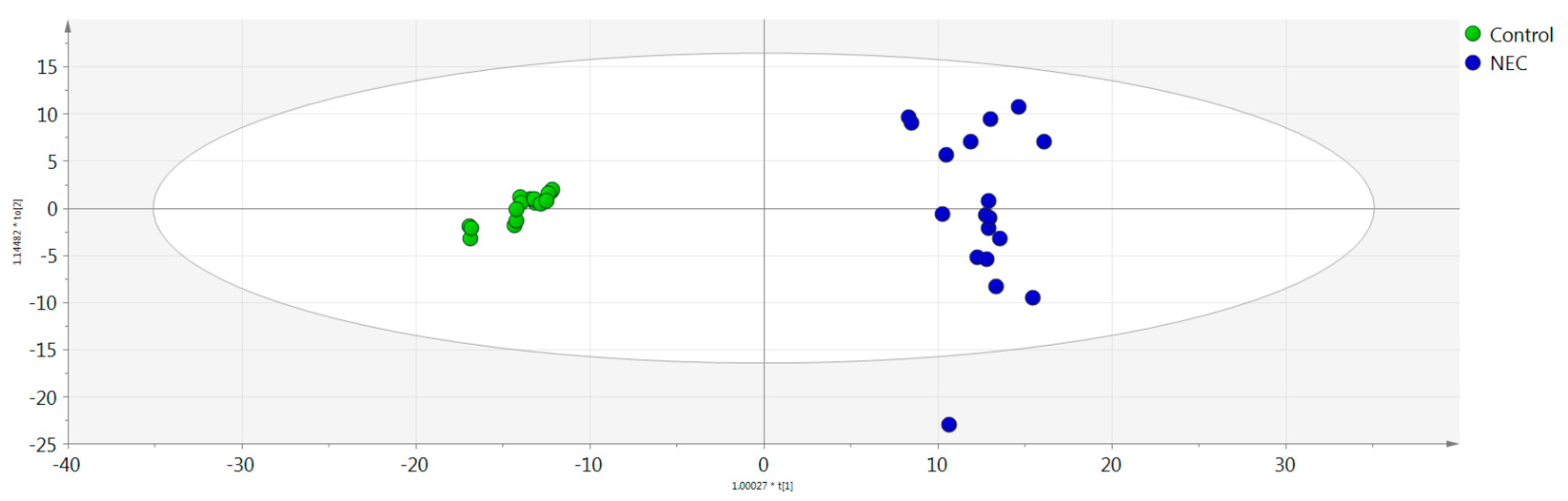
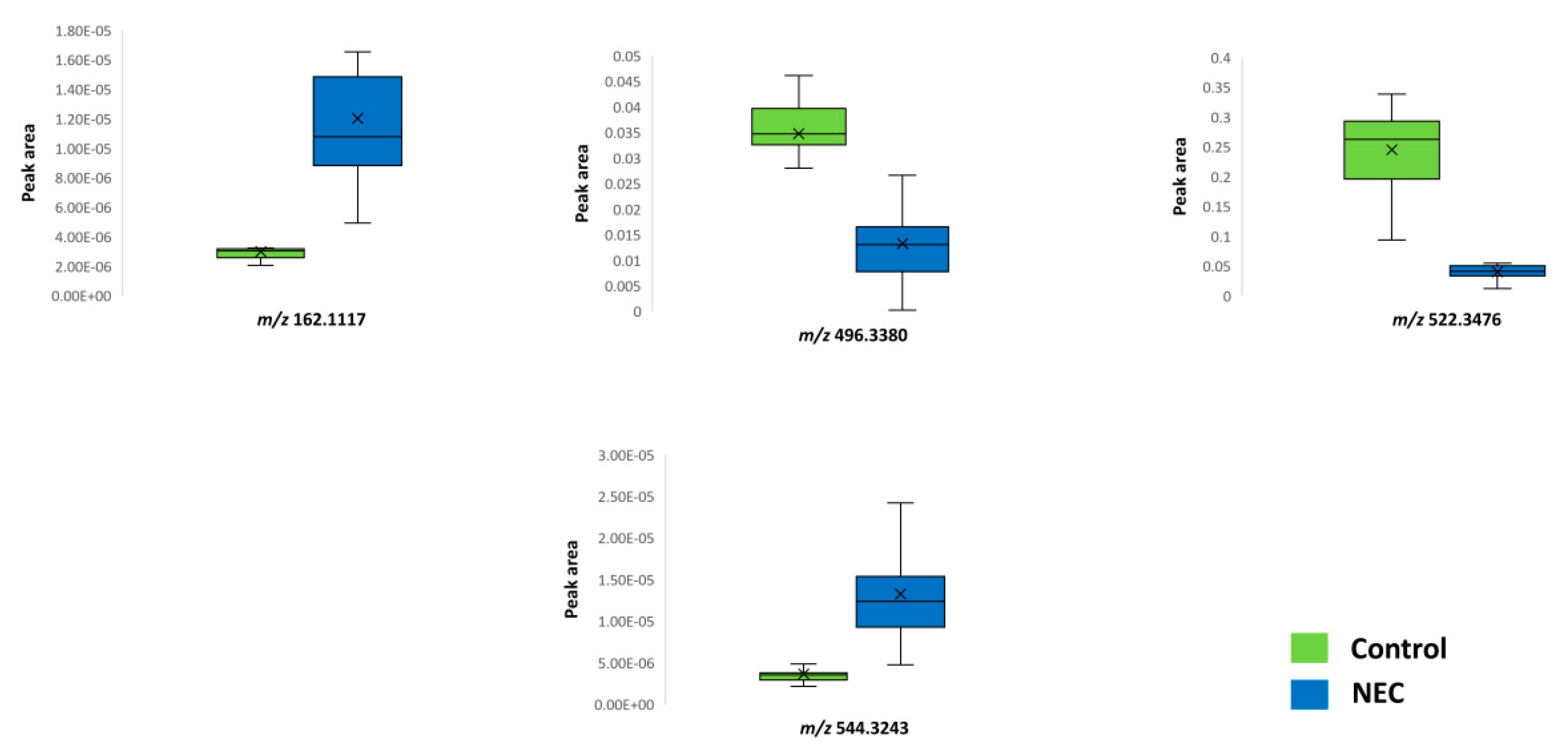
3.2.2. Untargeted Metabolomics NEC
3.2.3. Metabolites Identification
4. Discussion
4.1. Neonates with LOS
4.2. Neonates with NEC
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- EMA Expert Meeting on Neonatal and Paediatric Sepsis. Available online: https://www.ema.europa.eu/en/events/expert-meeting-neonatal-paediatric-sepsis (accessed on 5 May 2022).
