
The Incidence of Severe Hypercalcaemia-Induced Mental Status Changes in Patients Treated with Antibiotic-Loaded Calcium Sulphate Depot for Orthopaedic Infections


Abstract
:1. Introduction
2. Patients and Methods
3. Results
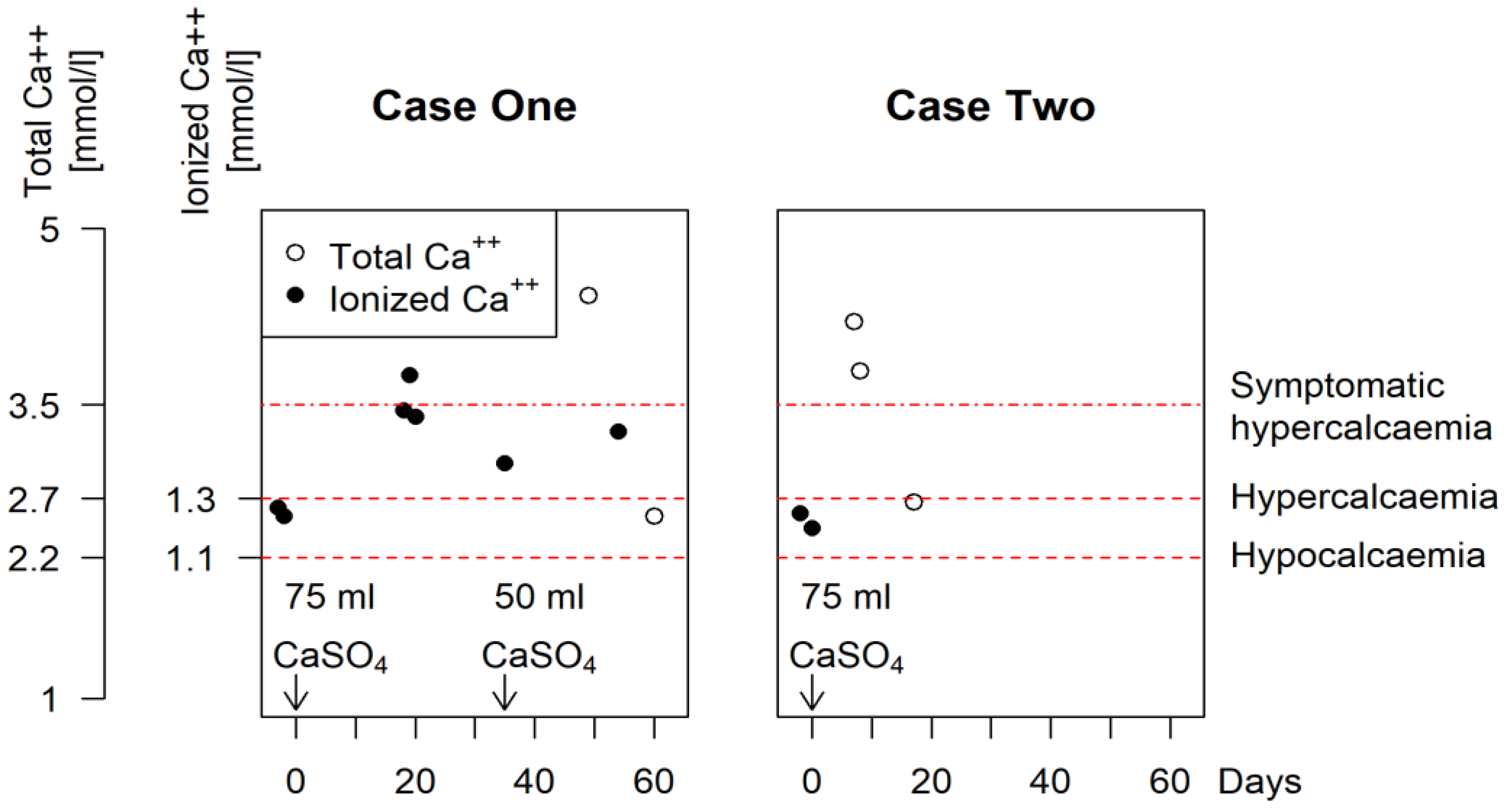
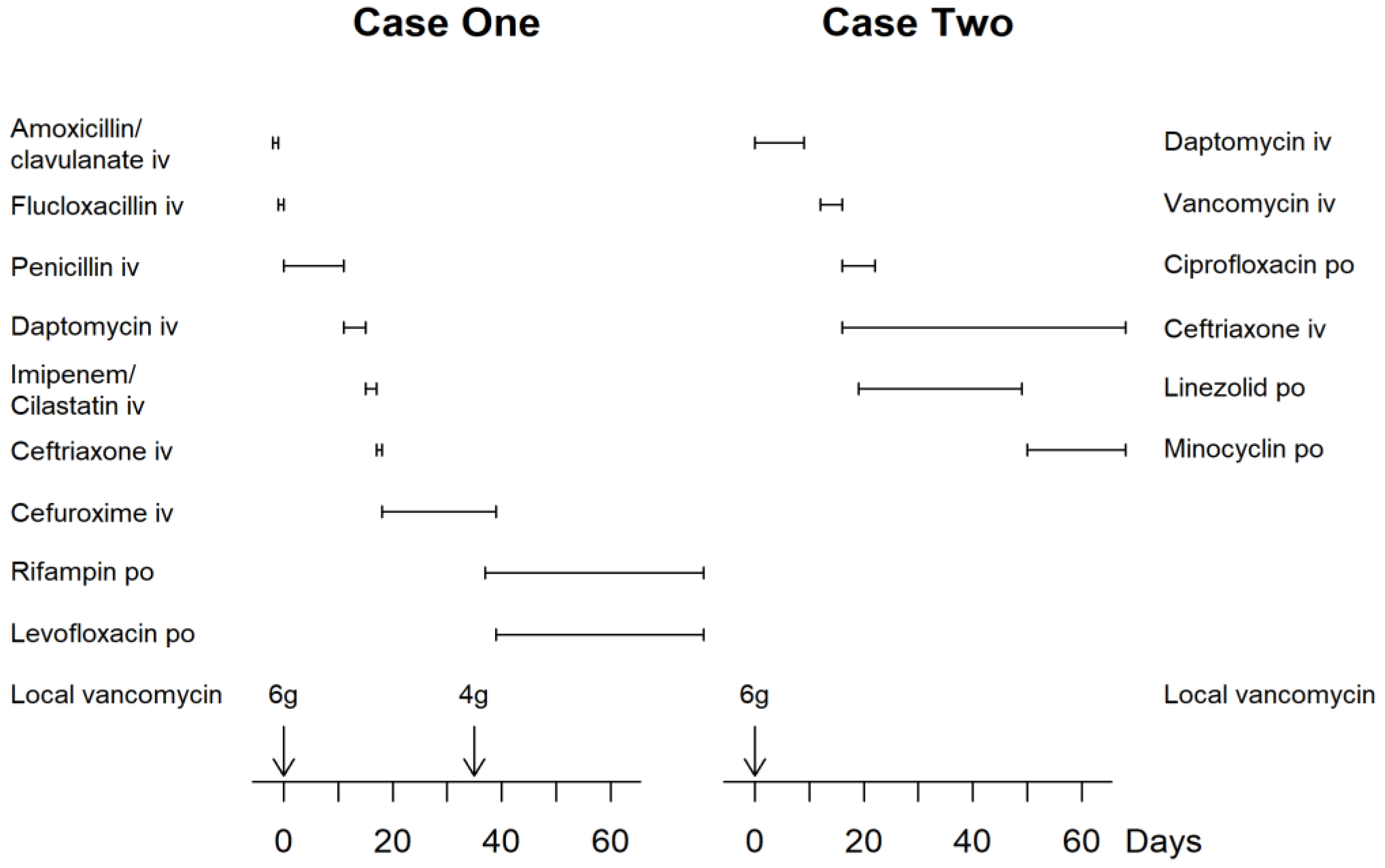
3.1. Case One
3.2. Case Two
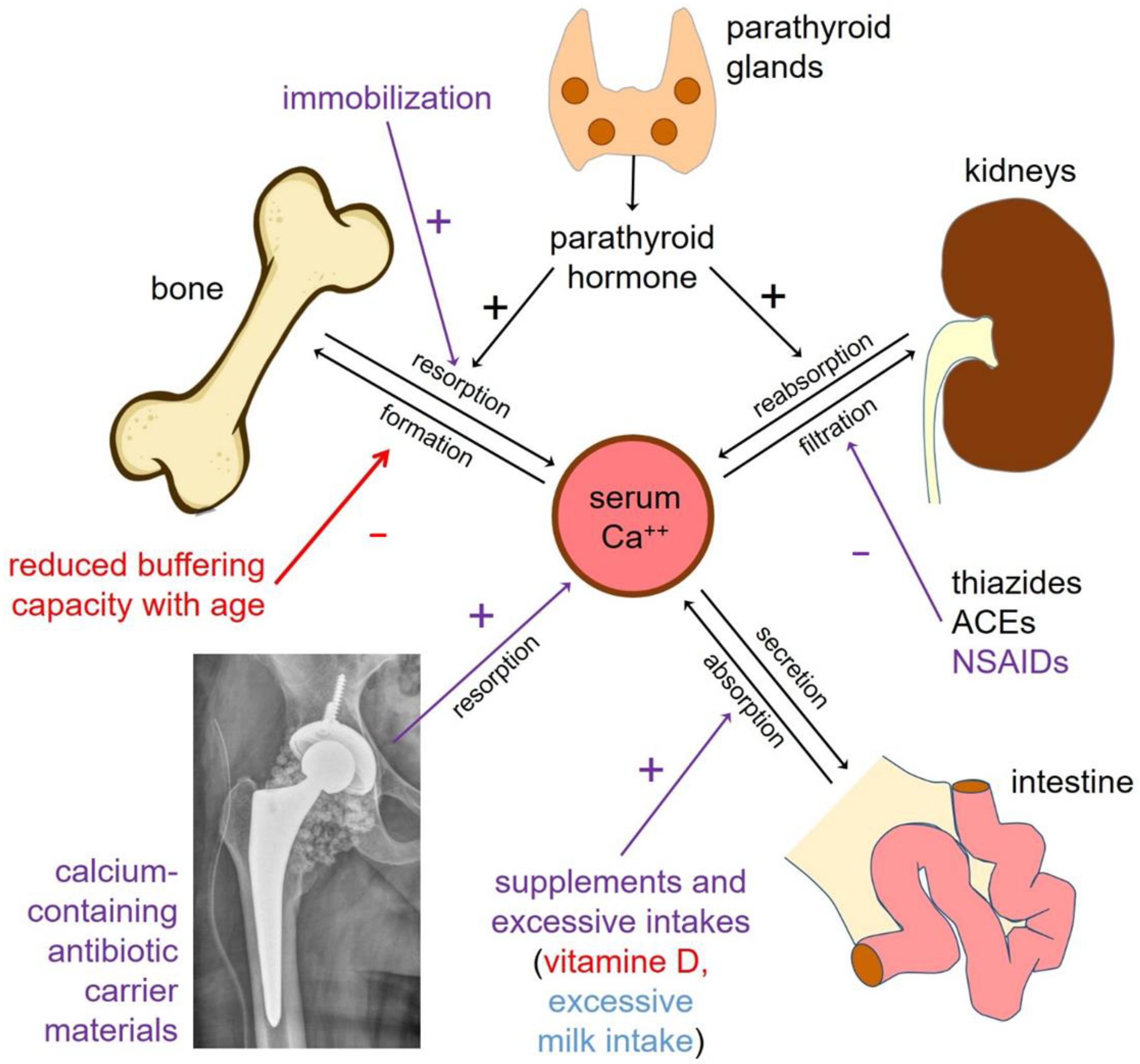
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ferguson, J.Y.; Dudareva, M.; Riley, N.D.; Stubbs, D.; Atkins, B.L.; McNally, M.A. The use of a biodegradable antibiotic-loaded calcium sulphate carrier containing tobramycin for the treatment of chronic osteomyelitis: A series of 195 cases. Bone Jt. J. 2014, 96, 829–836. [Google Scholar] [CrossRef] [PubMed]
- McKee, M.D.; Li-Bland, E.A.; Wild, L.M.; Schemitsch, E.H. A prospective, randomized clinical trial comparing an antibiotic-impregnated bioabsorbable bone substitute with standard antibiotic-impregnated cement beads in the treatment of chronic osteomyelitis and infected nonunion. J. Orthop. Trauma 2010, 24, 483–490. [Google Scholar] [CrossRef] [PubMed]
