
High Serum IL-31 Concentration Is Associated with Itch among Renal Transplant Recipients

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Itch
2.3. IL-31 Concentration
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ständer, S.; Weisshaar, E.; Mettang, T.; Szepietowski, J.C.; Carstens, E.; Ikoma, A.; Bergasa, N.; Gieler, U.; Misery, L.; Wallengren, J.; et al. Clinical classification of itch: A position paper of the International Forum for the Study of Itch. Acta Derm. Venereol. 2007, 87, 291–294. [Google Scholar] [CrossRef] [Green Version]
- Matterne, U.; Apfelbacher, C.J.; Vogelgsang, L.; Loerbroks, A.; Weisshaar, E. Incidence and determinants of chronic pruritus: A population-based cohort study. Acta Derm. Venereol. 2013, 93, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Weisshaar, E.; Szepietowski, J.C.; Dalgard, F.J.; Garcovich, S.; Gieler, U.; Giménez-Arnau, A.M.; Lambert, J.; Leslie, T.; Mettang, T.; Misery, L.; et al. European S2k Guideline on Chronic Pruritus. Acta Derm. Venereol. 2019, 99, 469–506. [Google Scholar]
- Combs, S.A.; Teixeira, J.P.; Germain, M.J. Pruritus in Kidney Disease. Semin Nephrol. 2015, 35, 383–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimata, N.; Fuller, D.S.; Saito, A.; Akizawa, T.; Fukuhara, S.; Pisoni, R.L.; Robinson, B.M.; Akiba, T. Pruritus in hemodialysis patients: Results from the Japanese Dialysis Outcomes and Practice Patterns Study (JDOPPS). Hemodial Int. 2014, 18, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Pisoni, R.L.; Wikström, B.; Elder, S.J.; Akizawa, T.; Asano, Y.; Keen, M.L.; Saran, R.; Mendelssohn, D.C.; Young, E.W.; Port, F.K. Pruritus in haemodialysis patients: International results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol. Dial. Transplant. 2006, 21, 3495–3505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayani, K.; Weiss, M.; Weisshaar, E. Clinical Findings and Provision of Care in Haemodialysis Patients with Chronic Itch: New Results from the German Epidemiological Haemodialysis Itch Study. Acta Derm. Venereol. 2016, 96, 361–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krajewski, P.K.; Olczyk, P.; Krajewska, M.; Krajewski, W.; Szepietowski, J.C. Clinical Characteristics of Itch in Renal Transplant Recipients. Front. Med. 2020, 7, 615334. [Google Scholar] [CrossRef]
- Krajewski, P.K.; Tyczyńska, K.; Bardowska, K.; Olczyk, P.; Krajewska, M.; Szepietowski, J.C. Psychosocial Burden of Itch among Renal Transplant Recipients. Toxins 2022, 14, 320. [Google Scholar] [CrossRef]
- Wieczorek, A.; Krajewski, P.; Kozioł-Gałczyńska, M.; Szepietowski, J.C. Opioid receptors expression in the skin of haemodialysis patients suffering from uraemic pruritus. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 2368–2372. [Google Scholar] [CrossRef]