- Tuzun, F.; Ozkan, H.; Cetinkaya, M.; Yucesoy, E.; Kurum, O.; Cebeci, B.; Cakmak, E.; Ozkutuk, A.; Keskinoglu, P.; Baysal, B.; et al. Is European Medicines Agency (EMA) Sepsis Criteria Accurate for Neonatal Sepsis Diagnosis or Do We Need New Criteria? PLoS ONE 2019, 14, e0218002. [Google Scholar] [CrossRef]
- Eaton, S.; Rees, C.M.; Hall, N.J. Current Research in Necrotizing Enterocolitis. Early Hum. Dev. 2016, 97, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Stoll, B.J.; Hansen, N.; Fanaroff, A.A.; Wright, L.L.; Carlo, W.A.; Ehrenkranz, R.A.; Lemons, J.A.; Donovan, E.F.; Stark, A.R.; Tyson, J.E.; et al. Late-Onset Sepsis in Very Low Birth Weight Neonates: The Experience of the NICHD Neonatal Research Network. Pediatrics 2002, 110, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Lutsar, I.; Chazallon, C.; Trafojer, U.; de Cabre, V.M.; Auriti, C.; Bertaina, C.; Calo Carducci, F.I.; Canpolat, F.E.; Esposito, S.; Fournier, I.; et al. Meropenem vs Standard of Care for Treatment of Neonatal Late Onset Sepsis (NeoMero1): A Randomised Controlled Trial. PLoS ONE 2020, 15, e0229380. [Google Scholar] [CrossRef]
- Jones, I.H.; Hall, N.J. Contemporary Outcomes for Infants with Necrotizing Enterocolitis—A Systematic Review. J. Pediatr. 2020, 220, 86–92.e3. [Google Scholar] [CrossRef]
- McGovern, M.; Flynn, L.; Coyne, S.; Molloy, E.J. Question 2: Does Coagulase Negative Staphylococcal Sepsis Cause Neurodevelopmental Delay in Preterm Infants? Arch. Dis. Child. 2019, 104, 97–100. [Google Scholar] [CrossRef] [PubMed]
- INIS Collaborative Group; Brocklehurst, P.; Farrell, B.; King, A.; Juszczak, E.; Darlow, B.; Haque, K.; Salt, A.; Stenson, B.; Tarnow-Mordi, W. Treatment of Neonatal Sepsis with Intravenous Immune Globulin. N. Engl. J. Med. 2011, 365, 1201–1211. [Google Scholar] [CrossRef] [PubMed]
- Niemarkt, H.J.; de Meij, T.G.J.; van de Velde, M.E.; van der Schee, M.P.; van Goudoever, J.B.; Kramer, B.W.; Andriessen, P.; de Boer, N.K.H. Necrotizing Enterocolitis: A Clinical Review on Diagnostic Biomarkers and the Role of the Intestinal Microbiota. Inflamm. Bowel Dis. 2015, 21, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Agakidou, E.; Agakidis, C.; Gika, H.; Sarafidis, K. Emerging Biomarkers for Prediction and Early Diagnosis of Necrotizing Enterocolitis in the Era of Metabolomics and Proteomics. Front. Pediatr. 2020, 8, 602255. [Google Scholar] [CrossRef]
- Theodoridis, G.A.; Gika, H.G.; Want, E.J.; Wilson, I.D. Liquid Chromatography-Mass Spectrometry Based Global Metabolite Profiling: A Review. Anal. Chim. Acta 2012, 711, 7–16. [Google Scholar] [CrossRef]
- Gika, H.G.; Theodoridis, G.A.; Plumb, R.S.; Wilson, I.D. Current Practice of Liquid Chromatography-Mass Spectrometry in Metabolomics and Metabonomics. J. Pharm. Biomed. Anal. 2014, 87, 12–25. [Google Scholar] [CrossRef] [PubMed]
- Gude, S.S.; Peddi, N.C.; Vuppalapati, S.; Venu Gopal, S.; Marasandra Ramesh, H.; Gude, S.S. Biomarkers of Neonatal Sepsis: From Being Mere Numbers to Becoming Guiding Diagnostics. Cureus 2022, 14, e23215. [Google Scholar] [CrossRef] [PubMed]
