
Cystoid Macular Edema after Rhegmatogenous Retinal Detachment Repair with Pars Plana Vitrectomy: Rate, Risk Factors, and Outcomes

 , , , , , ,
, , , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Data Sources and Measurements
2.3. Patient Selection and Groups
2.4. Outcomes
2.5. Statistical Analysis
3. Results
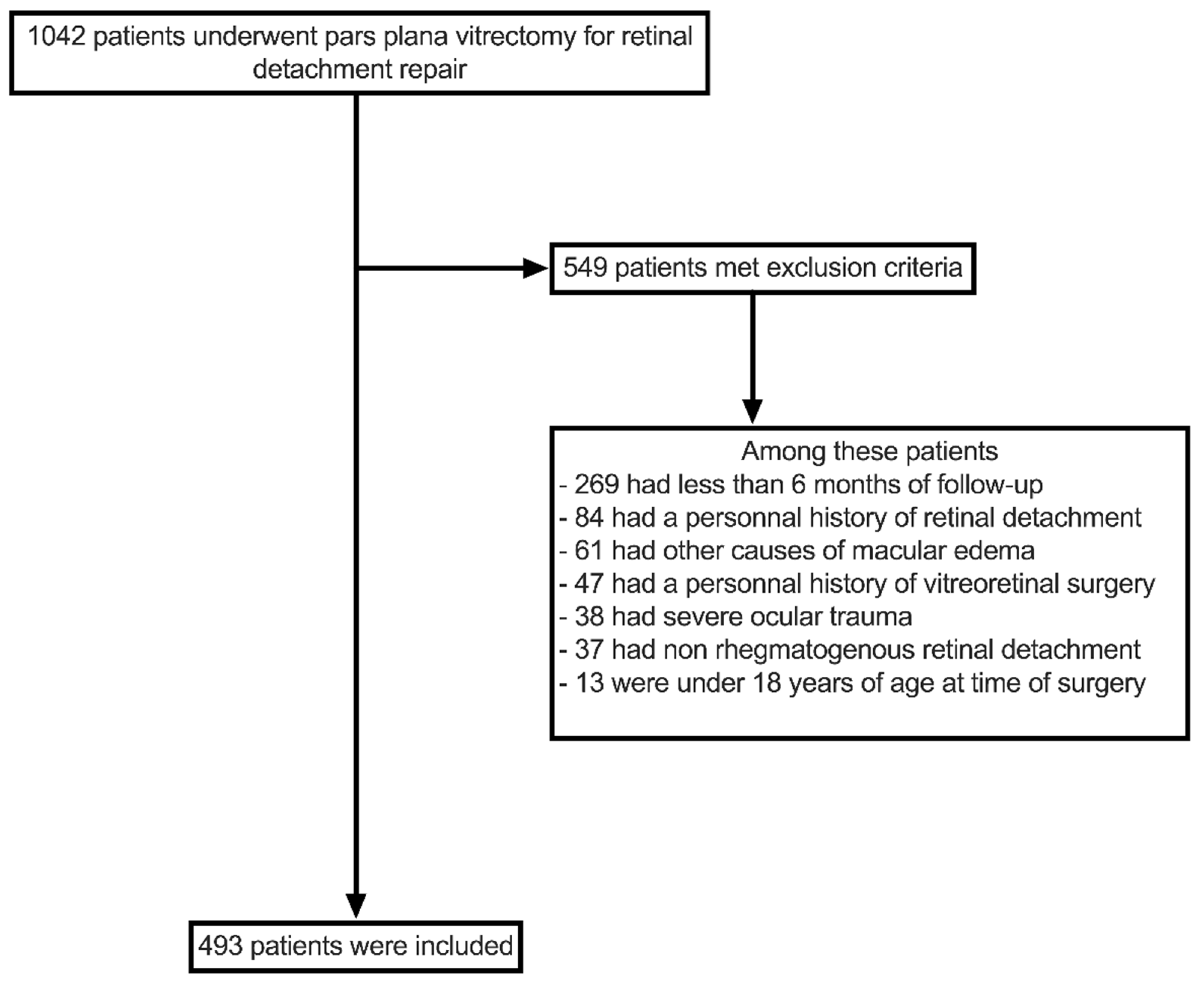
3.1. Study Participants
3.2. Cystoid Macular Edema Rate and Risk Factors
3.3. Visual and Anatomical Outcomes
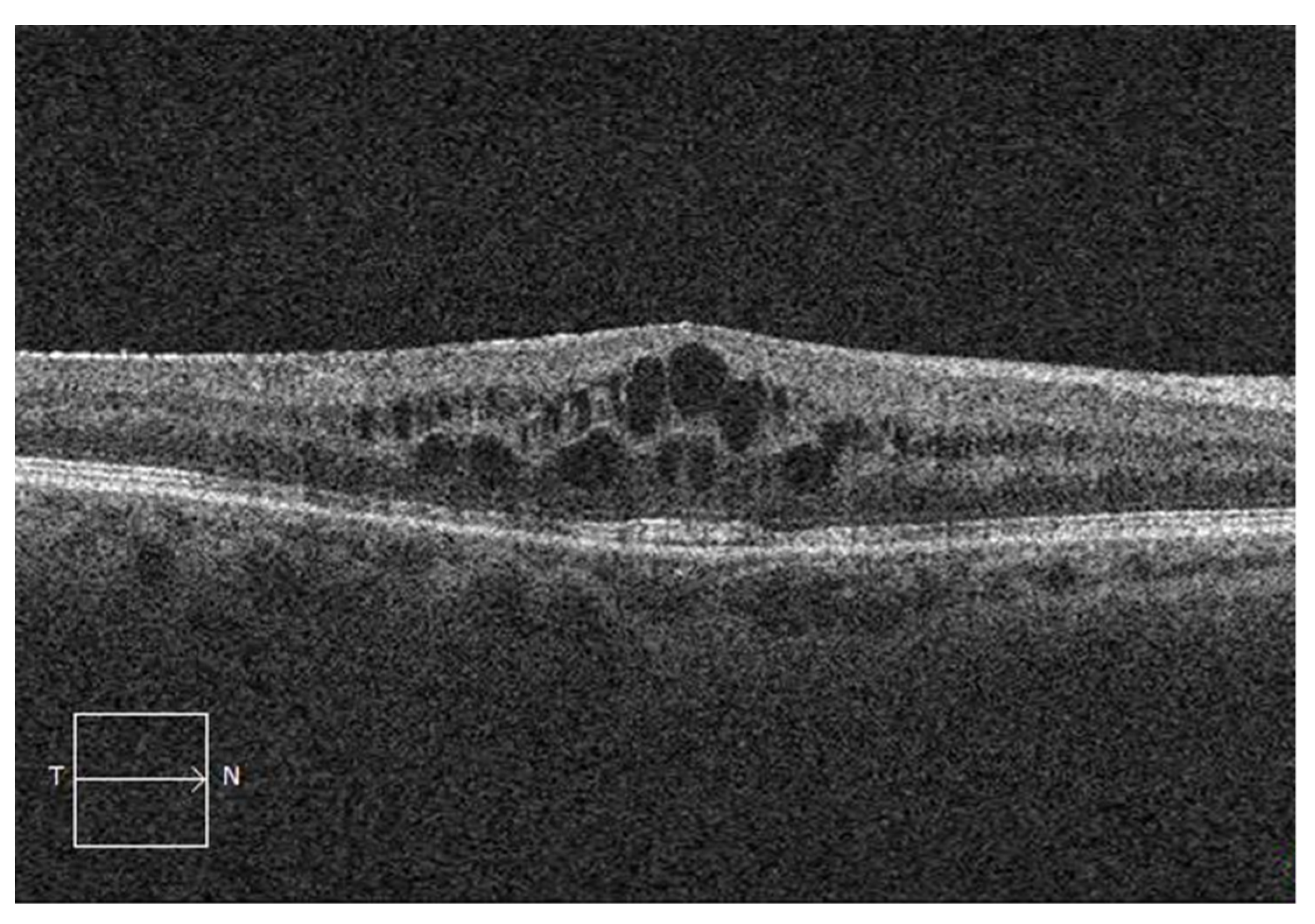
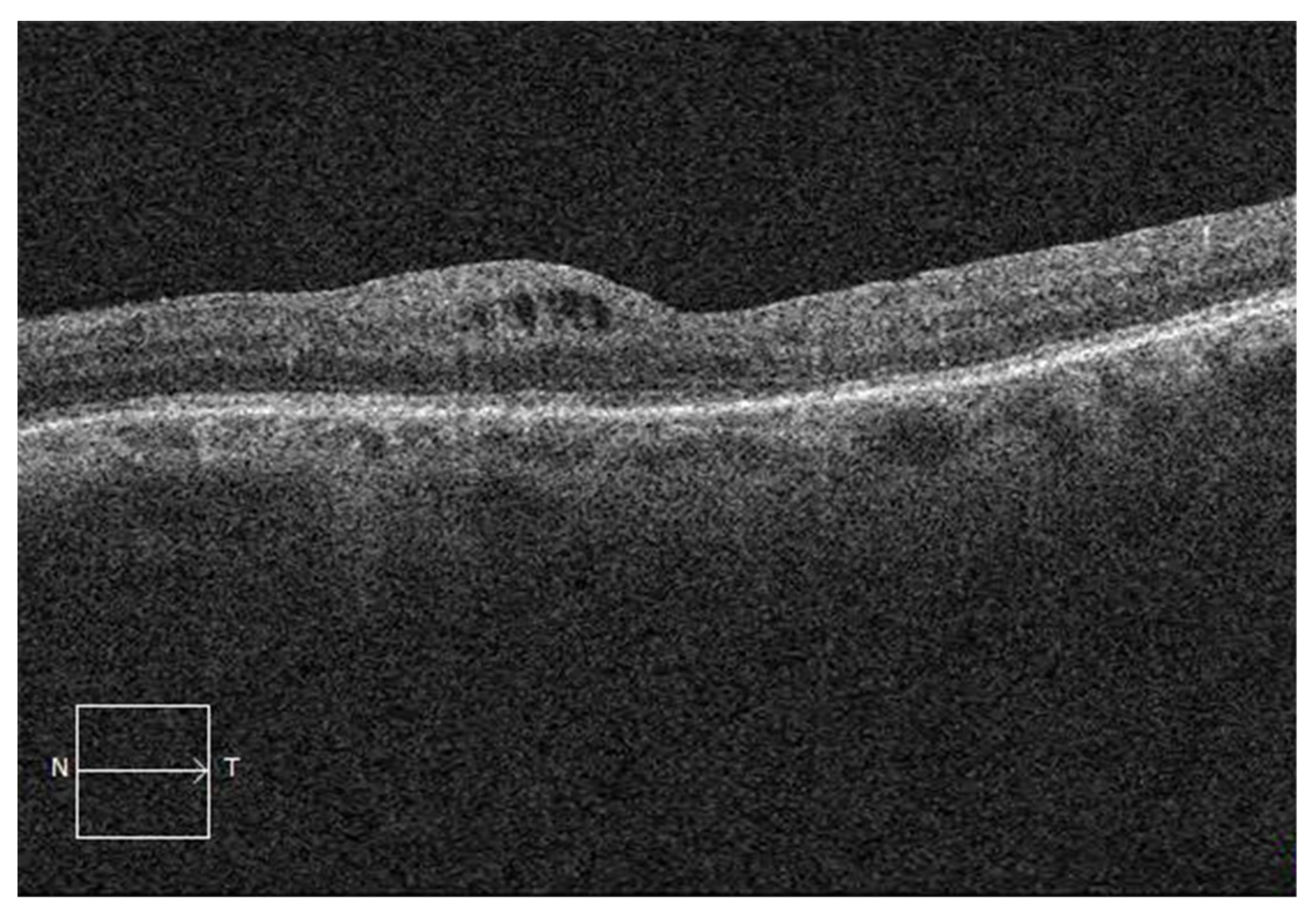
3.4. SD-OCT Characteristics of Postoperative CME
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rowe, J.A.; Erie, J.C.; Baratz, K.H.; Hodge, D.O.; Gray, D.T.; Butterfield, L.; Robertson, D.M. Retinal detachment in Olmsted County, Minnesota, 1976 through 1995. Ophthalmology 1999, 106, 154–159. [Google Scholar] [CrossRef]
- Steel, D.; Fraser, S. Retinal detachment. BMJ Clin. Evid. 2008, 2008, 710. [Google Scholar]
- Ross, W.H. Visual recovery after macula-off retinal detachment. Eye 2002, 16, 440–446. [Google Scholar] [CrossRef]
- Miller, D.M.; Riemann, C.D.; Foster, R.E.; Petersen, M.R. Primary repair of retinal detachment with 25-gauge pars plana vitrectomy. Retina 2008, 28, 931–936. [Google Scholar] [CrossRef] [PubMed]
- Shinkai, Y.; Oshima, Y.; Yoneda, K.; Kogo, J.; Imai, H.; Watanabe, A.; Matsui, Y.; Suzuki, K.; Sotozono, C. Multicenter survey of sutureless 27-gauge vitrectomy for primary rhegmatogenous retinal detachment: A consecutive series of 410 cases. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 2591–2600. [Google Scholar] [CrossRef] [PubMed]
- Moinuddin, O.; Abuzaitoun, R.O.; Hwang, M.W.; Sathrasala, S.K.; Chen, X.D.; Stein, J.D.; Johnson, M.W.; Zacks, D.N.; Wubben, T.J.; Besirli, C.G. Surgical repair of primary non-complex rhegmatogenous retinal detachment in the modern era of small-gauge vitrectomy. BMJ Open Ophthalmol. 2021, 6, e000651. [Google Scholar] [CrossRef]
- Okamoto, F.; Sugiura, Y.; Okamoto, Y.; Hiraoka, T.; Oshika, T. Metamorphopsia and optical coherence tomography findings after rhegmatogenous retinal detachment surgery. Am. J. Ophthalmol. 2014, 157, 214–220.e211. [Google Scholar] [CrossRef] [PubMed]
