
Risk of SARS-CoV-2 Reinfections in a Prospective Inception Cohort Study: Impact of COVID-19 Vaccination

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
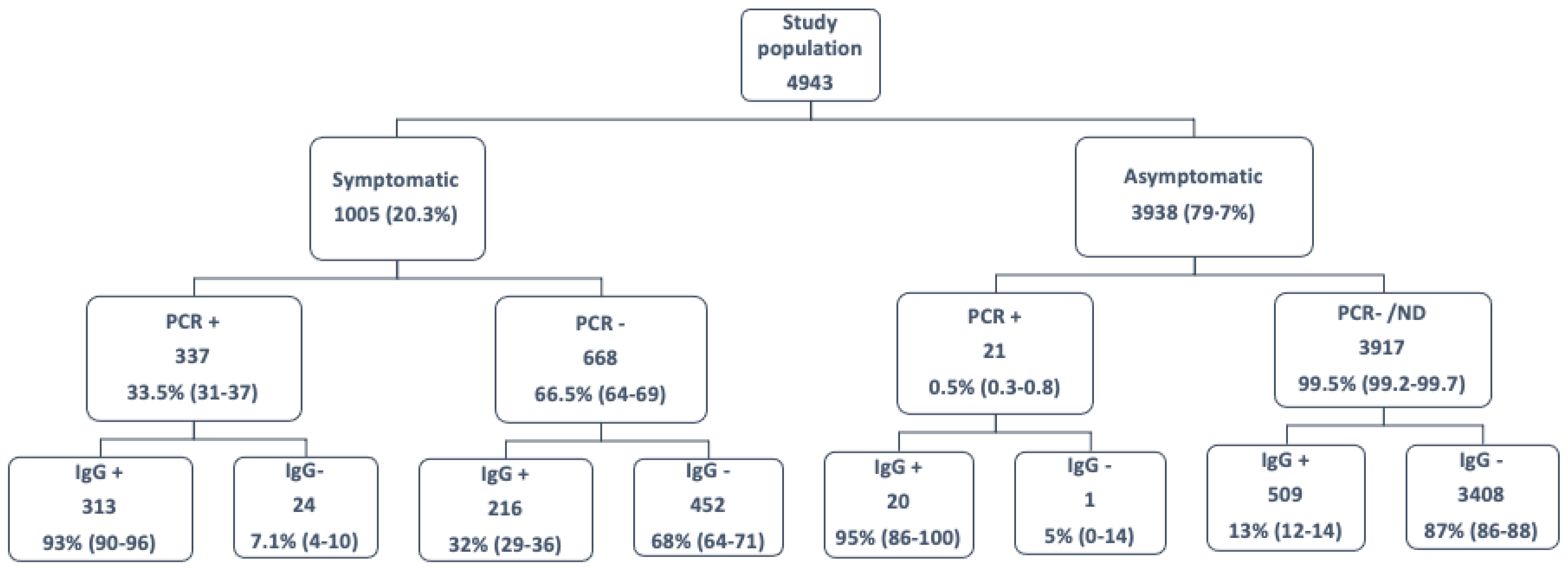
- (a)
- Symptomatic HCWs with a confirmed disease (positive PCR OR/AND positive specific serology);
- (b)
- Symptomatic HCWs with positive PCR AND negative serology;
- (c)
- Symptomatic HCWs suggestive of COVID-19 but without laboratory confirmation (negative PCR AND negative specific serology);
- (d)
- Asymptomatic cases tested positive for viral RNA, due to close contact with a partner or an unknown patient, OR with a positive serology result in the early survey;
- (e)
- Asymptomatic patients who were not tested for viral RNA or were negative, and who had a negative serology result in the early survey.