- Szepietowski, J.C.; Reich, A.; Schwartz, R.A. Uraemic xerosis. Nephrol. Dial. Transplant. 2004, 19, 2709–2712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weisshaar, E. Epidemiology of uraemic itch: New data. Eur. J. Pain. 2016, 20, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Kaysen, G.A. The microinflammatory state in uremia: Causes and potential consequences. J. Am. Soc. Nephrol. 2001, 12, 1549–1557. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, T.; Kursewicz, C.D.; Fayne, R.A.; Nanda, S.; Shah, S.M.; Nattkemper, L.; Yokozeki, H.; Yosipovitch, G. Pathophysiologic mechanisms of itch in bullous pemphigoid. J. Am. Acad. Dermatol. 2020, 83, 53–62. [Google Scholar] [CrossRef]
- Hashimoto, T.; Kursewicz, C.D.; Fayne, R.A.; Nanda, S.; Shah, S.M.; Nattkemper, L.; Yokozeki, H.; Yosipovitch, G. Mechanisms of Itch in Stasis Dermatitis: Significant Role of IL-31 from Macrophages. J. Investig. Dermatol. 2020, 140, 850–859.e3. [Google Scholar] [CrossRef]
- Hashimoto, T.; Nattkemper, L.A.; Kim, H.S.; Kursewicz, C.D.; Fowler, E.; Shah, S.M.; Nanda, S.; Fayne, R.A.; Paolini, J.F.; Romanelli, P.; et al. Itch intensity in prurigo nodularis is closely related to dermal interleukin-31, oncostatin M, IL-31 receptor alpha and oncostatin M receptor beta. Exp. Dermatol. 2021, 30, 804–810. [Google Scholar] [CrossRef]
- Kato, A.; Fujii, E.; Watanabe, T.; Takashima, Y.; Matsushita, H.; Furuhashi, T.; Morita, A. Distribution of IL-31 and its receptor expressing cells in skin of atopic dermatitis. J. Dermatol. Sci. 2014, 74, 229–235. [Google Scholar]
- Kim, H.J.; Zeidi, M.; Bonciani, D.; Pena, S.M.; Tiao, J.; Sahu, S.; Werth, V. Itch in dermatomyositis: The role of increased skin interleukin-31. Br. J. Dermatol. 2018, 179, 669–678. [Google Scholar] [CrossRef]
- Kim, S.; Kim, H.J.; Yang, H.S.; Kim, E.; Huh, I.S.; Yang, J.M. IL-31 Serum Protein and Tissue mRNA Levels in Patients with Atopic Dermatitis. Ann. Dermatol. 2011, 23, 468–473. [Google Scholar] [CrossRef] [Green Version]
- Raap, U.; Weißmantel, S.; Gehring, M.; Eisenberg, A.M.; Kapp, A.; Fölster-Holst, R. IL-31 significantly correlates with disease activity and Th2 cytokine levels in children with atopic dermatitis. Pediatr. Allergy Immunol. 2012, 23, 285–288. [Google Scholar] [CrossRef]
- Świerczyńska, K.; Krajewski, P.K.; Nowicka-Suszko, D.; Białynicki-Birula, R.; Krajewska, M.; Szepietowski, J.C. The Serum Level of IL-31 in Patients with Chronic Kidney Disease-Associated Pruritus: What Can We Expect? Toxins 2022, 14, 197. [Google Scholar] [CrossRef] [PubMed]
