
Impact of KRAS Mutation Subtypes and Co-Occurring Mutations on Response and Outcome in Advanced NSCLC Patients following First-Line Treatment



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Objectives
2.2. Patients
2.3. Study Design and Assessments
2.4. End Points and Assessments
2.5. Capture-Based Targeted DNA Sequencing
2.6. Sequence-Data Analysis
2.7. Statistical Analysis
3. Results
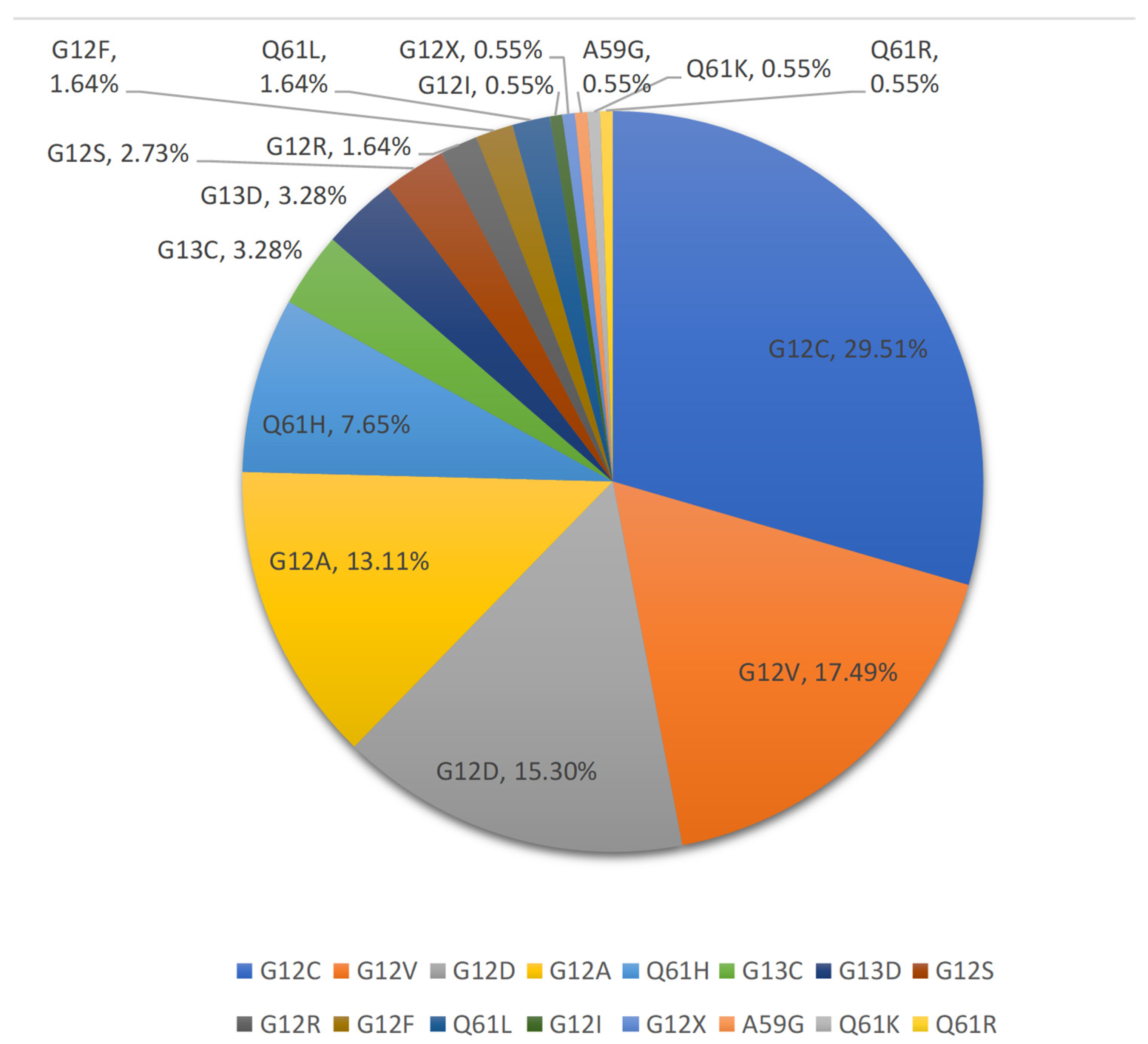
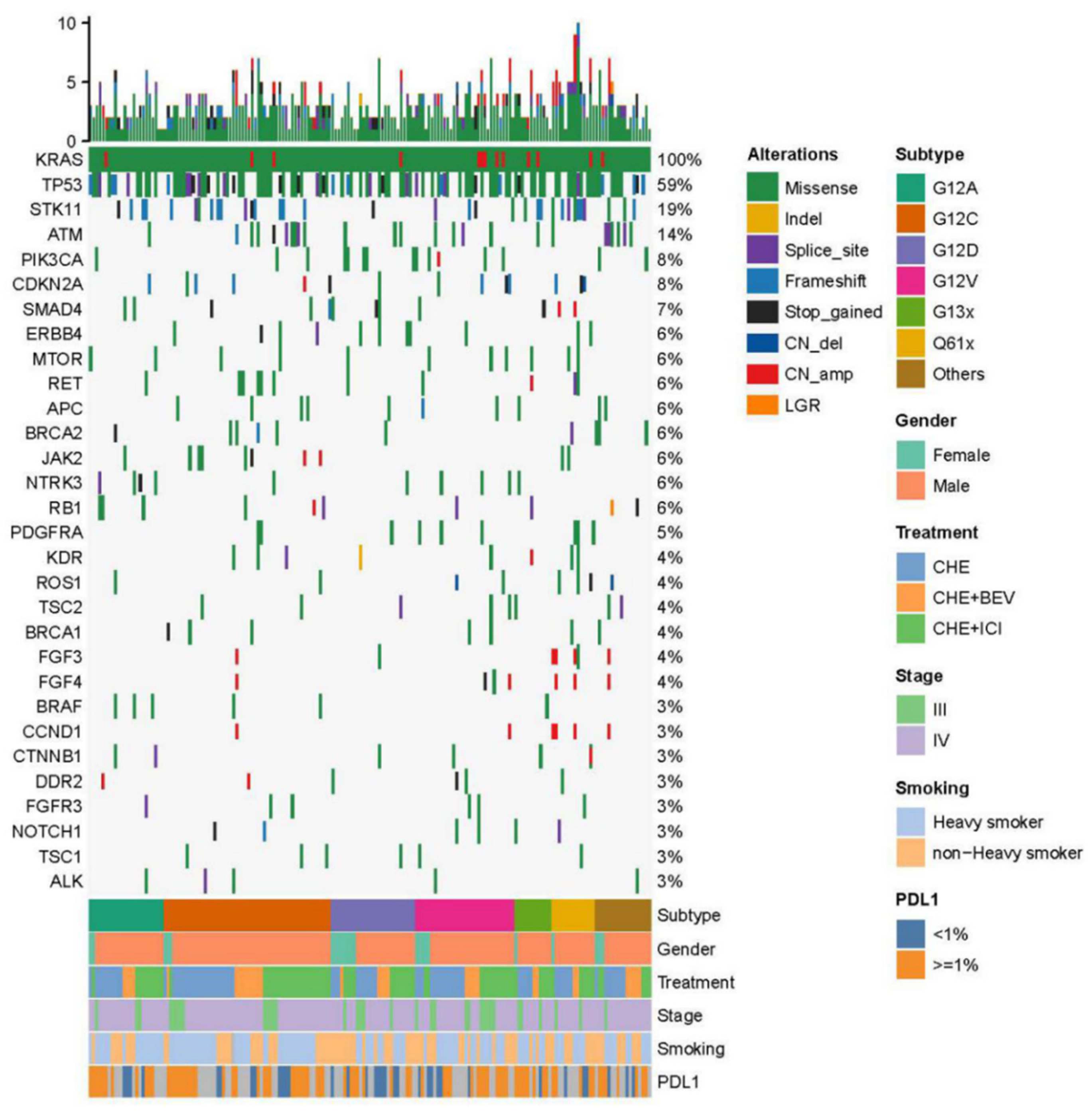
3.1. Clinical Characteristics and Genotype Subsection
3.2. Efficacy
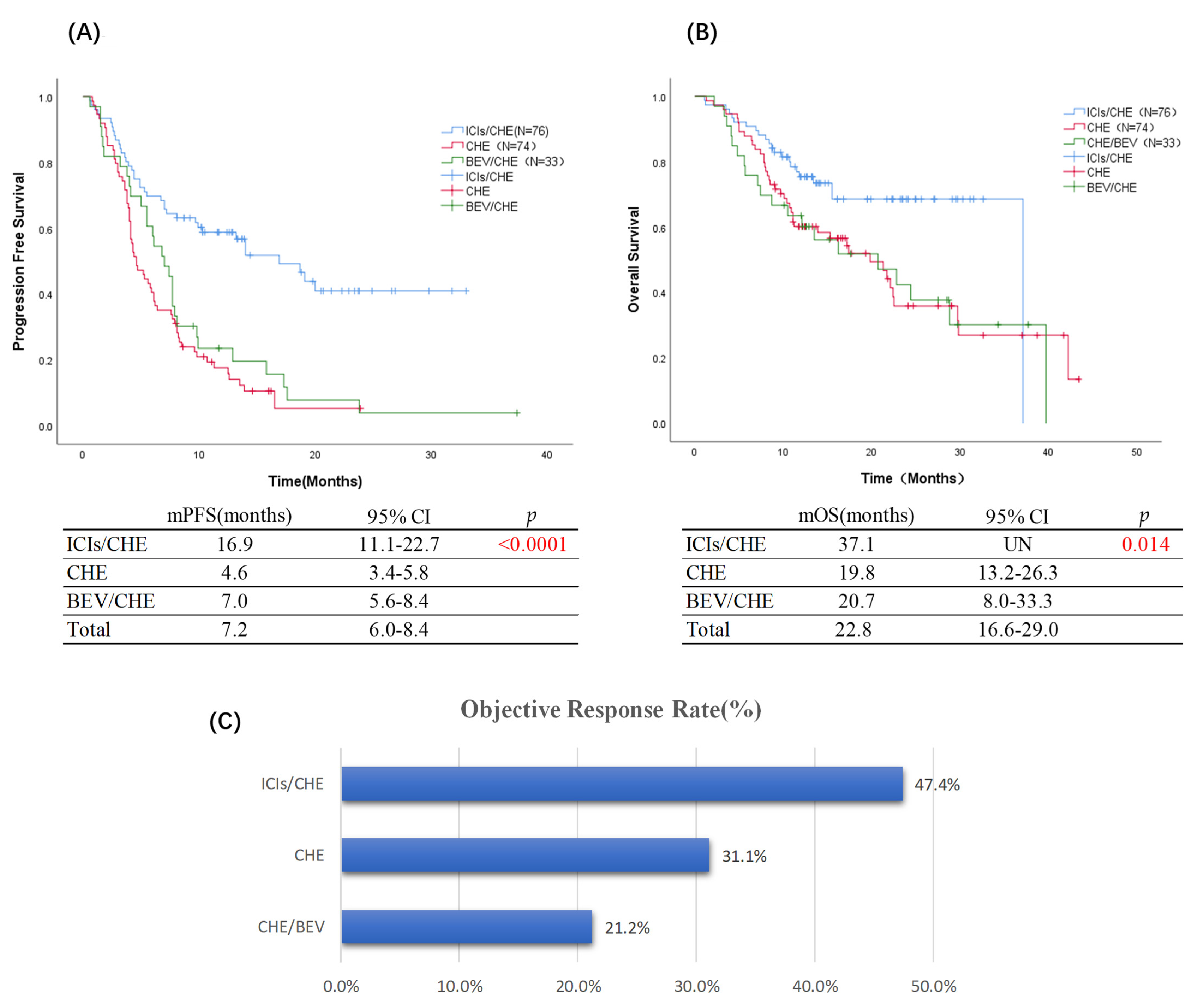
3.2.1. Overall Population
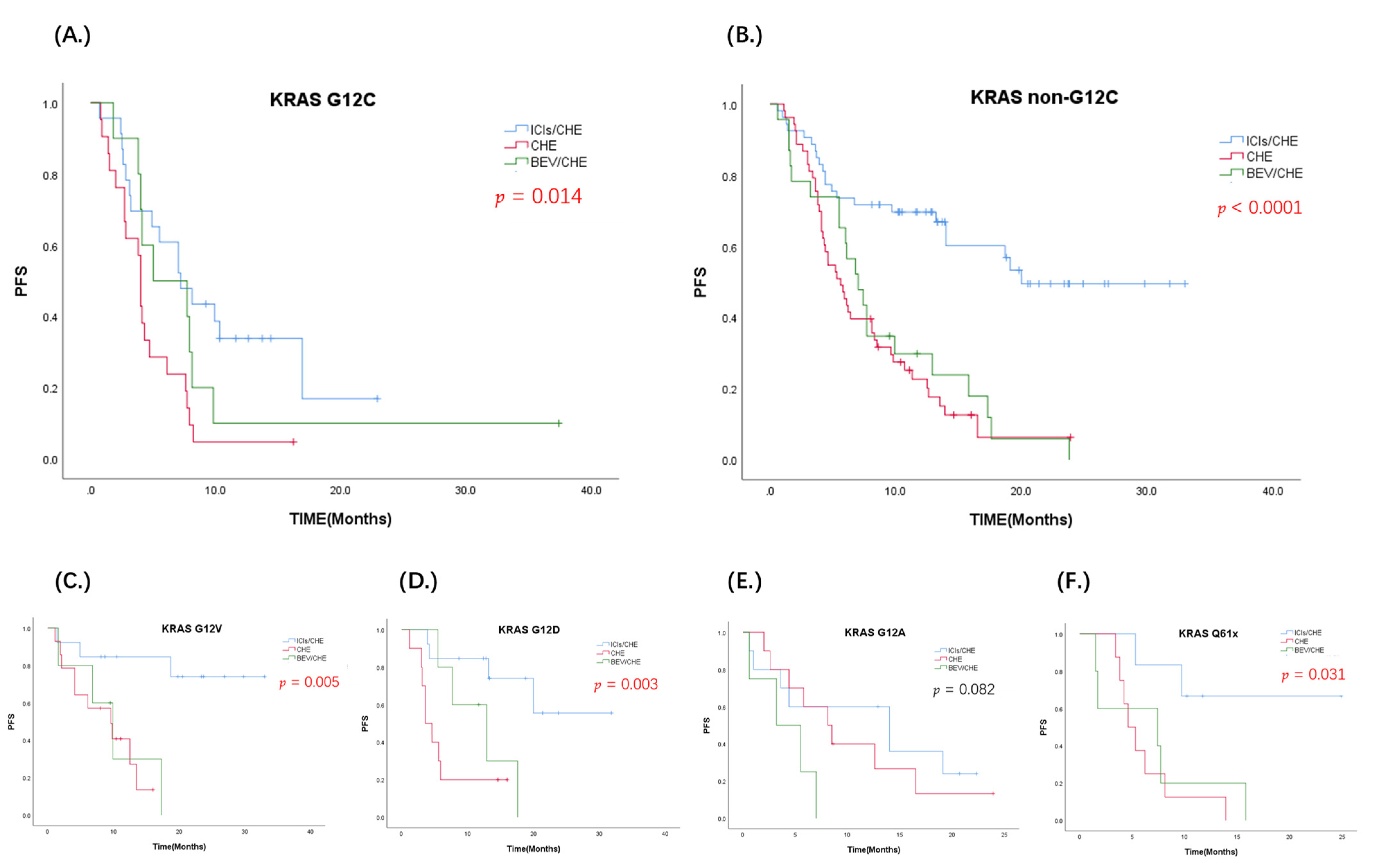
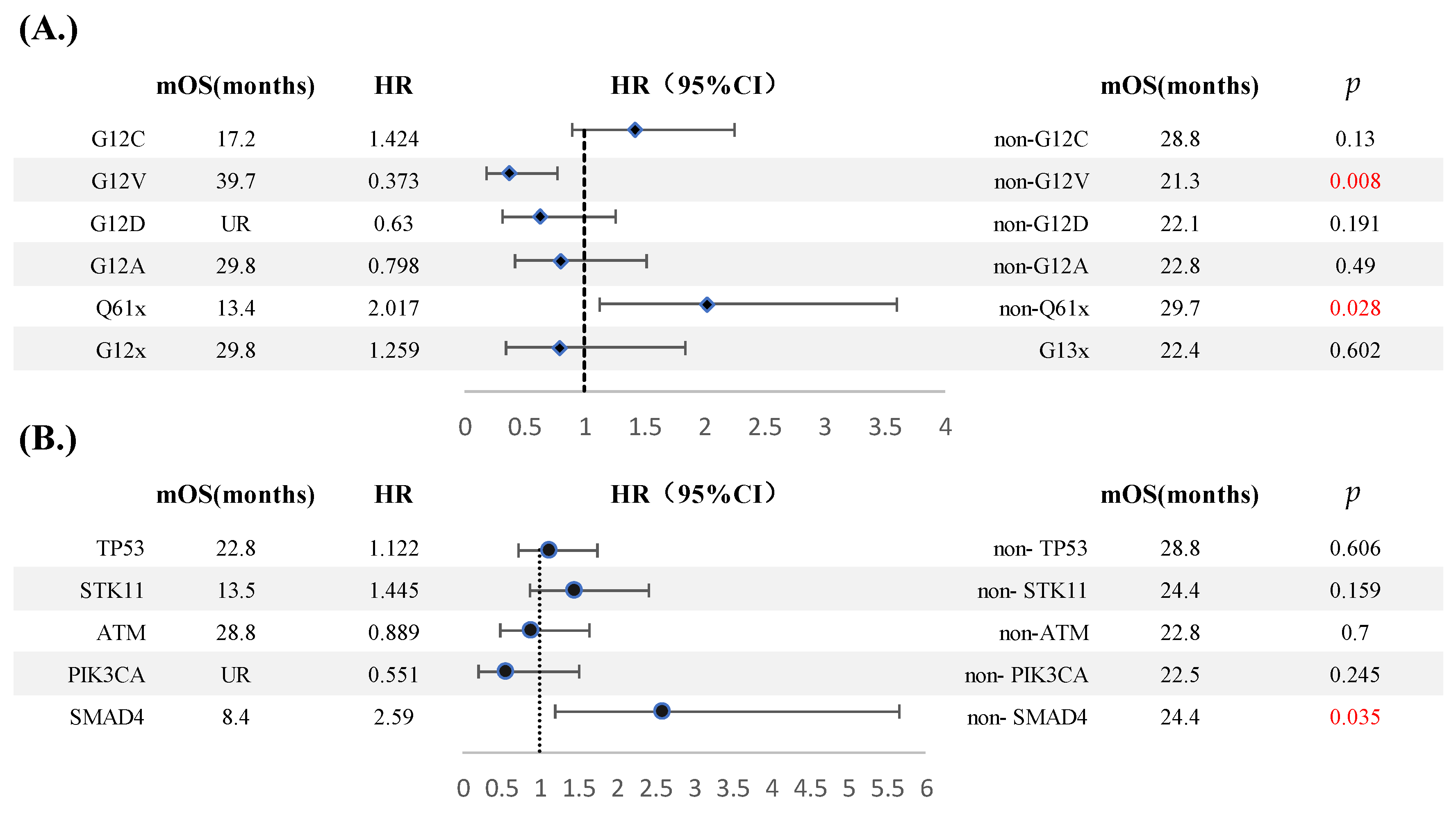
3.2.2. Value of KRAS Subtypes
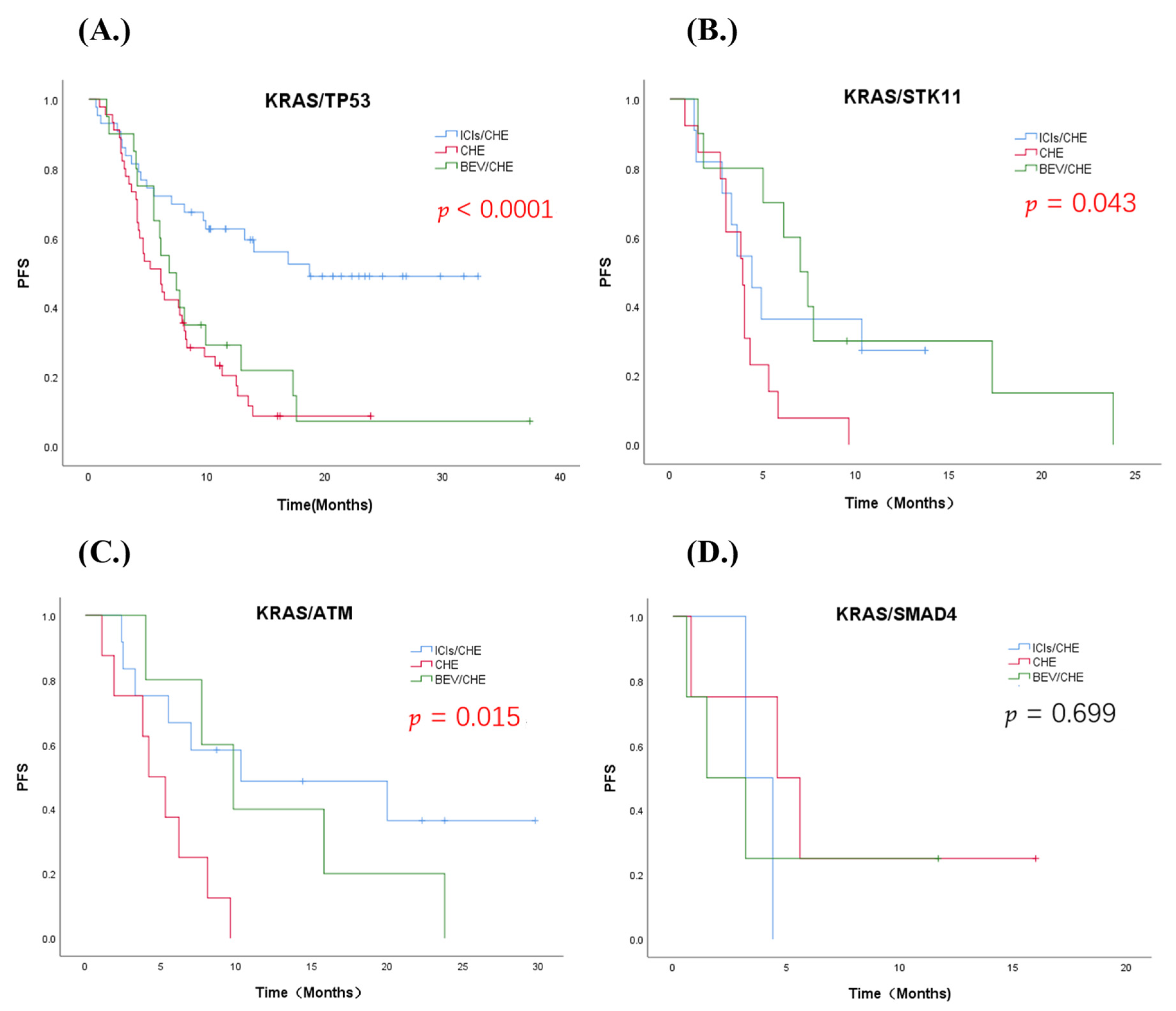
3.2.3. Value of Co-Occurring Mutations
3.3. Prognosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Skoulidis, F.; Heymach, J.V. Co-occurring genomic alterations in non-small-cell lung cancer biology and therapy. Nat. Rev. Cancer 2019, 19, 495–509. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.-Y.; Sun, H.; Zhou, J.-Y.; Jie, G.-L.; Xie, Z.; Shao, Y.; Zhang, X.; Ye, J.-Y.; Chen, C.-X.; Zhang, X.-C.; et al. Clinical characteristics and prognostic value of theKRAS G12Cmutation in Chinese non-small cell lung cancer patients. Biomark. Res. 2020, 8, 22. [Google Scholar] [CrossRef] [PubMed]
- Adachi, Y.; Ito, K.; Hayashi, Y.; Kimura, R.; Tan, T.Z.; Yamaguchi, R.; Ebi, H. Epithelial-to-Mesenchymal Transition is a Cause of Both Intrinsic and Acquired Resistance to KRAS G12C Inhibitor in KRAS G12C-Mutant Non-Small Cell Lung Cancer. Clin. Cancer Res. 2020, 26, 5962–5973. [Google Scholar] [CrossRef]
- Renaud, S.; Seitlinger, J.; Falcoz, P.-E.; Schaeffer, M.; Voegeli, A.-C.; Le Legrain, M.; Beau-Faller, M.; Massard, G. Specific KRAS amino acid substitutions and EGFR mutations predict site-specific recurrence and metastasis following non-small-cell lung cancer surgery. Br. J. Cancer 2016, 115, 346–353. [Google Scholar] [CrossRef] [Green Version]