- Fanos, V.; Caboni, P.; Corsello, G.; Stronati, M.; Gazzolo, D.; Noto, A.; Lussu, M.; Dessì, A.; Giuffrè, M.; Lacerenza, S.; et al. Urinary (1)H-NMR and GC-MS Metabolomics Predicts Early and Late Onset Neonatal Sepsis. Early Hum. Dev. 2014, 90 (Suppl. S1), S78–S83. [Google Scholar] [CrossRef]
- Dessì, A.; Liori, B.; Caboni, P.; Corsello, G.; Giuffrè, M.; Noto, A.; Serraino, F.; Stronati, M.; Zaffanello, M.; Fanos, V. Monitoring Neonatal Fungal Infection with Metabolomics. J. Matern. Fetal Neonatal Med. 2014, 27 (Suppl. S2), 34–38. [Google Scholar] [CrossRef] [PubMed]
- Sarafidis, K.; Chatziioannou, A.C.; Thomaidou, A.; Gika, H.; Mikros, E.; Benaki, D.; Diamanti, E.; Agakidis, C.; Raikos, N.; Drossou, V.; et al. Urine Metabolomics in Neonates with Late-Onset Sepsis in a Case-Control Study. Sci. Rep. 2017, 7, 45506. [Google Scholar] [CrossRef]
- Morrow, A.L.; Lagomarcino, A.J.; Schibler, K.R.; Taft, D.H.; Yu, Z.; Wang, B.; Altaye, M.; Wagner, M.; Gevers, D.; Ward, D.V.; et al. Early Microbial and Metabolomic Signatures Predict Later Onset of Necrotizing Enterocolitis in Preterm Infants. Microbiome 2013, 1, 13. [Google Scholar] [CrossRef]
- Thomaidou, A.; Chatziioannou, A.C.; Deda, O.; Benaki, D.; Gika, H.; Mikros, E.; Agakidis, C.; Raikos, N.; Theodoridis, G.; Sarafidis, K. A Pilot Case-Control Study of Urine Metabolomics in Preterm Neonates with Necrotizing Enterocolitis. J. Chromatogr. B 2019, 1117, 10–21. [Google Scholar] [CrossRef] [PubMed]
- Picaud, J.-C.; De Magistris, A.; Mussap, M.; Corbu, S.; Dessì, A.; Noto, A.; Fanos, V.; Cesare Marincola, F. Urine NMR Metabolomics Profile of Preterm Infants with Necrotizing Enterocolitis Over the First Two Months of Life: A Pilot Longitudinal Case-Control Study. Front. Mol. Biosci. 2021, 8, 680159. [Google Scholar] [CrossRef]
- Berkhout, D.J.C.; van Keulen, B.J.; Niemarkt, H.J.; Bessem, J.R.; de Boode, W.P.; Cossey, V.; Hoogenes, N.; Hulzebos, C.V.; Klaver, E.; Andriessen, P.; et al. Late-Onset Sepsis in Preterm Infants Can Be Detected Preclinically by Fecal Volatile Organic Compound Analysis: A Prospective, Multicenter Cohort Study. Clin. Infect. Dis. 2019, 68, 70–77. [Google Scholar] [CrossRef]
- Rusconi, B.; Jiang, X.; Sidhu, R.; Ory, D.S.; Warner, B.B.; Tarr, P.I. Gut Sphingolipid Composition as a Prelude to Necrotizing Enterocolitis. Sci. Rep. 2018, 8, 10984. [Google Scholar] [CrossRef] [Green Version]
- Mickiewicz, B.; Vogel, H.J.; Wong, H.R.; Winston, B.W. Metabolomics as a Novel Approach for Early Diagnosis of Pediatric Septic Shock and Its Mortality. Am. J. Respir. Crit. Care Med. 2013, 187, 967–976. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.J.; Nelson, A.; Treumann, A.; Skeath, T.; Cummings, S.P.; Embleton, N.D.; Berrington, J.E. Metabolomic and Proteomic Analysis of Serum from Preterm Infants with Necrotising Entercolitis and Late-Onset Sepsis. Pediatr. Res. 2016, 79, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Wilcock, A.; Begley, P.; Stevens, A.; Whatmore, A.; Victor, S. The Metabolomics of Necrotising Enterocolitis in Preterm Babies: An Exploratory Study. J. Matern. Fetal Neonatal Med. 2016, 29, 758–762. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Li, W.; Wang, G.; Yu, M.; Zhong, J.; Xu, C.; Li, D.; Zhou, Y. Gas Chromatography-Mass Spectrometry Based Serum Metabolic Analysis for Premature Infants and the Relationship with Necrotizing Enterocolitis: A Cross-Sectional Study. Ital. J. Pediatr. 2019, 45, 54. [Google Scholar] [CrossRef]
- Sinclair, T.J.; Ye, C.; Chen, Y.; Zhang, D.; Li, T.; Ling, X.B.; Cohen, H.J.; Shaw, G.M.; Stevenson, D.K.; Chace, D.; et al. Progressive Metabolic Dysfunction and Nutritional Variability Precedes Necrotizing Enterocolitis. Nutrients 2020, 12, E1275. [Google Scholar] [CrossRef] [PubMed]
- Mardegan, V.; Giordano, G.; Stocchero, M.; Pirillo, P.; Poloniato, G.; Donadel, E.; Salvadori, S.; Giaquinto, C.; Priante, E.; Baraldi, E. Untargeted and Targeted Metabolomic Profiling of Preterm Newborns with EarlyOnset Sepsis: A Case-Control Study. Metabolites 2021, 11, 115. [Google Scholar] [CrossRef] [PubMed]
- Moltu, S.J.; Sachse, D.; Blakstad, E.W.; Strømmen, K.; Nakstad, B.; Almaas, A.N.; Westerberg, A.C.; Rønnestad, A.; Brække, K.; Veierød, M.B.; et al. Urinary Metabolite Profiles in Premature Infants Show Early Postnatal Metabolic Adaptation and Maturation. Nutrients 2014, 6, 1913–1930. [Google Scholar] [CrossRef]
- Kliegman, R.M.; Walsh, M.C. Neonatal Necrotizing Enterocolitis: Pathogenesis, Classification, and Spectrum of Illness. Curr. Probl. Pediatr. 1987, 17, 213–288. [Google Scholar] [CrossRef]
- Gika, H.G.; Theodoridis, G.A.; Wingate, J.E.; Wilson, I.D. Within-Day Reproducibility of an HPLC-MS-Based Method for Metabonomic Analysis: Application to Human Urine. J. Proteom. Res. 2007, 6, 3291–3303. [Google Scholar] [CrossRef]
- Pang, Z.; Zhou, G.; Ewald, J.; Chang, L.; Hacariz, O.; Basu, N.; Xia, J. Using MetaboAnalyst 5.0 for LC–HRMS Spectra Processing, Multi-Omics Integration and Covariate Adjustment of Global Metabolomics Data. Nat. Protoc. 2022, 17, 1735–1761. [Google Scholar] [CrossRef]
- Gika, H.G.; Macpherson, E.; Theodoridis, G.A.; Wilson, I.D. Evaluation of the Repeatability of Ultra-Performance Liquid Chromatography-TOF-MS for Global Metabolic Profiling of Human Urine Samples. J. Chromatogr. B 2008, 871, 299–305. [Google Scholar] [CrossRef]
- Boldyreva, L.V.; Morozova, M.V.; Saydakova, S.S.; Kozhevnikova, E.N. Fat of the Gut: Epithelial Phospholipids in Inflammatory Bowel Diseases. Int. J. Mol. Sci. 2021, 22, 11682. [Google Scholar] [CrossRef] [PubMed]
- Vance, D.E. Phospholipid Methylation in Mammals: From Biochemistry to Physiological Function. Biochim. Biophys. Acta 2014, 1838, 1477–1487. [Google Scholar] [CrossRef]
- Nilsson, Å.; Duan, R.-D. Pancreatic and Mucosal Enzymes in Choline Phospholipid Digestion. Am. J. Physiol. Gastrointest. Liver Physiol. 2019, 316, G425–G445. [Google Scholar] [CrossRef]
