
Chronic Lung Allograft Dysfunction Is Associated with Increased Levels of Cell-Free Mitochondrial DNA in Bronchoalveolar Lavage Fluid of Lung Transplant Recipients

 , , , , , and
, , , , , and 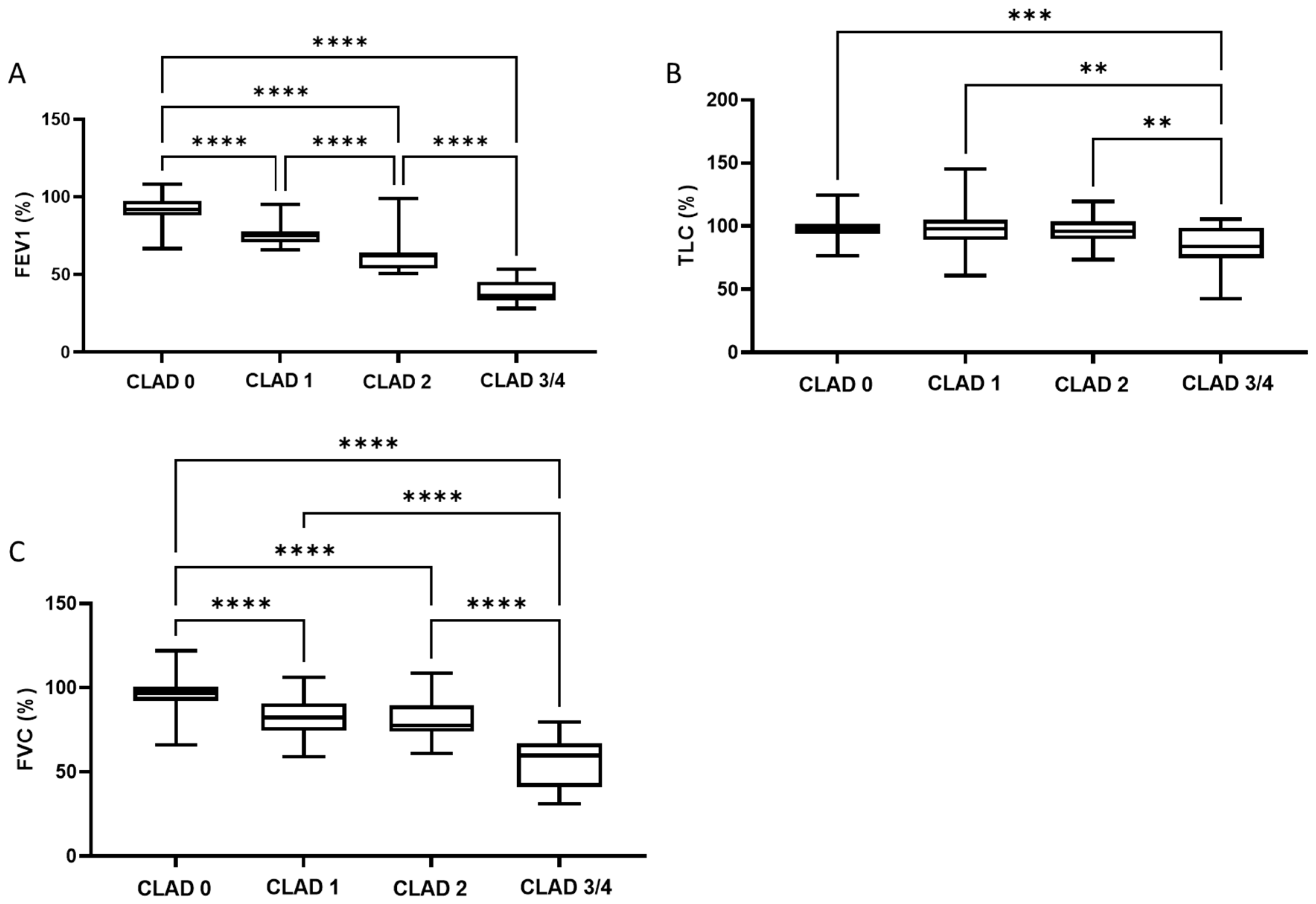{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Management of Lung Transplantation and Surveillance
2.3. Quantification of mtDNA
2.4. Clinical Data Recruitment and BAL Analyses
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
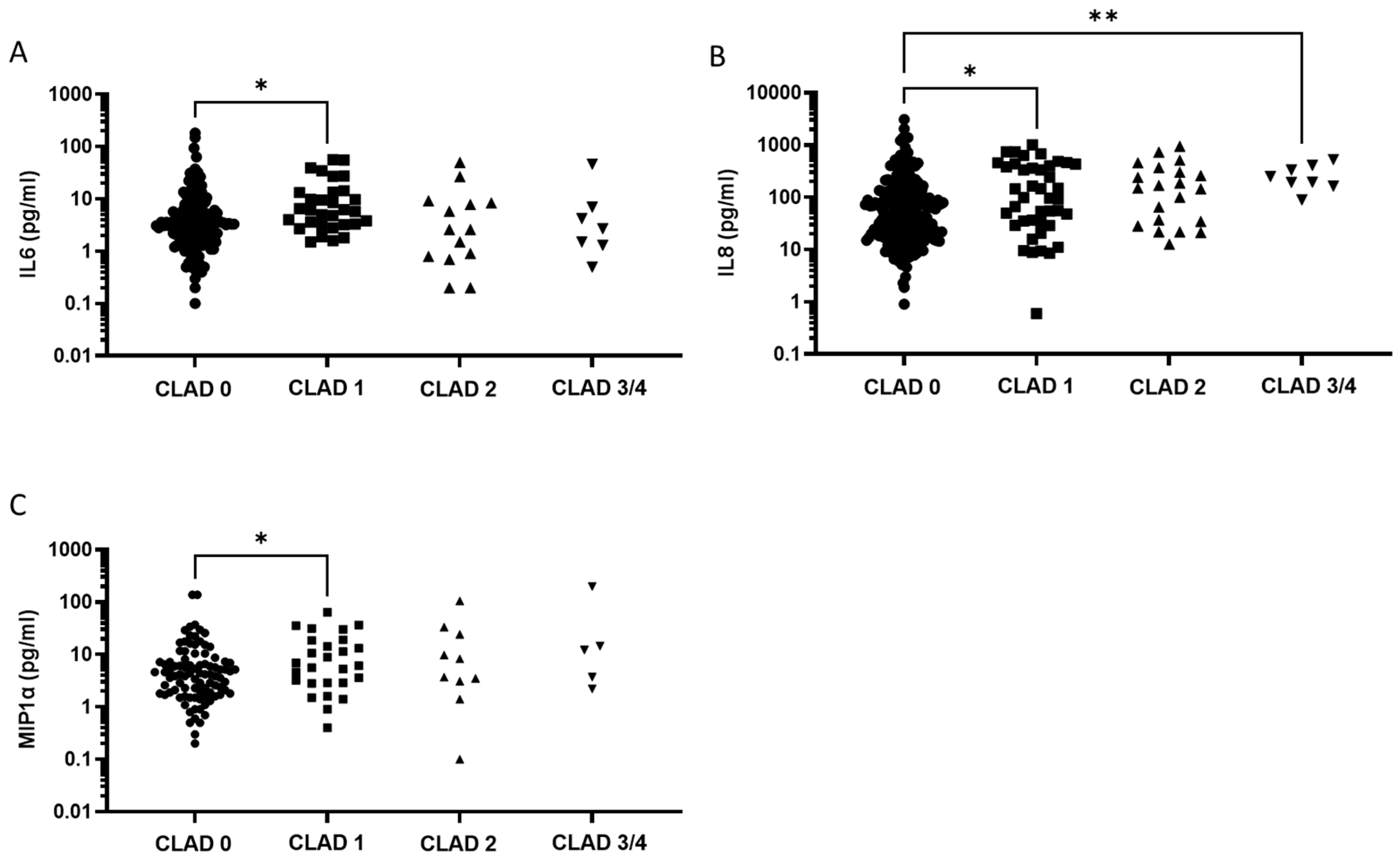
3.2. BAL Characteristics
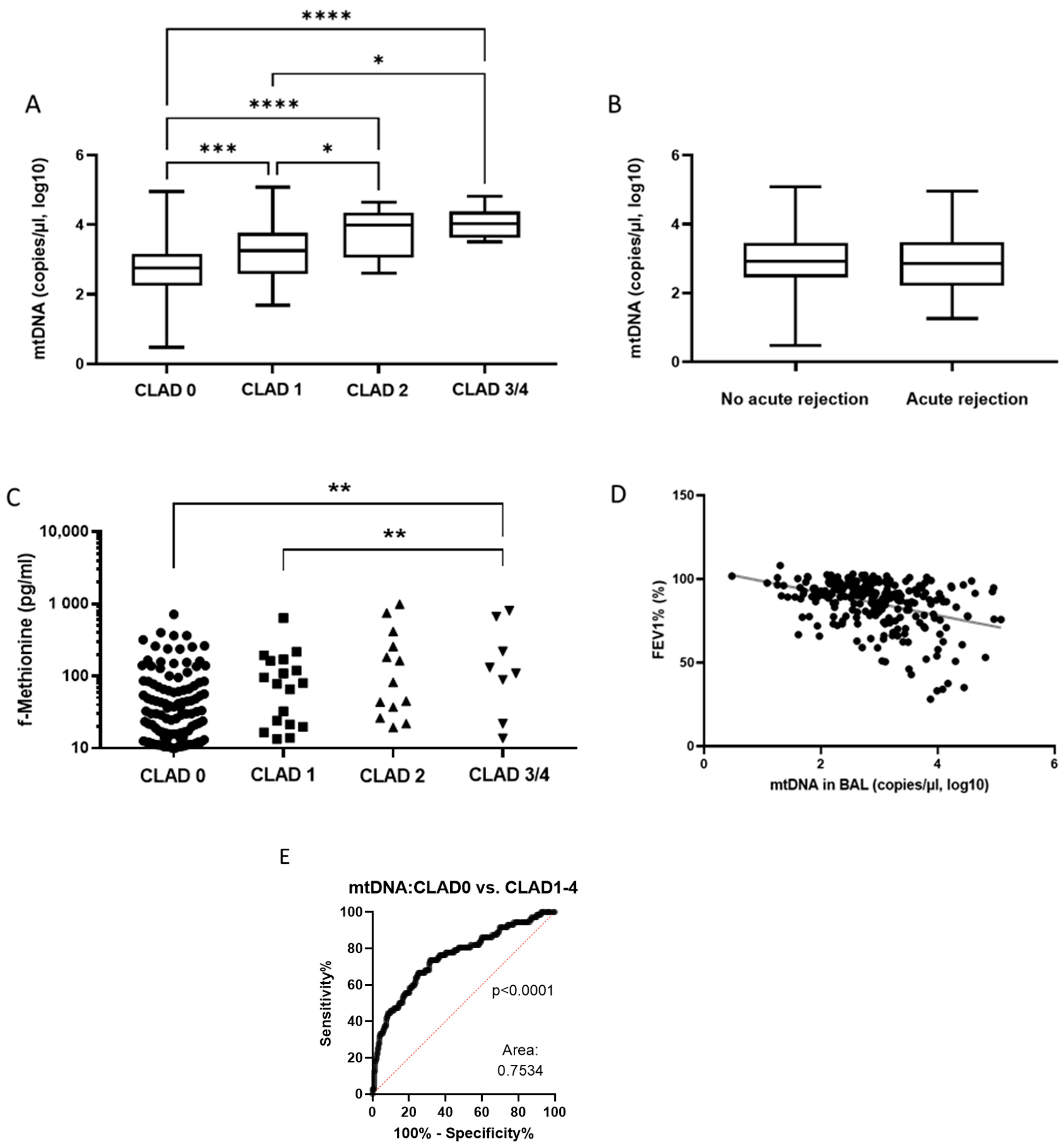
3.3. Mitochondrial Biomarkers in BAL Fluid
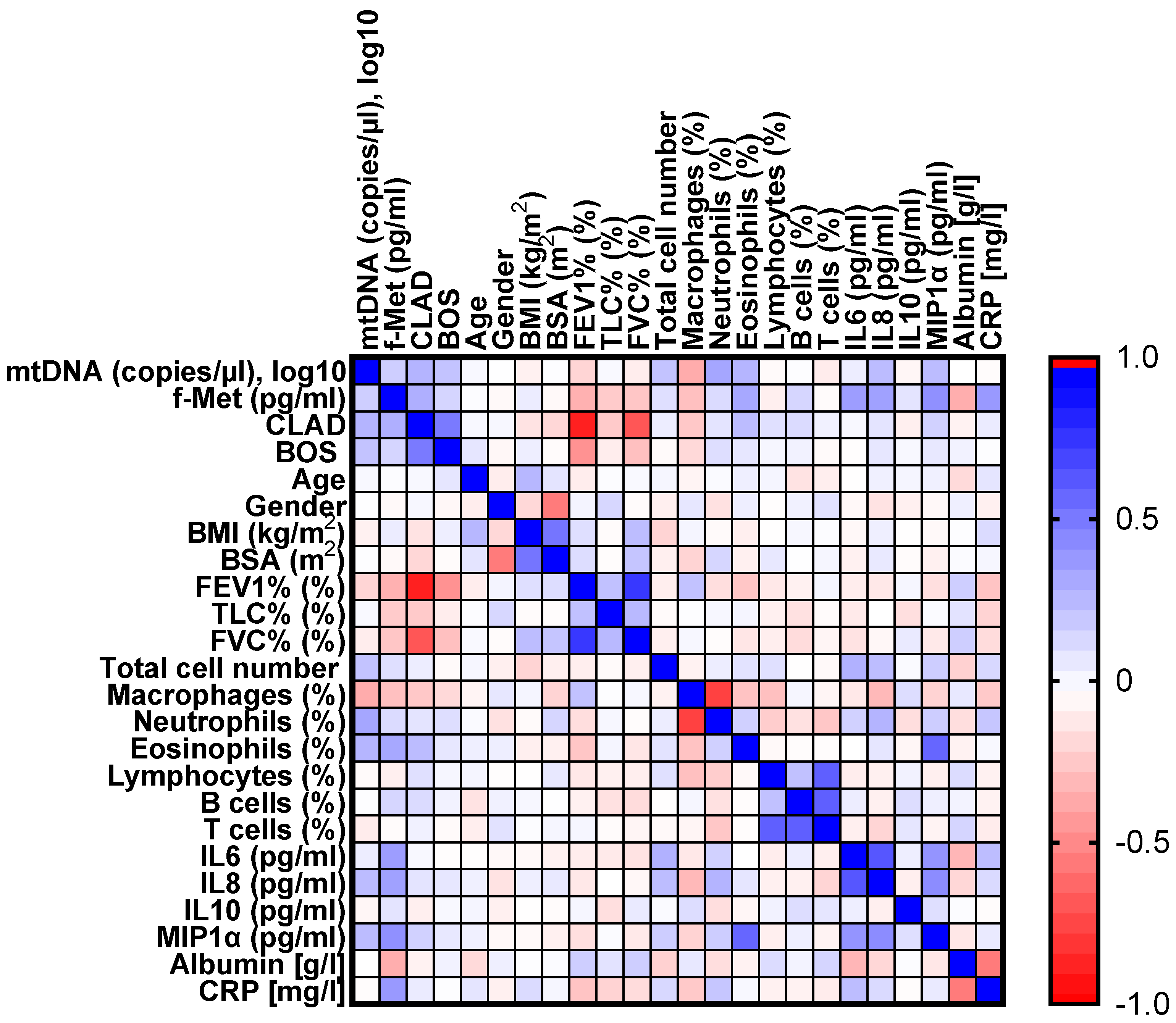
3.4. Correlation Matrix Analysis of Mitochondrial and Inflammatory Biomarkers
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hartert, M.; Senbaklavaci, Ö.; Gohrbandt, B.; Fischer, B.M.; Buhl, R.; Vahl, C.-F. Lung Transplantation. Dtsch Aerzteblatt Online 2014, 111, 107–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yusen, R.D.; Edwards, L.B.; Kucheryavaya, A.Y.; Benden, C.; Dipchand, A.I.; Dobbels, F.; Kirk, R.; Lund, L.H.; Rahmel, A.O.; Stehlik, J.; et al. The Registry of the International Society for Heart and Lung Transplantation: Thirty-first Adult Lung and Heart–Lung Transplant Report—2014; Focus Theme: Retransplantation. J. Heart Lung Transplant. 2014, 33, 1009–1024. [Google Scholar] [CrossRef] [PubMed]
- Hecker, M.; Hecker, A.; Kramm, T.; Askevold, I.; Kuhnert, S.; Reichert, M.; Mayer, E.; Seeger, W.; Padberg, W.; Mayer, K. Use of very old donors for lung transplantation: A dual-centre retrospective analysis. Eur. J. Cardio-Thoracic Surg. 2017, 52, 1049–1054. [Google Scholar] [CrossRef]
- Bos, S.; Vos, R.; Van Raemdonck, D.E.; Verleden, G.M. Survival in adult lung transplantation: Where are we in 2020? Curr. Opin. Organ Transplant. 2020, 25, 268–273. [Google Scholar] [CrossRef]
