
Octogenarians Are the New Sexagenarians: Cruciate-Retaining Total Knee Arthroplasty Is Not Inferior to Posterior-Stabilized Arthroplasty in Octogenarian Patients

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Rehabilitation Protocol
2.2. Clinical Evaluation
2.3. Survivorship
2.4. Statistical Analysis
2.5. Data Analysis
3. Results
3.1. Demographic Data
3.2. Clinical Results
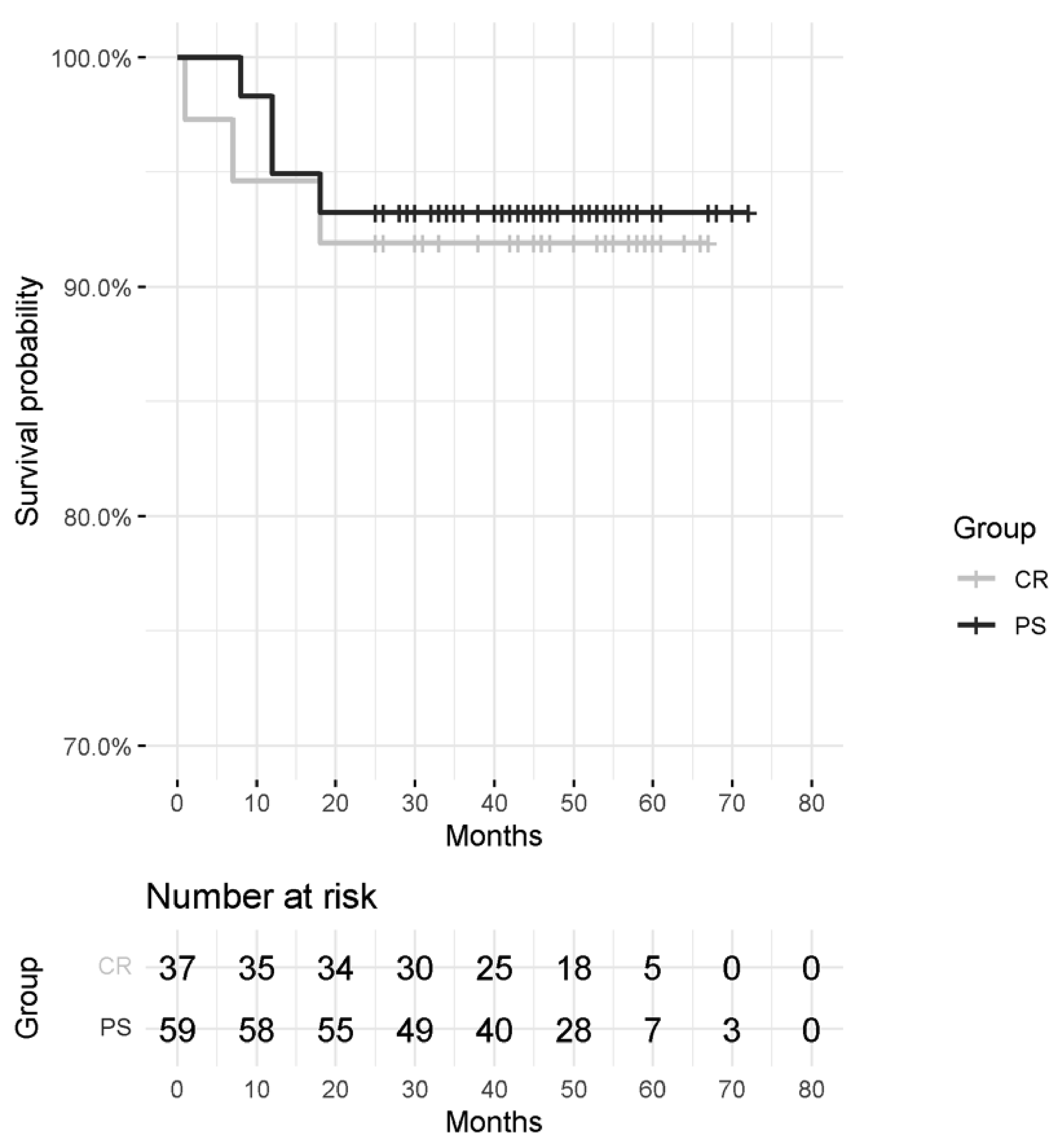
3.3. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sharma, L. Osteoarthritis of the Knee. N. Engl. J. Med. 2021, 384, 51–59. [Google Scholar] [CrossRef]
- Sanderson, W.C.; Scherbov, S. Measuring the speed of aging across population subgroups. PLoS ONE 2014, 9, e96289. [Google Scholar] [CrossRef] [Green Version]
- Vitaloni, M.; Botto-van Bemden, A.; Sciortino Contreras, R.M.; Scotton, D.; Bibas, M.; Quintero, M.; Monfort, J.; Carné, X.; de Abajo, F.; Oswald, E.; et al. Global management of patients with knee osteoarthritis begins with quality of life assessment: A systematic review. BMC Musculoskelet. Disord. 2019, 20, 493. [Google Scholar] [CrossRef]
- Li, N.; Tan, Y.; Deng, Y.; Chen, L. Posterior cruciate-retaining versus posterior stabilized total knee arthroplasty: A meta-analysis of randomized controlled trials. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 556–564. [Google Scholar] [CrossRef]
- Longo, U.G.; Ciuffreda, M.; Mannering, N.; D’Andrea, V.; Locher, J.; Salvatore, G.; Denaro, V. Outcomes of Posterior-Stabilized Compared with Cruciate-Retaining Total Knee Arthroplasty. J. Knee Surg. 2018, 31, 321–340. [Google Scholar] [CrossRef]
- Song, S.J.; Park, C.H.; Bae, D.K. What to Know for Selecting Cruciate-Retaining or Posterior-Stabilized Total Knee Arthroplasty. Clin. Orthop. Surg. 2019, 11, 142–150. [Google Scholar] [CrossRef]
- The Swedish Knee Arthroplasty Register; Annual Report 2020—Part I; Lund University: Lund, Sweden. 2020. Available online: https://www.myknee.se/pdf/SVK_2020_Eng_1.0.pdf (accessed on 19 May 2022).
- Broberg, J.S.; Ndoja, S.; MacDonald, S.J.; Lanting, B.A.; Teeter, M.G. Comparison of Contact Kinematics in Posterior-Stabilized and Cruciate-Retaining Total Knee Arthroplasty at Long-Term Follow-Up. J. Arthroplast. 2020, 35, 272–277. [Google Scholar] [CrossRef] [Green Version]