- Ferrario, M.; Brunelli, L.; Su, F.; Herpain, A.; Pastorelli, R. The Systemic Alterations of Lipids, Alanine-Glucose Cycle and Inter-Organ Amino Acid Metabolism in Swine Model Confirms the Role of Liver in Early Phase of Septic Shock. Front. Physiol. 2019, 10, 11. [Google Scholar] [CrossRef] [PubMed]
- Schmerler, D.; Neugebauer, S.; Ludewig, K.; Bremer-Streck, S.; Brunkhorst, F.M.; Kiehntopf, M. Targeted Metabolomics for Discrimination of Systemic Inflammatory Disorders in Critically Ill Patients. J. Lipid Res. 2012, 53, 1369–1375. [Google Scholar] [CrossRef]
- Drobnik, W.; Liebisch, G.; Audebert, F.-X.; Frohlich, D.; Gluck, T.; Vogel, P.; Rothe, G.; Schmitz, G. Plasma Ceramide and Lysophosphatidylcholine Inversely Correlate with Mortality in Sepsis Patients. J. Lipid Res. 2003, 44, 754–761. [Google Scholar] [CrossRef]
- Cho, W.H.; Park, T.; Park, Y.Y.; Huh, J.W.; Lim, C.-M.; Koh, Y.; Song, D.-K.; Hong, S.-B. Clinical Significance of Enzymatic Lysophosphatidylcholine (LPC) Assay Data in Patients with Sepsis. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 1805–1810. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.J.; Jung, J.S.; Lee, J.E.; Lee, J.; Huh, S.O.; Kim, H.S.; Jung, K.C.; Cho, J.Y.; Nam, J.S.; Suh, H.W.; et al. Therapeutic Effects of Lysophosphatidylcholine in Experimental Sepsis. Nat. Med. 2004, 10, 161–167. [Google Scholar] [CrossRef]
- Park, D.W.; Kwak, D.S.; Park, Y.Y.; Chang, Y.; Huh, J.W.; Lim, C.M.; Koh, Y.; Song, D.K.; Hong, S.B. Impact of Serial Measurements of Lysophosphatidylcholine on 28-Day Mortality Prediction in Patients Admitted to the Intensive Care Unit with Severe Sepsis or Septic Shock. J. Crit. Care 2014, 29, 882.e5–882.e11. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.H.; Shin, M.H.; Park, J.M.; Lee, S.G.; Ku, N.S.; Kim, Y.S.; Park, M.S.; Pyun, J.C.; Chung, K.S. Diagnosis and Mortality Prediction of Sepsis via Lysophosphatidylcholine 16:0 Measured by MALDI-TOF MS. Sci. Rep. 2020, 10, 13833. [Google Scholar] [CrossRef] [PubMed]
- Treede, I.; Braun, A.; Sparla, R.; Kühnel, M.; Giese, T.; Turner, J.R.; Anes, E.; Kulaksiz, H.; Füllekrug, J.; Stremmel, W.; et al. Anti-Inflammatory Effects of Phosphatidylcholine. J. Biol. Chem. 2007, 282, 27155–27164. [Google Scholar] [CrossRef] [PubMed]
- Ehehalt, R.; Wagenblast, J.; Erben, G.; Lehmann, W.D.; Hinz, U.; Merle, U.; Stremmel, W. Phosphatidylcholine and Lysophosphatidylcholine in Intestinal Mucus of Ulcerative Colitis Patients. A Quantitative Approach by NanoElectrospray-Tandem Mass Spectrometry. Scand. J. Gastroenterol. 2004, 39, 737–742. [Google Scholar] [CrossRef] [PubMed]