- Verleden, G.M.; Glanville, A.R.; Lease, E.D.; Fisher, A.J.; Calabrese, F.; Corris, P.A.; Ensor, C.R.; Gottlieb, J.; Hachem, R.R.; Lama, V.; et al. Chronic lung allograft dysfunction: Definition, diagnostic criteria, and approaches to treatment―A consensus report from the Pulmonary Council of the ISHLT. J. Heart Lung Transplant. 2019, 38, 493–503. [Google Scholar] [CrossRef] [Green Version]
- Sato, M.; Waddell, T.K.; Wagnetz, U.; Roberts, H.C.; Hwang, D.M.; Haroon, A.; Wagnetz, D.; Chaparro, C.; Singer, K.G.; Hutcheon, M.A.; et al. Restrictive allograft syndrome (RAS): A novel form of chronic lung allograft dysfunction. J. Heart Lung Transplant. 2011, 30, 735–742. [Google Scholar] [CrossRef]
- Vos, R.; Eynde, R.; Vanden Ruttens, D.; Verleden, S.E.; Vanaudenaerde, B.M.; Dupont, L.J.; Yserbyt, J.; Verbeken, E.K.; Neyrinck, A.P.; Van Raemdonck, D.E.; et al. Montelukast in chronic lung allograft dysfunction after lung transplantation. J. Heart Lung Transplant. 2019, 38, 516–527. [Google Scholar] [CrossRef] [Green Version]
- Ruttens, D.; Verleden, S.E.; Demeyer, H.; Van Raemdonck, D.E.; Yserbyt, J.; Dupont, L.J.; Vanaudenaerde, B.M.; Vos, R.; Verleden, G.M. Montelukast for bronchiolitis obliterans syndrome after lung transplantation: A randomized controlled trial. PLoS ONE 2018, 13, e0193564. [Google Scholar] [CrossRef] [Green Version]
- Patrucco, F.; Allara, E.; Boffini, M.; Rinaldi, M.; Costa, C.; Albera, C.; Solidoro, P. Twelve-month effects of everolimus on renal and lung function in lung transplantation: Differences in chronic lung allograft dysfunction phenotypes. Ther. Adv. Chronic. Dis. 2021, 12, 204062232199344. [Google Scholar] [CrossRef]
- Furuya, Y.; Witt, C.; Trulock, E.P.; Byers, D.; Kulkarni, H.; Tague, L.K.; Aguilar, P.; Kreisel, D.; Puri, V.; Gelman, A.; et al. Extracorporeal Photopheresis (ECP) in the Management of Chronic Lung Allograft Dysfunction. J. Heart Lung Transplant. 2019, 38, S165–S166. [Google Scholar] [CrossRef]