- Soong, J.; Ou Yang, Y.; Ling, Z.M.; Chia, S.L.; Lo, N.N.; Yeo, S.J. Cruciate retaining and posterior stabilized total knee arthroplasty in severe varus osteoarthritis knee: A match-pair comparative study in an Asian population. J. Orthop. Surg. 2021, 9, 23094990211055224. [Google Scholar] [CrossRef]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13 (Suppl. S1), S31–S34. [Google Scholar] [CrossRef]
- Gademan, M.G.; Hofstede, S.N.; Vliet Vlieland, T.P.; Nelissen, R.G.; Marang-van de Mheen, P.J. Indication criteria for total hip or knee arthroplasty in osteoarthritis: A state-of-the-science overview. BMC Musculoskelet. Disord. 2016, 17, 463. [Google Scholar] [CrossRef] [Green Version]
- D’Anchise, R.; Andreata, M.; Balbino, C.; Manta, N. Posterior cruciate ligament-retaining and posterior-stabilized total knee arthroplasty: Differences in surgical technique. Joints 2013, 1, 5–9. [Google Scholar]
- Heller, G.Z.; Manuguerra, M.; Chow, R. How to analyze the Visual Analogue Scale: Myths, truths and clinical relevance. Scand. J. Pain 2017, 13, 67–75. [Google Scholar] [CrossRef]
- Padua, R.; Zanoli, G.; Ceccarelli, E.; Romanini, E.; Bondì, R.; Campi, A. The Italian version of the Oxford 12-item Knee Questionnaire-cross-cultural adaptation and validation. Int. Orthop. 2003, 27, 214–216. [Google Scholar] [CrossRef] [Green Version]
- Scuderi, G.R.; Bourne, R.B.; Noble, P.C.; Benjamin, J.B.; Lonner, J.H.; Scott, W.N. The new Knee Society Knee Scoring System. Clin. Orthop. Relat. Res. 2012, 470, 3–19. [Google Scholar] [CrossRef] [Green Version]
- Lacny, S.; Wilson, T.; Clement, F.; Roberts, D.J.; Faris, P.D.; Ghali, W.A.; Marshall, D.A. Kaplan-Meier Survival Analysis Overestimates the Risk of Revision Arthroplasty: A Meta-analysis. Clin. Orthop. Relat. Res. 2015, 473, 3431–3442. [Google Scholar] [CrossRef] [Green Version]
- Singleton, N.; Nicholas, B.; Gormack, N.; Stokes, A. Differences in outcome after cruciate retaining and posterior stabilized total knee arthroplasty. J. Orthop. Surg. 2019, 27, 2309499019848154. [Google Scholar] [CrossRef]
- Kolisek, F.R.; McGrath, M.S.; Marker, D.R.; Jessup, N.; Seyler, T.M.; Mont, M.A.; Lowry Barnes, C. Posterior-stabilized versus posterior cruciate ligament-retaining total knee arthroplasty. Iowa Orthop. J. 2009, 29, 23–27. [Google Scholar]
- Heckmann, N.D.; Steck, T.; Sporer, S.M.; Meneghini, R.M. Conforming Polyethylene Inserts in Total Knee Arthroplasty: Beyond the Posterior-Stabilized and Cruciate-Retaining Debate. J. Am. Acad. Orthop. Surg. 2021, 29, e1097–e1104. [Google Scholar] [CrossRef]