- Ständer, S.; Augustin, M.; Reich, A.; Blome, C.; Ebata, T.; Phan, N.Q.; Szepietowski, J. Pruritus assessment in clinical trials: Consensus recommendations from the International Forum for the Study of Itch (IFSI) Special Interest Group Scoring Itch in Clinical Trials. Acta Derm. Venereol. 2013, 93, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Reich, A.; Mędrek, K.; Szepietowski, J. Czteropunktowy kwestionariusz oceny świądu—walidacja kwestionariusza. Dermatol. Rev./Przegląd Dermatol. 2012, 99, 600–604. [Google Scholar]
- Datsi, A.; Steinhoff, M.; Ahmad, F.; Alam, M.; Buddenkotte, J. Interleukin-31: The “itchy” cytokine in inflammation and therapy. Allergy 2021, 76, 2982–2997. [Google Scholar] [CrossRef] [PubMed]
- Furue, M.; Furue, M. Interleukin-31 and Pruritic Skin. J. Clin. Med. 2021, 10, 1906. [Google Scholar] [PubMed]
- Dillon, S.R.; Sprecher, C.; Hammond, A.; Bilsborough, J.; Rosenfeld-Franklin, M.; Presnell, S.R.; Haugen, H.S.; Maurer, M.; Harder, B.; Johnston, J.; et al. Interleukin 31, a cytokine produced by activated T cells, induces dermatitis in mice. Nat. Immunol. 2004, 5, 752–760. [Google Scholar] [CrossRef] [PubMed]
- Bodoor, K.; Al-Qarqaz, F.; Heis, L.A.; Alfaqih, M.A.; Oweis, A.O.; Almomani, R.; Obeidat, M.A. IL-33/13 Axis and IL-4/31 Axis Play Distinct Roles in Inflammatory Process and Itch in Psoriasis and Atopic Dermatitis. Clin. Cosmet Investig. Dermatol. 2020, 13, 419–424. [Google Scholar] [CrossRef]
- Kabashima, K.; Irie, H. Interleukin-31 as a Clinical Target for Pruritus Treatment. Front. Med. 2021, 8, 638325. [Google Scholar] [CrossRef]
- Nobbe, S.; Dziunycz, P.; Mühleisen, B.; Bilsborough, J.; Dillon, S.R.; French, L.E.; Hofbauer, G.F.L. IL-31 expression by inflammatory cells is preferentially elevated in atopic dermatitis. Acta Derm. Venereol. 2012, 92, 24–28. [Google Scholar]
- Saleem, M.D.; Oussedik, E.; D’Amber, V.; Feldman, S.R. Interleukin-31 pathway and its role in atopic dermatitis: A systematic review. J. Dermatol. Treat. 2017, 28, 591–599. [Google Scholar] [CrossRef]
- Feld, M.; Garcia, R.; Buddenkotte, J.; Katayama, S.; Lewis, K.; Muirhead, G.; Hevezi, P.; Plesser, K.; Schrumpf, H.; Krjutskov, K.; et al. The pruritus- and TH2-associated cytokine IL-31 promotes growth of sensory nerves. J. Allergy Clin. Immunol. 2016, 138, 500–508.e24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, B.; Jegga, A.G.; Shanmukhappa, K.S.; Edukulla, R.; Khurana Hershey, G.H.; Medvedovic, M.; Dillon, S.R.; Madala, S.K. IL-31-Driven Skin Remodeling Involves Epidermal Cell Proliferation and Thickening That Lead to Impaired Skin-Barrier Function. PLoS ONE 2016, 11, e0161877. [Google Scholar]
- Grimstad, O.; Sawanobori, Y.; Vestergaard, C.; Bilsborough, J.; Olsen, U.B.; Grønhøj-Larsen, C.; Matsushima, K. Anti-interleukin-31-antibodies ameliorate scratching behaviour in NC/Nga mice: A model of atopic dermatitis. Exp. Dermatol. 2009, 18, 35–43. [Google Scholar] [PubMed]