- McPherson, M.D.F.E.; Dipane, B.A.M.; Sherif, M.D.S. Dissolvable Antibiotic Beads in Treatment of Periprosthetic Joint Infection and Revision Arthroplasty—The Use of Synthetic Pure Calcium Sulfate (Stimulan®) Impregnated with Vancomycin&Tobramycin. Reconstr. Rev. 2013, 3. [Google Scholar] [CrossRef] [Green Version]
- Flierl, M.A.; Culp, B.M.; Okroj, K.T.; Springer, B.D.; Levine, B.R.; Della Valle, C.J. Poor Outcomes of Irrigation and Debridement in Acute Periprosthetic Joint Infection with Antibiotic-Impregnated Calcium Sulfate Beads. J. Arthroplast. 2017, 32, 2505–2507. [Google Scholar] [CrossRef] [PubMed]
- Wahl, P.; Guidi, M.; Benninger, E.; Rönn, K.; Gautier, E.; Buclin, T.; Magnin, J.-L.; Livio, F. The levels of vancomycin in the blood and the wound after the local treatment of bone and soft-tissue infection with antibiotic-loaded calcium sulphate as carrier material. Bone Jt. J. 2017, 99, 1537–1544. [Google Scholar] [CrossRef]
- Gramlich, Y.; Walter, G.; Klug, A.; Harbering, J.; Kemmerer, M.; Hoffmann, R. Procedure for single-stage implant retention for chronic periprosthetic infection using topical degradable calcium-based antibiotics. Int. Orthop. 2019, 43, 1559–1566. [Google Scholar] [CrossRef]
- Healy, A.H.; Reid, B.B.; Allred, B.D.; Doty, J.R. Antibiotic-impregnated beads for the treatment of aortic graft infection. Ann. Thorac. Surg. 2012, 93, 984–985. [Google Scholar] [CrossRef]
- Anagnostakos, K.; Wilmes, P.; Schmitt, E.; Kelm, J. Elution of gentamicin and vancomycin from polymethylmethacrylate beads and hip spacers in vivo. Acta Orthop. 2009, 80, 193–197. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, P.H.; Chang, Y.H.; Chen, S.H.; Ueng, S.W.; Shih, C.H. High concentration and bioactivity of vancomycin and aztreonam eluted from Simplex cement spacers in two-stage revision of infected hip implants: A study of 46 patients at an average follow-up of 107 days. J. Orthop. Res. 2006, 24, 1615–1621. [Google Scholar] [CrossRef]
- Perry, A.C.; Rouse, M.S.; Khaliq, Y.; Piper, K.E.; Hanssen, A.D.; Osmon, D.R.; Steckelberg, J.M.; Patel, R. Antimicrobial release kinetics from polymethylmethacrylate in a novel continuous flow chamber. Clin. Orthop. Relat. Res. 2002, 403, 49–53. [Google Scholar] [CrossRef]
- Post, V.; Wahl, P.; Richards, R.G.; Moriarty, T.F. Vancomycin displays time-dependent eradication of mature Staphylococcus aureus biofilms. J. Orthop. Res. 2017, 35, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Peltier, L.F. The use of plaster of Paris to fill defects in bone. Ann. Surg. 1957, 146, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Turner, T.M.; Urban, R.M.; Hall, D.J.; Chye, P.C.; Segreti, J.; Gitelis, S. Local and systemic levels of tobramycin delivered from calcium sulfate bone graft substitute pellets. Clin. Orthop. Relat. Res. 2005, 437, 97–104. [Google Scholar] [CrossRef] [PubMed]
- MAUDE Adverse Event Report; Wright Medical Group-Calcium Osteoset Beads US Department of Health and Human Services FDA: Silver Spring, MD, USA, 2005.