- Koh, I.J.; Chalmers, C.E.; Lin, C.C.; Park, S.B.; McGarry, M.H.; Lee, T.Q. Posterior stabilized total knee arthroplasty reproduces natural joint laxity compared to normal in kinematically aligned total knee arthroplasty: A matched pair cadaveric study. Arch. Orthop. Trauma Surg. 2021, 141, 119–127. [Google Scholar] [CrossRef]
- Marya, S.K.S.; Singh, C. Options and limitations of implant constraint. J. Orthop. 2020, 23, 18–24. [Google Scholar] [CrossRef]
- Verra, W.C.; van den Boom, L.G.; Jacobs, W.; Clement, D.J.; Wymenga, A.A.; Nelissen, R.G. Retention versus sacrifice of the posterior cruciate ligament in total knee arthroplasty for treating osteoarthritis. Cochrane Database Syst. Rev. 2013, 2013, CD004803. [Google Scholar] [CrossRef] [Green Version]
- Harato, K.; Bourne, R.B.; Victor, J.; Snyder, M.; Hart, J.; Ries, M.D. Midterm comparison of posterior cruciate-retaining versus substituting total knee arthroplasty using the Genesis II prosthesis. A multicenter prospective randomized clinical trial. Knee 2008, 15, 217–221. [Google Scholar] [CrossRef]
- Tanzer, M.; Smith, K.; Burnett, S. Posterior-stabilized versus cruciate-retaining total knee arthroplasty: Balancing the gap. J. Arthroplast. 2002, 17, 813–819. [Google Scholar] [CrossRef]
- Inouye, K.; Pedrazzani, E.S. Educational status, social economic status and evaluation of some dimensions of octogenarians’ quality of life. Revista Latino-Americana de Enfermagem 2007, 15, 742–747. [Google Scholar] [CrossRef] [Green Version]
- Morcos, M.W.; Nowak, L.; Schemitsch, E. Prolonged surgical time increases the odds of complications following total knee arthroplasty. Can J. Surg. 2021, 64, E273–E279. [Google Scholar] [CrossRef]
- Kuperman, E.F.; Schweizer, M.; Joy, P.; Gu, X.; Fang, M.M. The effects of advanced age on primary total knee arthroplasty: A meta-analysis and systematic review. BMC Geriatr. 2016, 16, 41. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, J.W.; Johnston, L.; Cochrane, L.; Boscainos, P.J. Total knee arthroplasty in the elderly: Does age affect pain, function or complications? Clin. Orthop. Relat. Res. 2013, 471, 1964–1969. [Google Scholar] [CrossRef] [Green Version]
- Souza, G.G.A.; Ramalho, R.S.C.; Albuquerque, R.S.P.E.; Barretto, J.M.; Chaves, R.S.M.; de Sousa, E.B. Higher risk of complications after total knee arthroplasty in octogenarians. Acta Ortop. Bras. 2020, 28, 177–181. [Google Scholar] [CrossRef]