2.1. Ethics Statement
2.2. Laboratory Procedures
2.3. Statistical Analysis
3. Results
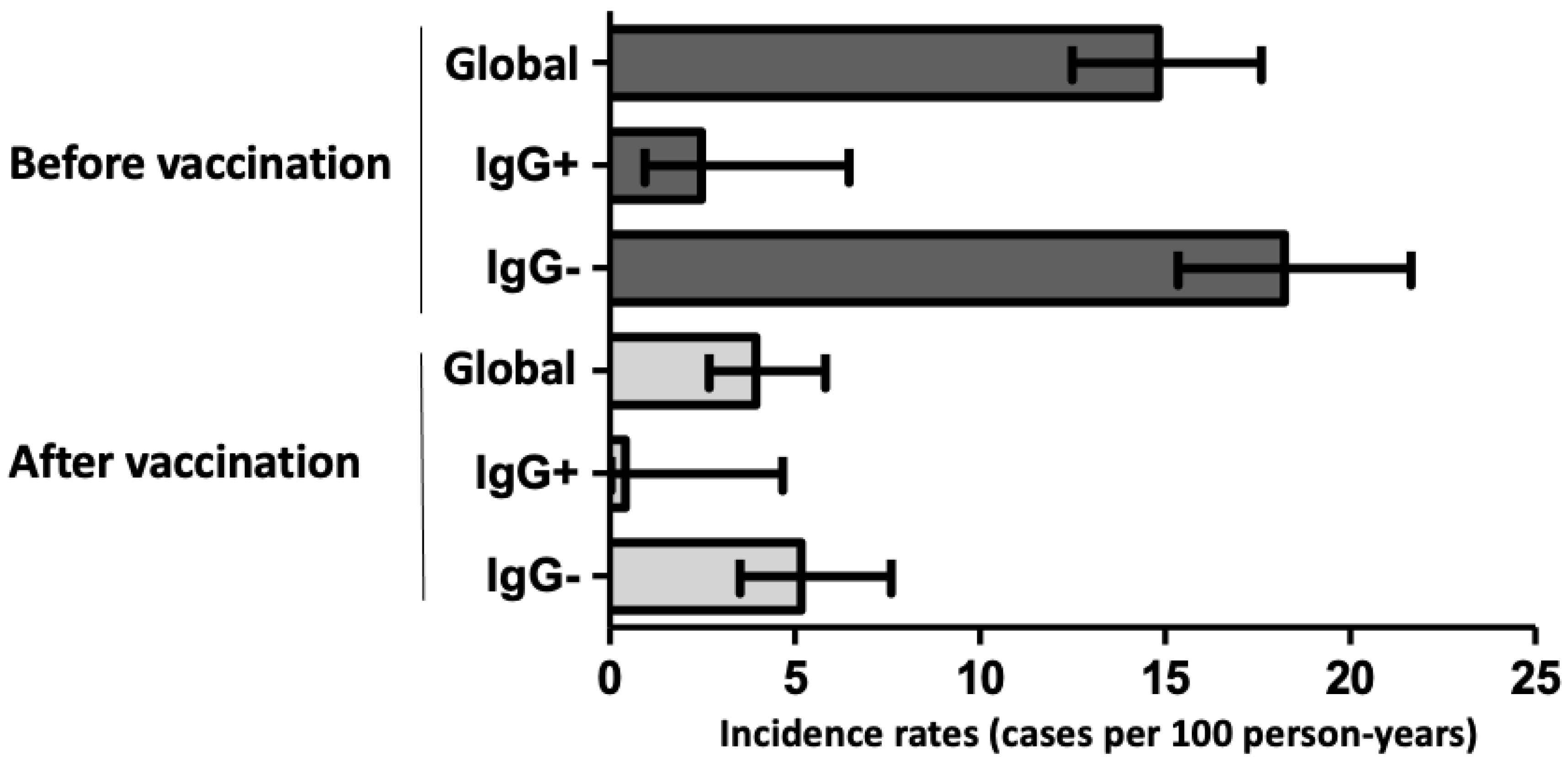
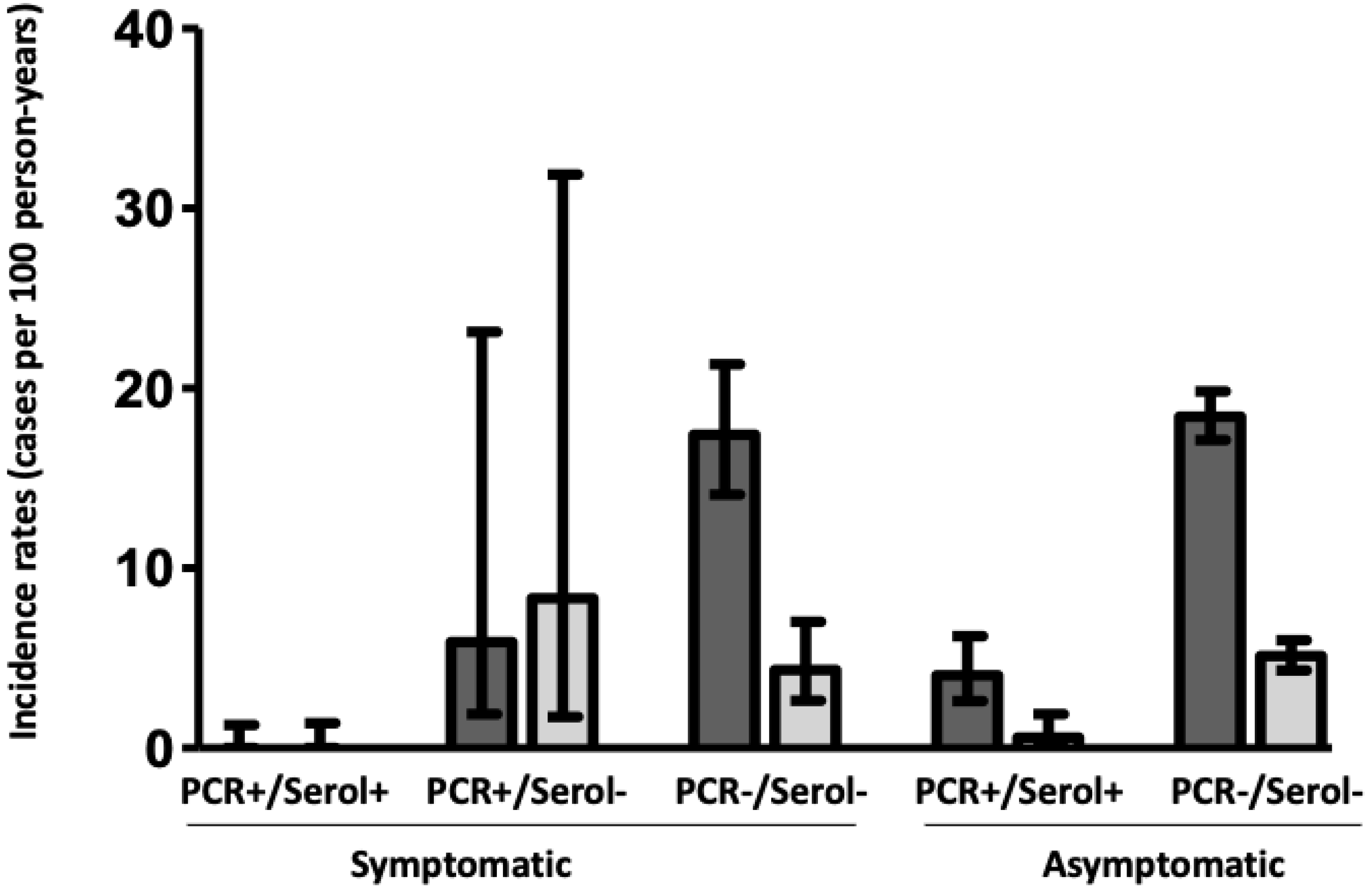
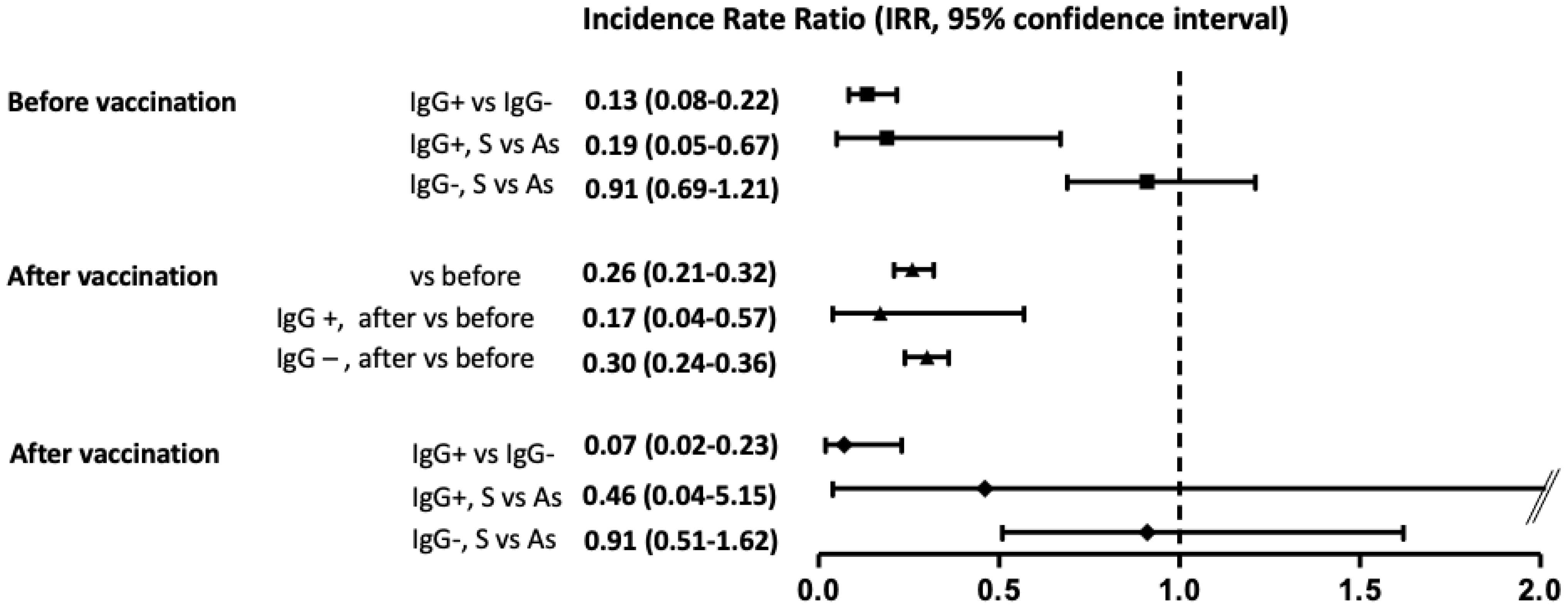
3.1. Infection/Reinfection before Vaccination
3.2. Infection/Reinfection after Vaccination
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Long, Q.X.; Tang, X.J.; Shi, Q.L.; Li, Q.; Deng, H.J.; Yuan, J.; Hu, J.L.; Xu, W.; Zhang, Y.; Lv, F.J.; et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat. Med. 2020, 26, 1200–1204. [Google Scholar] [CrossRef] [PubMed]
- Rydyznski Moderbacher, C.; Ramirez, S.I.; Dan, J.M.; Grifoni, A.; Hastie, K.M.; Weiskopf, D.; Belanger, S.; Abbott, R.K.; Kim, C.; Choi, J.; et al. Antigen-Specific Adaptive Immunity to SARS-CoV-2 in Acute COVID-19 and Associations with Age and Disease Severity. Cell 2020, 183, 996–1012.e1019. [Google Scholar] [CrossRef] [PubMed]
- Lynch, K.L.; Whitman, J.D.; Lacanienta, N.P.; Beckerdite, E.W.; Kastner, S.A.; Shy, B.R.; Goldgof, G.M.; Levine, A.G.; Bapat, S.P.; Stramer, S.L.; et al. Magnitude and kinetics of anti-SARS-CoV-2 antibody responses and their relationship to disease severity. Clin. Infect Dis. 2020, 72, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Casado, J.L.; Vizcarra, P.; Velasco, H.; Hammerle, J.; McGee, A.; Fernandez-Escribano, M.; Vallejo, A. Progressive and Parallel Decline of Humoral and T-Cell Immunity in Convalescent Healthcare Workers with Asymptomatic or Mild-to-Moderate Severe Acute Respiratory Syndrome Coronavirus 2 Infection. J. Infect. Dis. 2021, 224, 241–245. [Google Scholar] [CrossRef]