- West, H.J.; McCleland, M.; Cappuzzo, F.; Reck, M.; Mok, T.S.; Jotte, R.M.; Nishio, M.; Kim, E.; Morris, S.; Zou, W.; et al. Clinical efficacy of atezolizumab plus bevacizumab and chemotherapy in KRAS-mutated non-small cell lung cancer with STK11, KEAP1, or TP53 comutations: Subgroup results from the phase III IMpower150 trial. J. Immunother. Cancer 2022, 10, e003027. [Google Scholar] [CrossRef]
- Hong, D.S.; Fakih, M.G.; Strickler, J.H.; Desai, J.; Durm, G.A.; Shapiro, G.I.; Falchook, G.S.; Price, T.J.; Sacher, A.; Denlinger, C.S.; et al. KRAS(G12C) Inhibition with Sotorasib in Advanced Solid Tumors. N. Engl. J. Med. 2020, 383, 1207–1217. [Google Scholar] [CrossRef] [PubMed]
- Dogan, S.; Shen, R.; Ang, D.C.; Johnson, M.L.; D’Angelo, S.P.; Paik, P.K.; Brzostowski, E.B.; Riely, G.J.; Kris, M.G.; Zakowski, M.F.; et al. Molecular Epidemiology of EGFR and KRAS Mutations in 3,026 Lung Adenocarcinomas: Higher Susceptibility of Women to Smoking-Related KRAS-Mutant Cancers. Clin. Cancer Res. 2012, 18, 6169–6177. [Google Scholar] [CrossRef] [Green Version]
- Dumenil, C.; Vieira, T.; Rouleau, E.; Antoine, M.; Duruisseaux, M.; Poulot, V.; Lacave, R.; Cadranel, J.; Massiani, M.-A.; Wislez, M. Is there a specific phenotype associated with the different subtypes of KRAS mutations in patients with advanced non-small-cell lung cancers? Lung Cancer 2015, 90, 561–567. [Google Scholar] [CrossRef]
- Arbour, K.C.; Jordan, E.; Kim, H.R.; Dienstag, J.; Yu, H.A.; Sanchez-Vega, F.; Lito, P.; Berger, M.; Solit, D.B.; Hellmann, M.; et al. Effects of Co-occurring Genomic Alterations on Outcomes in Patients with KRAS-Mutant Non-Small Cell Lung Cancer. Clin. Cancer Res. 2018, 24, 334–340. [Google Scholar] [CrossRef] [Green Version]
- Skoulidis, F.; Byers, L.A.; Diao, L.; Papadimitrakopoulou, V.A.; Tong, P.; Izzo, J.; Behrens, C.; Kadara, H.; Parra, E.R.; Canales, J.R.; et al. Co-occurring Genomic Alterations Define Major Subsets of KRAS-Mutant Lung Adenocarcinoma with Distinct Biology, Immune Profiles, and Therapeutic Vulnerabilities. Cancer Discov. 2015, 5, 860–877. [Google Scholar] [CrossRef] [Green Version]