- Klasan, A.; Putnis, S.E.; Yeo, W.W.; Fritsch, B.A.; Coolican, M.R.; Parker, D.A. Advanced Age Is Not a Barrier to Total Knee Arthroplasty: A Detailed Analysis of Outcomes and Complications in an Elderly Cohort Compared with Average Age Total Knee Arthroplasty Patients. J. Arthroplast. 2019, 34, 1938–1945. [Google Scholar] [CrossRef]
- Passias, P.G.; Bono, O.J.; Bono, J.V. Total Knee Arthroplasty in Patients of Advanced Age: A Look at Outcomes and Complications. J. Knee Surg. 2020, 33, 1–7. [Google Scholar] [CrossRef]


{kind=link}
| Group | |||
|---|---|---|---|
| CR n = 37 Mean ± SD | PS n = 59 Mean ± SD | p-Value | |
| Age | 82.30 ± 2.17 | 81.51 ± 1.83 | 0.063 |
| Sex, n (%) | |||
| F | 27 (73.0) | 43 (72.9) | 1.000 |
| M | 10 (27.0) | 16 (27.1) | |
| Side, n (%) | |||
| Right | 21 (56.8) | 34 (57.6) | 1.000 |
| Left | 16 (43.2) | 25 (42.4) | |
| Surgical time | 48.70 ± 7.83 | 56.19 ± 11.43 | 0.001 * |
| Preoperative scores | |||
| VAS | 7.46 ± 1.39 | 7.39 ± 1.26 | 0.800 |
| Flexion | 90.35 ± 8.20 | 90.36 ± 9.39 | 0.998 |
| Extension | 4.86 ± 3.22 | 4.93 ± 2.86 | 0.853 |
| KSS | 36.76 ± 9.30 | 36.75 ± 8.79 | 0.995 |
| OKS | 20.59 ± 4.13 | 20.80 ± 3.60 | 0.692 |
| Follow-up (months) | |||
| T1 | 13.00 ± 0.97 | 12.98 ± 1.09 | 0.743 |
| T2 | 47.46 ± 12.26 | 47.35 ± 12.52 | 0.967 |
| CR Group | PS Group | Group Comparison | Time Comparison Adjusted p-Value | ||||
|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | p-Value | CR | PS | |||
| VAS | |||||||
| T0 | 7.46 ± 1.39 (n = 37) | 7.39 ± 1.26 (n = 59) | 0.800 | T0 | T1 | T0 | T1 |
| T1 | 1.66 ± 1.39 (n = 35) | 2.05 ± 1.34 (n = 57) | 0.179 | <0.001 * | - | <0.001 * | - |
| T2 | 1.56 ± 1.33 (n = 34) | 1.53 ± 1.02 (n = 55) | 0.900 | <0.001 * | >0.99 | <0.001 * | 0.002 * |
| Flexion (°) | |||||||
| T0 | 90.35 ± 8.20 (n = 37) | 90.36 ± 9.39 (n = 59) | 0.998 | T0 | T1 | T0 | T1 |
| T1 | 116.14 ± 5.57 (n = 35) | 113.16 ± 7.66 (n = 57) | 0.048* | <0.001 * | - | <0.001 * | - |
| T2 | 120.00 ± 3.69 (n = 34) | 118.91 ± 4.27 (n = 55) | 0.221 | <0.001 * | 0.007 * | <0.001 * | <0.001 * |
| Extension (°) | |||||||
| T0 | 4.86 ± 3.22 (n = 37) | 4.93 ± 2.86 (n = 59) | 0.853 | T0 | T1 | T0 | T1 |
| T1 | 1.14 ± 2.45 (n = 35) | 2.11 ± 2.98 (n = 57) | 0.093 | <0.001 * | - | <0.001 * | - |
| T2 | 1.18 ± 2.48 (n = 34) | 1.18 ± 2.35 (n = 55) | 0.915 | <0.001 * | >0.99 | <0.001 * | 0.014 * |
| KSS | |||||||