- Delolme, M.P.; Dugas, B.; Nicot, F.; Muselier, A.; Bron, A.M.; Creuzot-Garcher, C. Anatomical and functional macular changes after rhegmatogenous retinal detachment with macula off. Am. J. Ophthalmol. 2012, 153, 128–136. [Google Scholar] [CrossRef]
- Meredith, T.A.; Reeser, F.H.; Topping, T.M.; Aaberg, T.M. Cystoid macular edema after retinal detachment surgery. Ophthalmology 1980, 87, 1090–1095. [Google Scholar] [CrossRef]
- Dormegny, L.; Jeanjean, L.C.; Liu, X.; Messerlin, A.; Bourcier, T.; Sauer, A.; Speeg-Schatz, C.; Gaucher, D. Visual Impairment and Macular Vascular Remodeling Secondary to Retrograde Maculopathy in Retinal Detachment Treated with Silicon Oil Tamponade. Retina 2021, 41, 309–316. [Google Scholar] [CrossRef]
- Gharbiya, M.; Grandinetti, F.; Scavella, V.; Cecere, M.; Esposito, M.; Segnalini, A.; Gabrieli, C.B. Correlation between spectral-domain optical coherence tomography findings and visual outcome after primary rhegmatogenous retinal detachment repair. Retina 2012, 32, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Saber, E.E.; Bayoumy, A.S.M.; Elmohamady, M.N.; Faramawi, H.M. Macular microstructure and visual acuity after macula-off retinal detachment repair by 23-gauge vitrectomy plus silicone endotamponade. Clin. Ophthalmol. 2018, 12, 2005–2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Augustin, A.; Loewenstein, A.; Kuppermann, B.D. Macular edema. General pathophysiology. Dev. Ophthalmol. 2010, 47, 10–26. [Google Scholar]
- Bringmann, A.; Reichenbach, A.; Wiedemann, P. Pathomechanisms of cystoid macular edema. Ophthalmic Res. 2004, 36, 241–249. [Google Scholar] [CrossRef]
- Tranos, P.G.; Wickremasinghe, S.S.; Stangos, N.T.; Topouzis, F.; Tsinopoulos, I.; Pavesio, C.E. Macular edema. Surv. Ophthalmol. 2004, 49, 470–490. [Google Scholar] [CrossRef]
- Zur, D.; Loewenstein, A. Postsurgical Cystoid Macular Edema. Dev. Ophthalmol. 2017, 58, 178–190. [Google Scholar] [PubMed]