- Ezzat, M.H.; Hasan, Z.E.; Shaheen, K.Y. Serum measurement of interleukin-31 (IL-31) in paediatric atopic dermatitis: Elevated levels correlate with severity scoring. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 334–339. [Google Scholar] [CrossRef]
- Siniewicz-Luzeńczyk, K.; Stańczyk-Przyłuska, A.; Zeman, K. Correlation between serum interleukin-31 level and the severity of disease in children with atopic dermatitis. Postepy Dermatol. Alergol. 2013, 30, 282–285. [Google Scholar] [CrossRef] [Green Version]
- Otsuka, A.; Honda, T.; Doi, H.; Miyachi, Y.; Kabashima, K. An H1-histamine receptor antagonist decreases serum interleukin-31 levels in patients with atopic dermatitis. Br. J. Dermatol. 2011, 164, 455–456. [Google Scholar] [CrossRef]
- Szegedi, K.; Kremer, A.E.; Kezic, S.; Teunissen, M.B.; Bos, J.D.; Luiten, R.M.; Res, P.C.; Middelkamp-Hup, M.A. Increased frequencies of IL-31-producing T cells are found in chronic atopic dermatitis skin. Exp. Dermatol. 2012, 21, 431–436. [Google Scholar] [CrossRef] [Green Version]
- Neis, M.M.; Peters, B.; Dreuw, A.; Wenzel, J.; Bieber, T.; Mauch, C.; Krieg, T.; Stanzel, S.; Heinrich, P.C.; Merk, H.F. Enhanced expression levels of IL-31 correlate with IL-4 and IL-13 in atopic and allergic contact dermatitis. J. Allergy Clin. Immunol. 2006, 118, 930–937. [Google Scholar] [CrossRef]
- Raap, U.; Gehring, M.; Kleiner, S.; Rüdrich, U.; Eiz-Vesper, B.; Haas, H.; Kapp, A.; Gibbs, B.F. Human basophils are a source of—And are differentially activated by—IL-31. Clin. Exp. Allergy 2017, 47, 499–508. [Google Scholar] [CrossRef]
- Ko, M.J.; Peng, Y.S.; Chen, H.Y.; Hsu, S.P.; Pai, M.F.; Yang, J.Y.; Wen, S.-Y.; Jee, S.-H.; Wu, H.-Y.; Chiu, H.-C. Interleukin-31 is associated with uremic pruritus in patients receiving hemodialysis. J. Am. Acad. Dermatol. 2014, 71, 1151–1159.e1. [Google Scholar] [CrossRef]
- Haggag, M.; Kora, M.; Safan, M.; Yasien, H.; Yousef, A. Study of serum level of interleukin-31 in patients with uremic pruritus. Menoufia Med. J. 2020, 33, 257. [Google Scholar]
- Oweis, A.O.; Al-Qarqaz, F.; Bodoor, K.; Heis, L.; Alfaqih, M.A.; Almomani, R.; Obeidat, M.A.; Alshelleh, S.A. Elevated interleukin 31 serum levels in hemodialysis patients are associated with uremic pruritus. Cytokine 2021, 138, 155369. [Google Scholar] [CrossRef] [PubMed]
- Güvercin, B.; Kaynar, K.; Arıca, D.A.; Kural, B.V.; Ulusoy, Ş.; Cansız, M.; Selçuk, L.B.; Akyüz, A.; Kolaylı, C.C. The relationship between dermatological findings and serum interleukin 31 and serum uridine diphosphate glucose ceramide glucosyltransferase levels among patients with chronic kidney disease. Hippokratia 2019, 23, 75–80. [Google Scholar]