- Corris, P.A.; Ryan, V.A.; Small, T.; Lordan, J.; Fisher, A.J.; Meachery, G.; Johnson, G.; Ward, C. A randomised controlled trial of azithromycin therapy in bronchiolitis obliterans syndrome (BOS) post lung transplantation. Thorax 2015, 70, 442–450. [Google Scholar] [CrossRef] [Green Version]
- Tissot, A.; Danger, R.; Claustre, J.; Magnan, A.; Brouard, S. Early Identification of Chronic Lung Allograft Dysfunction: The Need of Biomarkers. Front. Immunol. 2019, 10, 1681. [Google Scholar] [CrossRef] [Green Version]
- Verhoeven, J.G.H.P.; Boer, K.; Van Schaik, R.H.N.; Manintveld, O.C.; Huibers, M.M.H.; Baan, C.C.; Hesselink, D.A. Liquid Biopsies to Monitor Solid Organ Transplant Function: A Review of New Biomarkers. Ther. Drug Monit. 2018, 40, 515–525. [Google Scholar] [CrossRef]
- Agbor-Enoh, S.; Wang, Y.; Tunc, I.; Jang, M.K.; Davis, A.; De Vlaminck, I.; Luikart, H.; Shah, P.D.; Timofte, I.; Brown, A.W.; et al. Donor-derived cell-free DNA predicts allograft failure and mortality after lung transplantation. eBioMedicine 2019, 40, 541–553. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Verleden, S.; Zarinsefat, A.; Vanaudenaerde, B.; Vos, R.; Verleden, G.; Sarwal, R.D.; Sigdel, T.K.; Liberto, J.M.; Damm, I.; et al. Cell-Free DNA and CXCL10 Derived from Bronchoalveolar Lavage Predict Lung Transplant Survival. J. Clin. Med. 2019, 8, 241. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.A.; Sammy, M.J.; Ballinger, S.W. An evolutionary, or “Mitocentric” perspective on cellular function and disease. Redox Biol. 2020, 36, 101568. [Google Scholar] [CrossRef]
- Jorch, S.K.; Kubes, P. An emerging role for neutrophil extracellular traps in noninfectious disease. Nat. Med. 2017, 23, 279–287. [Google Scholar] [CrossRef]
- Mallavia, B.; Liu, F.; Lefrançais, E.; Cleary, S.J.; Kwaan, N.; Tian, J.J.; Magnen, M.; Sayah, D.M.; Soong, A.; Chen, J.; et al. Mitochondrial DNA Stimulates TLR9-Dependent Neutrophil Extracellular Trap Formation in Primary Graft Dysfunction. Am. J. Respir. Cell Mol. Biol. 2020, 62, 364–372. [Google Scholar] [CrossRef]