- Daruich, A.; Matet, A.; Moulin, A.; Kowalczuk, L.; Nicolas, M.; Sellam, A.; Rothschild, P.R.; Omri, S.; Gélizé, E.; Jonet, L.; et al. Mechanisms of macular edema: Beyond the surface. Prog. Retin. Eye Res. 2018, 63, 20–68. [Google Scholar] [CrossRef] [PubMed]
- Catier, A.; Tadayoni, R.; Paques, M.; Erginay, A.; Haouchine, B.; Gaudric, A.; Massin, P. Characterization of macular edema from various etiologies by optical coherence tomography. Am. J. Ophthalmol. 2005, 140, 200–206. [Google Scholar] [CrossRef]
- Li, Y.; Xia, X.; Paulus, Y.M. Advances in Retinal Optical Imaging. Photonics 2018, 5, 9. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.Y.; Kim, H.K.; Kim, S.H.; Kim, S.S. Incidence and Risk Factors of Cystoid Macular Edema after Vitrectomy with Silicone Oil Tamponade for Retinal Detachment. Korean J. Ophthalmol. 2018, 32, 204–210. [Google Scholar] [CrossRef]
- Sabates, N.R.; Sabates, F.N.; Sabates, R.; Lee, K.Y.; Ziemianski, M.C. Macular changes after retinal detachment surgery. Am. J. Ophthalmol. 1989, 108, 22–29. [Google Scholar] [CrossRef]
- Ahmadieh, H.; Moradian, S.; Faghihi, H.; Parvaresh, M.M.; Ghanbari, H.; Mehryar, M.; Heidari, E.; Behboudi, H.; Banaee, T.; Golestan, B. Anatomic and visual outcomes of scleral buckling versus primary vitrectomy in pseudophakic and aphakic retinal detachment: Six-month follow-up results of a single operation—Report no. 1. Ophthalmology 2005, 112, 1421–1429. [Google Scholar] [CrossRef] [PubMed]
- Pole, C.; Chehaibou, I.; Govetto, A.; Garrity, S.; Schwartz, S.D.; Hubschman, J.P. Macular edema after rhegmatogenous retinal detachment repair: Risk factors, OCT analysis, and treatment responses. Int. J. Retin. Vitr. 2021, 7, 9. [Google Scholar] [CrossRef] [PubMed]
- Chatziralli, I.; Theodossiadis, G.; Dimitriou, E.; Kazantzis, D.; Theodossiadis, P. Macular Edema after Successful Pars Plana Vitrectomy for Rhegmatogenous Retinal Detachment: Factors Affecting Edema Development and Considerations for Treatment. Ocul. Immunol. Inflamm. 2021, 29, 187–192. [Google Scholar] [CrossRef]