| T1 | 36.76 ± 9.30 (n = 37) | 36.75 ± 8.79 (n = 59) | 0.995 | T0 | T1 | T0 | T1 |
| T2 | 91.00 ± 5.53 (n = 35) | 89.39 ± 7.08 (n = 57) | 0.253 | <0.001 * | - | <0.001 * | - |
| T3 | 91.62 ± 5.03 (n = 34) | 91.09 ± 5.50 (n = 55) | 0.652 | <0.001 * | 0.316 | <0.001 * | 0.002 * |
| OKS | |||||||
| T1 | 20.59 ± 4.13 (n = 37) | 20.80 ± 3.60 (n = 59) | 0.692 | T0 | T1 | T0 | T1 |
| T2 | 43.86 ± 1.77 (n = 35) | 43.72 ± 2.03 (n = 57) | 0.588 | <0.001 * | - | <0.001 * | - |
| T3 | 44.09 ± 1.85 (n = 34) | 43.98 ± 2.26 (n = 55) | 0.772 | <0.001 * | >0.99 | <0.001 * | >0.99 |
| Group | ||
|---|---|---|
| CR n = 37 | PS n = 59 | |
| Failures at T1 | ||
| Death | 1 (7th month) | 1 (8th month) |
| Infection | 1 (1st month) | 0 |
| Periprosthetic Fracture | 0 | 1 (12th month) |
| Failures at T2 | ||
| Death | 1 (18th month) | 2 (18th and 28th month) |
| Total number of failures | 3 | 4 |
| Month | Number of Patients at Risk | Number of Failures | Survival Probability % (SE) |
|---|---|---|---|
| CR group | |||
| 1 | 37 | 1 | 97.3 (2.67) |
| 7 | 36 | 1 | 94.6 (3.72) |
| 18 | 35 | 1 | 91.9 (4.49) |
| PS group | |||
| 8 | 59 | 1 | 98.3 (1.68) |
| 12 | 58 | 2 | 94.9 (2.86) |
| 18 | 56 | 1 | 93.2 (3.27) |
| Difference in survival time: chi-squared test p-value = 0.789 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Ambrosi, R.; Menon, P.H.; Salunke, A.; Mariani, I.; Palminteri, G.; Basile, G.; Ursino, N.; Mangiavini, L.; Hantes, M. Octogenarians Are the New Sexagenarians: Cruciate-Retaining Total Knee Arthroplasty Is Not Inferior to Posterior-Stabilized Arthroplasty in Octogenarian Patients. J. Clin. Med. 2022, 11, 3795. https://doi.org/10.3390/jcm11133795
D’Ambrosi R, Menon PH, Salunke A, Mariani I, Palminteri G, Basile G, Ursino N, Mangiavini L, Hantes M. Octogenarians Are the New Sexagenarians: Cruciate-Retaining Total Knee Arthroplasty Is Not Inferior to Posterior-Stabilized Arthroplasty in Octogenarian Patients. Journal of Clinical Medicine. 2022; 11(13):3795. https://doi.org/10.3390/jcm11133795
Chicago/Turabian StyleD’Ambrosi, Riccardo, Prem Haridas Menon, Abhijeet Salunke, Ilaria Mariani, Giovanni Palminteri, Giuseppe Basile, Nicola Ursino, Laura Mangiavini, and Michael Hantes. 2022. "Octogenarians Are the New Sexagenarians: Cruciate-Retaining Total Knee Arthroplasty Is Not Inferior to Posterior-Stabilized Arthroplasty in Octogenarian Patients" Journal of Clinical Medicine 11, no. 13: 3795. https://doi.org/10.3390/jcm11133795