- Zer, A.; Ding, K.; Lee, S.M.; Goss, G.D.; Seymour, L.; Ellis, P.M.; Hackshaw, A.; Bradbury, P.A.; Han, L.; O’Callaghan, C.J.; et al. Pooled Analysis of the Prognostic and Predictive Value of KRAS Mutation Status and Mutation Subtype in Patients with Non-Small Cell Lung Cancer Treated with Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors. J. Thorac. Oncol. 2016, 11, 312–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arbour, K.C.; Rizvi, H.; Plodkowski, A.J.; Hellmann, M.D.; Knezevic, A.; Heller, G.; Yu, H.A.; Ladanyi, M.; Kris, M.G.; Arcila, M.E.; et al. Treatment Outcomes and Clinical Characteristics of Patients with KRAS-G12C-Mutant Non-Small Cell Lung Cancer. Clin. Cancer Res. 2021, 27, 2209–2215. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, F.A.; Domerg, C.; Hainaut, P.; Jaenne, P.A.; Pignon, J.-P.; Graziano, S.; Douillard, J.-Y.; Brambilla, E.; Le Chevalier, T.; Seymour, L.; et al. Pooled Analysis of the Prognostic and Predictive Effects of KRAS Mutation Status and KRAS Mutation Subtype in Early-Stage Resected Non-Small-Cell Lung Cancer in Four Trials of Adjuvant Chemotherapy. J. Clin. Oncol. 2013, 31, 2173–2181. [Google Scholar] [CrossRef] [Green Version]
- Skoulidis, F.; Goldberg, M.E.; Greenawalt, D.M.; Hellmann, M.D.; Awad, M.M.; Gainor, J.F.; Schrock, A.B.; Hartmaier, R.J.; Trabucco, S.E.; Gay, L.; et al. STK11/LKB1 Mutations and PD-1 Inhibitor Resistance in KRAS-Mutant Lung Adenocarcinoma. Cancer Discov. 2018, 8, 822–835. [Google Scholar] [CrossRef] [Green Version]
- Tomasini, P.; Mascaux, C.; Jao, K.; Labbe, C.; Kamel-Reid, S.; Stockley, T.; Hwang, D.M.; Leighl, N.B.; Liu, G.; Bradbury, P.A.; et al. Effect of Coexisting KRAS and TP53 Mutations in Patients Treated With Chemotherapy for Non-small-cell Lung Cancer. Clin. Lung Cancer 2019, 20, E338–E345. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodriguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gumus, M.; Mazieres, J.; Hermes, B.; Senler, F.C.; Csoszi, T.; Fulop, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Gadgeel, S.; Rodriguez-Abreu, D.; Felip, E.; Esteban, E.; Speranza, G.; Reck, M.; Hui, R.; Boyer, M.; Garon, E.B.; Horinouchi, H.; et al. KRAS mutational status and efficacy in KEYNOTE-189: Pembrolizumab (pembro) plus chemotherapy (chemo) vs. placebo plus chemo as first-line therapy for metastatic non-squamous NSCLC. Ann. Oncol. 2019, 30, 64–65. [Google Scholar] [CrossRef]
- Herbst, R.S.; Lopes, G.; Kowalski, D.M.; Kasahara, K.; Wu, Y.L.; De Castro, G., Jr.; Cho, B.C.; Turna, H.Z.; Cristescu, R.; Aurora-Garg, D.; et al. Association of KRAS mutational status with response to pembrolizumab monotherapy given as first-line therapy for PD-L1-positive advanced non-squamous NSCLC in KEYNOTE-042. Ann. Oncol. 2019, 30, 63–64. [Google Scholar] [CrossRef]
- Cai, D.; Hu, C.; Li, L.; Deng, S.; Yang, J.; Han, H.-Z.; Li, M. The prevalence and prognostic value of KRAS co-mutation subtypes in Chinese advanced non-small cell lung cancer patients. Cancer Med. 2020, 9, 84–93. [Google Scholar] [CrossRef] [Green Version]
- Jia, Y.; Jiang, T.; Li, X.; Zhao, C.; Zhang, L.; Zhao, S.; Liu, X.; Qiao, M.; Luo, J.; Shi, J.; et al. Characterization of distinct types of KRAS mutation and its impact on first-line platinum-based chemotherapy in Chinese patients with advanced non-small cell lung cancer. Oncol. Lett. 2017, 14, 6525–6532. [Google Scholar] [CrossRef]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fulop, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, Z.-Y.; Zhong, W.-Z.; Liu, S.Y.; Xie, Z.; Wu, S.-P.; Wu, Y.L. Potential Predictive Value of TP53 and KRAS Mutation Status for Response to PD-1 Blockade Immunotherapy in Lung Adenocarcinoma. J. Thorac. Oncol. 2017, 12, S432–S433. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Zheng, S.; Jin, R.; Wang, X.; Wang, F.; Zang, R.; Xu, H.; Lu, Z.; Huang, J.; Lei, Y.; et al. The superior efficacy of anti-PD-1/PD-L1 immunotherapy in KRAS-mutant non-small cell lung cancer that correlates with an inflammatory phenotype for updates and increased immunogenicity. Cancer Lett. 2020, 470, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Aredo, J.V.; Padda, S.K.; Kunder, C.A.; Han, S.S.; Neal, J.W.; Shrager, J.B.; Wakelee, H.A. Impact of KRAS mutation subtype and concurrent pathogenic mutations on non-small cell lung cancer outcomes. Lung Cancer 2019, 133, 144–150. [Google Scholar] [CrossRef]