- Carlson, C.R., Jr.; Markulis, E.; Thompson, E.; Havill, J. A novel case of hypercalcemia following the use of calcium sulfate beads. Nephrol. Open J. 2015, 1, 17–19. [Google Scholar] [CrossRef]
- Kallala, R.; Haddad, F.S. Hypercalcaemia following the use of antibiotic-eluting absorbable calcium sulphate beads in revision arthroplasty for infection. Bone Jt. J. 2015, 97, 1237–1241. [Google Scholar] [CrossRef]
- Forte, M.; Pellegrino, R. Severe Hypercalcemia Following the Implantation of Antibiotic Impregnated Calcium Sulfate Beads for Prosthetic Joint infection. West Va. Med. J. 2017, 2698. [Google Scholar] [CrossRef]
- Wahl, P.; Livio, F.; Jacobi, M.; Gautier, E.; Buclin, T. Systemic exposure to tobramycin after local antibiotic treatment with calcium sulphate as carrier material. Arch. Orthop. Trauma Surg. 2011, 131, 657–662. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Maier, J.D.; Levine, S.N. Hypercalcemia in the Intensive Care Unit: A Review of Pathophysiology, Diagnosis, and Modern Therapy. J. Intensive Care Med. 2015, 30, 235–252. [Google Scholar] [CrossRef]
- Thomas, M.V.; Puleo, D.A.; Al-Sabbagh, M. Calcium sulfate: A review. J. Long Term Eff. Med. Implant. 2005, 15, 599–607. [Google Scholar] [CrossRef]
- Matkovic, V. Calcium metabolism and calcium requirements during skeletal modeling and consolidation of bone mass. Am. J. Clin. Nutr. 1991, 54, 245–260. [Google Scholar] [CrossRef]
- Matkovic, V. Calcium intake and peak bone mass. N. Engl. J. Med. 1992, 327, 119–120. [Google Scholar] [CrossRef] [PubMed]
- Heaney, R.P.; Abrams, S.; Dawson-Hughes, B.; Looker, A.; Marcus, R.; Matkovic, V.; Weaver, C. Peak bone mass. Osteoporos. Int. 2000, 11, 985–1009. [Google Scholar] [CrossRef] [PubMed]
- Nordin, B.E.; Peacock, M. Role of kidney in regulation of plasma-calcium. Lancet 1969, 2, 1280–1283. [Google Scholar] [CrossRef]
- Bouillon, R.; Carmeliet, G.; Boonen, S. Ageing and calcium metabolism. Baillieres Clin. Endocrinol. Metab. 1997, 11, 341–365. [Google Scholar] [CrossRef]
- Felsenfeld, A.J.; Levine, B.S. Milk alkali syndrome and the dynamics of calcium homeostasis. Clin. J. Am. Soc. Nephrol. 2006, 1, 641–654. [Google Scholar] [CrossRef]
- Greger, R. New insights into the molecular mechanism of the action of diuretics. Nephrol. Dial. Transplant. 1999, 14, 536–540. [Google Scholar] [CrossRef] [Green Version]
- Sebastian, A. Thiazides and bone. Am. J. Med. 2000, 109, 429–430. [Google Scholar] [CrossRef]
- Valour, F.; Karsenty, J.; Bouaziz, A.; Ader, F.; Tod, M.; Lustig, S.; Laurent, F.; Ecochard, R.; Chidiac, C.; Ferry, T. Antimicrobial-related severe adverse events during treatment of bone and joint infection due to methicillin-susceptible Staphylococcus aureus. Antimicrob. Agents Chemother. 2014, 58, 746–755. [Google Scholar] [CrossRef] [Green Version]
- Schrank, G.M.; Wright, S.B.; Branch-Elliman, W.; LaSalvia, M.T. A retrospective analysis of adverse events among patients receiving daptomycin versus vancomycin during outpatient parenteral antimicrobial therapy. Infect. Control. Hosp. Epidemiol. 2018, 39, 947–954. [Google Scholar] [CrossRef]
- Hagiya, H.; Kokado, R.; Ueda, A.; Okuno, H.; Morii, D.; Hamaguchi, S.; Yamamoto, N.; Yoshida, H.; Tomono, K. Association of Adverse Drug Events with Broad-spectrum Antibiotic Use in Hospitalized Patients: A Single-center Study. Intern. Med. 2019, 58, 2621–2625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowler, V.G., Jr.; Boucher, H.W.; Corey, G.R.; Abrutyn, E.; Karchmer, A.W.; Rupp, M.E.; Levine, D.P.; Chambers, H.F.; Tally, F.P.; Vigliani, G.A.; et al. Daptomycin versus standard therapy for bacteremia and endocarditis caused by Staphylococcus aureus. N. Engl. J. Med. 2006, 355, 653–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrestha, N.K.; Mason, P.; Gordon, S.M.; Neuner, E.; Nutter, B.; O’Rourke, C.; Rehm, S.J. Adverse events, healthcare interventions and healthcare utilization during home infusion therapy with daptomycin and vancomycin: A propensity score-matched cohort study. J. Antimicrob. Chemother. 2014, 69, 1407–1415. [Google Scholar] [CrossRef] [Green Version]