- Hecker, M.; Hecker, A.; Askevold, I.; Kuhnert, S.; Reichert, M.; Guth, S.; Mayer, E.; Slania, H.; Schuettler, C.G.; Seeger, W.; et al. Indefinite cytomegalovirus prophylaxis with valganciclovir after lung transplantation. Transpl. Infect. Dis. 2019, 21, e13138. [Google Scholar] [CrossRef]
- Chiu, R.W.K.; Chan, L.Y.S.; Lam, N.Y.L.; Tsui, N.B.Y.; Ng, E.K.O.; Rainer, T.H.; Dennis Lo, Y.M. Quantitative analysis of circulating mitochondrial DNA in plasma. Clin. Chem. 2003, 49, 719–726. [Google Scholar] [CrossRef] [Green Version]
- Keller, M.; Bush, E.; Diamond, J.M.; Shah, P.; Matthew, J.; Brown, A.W.; Sun, J.; Timofte, I.; Kong, H.; Tunc, I.; et al. Use of donor-derived-cell-free DNA as a marker of early allograft injury in primary graft dysfunction (PGD) to predict the risk of chronic lung allograft dysfunction (CLAD). J. Heart Lung Transplant. 2021, 40, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Scozzi, D.; Ibrahim, M.; Liao, F.; Lin, X.; Hsiao, H.; Hachem, R.; Tague, L.K.; Ricci, A.; Kulkarni, H.S.; Huang, J.H.; et al. Mitochondrial damage–associated molecular patterns released by lung transplants are associated with primary graft dysfunction. Am. J. Transplant. 2019, 19, 1464–1477. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, N.; Agbor-Enoh, S. Cell-free DNA beyond a biomarker for rejection: Biological trigger of tissue injury and potential therapeutics. J. Heart Lung Transplant. 2021, 40, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Kanou, T.; Nakahira, K.; Choi, A.M.; Yeung, J.C.; Cypel, M.; Liu, M.; Keshavjee, S. Cell-free DNA in human ex vivo lung perfusate as a potential biomarker to predict the risk of primary graft dysfunction in lung transplantation. J. Thorac. Cardiovasc. Surg. 2021, 162, 490–499.e2. [Google Scholar] [CrossRef] [PubMed]