- Geiger, O.; López-Lara, I.M.; Sohlenkamp, C. Phosphatidylcholine Biosynthesis and Function in Bacteria. Biochim. Biophys. Acta 2013, 1831, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Mingorance, C.; Rodríguez-Rodríguez, R.; Justo, M.L.; Alvarez de Sotomayor, M.; Herrera, M.D. Critical Update for the Clinical Use of L-Carnitine Analogs in Cardiometabolic Disorders. Vasc. Health Risk Manag. 2011, 7, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.-J.; Lin, J.-S.; Lin, Y.-C.; Lin, P.-T. Effects of L-Carnitine Supplementation on Oxidative Stress and Antioxidant Enzymes Activities in Patients with Coronary Artery Disease: A Randomized, Placebo-Controlled Trial. Nutr. J. 2014, 13, 79. [Google Scholar] [CrossRef]
- Akisu, M.; Ozmen, D.; Baka, M.; Habif, S.; Yalaz, M.; Arslanoglu, S.; Kultursay, N.; Bayindir, O. Protective Effect of Dietary Supplementation with L-Arginine and L-Carnitine on Hypoxia/Reoxygenation-Induced Necrotizing Enterocolitis in Young Mice. Neonatology 2002, 81, 260–265. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| m/z_RT | VIP | p(corr) | q-Value | Possible Identity |
|---|---|---|---|---|
| 468.308_7.5 | 3.5 | −0.71 | 3.7 × 10−4 | PC (14:0/0:0) or LysoPC (14:0/0:0) |
| 496.321_8.6 | 6.8 | −0.66 | 1.2 × 10−3 | PC (16:0/0:0) or LysoPC (16:0/0:0) |
| 520.340_8.0 | 4.3 | −0.52 | 3.7 × 10−3 | PC (18:2/0:0) or LysoPC (18:2/0:0) |
| 524.371_9.5 | 4.4 | −0.67 | 3.6 × 10−4 | PC (18:0/0:0) or LysoPC (18:0/0:0) |
| 546.355_8.5 | 4.6 | −0.55 | 5.4 × 10−3 | PC (20:3/0:0) or LysoPC (20:3/0:0) |
| 594.378_9.2 | 1.5 | 0.64 | 2.7 × 10−2 | Unknown |
| 638.939_9.0 | 1.4 | 0.55 | 5.4 × 10−2 | Unknown |
| m/z_RT | VIP | q-Value | p(corr) | Possible Identity |
|---|---|---|---|---|
| 120.0808_2.1 | 1.4 | 3.3 × 10−5 | 0.73 | Unknown |
| 146.0593_2.9 | 1.34 | 2.1 × 10−4 | 0.71 | Unknown |
| 162.1117_0.7 | 1.33 | 3.1 × 10−4 | 0.71 | L-carnitine |
| 188.0693_2.9 | 1.36 | 1.3 × 10−4 | 0.72 | Unknown |
| 225.1968_6.3 | 1.36 | 9.2 × 10−5 | 0.73 | Unknown |
| 272.2582_6.7 | 1.3 | 4.0 × 10−4 | 0.74 | Unknown |
| 496.3380_8.4 | 1.28 | 1.4 × 10−3 | −0.78 | PC (16:0/0:0) or LysoPC (16:0/0:0) |
| 522.3476_9.0 | 1.52 | 1.4 × 10−3 | −0.87 | PC (18:1/0:0) or LysoPC (18:1/0:0) |
| 544.3243_8.2 | 1.39 | 4.8 × 10−3 | 0.73 | PC(20:4/0:0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thomaidou, A.; Deda, O.; Begou, O.; Lioupi, A.; Kontou, A.; Gika, H.; Agakidou, E.; Theodoridis, G.; Sarafidis, K. A Prospective, Case-Control Study of Serum Metabolomics in Neonates with Late-Onset Sepsis and Necrotizing Enterocolitis. J. Clin. Med. 2022, 11, 5270. https://doi.org/10.3390/jcm11185270
Thomaidou A, Deda O, Begou O, Lioupi A, Kontou A, Gika H, Agakidou E, Theodoridis G, Sarafidis K. A Prospective, Case-Control Study of Serum Metabolomics in Neonates with Late-Onset Sepsis and Necrotizing Enterocolitis. Journal of Clinical Medicine. 2022; 11(18):5270. https://doi.org/10.3390/jcm11185270
Chicago/Turabian StyleThomaidou, Agathi, Olga Deda, Olga Begou, Artemis Lioupi, Angeliki Kontou, Helen Gika, Eleni Agakidou, Georgios Theodoridis, and Kosmas Sarafidis. 2022. "A Prospective, Case-Control Study of Serum Metabolomics in Neonates with Late-Onset Sepsis and Necrotizing Enterocolitis" Journal of Clinical Medicine 11, no. 18: 5270. https://doi.org/10.3390/jcm11185270