- Gu, M.; Xu, T.; Chang, P. KRAS/LKB1 and KRAS/TP53 co-mutations create divergent immune signatures in lung adenocarcinomas. Ther. Adv. Med. Oncol. 2021, 13, 1–13. [Google Scholar] [CrossRef]
- Pons-Tostivint, E.; Lugat, A.; Fontenau, J.F.; Denis, M.G.; Bennouna, J. STK11/LKB1 Modulation of the Immune Response in Lung Cancer: From Biology to Therapeutic Impact. Cells 2021, 10, 3129. [Google Scholar] [CrossRef]
- Chaft, J.E.; Rusch, V.; Ginsberg, M.S.; Paik, P.K.; Finley, D.J.; Kris, M.G.; Price, K.A.R.; Azzoli, C.G.; Fury, M.G.; Riely, G.J.; et al. Phase II trial of neoadjuvant bevacizumab plus chemotherapy and adjuvant bevacizumab in patients with resectable nonsquamous non-small-cell lung cancers. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2013, 8, 1084–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghimessy, A.K.; Gellert, A.; Schlegl, E.; Hegedus, B.; Raso, E.; Barbai, T.; Timar, J.; Ostoros, G.; Megyesfalvi, Z.; Gieszer, B.; et al. KRAS Mutations Predict Response and Outcome in Advanced Lung Adenocarcinoma Patients Receiving First-Line Bevacizumab and Platinum-Based Chemotherapy. Cancers 2019, 11, 1514. [Google Scholar] [CrossRef] [Green Version]
- Bonanno, L.; De Paoli, A.; Zulato, E.; Esposito, G.; Calabrese, F.; Favaretto, A.; Santo, A.; Del Conte, A.; Chilosi, M.; Oniga, F.; et al. LKB1 Expression Correlates with Increased Survival in Patients with Advanced Non-Small Cell Lung Cancer Treated with Chemotherapy and Bevacizumab. Clin. Cancer Res. 2017, 23, 3316–3324. [Google Scholar] [CrossRef] [Green Version]