- Nykänen, A.; Raivio, P.; Peräkylä, L.; Stark, C.; Huuskonen, A.; Lemström, K.; Halme, M.; Hämmäinen, P. Incidence and impact of chronic lung allograft dysfunction after lung transplantation—single-center 14-year experience. Scand. Cardiovasc. J. 2020, 54, 192–199. [Google Scholar] [CrossRef]
- Royer, P.J.; Olivera-Botello, G.; Koutsokera, A.; Aubert, J.D.; Bernasconi, E.; Tissot, A.; Pison, C.; Nicod, L.; Boissel, J.P.; Magnan, A.; et al. Chronic lung allograft dysfunction: A systematic review of mechanisms. Transplantation 2016, 100, 1803–1814. [Google Scholar] [CrossRef] [Green Version]
- Sikkeland, L.I.B.; Durheim, M.T.; Riste, T.B.; Kongerud, J.; Alexis, N.E.; Holm, A.M. Relation of sputum neutrophilia to the development of chronic lung allograft dysfunction after lung transplantation. Clin. Transplant. 2021, 35, e14188. [Google Scholar] [CrossRef]
- DiGiovine, B.; Lynch, J.P.; Martinez, F.J.; Flint, A.; Whyte, R.I.; Iannettoni, M.D.; Arenberg, A.; Burdick, M.; Glass, M.C.; Wilke, C.A.; et al. Bronchoalveolar lavage neutrophilia is associated with obliterative bronchiolitis after lung transplantation: Role of IL-8. J. Immunol. 1996, 157, 4194–4202. [Google Scholar]
- Neurohr, C.; Huppmann, P.; Samweber, B.; Leuschner, S.; Zimmermann, G.; Leuchte, H.; Baumgartner, R.; Hatz, R.; Frey, L.; Ueberfuhr, P.; et al. Prognostic value of bronchoalveolar lavage neutrophilia in stable lung transplant recipients. J. Heart Lung Transplant. 2009, 28, 468–474. [Google Scholar] [CrossRef]
- Belperio, J.A.; Keane, M.P.; Burdick, M.D.; Gomperts, B.; Xue, Y.Y.; Hong, K.; Mestas, J.; Ardehali, A.; Mehrad, B.; Saggar, J.; et al. Role of CXCR2/CXCR2 ligands in vascular remodeling during bronchiolitis obliterans syndrome. J. Clin. Investig. 2005, 115, 1150–1162. [Google Scholar] [CrossRef] [Green Version]