- Carsetti, R.; Zaffina, S.; Piano Mortari, E.; Terreri, S.; Corrente, F.; Capponi, C.; Palomba, P.; Mirabella, M.; Cascioli, S.; Palange, P.; et al. Different Innate and Adaptive Immune Responses to SARS-CoV-2 Infection of Asymptomatic, Mild, and Severe Cases. Front. Immunol. 2020, 11, 610300. [Google Scholar] [CrossRef]
- Trinite, B.; Tarres-Freixas, F.; Rodon, J.; Pradenas, E.; Urrea, V.; Marfil, S.; Rodriguez de la Concepcion, M.L.; Avila-Nieto, C.; Aguilar-Gurrieri, C.; Barajas, A.; et al. SARS-CoV-2 infection elicits a rapid neutralizing antibody response that correlates with disease severity. Sci. Rep. 2021, 11, 2608. [Google Scholar] [CrossRef]
- Chau, N.V.V.; Thanh Lam, V.; Thanh Dung, N.; Yen, L.M.; Minh, N.N.Q.; Hung, L.M.; Ngoc, N.M.; Dung, N.T.; Man, D.N.H.; Nguyet, L.A.; et al. The natural history and transmission potential of asymptomatic SARS-CoV-2 infection. Clin. Infect. Dis. 2020, 10, 2679–2687. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Oran, D.P.; Topol, E.J. Prevalence of Asymptomatic SARS-CoV-2 Infection: A Narrative Review. Ann. Intern. Med. 2020, 173, 362–367. [Google Scholar] [CrossRef]
- Edridge, A.W.D.; Kaczorowska, J.; Hoste, A.C.R.; Bakker, M.; Klein, M.; Loens, K.; Jebbink, M.F.; Matser, A.; Kinsella, C.M.; Rueda, P.; et al. Seasonal coronavirus protective immunity is short-lasting. Nat. Med. 2020, 26, 1691–1693. [Google Scholar] [CrossRef]
- Barrett, E.S.; Horton, D.B.; Roy, J.; Xia, W.; Greenberg, P.; Andrews, T.; Gennaro, M.L.; Parmar, V.; Russell, W.D.; Reilly, N.; et al. Risk Factors for Severe Acute Respiratory Syndrome Coronavirus 2 Infection in Hospital Workers: Results from a Screening Study in New Jersey, United States in Spring 2020. Open Forum Infect. Dis. 2020, 7, ofaa534. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Rodriguez-Dominguez, M.; Romero-Hernandez, B.; Marcos-Mencia, D.; Fernandez-Escribano, M.; Ferre-Masferrer, M.; Galan, J.C.; Canton, R. SARS-CoV-2 antibodies and utility of point of care testing in Health Care Workers from a spanish University Hospital in Madrid. Clin. Microbiol. Infect. 2021, 27, 1067–1068. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Dao, T.L.; Hoang, V.T.; Gautret, P. Recurrence of SARS-CoV-2 viral RNA in recovered COVID-19 patients: A narrative review. Eur. J. Clin. Microbiol. Infect Dis. 2021, 40, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Lai, X.; Wang, M.; Qin, C.; Tan, L.; Ran, L.; Chen, D.; Zhang, H.; Shang, K.; Xia, C.; Wang, S.; et al. Coronavirus Disease 2019 (COVID-2019) Infection among Health Care Workers and Implications for Prevention Measures in a Tertiary Hospital in Wuhan, China. JAMA Netw. Open 2020, 3, e209666. [Google Scholar] [CrossRef] [PubMed]
- Hunter, E.; Price, D.A.; Murphy, E.; van der Loeff, I.S.; Baker, K.F.; Lendrem, D.; Lendrem, C.; Schmid, M.L.; Pareja-Cebrian, L.; Welch, A.; et al. First experience of COVID-19 screening of health-care workers in England. Lancet 2020, 395, e77–e78. [Google Scholar] [CrossRef]
- Galan, M.I.; Velasco, M.; Casas, M.L.; Goyanes, M.J.; Rodriguez-Caravaca, G.; Losa-Garcia, J.E.; Noguera, C.; Castilla, V.; Working Group Alcorcón COVID-19 Investigators. Hospital-Wide SARS-CoV-2 seroprevalence in health care workers in a Spanish teaching hospital. Enferm. Infecc. Microbiol. Clin. 2020, 40, 302–309. [Google Scholar] [CrossRef]