- Rodenhuis, S.; van de Wetering, M.L.; Mooi, W.J.; Evers, S.G.; van Zandwijk, N.; Bos, J.L. Mutational activation of the K-ras oncogene. A possible pathogenetic factor in adenocarcinoma of the lung. N. Engl. J. Med. 1987, 317, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Meng, D.; Yuan, M.; Li, X.; Chen, L.; Yang, J.; Zhao, X.; Ma, W.; Xin, J. Prognostic value of K-RAS mutations in patients with non-small cell lung cancer: A systematic review with meta-analysis. Lung Cancer 2013, 81, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Jiang, W.; Wang, H.; He, J.; Su, C.; Yu, Q. Impact of Smoking History on Response to Immunotherapy in Non-Small-Cell Lung Cancer: A Systematic Review and Meta-Analysis. Front. Oncol 2021, 11, 703143. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.-N.; Ma, Y.-F.; Li, Z.; Hu, J.-A.; Xu, Z.-H. KRAS G12V mutation upregulates PD-L1 expression via TGF-beta/EMT signaling pathway in human non-small-cell lung cancer. Cell Biol. Int. 2021, 45, 795–803. [Google Scholar] [CrossRef]
- Gu, J.; Zhou, Y.; Huang, L.; Ou, W.; Wu, J.; Li, S.; Xu, J.; Feng, J.; Liu, B. TP53 mutation is associated with a poor clinical outcome for non-small cell lung cancer: Evidence from a meta-analysis. Mol. Clin. Oncol. 2016, 5, 705–713. [Google Scholar] [CrossRef] [Green Version]
- Goldstraw, P.; Ball, D.; Jett, J.R.; Le Chevalier, T.; Lim, E.; Nicholson, A.G.; Shepherd, F.A. Non-small-cell lung cancer. Lancet 2011, 378, 1727–1740. [Google Scholar] [CrossRef]
- Ke, Z.; Zhang, X.; Ma, L.; Wang, L. Expression of DPC4/Smad4 in non-small-cell lung carcinoma and its relationship with angiogenesis. Neoplasma 2008, 55, 323–329. [Google Scholar]
- Zhang, S.; Takaku, M.; Zou, L.Y.; Gu, A.D.; Chou, W.C.; Zhang, G.; Wu, B.; Kong, Q.; Thomas, S.Y.; Serody, J.S.; et al. Reversing SKI-SMAD4-mediated suppression is essential for T(H)17 cell differentiation. Nature 2017, 551, 105–109. [Google Scholar] [CrossRef]
- Salazar, Y.; Zheng, X.; Brunn, D.; Raifer, H.; Picard, F.; Zhang, Y.; Winter, H.; Guenther, S.; Weigert, A.; Weigmann, B.; et al. Microenvironmental Th9 and Th17 lymphocytes induce metastatic spreading in lung cancer. J. Clin. Investig. 2020, 130, 3560–3575. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CHE/ICIs (N = 76) | CHE (N = 74) | CHE/BEV (N = 33) | Total (N = 183) | p-Value | |