- Rossetti, L.; Chaudhuri, J.; Dickersin, K. Medical prophylaxis and treatment of cystoid macular edema after cataract surgery. The results of a meta-analysis. Ophthalmology 1998, 105, 397–405. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Baudin, F.; Deschasse, C.; Gabrielle, P.H.; Berrod, J.P.; Le Mer, Y.; Arndt, C.; Tadayoni, R.; Delyfer, M.N.; Weber, M.; Gaucher, D.; et al. Functional and anatomical outcomes after successful repair of macula-off retinal detachment: A 12-month follow-up of the DOREFA study. Acta Ophthalmol. 2021, 99, e1190–e1197. [Google Scholar] [CrossRef]
- Banker, T.P.; Reilly, G.S.; Jalaj, S.; Weichel, E.D. Epiretinal membrane and cystoid macular edema after retinal detachment repair with small-gauge pars plana vitrectomy. Eur. J. Ophthalmol. 2015, 25, 565–570. [Google Scholar] [CrossRef]
- Han, J.V.; Patel, D.V.; Squirrell, D.; McGhee, C.N. Cystoid macular oedema following cataract surgery: A review. Clin. Exp. Ophthalmol. 2019, 47, 346–356. [Google Scholar] [CrossRef] [Green Version]
- Kobashi, H.; Takano, M.; Yanagita, T.; Shiratani, T.; Wang, G.; Hoshi, K.; Shimizu, K. Scleral buckling and pars plana vitrectomy for rhegmatogenous retinal detachment: An analysis of 542 eyes. Curr. Eye Res. 2014, 39, 204–211. [Google Scholar] [CrossRef]
- Bourla, D.H.; Bor, E.; Axer-Siegel, R.; Mimouni, K.; Weinberger, D. Outcomes and complications of rhegmatogenous retinal detachment repair with selective sutureless 25-gauge pars plana vitrectomy. Am. J. Ophthalmol. 2010, 149, 630–634.e631. [Google Scholar] [CrossRef] [PubMed]
- Joseph, D.P.; Ryan, E.H.; Ryan, C.M.; Forbes, N.J.; Wagley, S.; Yonekawa, Y.; Mittra, R.A.; Parke, D.W.; Emerson, G.G.; Shah, G.K.; et al. Primary Retinal Detachment Outcomes Study: Pseudophakic Retinal Detachment Outcomes: Primary Retinal Detachment Outcomes Study Report Number 3. Ophthalmology 2020, 127, 1507–1514. [Google Scholar] [CrossRef] [PubMed]
- Reeves, M.-G.R.; Afshar, A.R.; Pershing, S. Need for Retinal Detachment Reoperation Based on Primary Repair Method Among Commercially Insured Patients, 2003–2016. Am. J. Ophthalmol. 2021, 229, 71–81. [Google Scholar] [CrossRef]