- Gomez-Ochoa, S.A.; Franco, O.H.; Rojas, L.Z.; Raguindin, P.F.; Roa-Diaz, Z.M.; Wyssmann, B.M.; Guevara, S.L.R.; Echeverria, L.E.; Glisic, M.; Muka, T. COVID-19 in Health-Care Workers: A Living Systematic Review and Meta-Analysis of Prevalence, Risk Factors, Clinical Characteristics, and Outcomes. Am. J. Epidemiol. 2021, 190, 161–175. [Google Scholar] [CrossRef]
- Kluytmans-van den Bergh, M.F.Q.; Buiting, A.G.M.; Pas, S.D.; Bentvelsen, R.G.; van den Bijllaardt, W.; van Oudheusden, A.J.G.; van Rijen, M.M.L.; Verweij, J.J.; Koopmans, M.P.G.; Kluytmans, J. Prevalence and Clinical Presentation of Health Care Workers with Symptoms of Coronavirus Disease 2019 in 2 Dutch Hospitals during an Early Phase of the Pandemic. JAMA Netw. Open. 2020, 3, e209673. [Google Scholar] [CrossRef]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brunink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill. 2020, 25, 2000045. [Google Scholar] [CrossRef]
- Elliott, J.; Whitaker, M.; Bodinier, B.; Eales, O.; Riley, S.; Ward, H.; Cooke, G.; Darzi, A.; Chadeau-Hyam, M.; Elliott, P. Predictive symptoms for COVID-19 in the community: REACT-1 study of over 1 million people. PLoS Med. 2021, 18, e1003777. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Valdes, A.M.; Freidin, M.B.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Ganesh, S.; Varsavsky, T.; Cardoso, M.J.; El-Sayed Moustafa, J.S.; et al. Real-time tracking of self-reported symptoms to predict potential COVID-19. Nat. Med. 2020, 26, 1037–1040. [Google Scholar] [CrossRef]