|---|---|---|---|---|---|
| Age—years old | |||||
| Median | 62.1 | 64.1 | 63.1 | 63.1 | |
| Range | 31–81 | 47–76 | 47–77 | 31–81 | |
| Sex (%) | 0.278 | ||||
| Male | 63 (82.9%) | 65 (87.8%) | 31 (93.9%) | 159 (86.9%) | |
| Female | 13 (17.1%) | 9 (12.2%) | 2 (6.1%) | 24 (13.1%) | |
| Disease stage (%) | 0.094 | ||||
| III | 18 (23.7%) | 15 (20.3%) | 2 (6.1%) | 35 (19.1%) | |
| IV | 58 (76.3%) | 59 (79.7%) | 31 (93.9%) | 148 (80.9%) | |
| Smoking status (%) | 0.569 | ||||
| More than 20 pack-years | 43 (56.6%) | 44 (59.5%) | 16 (48.5%) | 100 (54.6%) | |
| Less than 20 pack-years | 33 (43.4%) | 30 (40.5%) | 17 (51.5%) | 83 (45.4%) | |
| Lesion location | 0.630 | ||||
| Upper left | 20 (26.3%) | 25 (33.8%) | 13 (39.4%) | 58 (31.7%) | |
| Lower left | 9 (11.8%) | 10 (13.5%) | 2 (6.1%) | 21 (11.5%) | |
| Upper right | 32 (42.1%) | 26 (35.1%) | 12 (36.4%) | 70 (38.3%) | |
| Right middle | 5 (6.6%) | 1 (1.4%) | 1 (3.0%) | 7 (3.8%) | |
| Lower right | 10 (13.2%) | 12 (16.2%) | 4 (12.1%) | 26 (14.2%) | |
| ECOG PS score (%) | 0.209 | ||||
| 0 | 33 (%) | 24 (32.4%) | 16 (48.5%) | 73 (39.9%) | |
| 1 | 43 (%) | 50 (67.6%) | 17 (51.5%) | 110 (60.1%) | |
| Histologic type (%) | 0.174 | ||||
| Adenocarcinoma | 59 (77.6%) | 61 (82.4%) | 31 (93.9%) | 151 (82.5%) | |
| Squamous carcinoma | 3 (3.9%) | 3 (4.1%) | 0 (0%) | 6 (3.3%) | |
| NSCLC not otherwise specified (NSCLC-NOS) | 14 (18.4%) | 8 (10.8%) | 2 (6.1%) | 22 (12.0%) | |
| Neuroendocrine carcinoma | 0 (0%) | 2 (2.7%) | 0 (0%) | 2 (1.1%) | |
| Metastatic organ (%) | 0.847 | ||||
| Intrathoracic | 25 (32.9%) | 37 (50.0%) | 21 (63.6%) | 83 (45.4%) | |
| Brain | 10 (13.2%) | 8 (10.8%) | 9 (27.3%) | 27 (14.8%) | |
| Bone | 28 (36.8%) | 35 (47.3%) | 16 (48.5%) | 79 (43.2%) | |
| Adrenal gland | 11 (14.5%) | 6 (8.1%) | 5 (15.2%) | 22 (12.0%) | |
| Liver | 3 (4.0%) | 3 (4.1%) | 2 (6.1%) | 8 (4.4%) | |
| Others | 9 (11.8%) | 9 (12.2%) | 5 (15.2%) | 23 (12.6%) | |
| PD-L1 expression (%) | N = 56/76(73.7%) | N = 40/74(54.1%) | N = 18/33 (54.5%) | N = 114/183 (62.3%) | 0.003 |