- Mohabati, D.; Hoyng, C.B.; Yzer, S.; Boon, C.J.F. Clinical characteristics and outcome of posterior cystoid macular degeneration in chronic central serous chorioretinopathy. Retina 2020, 40, 1742–1750. [Google Scholar] [CrossRef] [PubMed]
- Romano, V.; Angi, M.; Scotti, F.; Del Grosso, R.; Romano, D.; Semeraro, F.; Vinciguerra, P.; Costagliola, C.; Romano, M.R. Inflammation and macular oedema after pars plana vitrectomy. Mediat. Inflamm. 2013, 2013, e971758. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| n = 493 | |
|---|---|
| Age (year) | 63 (10.9) |
| Gender-Male | 324 (65.7%) |
| Lens status | |
| Phakic | 304 (61.7%) |
| Pseudophakic | 187 (37.9%) |
| Aphakic | 2 (0.4%) |
| Axial length (mm) * | 24.78 (1.78) |
| Diabetes mellitus * | 43 (8.78%) |
| Initial BCVA (LogMAR) * | 1.23 (0.93) |
| Extent of RRD (1–4 quadrants) | |
| 1 | 66 (13.4%) |
| 2 | 209 (42.4%) |
| 3 | 90 (18.2%) |
| 4 | 128 (26.0%) |
| Number of retinal tears * | |
| 0 | 23 (4.7%) |
| 1 | 253 (51.7%) |
| 2 | 101 (20.7%) |
| 3 | 57 (11.7%) |
| 4 and more | 55 (11.2%) |
| Proliferative vitreoretinopathy * | |
| Grade A | 101 (21.0%) |
| Grade B | 305 (63.6%) |
| Grade C | 74 (15.4%) |
| Macular status | |
| On | 138 (28.0%) |
| Off | 355 (72.0%) |
| Time to surgery after first symptoms (days) * | 17 (22) |
| Surgical procedure | |
| Pseudophakic-PPV only | 182 (36.9%) |
| Phakic-PPV only | 258 (52.3%) |
| Phakic-PPV with simultaneous PKE | 53 (10.8%) |
| Secondary cataract surgery | |
| Not applicable | 272 (55.2%) |
| Under 3 months | 51 (10.3%) |
| Between 3 and 6 months | 81 (16.4%) |
| Between 6 and 12 months | 89 (18.1%) |
| Single surgery anatomical success | 370 (75.0%) |
| Cystoid macular edema rate within the first 12 months *,† | 165 (33.9%) |
| Cystoid macular edema rate at 12 months * | 97 (28.1%) |
| nCME (n = 248) | aCME (n = 97) | OR * | 95% CI | p Value | |
|---|---|---|---|---|---|
| Age (year) | 62 (56, 69) | 65 (57, 70) | 1.00 | 0.98–1.02 | 0.86 |
| Gender-Male | 165 (66.5%) | 61 (62.9%) | 0.85 | 0.52–1.40 | 0.52 |
| Lens status | |||||
| Phakic | 155 (62.5%) | 60 (61.9%) | — | — | |