- Lumley, S.F.; O’Donnell, D.; Stoesser, N.E.; Matthews, P.C.; Howarth, A.; Hatch, S.B.; Marsden, B.D.; Cox, S.; James, T.; Warren, F.; et al. Antibody Status and Incidence of SARS-CoV-2 Infection in Health Care Workers. N. Engl. J. Med. 2021, 384, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Abu-Raddad, L.J.; Chemaitelly, H.; Coyle, P.; Malek, J.A.; Ahmed, A.A.; Mohamoud, Y.A.; Younuskunju, S.; Ayoub, H.H.; Al Kanaani, Z.; Al Kuwari, E.; et al. SARS-CoV-2 antibody-positivity protects against reinfection for at least seven months with 95% efficacy. EClinicalMedicine 2021, 35, 100861. [Google Scholar] [CrossRef] [PubMed]
- Casado, J.L.; Haemmerle, J.; Vizcarra, P.; Rodriguez-Dominguez, M.; Velasco, T.; Velasco, H.; Centenera, E.; Romero-Hernandez, B.; Fernandez-Escribano, M.; Vallejo, A. T-cell response after first dose of BNT162b2 SARS-CoV-2 vaccine among healthcare workers with previous infection or cross-reactive immunity. Clin. Transl. Immunol. 2021, 10, e1341. [Google Scholar] [CrossRef] [PubMed]
- Hansen, C.H.; Michlmayr, D.; Gubbels, S.M.; Molbak, K.; Ethelberg, S. Assessment of protection against reinfection with SARS-CoV-2 among 4 million PCR-tested individuals in Denmark in 2020: A population-level observational study. Lancet 2021, 397, 1204–1212. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Symptomatic | Asymptomatic | |||
|---|---|---|---|---|---|
| PCR+/Serol+ (n = 529) | PCR+/Serol− (n = 24) | PCR−/Serol− (n = 452) | Serol+ (n = 529) | Serol− (n = 3408) | |
| Female sex | 398 (75) | 12 (50) | 371 (82) | 296 (56) | 1704 (50) |
| Age (years) | 44 (32–60) | 39 (22–52) | 44 (33–61) | 41 (23–59) | 47 (24–60) |
| Comorbidities | |||||
| Hypertension | 44 (8) | 4 (13) | 23 (5) | 42 (8) | 68 (2) |
| Diabetes | 11 (2) | 0 | 9 (2) | 0 | 22 (0.6) |
| BMI (Kg/m2) | 24.8 (22.1–26.2) | 26.8 (23–27.3) | 24 (23.5–26) | 26.6 (24.1–27) | 27.2 (24–29.1) * |