- Reynaud-Gaubert, M.; Marin, V.; Thirion, X.; Farnarier, C.; Thomas, P.; Badier, M.; Bongrand, P.; Giudicelli, R.; Fuentes, P. Upregulation of chemokines in bronchoalveolar lavage fluid as a predictive marker of post-transplant airway obliteration. J. Heart Lung Transplant. 2002, 21, 721–730. [Google Scholar] [CrossRef]
- Amubieya, O.; Ramsey, A.; Derhovanessian, A.; Fishbein, G.A.; Lynch, J.P.; Belperio, J.A.; Weigt, S.S. Chronic Lung Allograft Dysfunction: Evolving Concepts and Therapies. Semin. Respir. Crit. Care Med. 2021, 42, 392–410. [Google Scholar] [CrossRef] [PubMed]
- Verleden, S.E.; Martens, A.; Ordies, S.; Neyrinck, A.P.; Van Raemdonck, D.E.; Verleden, G.M.; Vanaudenaerde, B.M.; Vos, R. Immediate post-operative broncho-alveolar lavage IL-6 and IL-8 are associated with early outcomes after lung transplantation. Clin. Transplant. 2018, 32, e13219. [Google Scholar] [CrossRef] [PubMed]
- Ruttens, D.; Verleden, S.E.; Vandermeulen, E.; Bellon, H.; Vanaudenaerde, B.M.; Somers, J.; Schoonis, A.; Schaevers, V.; Van Raemdonck, D.E.; Neyrinck, A.; et al. Prophylactic Azithromycin Therapy After Lung Transplantation: Post hoc Analysis of a Randomized Controlled Trial. Am. J. Transplant. 2016, 16, 254–261. [Google Scholar] [CrossRef]
- Verleden, G.M.; Vanaudenaerde, B.M.; Dupont, L.J.; Van Raemdonck, D.E. Azithromycin reduces airway neutrophilia and interleukin-8 in patients with bronchiolitis obliterans syndrome. Am. J. Respir. Crit. Care Med. 2006, 174, 566–570. [Google Scholar] [CrossRef]
- Herrera, S.; Gohir, W.; Foroutan, F.; Aguilar, C.; Juvet, S.; Martinu, T.; Kumar, D.; Humar, A.; Rotstein, C.; Keshavjee, S.; et al. Cytokine profile in lung transplant recipients with Aspergillus spp colonization. Transpl. Infect. Dis. 2019, 21, e13060. [Google Scholar] [CrossRef]
- Meloni, F.; Solari, N.; Miserere, S.; Morosini, M.; Cascina, A.; Klersy, C.; Arbustini, E.; Pellegrini, C.; Vigano, M.; Fietta, A.M. Chemokine redundancy in BOS pathogenesis. A possible role also for the CC chemokines: MIP3-beta, MIP3-alpha, MDC and their specific receptors. Transpl. Immunol. 2008, 18, 275–280. [Google Scholar] [CrossRef]