| Pseudophakic | 92 (37.1%) | 37 (38.1%) | 1.04 | 0.64–1.68 | 0.88 |
| Aphakic | 1 (0.4%) | 0 (0.0%) | 0.00 | >0.99 | |
| Axial length (mm) † | 24.44 (23.68, 25.70) | 24.64 (23.95, 25.65) | 1.03 | 0.88–1.20 | 0.73 |
| Diabetes mellitus † | 22 (8.9%) | 10 (10.4%) | 1.19 | 0.52–2.55 | 0.67 |
| Initial BCVA (LogMAR) † | 0.85 (0.16, 2.30) | 2.30 (0.70, 2.30) | 1.72 | 1.32–2.27 | <0.001 |
| Macular status-Off | 175 (71.0%) | 79 (81.4%) | 1.80 | 1.02–3.28 | 0.048 |
| Extent of RRD (1–4 quadrants) | 1.43 | 1.13–1.81 | 0.003 | ||
| 1 | 36 (14.5%) | 7 (7.2%) | |||
| 2 | 107 (43.1%) | 36 (37.1%) | |||
| 3 | 49 (19.8%) | 17 (17.6%) | |||
| 4 | 56 (22.6%) | 37 (38.1%) | |||
| Proliferative vitreoretinopathy † | |||||
| Grade A and B | 215 (89.2%) | 64 (67.4%) | — | — | |
| Grade C | 26 (10.8%) | 31 (32.6%) | 4.01 | 2.22–7.28 | <0.001 |
| Vitreous hemorrhage | 37 (14.9%) | 12 (12.4%) | 0.81 | 0.39–1.58 | 0.54 |
| Time to surgery after first symptoms (days) † | 10 (5, 20) | 8 (5, 14) | 1.01 | 1.00–1.02 | 0.19 |
| Surgical procedure | |||||
| Phakic-PPV only | 136 (54.8%) | 49 (50.5%) | — | — | |
| Pseudophakic-PPV only | 92 (37.1%) | 36 (37.1%) | 1.09 | 0.65–1.80 | 0.75 |
| Phakic-PPV with simultaneous PKE | 20 (8.1%) | 12 (12.4%) | 1.67 | 0.74–3.62 | 0.20 |
| Tamponade agent | |||||
| Hexafluoride (SF6) | 161 (64.9%) | 47 (48.5%) | — | — | |
| Air | 2 (0.8%) | 0 (0.0%) | 0.00 | 0.98 | |
| Hexafluoroethane (C2F6) | 45 (18.2%) | 20 (20.6%) | 1.52 | 0.81–2.81 | 0.18 |
| Octafluoropropane (C3F8) | 5 (2.0%) | 1 (1.0%) | 0.69 | 0.04–4.39 | 0.73 |
| Silicone oil | 35 (14.1%) | 29 (29.9%) | 2.84 | 1.57–5.13 | <0.001 |
| Retinopexy type † | |||||
| Cryotherapy | 65 (26.4%) | 9 (9.3%) | — | — | |
| Endolaser | 135 (54.9%) | 75 (77.3%) | 4.01 | 1.98–9.05 | <0.001 |
| Combined cryotherapy and endolaser | 46 (18.7%) | 13 (13.4%) | 2.04 | 0.81–5.33 | 0.13 |
| Retinotomy † | 66 (26.7%) | 28 (28.9%) | 1.11 | 0.65–1.86 | 0.69 |
| Retinectomy † | 2 (0.8%) | 5 (5.2%) | 6.66 | 1.41–47.1 | 0.02 |
| Internal limiting membrane peeling † | 27 (10.9%) | 26 (27.1%) | 3.03 | 1.65–5.54 | <0.001 |