- Kimmel, M.; Alscher, D.M.; Dunst, R.; Braun, N.; Machleidt, C.; Kiefer, T.; Stülten, C.; Van Der Kuip, H.; Pauli-Magnus, C.; Raub, U.; et al. The role of micro-inflammation in the pathogenesis of uraemic pruritus in haemodialysis patients. Nephrol. Dial. Transplant. 2006, 21, 749–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fallahzadeh, M.K.; Roozbeh, J.; Geramizadeh, B.; Namazi, M.R. Interleukin-2 serum levels are elevated in patients with uremic pruritus: A novel finding with practical implications. Nephrol. Dial. Transplant. 2011, 26, 3338–3344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virga, G.; Visentin, I.; La Milia, V.; Bonadonna, A. Inflammation and pruritus in haemodialysis patients. Nephrol. Dial. Transplant. 2002, 17, 2164–2169. [Google Scholar] [CrossRef] [Green Version]
- Reszke, R.; Szepietowski, J.C. End-Stage Renal Disease Chronic Itch and Its Management. Dermatol. Clin. 2018, 36, 277–292. [Google Scholar] [CrossRef]
- Zachariae, R.; Lei, U.; Haedersdal, M.; Zachariae, C. Itch severity and quality of life in patients with pruritus: Preliminary validity of a Danish adaptation of the itch severity scale. Acta Derm. Venereol. 2012, 92, 508–514. [Google Scholar] [CrossRef] [Green Version]
- Suseł, J.; Batycka-Baran, A.; Reich, A.; Szepietowski, J.C. Uraemic pruritus markedly affects the quality of life and depressive symptoms in haemodialysis patients with end-stage renal disease. Acta Derm. Venereol. 2014, 94, 276–281. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, M.K.; Elshahid, A.R.; El Baz, T.Z.; Elazab, R.M.; Elhoseiny, S.A.; Elsaie, M.L. Impact of Uraemic Pruritus on Quality of Life among End Stage Renal Disease Patients on Dialysis. J. Clin. Diagn. Res. 2016, 10, Wc01-5. [Google Scholar] [CrossRef]
- Szepietowski, J.C.; Balaskas, E.; Taube, K.M.; Taberly, A.; Dupuy, P. Quality of life in patients with uraemic xerosis and pruritus. Acta Derm. Venereol. 2011, 91, 313–317. [Google Scholar] [PubMed] [Green Version]
- Heisig, M.; Reich, A.; Szepietowski, J.C. Alexithymia in Uraemic Pruritus. Acta Derm Venereol. 2016, 96, 699–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruzicka, T.; Mihara, R. Anti-Interleukin-31 Receptor A Antibody for Atopic Dermatitis. N. Engl. J. Med. 2017, 376, 2093. [Google Scholar] [CrossRef] [PubMed]
- Ständer, S.; Yosipovitch, G.; Legat, F.J.; Lacour, J.P.; Paul, C.; Narbutt, J.; Bieber, T.; Misery, L.; Wollenberg, A.; Reich, A.; et al. Trial of Nemolizumab in Moderate-to-Severe Prurigo Nodularis. N. Engl. J. Med. 2020, 382, 706–716. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.; Hu, F.; Dan, M.; Sang, Y.; Abulikemu, K.; Wang, Q.; Hong, Y.; Kang, X. Safety and Efficacy of Nemolizumab for Atopic Dermatitis With Pruritus: A Systematic Review and Meta-Regression Analysis of Randomized Controlled Trials. Front. Immunol. 2022, 13, 825312. [Google Scholar] [CrossRef]