- Wenceslau, C.F.; Szasz, T.; McCarthy, C.G.; Baban, B.; NeSmith, E.; Webb, R.C. Mitochondrial N-formyl peptides cause airway contraction and lung neutrophil infiltration via formyl peptide receptor activation. Pulm. Pharmacol. Ther. 2016, 37, 49–56. [Google Scholar] [CrossRef]
- Wenceslau, C.F.; McCarthy, C.G.; Szasz, T.; Goulopoulou, S.; Webb, R.C. Mitochondrial N-formyl peptides induce cardiovascular collapse and sepsis-like syndrome. Am. J. Physiol. Heart Circ. Physiol. 2015, 308, H768–H777. [Google Scholar] [CrossRef] [Green Version]
- Supinski, G.S.; Schroder, E.A.; Callahan, L.A. Mitochondria and Critical Illness. Chest 2020, 157, 310–322. [Google Scholar] [CrossRef]
- Chawla, L.S.; Amdur, R.L.; Faselis, C.; Li, P.; Kimmel, P.L.; Palant, C.E. Impact of Acute Kidney Injury in Patients Hospitalized With Pneumonia. Crit. Care Med. 2017, 45, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Timmermans, K.; Kox, M.; Vaneker, M.; van den Berg, M.; John, A.; van Laarhoven, A.; Van der Hoeven, H.; Scheffer, G.J.; Pickers, P. Plasma levels of danger-associated molecular patterns are associated with immune suppression in trauma patients. Intensive Care Med. 2016, 42, 551–561. [Google Scholar] [CrossRef] [PubMed]
- Suwara, M.I.; Vanaudenaerde, B.M.; Verleden, S.E.; Vos, R.; Green, N.J.; Ward, C.; Borthwick, L.A.; Vandermeulen, E.; Jordan, J.; Van Raemdonck, D.E.; et al. Mechanistic differences between phenotypes of chronic lung allograft dysfunction after lung transplantation. Transpl. Int. 2014, 27, 857–867. [Google Scholar] [CrossRef] [Green Version]
- Devouassoux, G.; Drouet, C.; Pin, I.; Brambilla, C.; Brambilla, E.; Colle, P.-E.; Pison, C.; Grenoble Lung Transplant Group. Alveolar neutrophilia is a predictor for the bronchiolitis obliterans syndrome, and increases with degree of severity. Transpl. Immunol. 2002, 10, 303–310. [Google Scholar] [CrossRef]