| Use of PFCL † | 38 (15.5%) | 34 (35.4%) | 3.00 | 1.74–5.17 | <0.001 |
| Surgeon experience-fellow surgeon | 122 (49.2%) | 51 (52.6%) | 1.15 | 0.72–1.84 | 0.57 |
| Secondary cataract surgery within 6 months | 64 (25.8%) | 34 (35.1%) | 1.55 | 0.93–2.56 | 0.09 |
| Single surgery anatomical success | 194 (78.2%) | 60 (61.9%) | 2.22 | 1.33–3.68 | 0.002 |
| Number of RRD repair within 12 months † | 1.88 | 1.38–2.60 | <0.001 | ||
| 1 | 201 (81.1%) | 59 (61.5%) | |||
| 2 | 33 (13.3%) | 21 (21.9%) | |||
| 3 | 11 (4.4%) | 10 (10.4%) | |||
| 4 | 3 (1.2%) | 6 (6.2%) | |||
| Retinal re-detachment within 3 months † | 34 (13.7%) | 28 (29.2%) | 2.59 | 1.46–4.58 | 0.001 |
| nCME (n = 236) | aCME (n = 91) | OR * | 95% CI | p Value | |
|---|---|---|---|---|---|
| Initial BCVA (LogMAR) | 0.85 (0.16, 2.30) | 2.30 (0.81, 2.30) | 1.55 | 1.07–2.25 | 0.02 |
| Macular status-Off | 168 (71.2%) | 77 (84.6%) | 1.16 | 0.51–2.71 | 0.72 |
| Extent of RRD (1–4 quadrants) | 1.01 | 0.72–1.42 | 0.95 | ||
| 1 | 32 (13.6%) | 5 (5.5%) | |||
| 2 | 103 (43.6%) | 34 (37.4%) | |||
| 3 | 46 (19.5%) | 15 (16.5%) | |||
| 4 | 55 (23.3%) | 37 (40.6%) | |||
| Proliferative vitreoretinopathy | |||||
| Grade A and B | 211 (89.4%) | 62 (68.1%) | — | — | |
| Grade C | 25 (10.6%) | 29 (31.9%) | 2.88 | 1.04–8.16 | 0.04 |
| Tamponade agent | |||||
| Hexafluoride (SF6) | 153 (64.8%) | 45 (49.4%) | — | — | |
| Air | 2 (0.9%) | 0 (0.0%) | 0.00 | 0.99 | |
| Hexafluoroethane (C2F6) | 43 (18.2%) | 17 (18.7%) | 0.80 | 0.36–1.70 | 0.57 |
| Octafluoropropane (C3F8) | 5 (2.1%) | 1 (1.1%) | 0.29 | 0.01–2.44 | 0.32 |
| Silicone oil | 33 (14.0%) | 28 (30.8%) | 0.65 | 0.22–1.78 | 0.41 |
| Retinopexy type | |||||
| Cryotherapy | 63 (26,7%) | 8 (8.8%) | — | — | |
| Endolaser | 128 (54.2%) | 70 (76.9%) | 3.06 | 1.33–7.84 | 0.01 |
| Combined cryotherapy and endolaser | 45 (19.1%) | 13 (14.3%) | 1.46 | 0.52–4.23 | 0.47 |
| Retinectomy | 2 (0.9%) | 4 (4.4%) | 1.86 | 0.31–15.0 | 0.51 |
| Internal limiting membrane peeling | 26 (11.0%) | 26 (28.6%) | 0.97 | 0.36–2.51 | 0.94 |
| Use of PFCL | 37 (15.7%) | 33 (36.3%) | 1.43 | 0.60–3.35 | 0.41 |