- Kabashima, K.; Matsumura, T.; Komazaki, H.; Kawashima, M. Nemolizumab plus topical agents in patients with atopic dermatitis (AD) and moderate-to-severe pruritus provide improvement in pruritus and signs of AD for up to 68 weeks: Results from two phase III, long-term studies. Br. J. Dermatol. 2022, 186, 642–651. [Google Scholar] [CrossRef]
- Kinugasa, E.; Igawa, K.; Shimada, H.; Kondo, M.; Funakoshi, S.; Imada, N.; Itami, N.; Fukazawa, N.; Takubo, R.; Kawata, Y.; et al. Anti-pruritic effect of nemolizumab in hemodialysis patients with uremic pruritus: A phase II, randomized, double-blind, placebo-controlled clinical study. Clin. Exp. Nephrol. 2021, 25, 875–884. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | No Itch in Last 3 Days (n = 75) | Itch in Last 3 Days (n = 54) | p |
|---|---|---|---|
| Sex, n (%) | NS | ||
| Male | 46 (61.3) | 28 (51.9) | |
| Female | 29 (38.7) | 26 (48.1) | |
| Age (years, mean ± SD) | 51.24 ± 14.58 | 53.07 ± 12.0 | NS |
| BMI (kg/m2, mean ± SD) | 25.7 ± 5.5 | 26.22 ± 5.06 | NS |
| Time of disease (years, mean ± SD) | 18.47 ± 11.51 | 21.84 ± 13.01 | NS |
| Time on dialysis (years, mean ± SD) | 2.13 ± 1.84 | 2.72 ± 2.11 | NS |
| Time after KTx (years, mean ± SD) | 7.1 ± 7.45 | 8.7 ± 6.54 | NS |
| Atopy, n (%) | 12 (16) | 9 (16.7) | NS |
| Atopy in family n (%) | 11 (14.7) | 11 (20.4) | NS |
| Itch on dialysis n (%) | 13 (17.3) | 33 (61.1) | <0.001 |
| Itch (points, mean ± SD) | NA | 4.98 ± 2.41 | NA |
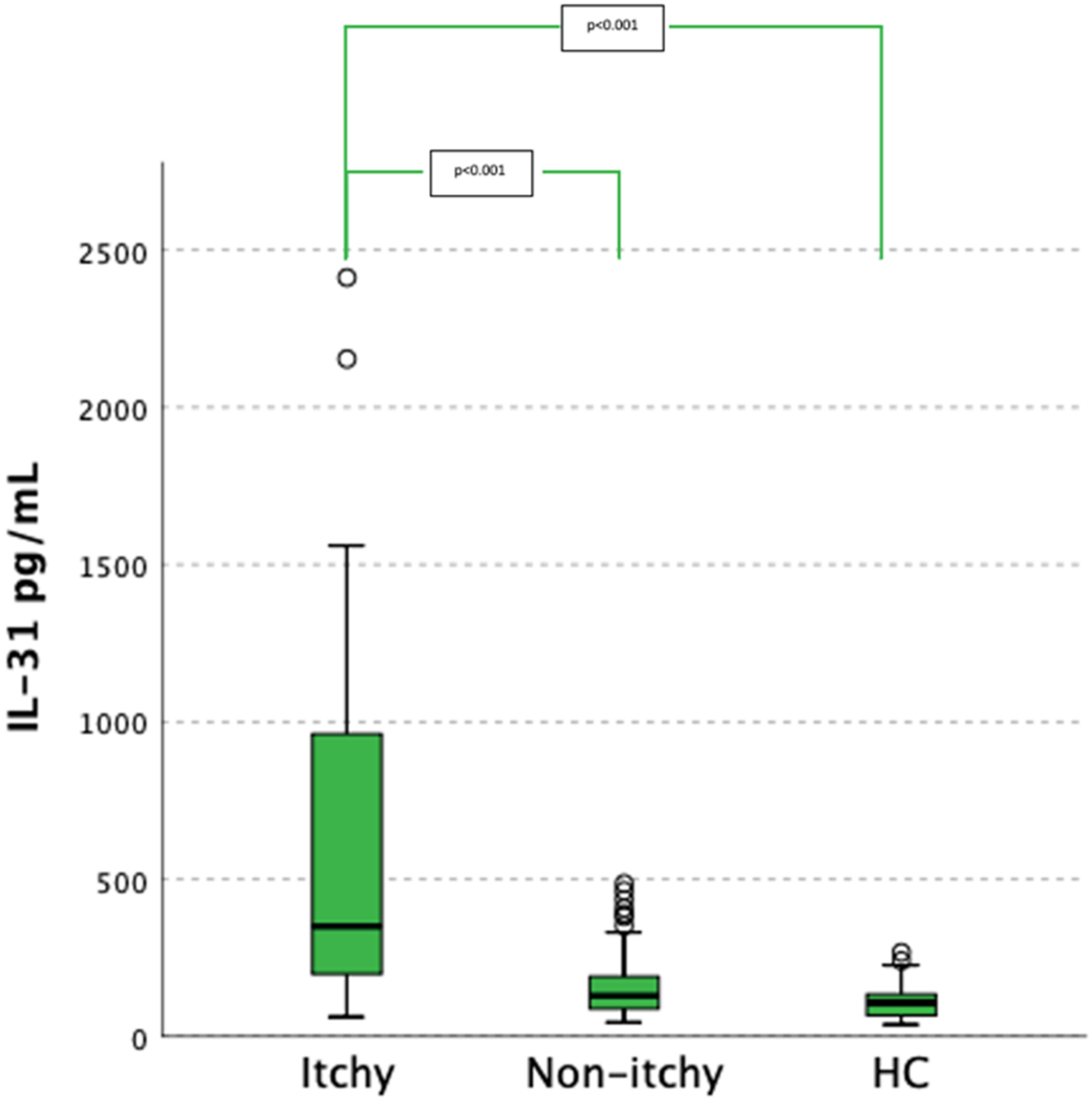
| Characteristics | No Itch in Last 3 Days (n = 75) | Itch in Last 3 Days (n = 54) | Healthy Controls | p | Post-Hoc |
|---|---|---|---|---|---|
| IL-31 level (pg, mean ± SD) | 161.49 ± 106.61 | 602.44 ± 534.5 | 110.33 ± 51.81 | <0.001 | Itch vs. no itch < 0.001 Itch vs. control < 0.001 No itch vs. control 0.058 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krajewski, P.K.; Tyczyńska, K.; Bardowska, K.; Olczyk, P.; Nowicka-Suszko, D.; Janczak, D.; Augustyniak-Bartosik, H.; Krajewska, M.; Szepietowski, J.C. High Serum IL-31 Concentration Is Associated with Itch among Renal Transplant Recipients. J. Clin. Med. 2022, 11, 4309. https://doi.org/10.3390/jcm11154309
Krajewski PK, Tyczyńska K, Bardowska K, Olczyk P, Nowicka-Suszko D, Janczak D, Augustyniak-Bartosik H, Krajewska M, Szepietowski JC. High Serum IL-31 Concentration Is Associated with Itch among Renal Transplant Recipients. Journal of Clinical Medicine. 2022; 11(15):4309. https://doi.org/10.3390/jcm11154309
Chicago/Turabian StyleKrajewski, Piotr K., Kinga Tyczyńska, Klaudia Bardowska, Piotr Olczyk, Danuta Nowicka-Suszko, Dariusz Janczak, Hanna Augustyniak-Bartosik, Magdalena Krajewska, and Jacek C. Szepietowski. 2022. "High Serum IL-31 Concentration Is Associated with Itch among Renal Transplant Recipients" Journal of Clinical Medicine 11, no. 15: 4309. https://doi.org/10.3390/jcm11154309