| COVID-19 frontline | 365 (69) | 13 (54) | 271 (60) | 335 (63) | 1670 (49) * |
| Symptoms | |||||
| Fever | 302 (57) | 15 (63) | 176 (39) | ||
| Headache | 249 (47) | 9 (38) | 199 (44) | ||
| Anosmia | 222 (42) | 11 (46) | 41 (9) * | ||
| Cough | 423 (80) | 17 (71) | 389 (86) | ||
| Ageusia | 102 (35) | 9 (38) | 41 (9) * | ||
| Sore throat | 233 (44) | 12 (50) | 267 (59) | ||
| Severity a | |||||
| Mild-moderate | 471 (89) | 24 (100) | 434 (96) * | ||
| Severe | 58 (11) | - | 18 (4) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casado, J.L.; Haemmerle, J.; Vizcarra, P.; Ramirez-Alonso, G.; Salazar-Tosco, A.; Romero-Hernandez, B.; Blasco, M.; Rodriguez-Dominguez, M.; Mirabella, I.G.; Vallejo, A.; et al. Risk of SARS-CoV-2 Reinfections in a Prospective Inception Cohort Study: Impact of COVID-19 Vaccination. J. Clin. Med. 2022, 11, 3352. https://doi.org/10.3390/jcm11123352
Casado JL, Haemmerle J, Vizcarra P, Ramirez-Alonso G, Salazar-Tosco A, Romero-Hernandez B, Blasco M, Rodriguez-Dominguez M, Mirabella IG, Vallejo A, et al. Risk of SARS-CoV-2 Reinfections in a Prospective Inception Cohort Study: Impact of COVID-19 Vaccination. Journal of Clinical Medicine. 2022; 11(12):3352. https://doi.org/10.3390/jcm11123352
Chicago/Turabian StyleCasado, José L., Johannes Haemmerle, Pilar Vizcarra, Gema Ramirez-Alonso, Andrea Salazar-Tosco, Beatriz Romero-Hernandez, Magdalena Blasco, Mario Rodriguez-Dominguez, Itria G. Mirabella, Alejandro Vallejo, and et al. 2022. "Risk of SARS-CoV-2 Reinfections in a Prospective Inception Cohort Study: Impact of COVID-19 Vaccination" Journal of Clinical Medicine 11, no. 12: 3352. https://doi.org/10.3390/jcm11123352