- Romanò, C.L.; Romanò, D.; Albisetti, A.; Meani, E. Preformed antibiotic-loaded cement spacers for two-stage revision of infected total hip arthroplasty. Long-term results. Hip Int. 2012, 22, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Khatod, M.; Cafri, G.; Inacio, M.C.; Schepps, A.L.; Paxton, E.W.; Bini, S.A. Revision total hip arthoplasty: Factors associated with re-revision surgery. J. Bone Jt. Surg. Am. 2015, 97, 359–366. [Google Scholar] [CrossRef]
- Badarudeen, S.; Shu, A.C.; Ong, K.L.; Baykal, D.; Lau, E.; Malkani, A.L. Complications After Revision Total Hip Arthroplasty in the Medicare Population. J. Arthroplast. 2017, 32, 1954–1958. [Google Scholar] [CrossRef]
- Koenig, K.; Huddleston, J.I., 3rd; Huddleston, H.; Maloney, W.J.; Goodman, S.B. Advanced age and comorbidity increase the risk for adverse events after revision total hip arthroplasty. J. Arthroplast. 2012, 27, 1402–1407. [Google Scholar] [CrossRef]
- Lora-Tamayo, J.; Senneville, É.; Ribera, A.; Bernard, L.; Dupon, M.; Zeller, V.; Li, H.K.; Arvieux, C.; Clauss, M.; Uçkay, I.; et al. The Not-So-Good Prognosis of Streptococcal Periprosthetic Joint Infection Managed by Implant Retention: The Results of a Large Multicenter Study. Clin. Infect. Dis. 2017, 64, 1742–1752. [Google Scholar] [CrossRef]
- Calvi, L.M.; Bushinsky, D.A. When is it appropriate to order an ionized calcium? J. Am. Soc. Nephrol. 2008, 19, 1257–1260. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Applications (n) | 215 | Case One | Case Two |
|---|---|---|---|
| Gender, n (%) | 138 (64) male; 77 (36) female | male | female |
| Age, median (range) | 69 years (5 to 90) | 68 years | 82 years |
| Site of infection, n (%) | Upper limb 11 (5) | Hip | Hip |
| Spine 2 (1) | |||
| Pelvis 9 (4) | |||
| Hip 124 (58) | |||
| Thigh 15 (7) | |||
| Knee 15 (7) | |||
| Lower leg 28 (13) | |||
| Foot and ankle 11 (5) | |||
| Type of infection, n (%) | PJI 1 127 (59) | Native joint septic arthritis | PJI |
| FRI 2 82 (38) | |||
| Native joint septic arthritis 2 (1) | |||
| Others 3 4 (2) | |||
| Renal function (eGFR), median (range) | 95 mL/min/1.7 m2 (9–272) | 50 | 68 |
| Quantities of CaSO4, median (range) | Ostoset 50 mL (5–250) | Osteoset 75 + 50 mL (staged procedure) | Osteoset 75 mL |
| Quantities of CaSO4 grouped, n (%) | ≤25 mL: 62 (29) | >75 mL | ≤75 mL |
| >25 to ≤50 mL: 71 (33) | |||
| >50 to ≤75 mL: 71 (33) | |||
| >75 mL: 11 (5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vallon, F.; Meier, C.; Gautier, E.; Wahl, P. The Incidence of Severe Hypercalcaemia-Induced Mental Status Changes in Patients Treated with Antibiotic-Loaded Calcium Sulphate Depot for Orthopaedic Infections. J. Clin. Med. 2022, 11, 4900. https://doi.org/10.3390/jcm11164900
Vallon F, Meier C, Gautier E, Wahl P. The Incidence of Severe Hypercalcaemia-Induced Mental Status Changes in Patients Treated with Antibiotic-Loaded Calcium Sulphate Depot for Orthopaedic Infections. Journal of Clinical Medicine. 2022; 11(16):4900. https://doi.org/10.3390/jcm11164900
Chicago/Turabian StyleVallon, Faustine, Christoph Meier, Emanuel Gautier, and Peter Wahl. 2022. "The Incidence of Severe Hypercalcaemia-Induced Mental Status Changes in Patients Treated with Antibiotic-Loaded Calcium Sulphate Depot for Orthopaedic Infections" Journal of Clinical Medicine 11, no. 16: 4900. https://doi.org/10.3390/jcm11164900