- Palmer, S.M.; Burch, L.H.; Trindade, A.J.; Davis, R.D.; Herczyk, W.F.; Reinsmoen, N.L.; Schwartz, D.A. Innate immunity influences long-term outcomes after human lung transplant. Am. J. Respir. Crit. Care Med. 2005, 171, 780–785. [Google Scholar] [CrossRef]
- Kastelijn, E.A.; van Moorsel, C.H.M.; Rijkers, G.T.; Ruven, H.J.T.; Karthaus, V.; Kwakkel-van Erp, J.M.; Van de Graaf, E.A.; Zanen, P.; Van Kessel, D.A.; Grutters, J.C.; et al. Polymorphisms in innate immunity genes associated with development of bronchiolitis obliterans after lung transplantation. J. Heart Lung Transplant. 2010, 29, 665–671. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schneck, E.; Askevold, I.; Rath, R.; Hecker, A.; Reichert, M.; Guth, S.; Koch, C.; Sander, M.; Seeger, W.; Mayer, K.; et al. Chronic Lung Allograft Dysfunction Is Associated with Increased Levels of Cell-Free Mitochondrial DNA in Bronchoalveolar Lavage Fluid of Lung Transplant Recipients. J. Clin. Med. 2022, 11, 4142. https://doi.org/10.3390/jcm11144142
Schneck E, Askevold I, Rath R, Hecker A, Reichert M, Guth S, Koch C, Sander M, Seeger W, Mayer K, et al. Chronic Lung Allograft Dysfunction Is Associated with Increased Levels of Cell-Free Mitochondrial DNA in Bronchoalveolar Lavage Fluid of Lung Transplant Recipients. Journal of Clinical Medicine. 2022; 11(14):4142. https://doi.org/10.3390/jcm11144142
Chicago/Turabian StyleSchneck, Emmanuel, Ingolf Askevold, Ramona Rath, Andreas Hecker, Martin Reichert, Stefan Guth, Christian Koch, Michael Sander, Werner Seeger, Konstantin Mayer, and et al. 2022. "Chronic Lung Allograft Dysfunction Is Associated with Increased Levels of Cell-Free Mitochondrial DNA in Bronchoalveolar Lavage Fluid of Lung Transplant Recipients" Journal of Clinical Medicine 11, no. 14: 4142. https://doi.org/10.3390/jcm11144142