| 0 | 12 (21.4%) | 11(27.5%) | 11 (61.1%) | 34 (29.8%) | |
| ≥1% | 44 (78.6%) | 29(72.5%) | 7 (38.9%) | 80 (70.2%) |
| Variable | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Gender | ||||||
| Male | 1 | |||||
| Female | 0.593 | 0.273–1.287 | 0.186 | 0.481 | 0.172–1.347 | 0.164 |
| performance status, PS | ||||||
| 0 | 1 | |||||
| 1 | 2.212 | 1.379–3.546 | 0.001 ** | 3.604 | 1.630–7.967 | 0.002 * |
| Stage | ||||||
| III | 1 | |||||
| IV | 2.722 | 1.255–5.908 | 0.011 * | 1.191 | 0.473–2.999 | 0.711 |
| Smoker | ||||||
| <20 pack-year | 1 | |||||
| ≥20 pack-year | 0.958 | 0.620–1.481 | 0.847 | 0.450 | 0.210–0.962 | 0.039 * |
| PD-L1 | ||||||
| 0% | 1 | |||||
| ≥1% | 0.292 | 0.377–1.341 | 0.711 | 1.504 | 0.629–3.595 | 0.359 |
| G12V | ||||||
| non-G12V | 1 | |||||
| G12V | 0.373 | 0.179–0.777 | 0.008 * | 0.432 | 0.148–1.257 | 0.124 |
| Q61x | ||||||
| non-Q61x | 1 | |||||
| Q61x | 1.961 | 1.079–3.563 | 0.027 * | 1.267 | 0.478–3.358 | 0.634 |
| STK11 | ||||||
| non-STK11 | 1 | |||||
| STK11 | 1.445 | 1.445–2.413 | 0.159 | 2.359 | 0.947–5.877 | 0.065 |
| SMAD4 | ||||||
| non-SMAD4 | 1 | |||||
| SMAD4 | 2.590 | 1.187–5.651 | 0.017 * | 4.293 | 1.179–15.628 | 0.027 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, Y.; Li, Z.; Jian, H.; Xia, L.; Lu, S. Impact of KRAS Mutation Subtypes and Co-Occurring Mutations on Response and Outcome in Advanced NSCLC Patients following First-Line Treatment. J. Clin. Med. 2022, 11, 4003. https://doi.org/10.3390/jcm11144003
Sun Y, Li Z, Jian H, Xia L, Lu S. Impact of KRAS Mutation Subtypes and Co-Occurring Mutations on Response and Outcome in Advanced NSCLC Patients following First-Line Treatment. Journal of Clinical Medicine. 2022; 11(14):4003. https://doi.org/10.3390/jcm11144003
Chicago/Turabian StyleSun, Yingjia, Ziming Li, Hong Jian, Liliang Xia, and Shun Lu. 2022. "Impact of KRAS Mutation Subtypes and Co-Occurring Mutations on Response and Outcome in Advanced NSCLC Patients following First-Line Treatment" Journal of Clinical Medicine 11, no. 14: 4003. https://doi.org/10.3390/jcm11144003