| Secondary cataract surgery within 6 months | 59 (25.0%) | 31 (34.1%) | 1.96 | 1.06–3.63 | 0.03 |
| Single surgery anatomical success | 189 (80.1%) | 57 (62.6%) | 0.67 | 0.18–2.15 | 0.51 |
| Number of RRD repair within 12 months | 2.09 | 1.00–4.67 | 0.06 | ||
| 1 | 196 (83.0%) | 57 (62.6%) | |||
| 2 | 29 (12.3%) | 21 (23.1%) | |||
| 3 | 9 (3.8%) | 8 (8.8%) | |||
| 4 | 2 (0.9%) | 5 (5.5%) | |||
| Retinal re-detachment within 3 months | 28 (11.9%) | 25 (27.5%) | 1.18 | 0.39–3.67 | 0.77 |
| tCME (n = 56) | cCME (n = 105) | OR * | 95% CI | p Value | |
|---|---|---|---|---|---|
| Outer retinal layer alteration | 38 (67.9%) | 86 (81.9%) | 2.14 | 1.01–4.56 | 0.046 |
| Macular cysts localization | |||||
| IRL | 41 (73.2%) | 35 (33.3%) | |||
| ORL | 1 (1.8%) | 4 (3.8%) | 4.69 | 0.66–94.0 | 0.18 |
| IRL and ORL | 12 (21.4%) | 66 (62.9%) | 6.44 | 3.08–14.3 | <0.001 |
| Subretinal fluid | 3 (5.4%) | 12 (11.4%) | 2.28 | 0.69–10.3 | 0.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merad, M.; Vérité, F.; Baudin, F.; Ghezala, I.B.; Meillon, C.; Bron, A.M.; Arnould, L.; Eid, P.; Creuzot-Garcher, C.; Gabrielle, P.-H. Cystoid Macular Edema after Rhegmatogenous Retinal Detachment Repair with Pars Plana Vitrectomy: Rate, Risk Factors, and Outcomes. J. Clin. Med. 2022, 11, 4914. https://doi.org/10.3390/jcm11164914
Merad M, Vérité F, Baudin F, Ghezala IB, Meillon C, Bron AM, Arnould L, Eid P, Creuzot-Garcher C, Gabrielle P-H. Cystoid Macular Edema after Rhegmatogenous Retinal Detachment Repair with Pars Plana Vitrectomy: Rate, Risk Factors, and Outcomes. Journal of Clinical Medicine. 2022; 11(16):4914. https://doi.org/10.3390/jcm11164914
Chicago/Turabian StyleMerad, Malik, Fabien Vérité, Florian Baudin, Inès Ben Ghezala, Cyril Meillon, Alain Marie Bron, Louis Arnould, Pétra Eid, Catherine Creuzot-Garcher, and Pierre-Henry Gabrielle. 2022. "Cystoid Macular Edema after Rhegmatogenous Retinal Detachment Repair with Pars Plana Vitrectomy: Rate, Risk Factors, and Outcomes" Journal of Clinical Medicine 11, no. 16: 4914. https://doi.org/10.3390/jcm11164914